
Abstract
Advance care planning (ACP) is inconsistently implemented in emergency departments (EDs), where time constraints limit meaningful patient engagement. Reframing ACP as a holistic, relational nursing practice may enhance its integration into acute care. Guided by Watson's Theory of Human Caring, the Brief Care Preferences Conversation Framework (BCPCF) was developed as a theory-informed nursing intervention to facilitate value-centered, whole-person conversations in time-limited encounters. This study aimed to develop and evaluate the feasibility and clinical utility of the BCPCF in the ED. Development included literature review, expert consultation, and iterative pilot testing. Final evaluation used a practice innovation approach incorporating field observations, workflow assessment, and clinician feedback. The BCPCF supported structured yet flexible conversations integrating physical, psychosocial, and spiritual dimensions of care, with an average duration of 25.3 min and minimal workflow disruption. Beyond feasibility, it facilitated narrative expression, meaning-making, and identification of patient-defined quality-of-life priorities. Documentation met Centers for Medicare and Medicaid Services standards and informed clinical decision making. As a holistic nursing intervention, the BCPCF operationalizes caring science in acute care, supporting relational presence, meaning-centered communication, and whole-person care.
Keywords
Background
Advance care planning (ACP) provides a structured approach for patients to express their preferences for end-of-life or serious-illness care, ensuring their autonomy is upheld even if they become unable to make decisions (Fahner et al., 2019). ACP is anchored to the virtue of respect for persons articulated in the Belmont Report (National commission for the Protection of Human Subjects of Biomedical and Behavioral Research, 1979), formulated in ethical principalism as respect for autonomy (Beauchamp & Childress, 2019), and legally codified in the Patient Self Determination Act of 1990 (Patient Self-Determination Act, 1990). ACP occurs and is documented in various forms including legally prepared documents such as advance directives and durable powers of attorney for health care (DPOA), patient-generated documents using publicly available guides, and provider documentation using either structured or unstructured formats (Jimenez et al., 2018). The overall aim of ACP is to provide goal concordant care, but this relies on patient engagement, provider documentation of the ACP in whatever form it happens to exist, and provider access to ACP documentation at the time of clinical decision making. Our health system, like most, has struggled to formulate processes for ACP that accomplish the patient engagement, documentation, and provider access requirements. ACP conversations do not happen regularly, are not documented consistently, and are often inaccessible in emergency situations when they are most relevant (Pyles et al., 2022; Walker et al., 2018; Waller et al., 2019). The authors identified a need for an ACP conversation framework that could be delivered in a brief, interview-based holistic format suitable for emergency department settings, while still generating substantive information essential for clinical decision making and allowing for translation into standardized, easily accessible documentation. This article describes the development process and feasibility results of the Brief Care Preferences Conversation Framework (BCPCF).
Holistic Theoretical Framework
The literature review and design of the conversation framework was conducted through the lens of Watson's Theory of Human Caring, which emphasizes holistic, relational, and value-based nursing practice (Watson, 2012). Watson conceptualizes persons as unified beings of mind, body, and spirit and positions caring relationships as the ethical foundation of nursing. Central to the theory are the Caritas Processes, several of which directly inform the ACP framework. The process of practicing loving-kindness and equanimity supports respectful engagement with patients as they explore future care preferences, while developing and sustaining a helping–trusting, caring relationship underpins the psychological safety required for meaningful ACP discussions (Watson, 2008). The framework also reflects the Caritas Processes of being authentically present and allowing expression of positive and negative feelings, acknowledging the emotional complexity inherent in serious illness and end-of-life planning (Watson, 2012). In addition, ACP conversations align with Watson's emphasis on supporting meaning-making and honoring existential dimensions of life and death, reinforcing the moral and spiritual dimensions of care.
The BCPCF operationalizes Watson's Caritas Processes through specific communicative practices embedded within the framework. For example, the opening invitation for the patient to “tell me about yourself” enacts Caritas Process 1 (practicing loving-kindness) and Process 4 (developing a helping–trusting relationship), establishing relational presence rather than task-oriented questioning. Exploration of fears, worries, and unacceptable health states reflects Caritas Process 5 (allowing expression of positive and negative feelings), while the structured reflection and summarization at the end of the conversation embodies Process 8 (creating a healing environment) by ensuring the patient feels heard, interpreted, and understood (Watson, 2012). The inclusion of spiritual assessment (FICA) aligns with Caritas Process 10, attending to existential and spiritual dimensions of care (Watson, 2012).
Grounding the framework in Watson's Theory of Human Caring reinforces ACP as a human-centered, ethical nursing practice rather than a purely procedural task. The BCPCF is conceptualized not merely as a communication guide, but as a holistic nursing intervention that supports meaning-making, relational presence, and whole-person assessment in the context of serious illness. This study represents a practice innovation and mixed-methods feasibility evaluation, incorporating iterative framework development, field-based observation, and qualitative clinician feedback.
Methods
Literature and Publicly Accessible Resources Review
Development of the BCPCF began with a rapid scoping of literature and publicly accessible resources for advance care planning. A literature database search was conducted within CINAHL using the Boolean search phrase “advance care plan*” AND (guide OR framework OR outline OR resource OR form OR template). Citations were limited to articles published in English and within the past 5 years and described a framework or guide for advance care planning in adult populations. The literature search resulted in 31 articles that described a tool or framework for ACP conversations. Figure 1 provides a screening process flow chart. Table 1 provides a brief overview of articles and a summary of content they included. When peer-reviewed publications pointed to specific guides, these guides were accessed and reviewed for content.
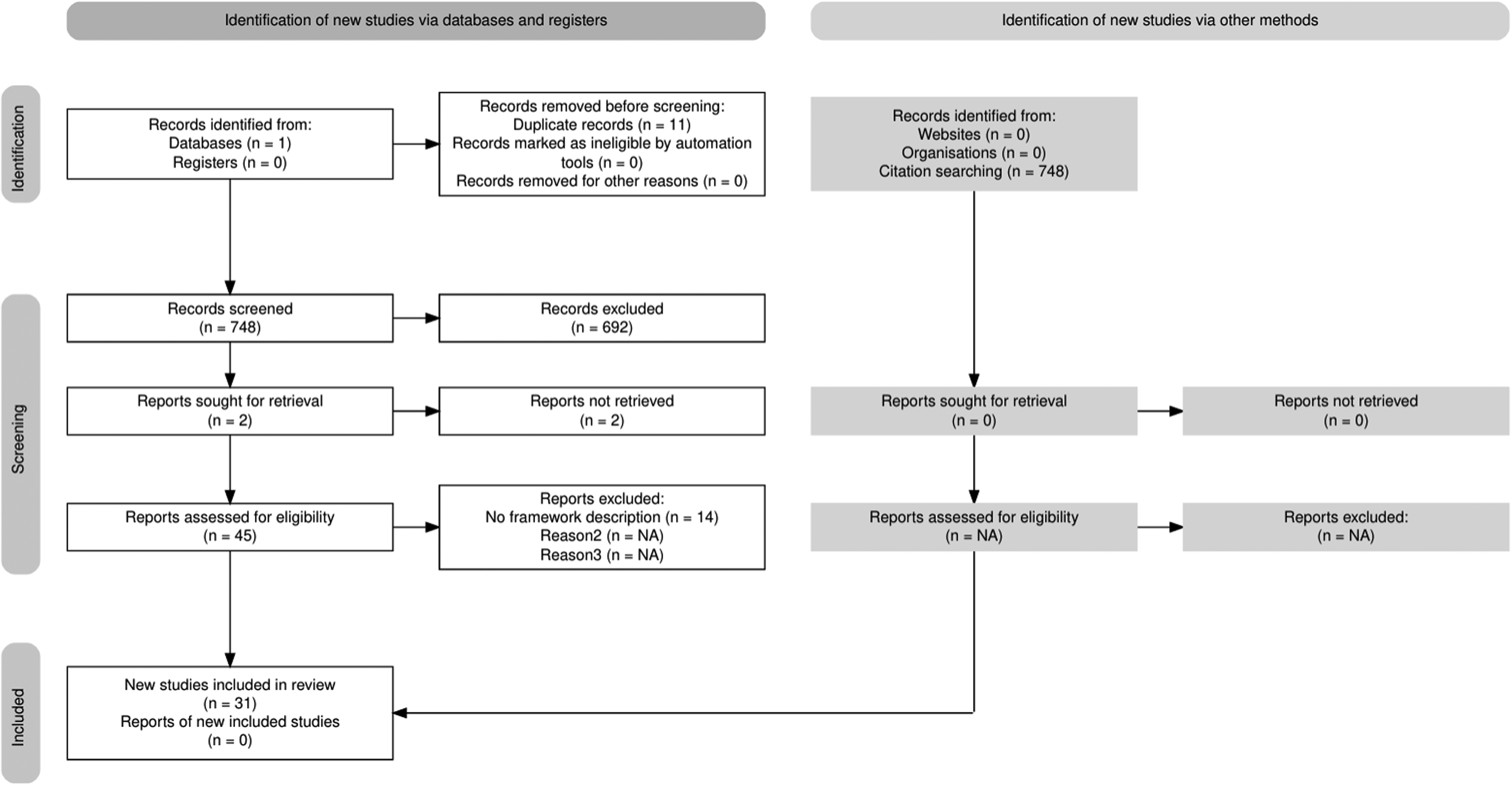
PRISMA flowchart.
Table of Literature
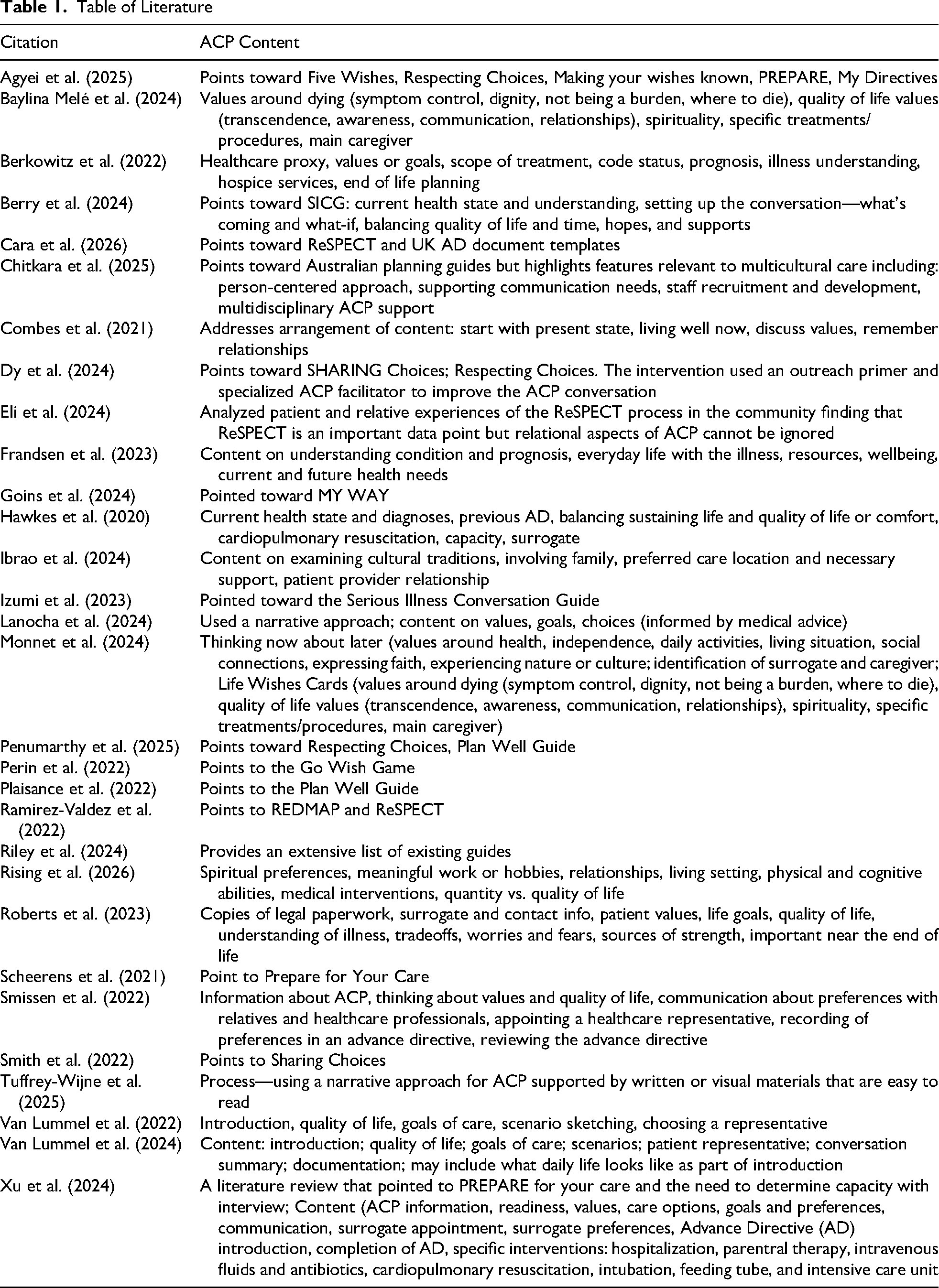
This survey of ACP communication tools included several common content themes and content organization strategies. Many studies mentioned and used or adapted previously published conversation guides or patient-facing fillable forms. Across all conversation guides identified the resources focused on patient values and quality of life priorities, understanding of current health state and prognosis, identification of a surrogate decision-maker, balancing life-prolonging treatment with comfort-focused care, scenarios and “what-if” planning, and finally cultural, spiritual, and/or relational considerations. Conversation guide content is usually structured to start with a discussion of the patient's current health state, diagnoses, and prognosis. The guides then move toward exploring patient values, quality of life goals, and cultural or spiritual beliefs before discussing appointment of a surrogate. Guides then generally move into conversations around goals of care, scenario-specific, and wishes around concrete treatment options like cardiopulmonary resuscitation. Guides often encourage patients or providers to include family, friends, or support persons in these conversations or to communicate the outcome of the conversation to important people.
After this rapid review of literature and available guides, BCPCFv1 was constructed. The script begins with an opening invitation for the patient to talk about themselves. Subsequent questions explore, in this order, support persons, values, quality of life values, health information sharing, concerns about medical treatment, balancing life-prolonging versus comfort-focused treatment at the end of life, specific treatment preferences, a spiritual assessment (FICA), encouragement to talk with trusted persons about their wishes, and a final open-ended question. Questions are either open-ended or on a one-to-one rating scale. A copy of this version is provided in Supplement 1.
Expert Review
The first draft of the BCPCF was sent to a multidisciplinary panel of five experts for review and suggested revisions. This panel included physicians, nurses, and an occupational therapist all with additional training in ethics, palliative care, or end-of-life care. These panel members also had a variety of practice backgrounds but most importantly, had experience in emergency department or inpatient acute care settings. Feedback on the first draft of the BCPCF emphasized shifting away from binary quality-versus-quantity questions and numerically scaled items, which were seen as unhelpful or misleading. Clinicians recommended using scenario-based discussions and free-text narratives to elicit values, clarify thresholds for treatment, and generate more actionable guidance for intensive care unit decision making. Additional recommendations included framing conversations in a way that supports rather than alarms patients, prioritizing identification and preparation of the surrogate decision maker, and exploring potential barriers to surrogate follow-through. Part of the reframing toward supportive language also included feedback on how the conversation would be introduced to both patients and medical staff. The panel felt that words like advance care planning, end-of-life, palliative care, or hospice tend to alarm patients, but also that clinicians are averse to those terms when they feel there are still curative treatment options for the patients. A decision was made to frame the conversation and the service to patients and providers as care preferences conversations. Overall, reviewers encouraged a flexible, patient-centered script that enhances communication. Using this feedback BCPCFv2 was produced (Supplement 2).
Initial Pilot Testing and Further Revision
In the next phase of development, BCPCFv2 was used in 48 patient encounters. During this pilot phase field notes were maintained documenting evolution in the content, organization, and general approach. Overall, the BCPCFv2 functioned as a highly structured documentation tool designed to standardize the capture of advance care planning information across clinical encounters. It worked well in the ED setting because it was brief and aimed at gathering information that was most relevant to clinical decision making. It organized the conversation into discrete domains: patient narrative, surrogacy and support, quality-of-life definitions, treatment preferences, and spiritual assessment (FICA) ensuring that each element was explicitly addressed and recorded. The BCPCFv2's question-driven format emphasized completeness, clarity, and reproducibility, supporting efficient communication among interdisciplinary teams. However, it did prioritize chartable data elements over conversational flow, working primarily as an electronic health record-aligned framework that translated patient values into organized, clinically accessible documentation. As a result, this version failed to integrate the person-centered Charitas Process fully.
Several possible improvements were noted during pilot testing. Prompts were needed to encourage clinicians to explore functional baseline, contextual life details, and patient priorities earlier in the conversation to support a more natural narrative arc. Replacing some rigid, question–answer fields with flexible narrative spaces would allow patients’ values and thresholds for acceptable treatment to emerge more organically. Guidance was needed on setting the stage, reducing communication barriers, and summarizing at the close to further align with real-time clinical communication, making it both structured and more patient-centered.
Final Version Pilot Testing
The final version of the BCPCF was tested again in the ED as part of a quality improvement project to increase ACP among admitted patients. Patients were approached for a Care Preferences Conversation if they had admission orders, decision-making capacity and at least one of the following additional qualifiers: age >70 or late stage chronic/terminal disease. Capacity was determined by the ED physician using the standard criteria of ability to communicate choices, understand relevant information, appreciate the situation and its consequences, and manipulating information rationally (Appelbaum & Grisso, 1988). Late stage chronic or terminal disease was defined as New York Heart Association class III or IV heart failure, chronic obstructive pulmonary disease requiring continuous supplemental oxygen outside of the hospital setting, end-stage renal disease requiring dialysis, cancer with metastasis, chronic degenerative neurological disease diagnosis (Alzheimer's, Parkinson's, Huntington's, Amyotrophic Lateral Sclerosis, etc.), liver cirrhosis requiring frequent large volume paracentesis and/or ascites that is unresponsive to sodium restriction and diuretics. Patients were identified by the ED physician and then added to an ED embedded specialized CARE PREFERENCES CONVERSATION provider's list who engaged the patient in the CARE PREFERENCES CONVERSATION conversation using the BCPCF while the patient was still in the ED.
The aim of this second-level testing was to assess the feasibility of BCPCF use in the ED setting and its effectiveness in capturing data about care preferences that could be documented according to ACP standards and was relevant for medical decision making. Feasibility was assessed by tracking disruptions in medical care delivery or patient transfer/throughput and the average time required to conduct the interview. Documentation quality was assessed via feedback from the medical coding and billing department, whether or not the documented notes meet standard requirements set by the Centers for Medicare and Medicaid for ACP (Centers for Medicare and Medicaid Services, 2024). Usefulness of the documented CARE PREFERENCES CONVERSATION content in medical decision making was assessed through informal direct feedback from physicians throughout the hospital on how the documentation was utilized.
Results
The Brief ACP Conversation Framework
The final BCPCF guide was developed through a process of rapid literature review, expert panel feedback, initial version pilot testing with revision, and final version pilot testing. The resulting guide provides a structured, repeatable approach to conducting serious illness and advance care planning discussions in a busy clinical setting. It begins by establishing rapport and preparing the environment, including introductions, clarifying the purpose of the conversation, identifying all individuals present, and addressing potential communication barriers such as hearing limitations, fatigue, or environmental distractions. The clinician then explores the patient's baseline functioning and living circumstances: where they reside, who supports them, and their abilities regarding mobility, activities of daily living, and use of medical equipment followed by an inquiry into the acute changes leading to the current hospitalization and what matters most in the patient's life at this time. The framework emphasizes understanding the patient's support system and discharge realities, including primary and backup helpers, availability of home services, and safety or logistical concerns such as falls, stairs, medication management, and transportation constraints. Preferences for information sharing and identification of surrogate decision makers are explicitly elicited, along with clarification of values and definitions of acceptable or unacceptable quality of life. These values guide discussions about specific medical decisions, including resuscitation, intubation, feeding tubes, and care location, as well as organ donation. The framework also incorporates a spiritual assessment using the FICA model (Puchalski, 2014). FICA explores patient's spiritual beliefs, how important those beliefs are to the patient and their decision making, whether those beliefs facilitate connection with a community, and how the team might addresss spiritual needs for the patient (Puchalski, 2014). The BCPCF then invites patients to share their worries during hospitalization to capture holistic concerns in a narrative form. Conversations conclude by summarizing key points, reflecting the patient's expressed values, documenting decisions, and ensuring continuity through communication with the broader care team. The final BCPCF can be found in Supplement 3.
Feasibility
Data were derived from field notes written over the course of the implementation by the interventionist. Field notes included observations of workflow integration and informal clinician feedback. While formal qualitative coding was not conducted, recurring patterns in clinician responses and workflow impact were documented and synthesized to assess feasibility and clinical utility. The BCPCF was found to be a feasible strategy for collecting ACP information from patients in the ED setting. Throughout the pilot period, including the testing and revision phase that produced BCPCFv2, the clinician conducted 185 conversation encounters with patients. In those encounters there were only eight delays in patient transport to testing or to the admitting floor, and only four delays for other medical teams attempting to see the patient. The average visit time for the BCPCF interview was 25.3 min. This amount of time might be difficult for acting ED providers to dedicate to ACP conversations and is rarely feasible due to clinical flow. However, a team-based or episodic conversation approach during boarding or periods awaiting imaging might improve feasibility. The ability to sustain relational, holistic conversations within a mean time of 25.3 min challenges assumptions that meaningful caring encounters are incompatible with emergency care workflows.
Reframing the intervention from advance care planning to care preferences conversations played a key role in facilitating acceptance among both clinicians and patients. The care preferences conversation clinician introduced the encounter using person-centered language (e.g., “I’m here to learn about you, your values, and your preferences so that the medical team can deliver care that aligns with who you are”). Comparable language was employed when communicating the purpose of the service to emergency department clinicians. Notably, throughout the pilot period, there were no refusals from either patients or clinicians to engage in care preferences conversations.
Documentation Quality
Documentation quality was reviewed by the documentation and coding specialist at the healthcare system. BCPCF produced care preferences conversation notes met all minimum requirements established by the Centers of Medicare and Medicaid for compliance and billing. Additionally, the documentation was formatted so that each of the primary categories in the BCPCF functioned as a header for narrative content. This make the documentation easy to reference for clinical decision making as well as quality review.
Utility for Medical Decision Making
Provider feedback revealed that the care preferences conversation notes generated by the BCPCF were helpful especially as informative data points for code status conversations and in serious illness conversations. One physician noted, “When I talked to the patient, he wanted to be a full code, but your note covered a lot more ground. I’ll have a follow up conversation.” In this case, the care preferences conversation facilitated additional relational interaction with the physician. Physicians took action upon do-not-attempt-resuscitation (DNAR) preferences in the care preferences conversation notes on a routine basis, changing patient code status orders. Additionally, care preferences conversation notes were referenced in goals of care and ethics conversations which facilitated transitions into palliative care versus curative treatment. Again, care preferences conversations were a starting point, facilitating additional person-center, relational interaction with the healthcare team. Nearly one-third of patients who were engaged in care preferences conversation also had a chaplaincy consult ordered to address existential and spiritual concerns raised during the conversation. Care preferences conversation notes were also utilized by case management as references for discharge planning and identification of resource needs. In one patient's case, after repeated visits to the ED and admissions, the BCPCF facilitated conversation uncovered that his primary reason for readmission was a lack of transportation to his dialysis appointments. He maintained strong preferences for curative treatment but lacked the resources to implement the treatment plan. Case management in the ED was able to mobilize resources to fill the gap. Overall, providers found that BCPCF-generated care preferences conversation notes delivered meaningful, actionable insights that improved code-status discussions, guided goals-of-care and ethics decisions, supported discharge planning, and even uncovered critical barriers to effective treatment, thereby enhancing both clinical decision making and patient care. Care preferences conversations became an anchoring point for more person-centered, holistic, multidisciplinary care in the ED.
Discussion
These findings suggest that transpersonal caring is not inherently time-intensive but can be intentionally structured within brief clinical encounters when supported by a theory-guided framework. This study extends beyond feasibility by demonstrating how structured communication can serve as a vehicle for transpersonal caring in high-acuity environments. Consistent with Watson's Theory of Human Caring, the BCPCF facilitated encounters that moved beyond information exchange to relational and meaning-centered engagement, even within the constraints of emergency care. Patients were not simply asked about treatment preferences; they were invited to articulate who they are, what matters most, and how they understand health, illness, and quality of life. For example, care preferences conversation conversations frequently surfaced existential concerns, including fear of dependency, loss of identity, and desire for dignity, underscoring the importance of addressing not only physical but also existential suffering in acute care settings.
Spirituality emerged as an essential yet often under-addressed dimension of care preferences conversation. The integration of the FICA tool allowed patients to articulate sources of meaning, hope, and strength, which in turn informed their preferences for treatment and acceptable outcomes. This highlights the role of nurses in facilitating spiritually integrated care, particularly in moments of vulnerability and uncertainty.
Prior research has consistently shown that care preferences conversation conversations occur infrequently, are documented inconsistently, and are often inaccessible at the point of clinical decision making, particularly in the emergency department (ED) where time pressures and workflow interruptions impede such discussions (Pyles et al., 2022; Walker et al., 2018; Waller et al., 2019). The BCPCF directly addresses these system-level gaps by providing a structured, repeatable method for eliciting patients’ values, treatment preferences, and contextual life circumstances in a manner aligned with both ethical commitments to autonomy and the practical constraints of emergency care. The iterative refinement of the BCPCF—shaped by expert input and grounded in common thematic elements identified across existing ACP guides—reflects the broader literature emphasizing patient-centered inquiry, surrogate identification, and scenario-based discussions as essential components of high-quality care preferences conversations. The feasibility and utility demonstrated in this study further align with evidence that structured care preferences conversation documentation enhances communication across interdisciplinary teams and supports more goal-concordant care. These findings therefore reinforce the need for scalable, ED-appropriate care preferences conversation tools that can reliably translate patient values into actionable clinical guidance.
The intentional shift in terminology from advance care planning to care preferences conversations was central to clinician and patient engagement. Care preferences conversation clinicians framed the encounter as an opportunity to understand patients as individuals and to elicit values and preferences that could meaningfully inform clinical care.
Relational and Meaning-Centered Dimensions of Care
Beyond feasibility, the BCPCF facilitated narrative expression and meaning-making among patients. Patients frequently shared personal values, life priorities, and definitions of acceptable quality of life, suggesting that the framework created space for existential reflection even within time-limited ED encounters. These narratives informed not only treatment preferences but also provided clinicians with deeper insight into the person behind the patient, strengthening relational engagement and supporting more individualized care. The inclusion of the FICA spiritual assessment revealed that spiritual beliefs often influenced patients’ perspectives on suffering, recovery, and acceptable interventions, though these insights were not routinely captured in standard ED documentation prior to implementation of the BCPCF.
Limitations
This study has several limitations. It was conducted within a single health system, which may limit generalizability to institutions with different workflows, staffing models, or documentation structures. The pilot relied on field notes and informal clinician feedback rather than formal qualitative or quantitative evaluation methods, potentially introducing bias. Additionally, care preferences conversation conversations were performed by a specialized clinician embedded in the ED, which may not reflect the feasibility of implementation in settings without dedicated care preferences conversation personnel. The embedded role of the care preferences conversation clinician may have influenced both uptake and perceived effectiveness, representing a potential source of implementation bias. Finally, the study did not evaluate patient experience, surrogate preparedness, or longitudinal alignment of care with expressed values, leaving important outcomes unmeasured. Currently, the limitations of this study necessitate additional, more rigorous testing and limit immediate transferability of this intervention to other care delivery sites.
Research Implications
The development and pilot testing of the BCPCF carries several important research implications for the nursing practice areas of emergency medicine, palliative care, and health-systems communication. The BCPCF should be more rigorously tested using established qualitative and quantitative methods. More generally the documented inconsistency, inaccessibility, and infrequency of care preferences conversation conversations in acute care settings highlights a persistent systems-level gap that future research should explore through comparative evaluations of ACP frameworks across diverse clinical environments. The BCPCF's iterative development—grounded in literature review, expert input, and pilot testing—demonstrates the value of mixed-methods approaches in creating clinically feasible communication tools, suggesting that future studies should further investigate how structured frameworks influence the quality, fidelity, and equity of ACP conversations. Additionally, the feasibility data, including minimal workflow disruptions and a consistent average completion time, indicate a need for research examining how team-based or episodic delivery models may optimize ACP conversation integration without burdening nurses or other clinicians in fast-paced practice environments like the ED. The demonstrated utility of BCPCF-generated documentation in downstream clinical decision making also raises important questions regarding how care preferences conversation notes shape interprofessional communication, guide treatment trajectories, and identify modifiable social or logistical barriers to care. Finally, given the framework's emphasis on narrative elicitation and patient-centered values, future research should examine its impact on patient experience, surrogate preparedness, and goal-concordant outcomes, thereby establishing a stronger evidence base for care preferences conversation interventions in high-acuity settings.
Practice Implications
The BCPCF presents several practice implications that are highly relevant for clinicians working in high-acuity environments such as the emergency department. First, the BCPCF positions nurses as leaders in advance care planning by equipping them with a structured yet flexible approach to facilitate complex, value-laden conversations. Nurses are uniquely situated to operationalize this framework given their focus on holistic assessment, relational continuity, and patient advocacy. Though, in order to facilitate nurses’ ability to implement the BCPCF, there is a stronger need for targeted training in communication, presence, and existential inquiry within nursing education. One important development is that nurses or other clinicians should frame advance care planning as care preferences conversations and use person-centered language that emphasizes understanding patients’ values and goals to guide care. Introducing these discussions as a way to align medical treatment with who the patient is, rather than as formal planning, can improve acceptance among both patients and clinical colleagues.
The BCPCF's structured yet patient-centered design offers a practical approach for integrating advance care planning into routine clinical workflows without imposing excessive cognitive or temporal burden on providers. By guiding nurses to systematically assess baseline function, living circumstances, surrogate decision-making structures, and patient-defined thresholds for acceptable quality of life, the framework enhances the clarity and relevance of care preferences conversation documentation for downstream decision-makers. Additionally, the incorporation of values-based inquiry and scenario-specific discussions promotes more nuanced and clinically actionable guidance, helping multidisciplinary clinicians align treatment plans with patient preferences even under conditions of uncertainty. The emphasis on communication, such as identifying information-sharing preferences, addressing spiritual concerns, and summarizing key decisions, reinforces interdisciplinary coordination and improves continuity across care transitions. Because the BCPCF can be deployed efficiently during ED boarding or periods of diagnostic waiting, it represents a feasible model for embedding care preferences conversation into fast-paced settings traditionally challenged by workflow interruptions. Overall, the BCPCF supports a culture of proactive, informed, and patient-aligned decision making, strengthening both the quality and ethical grounding of acute care practice.
Conclusion
The development and pilot testing of the BCPCF illustrate the potential for a structured, patient-centered approach to advance care planning within the constraints of emergency care. By integrating insights from existing ACP frameworks, expert review, and iterative testing, the BCPCF offers a practical model capable of eliciting nuanced patient values, informing clinical decision making, and improving documentation quality. Its feasibility in the emergency department demonstrates that meaningful care preferences conversations can occur even in time-pressured, interruption-prone settings when supported by a dedicated workflow and trained personnel. Although this study's single-site design, reliance on informal feedback, and lack of patient-centered outcomes limit generalizability, the findings point to promising avenues for future research. Continued refinement and broader evaluation of the BCPCF may contribute to more consistent, accessible, and goal-concordant care for seriously ill patients across acute care environments.
Supplemental Material
sj-docx-1-jhn-10.1177_08980101261458999 - Supplemental material for Development and Feasibility of the Brief Care Preferences Conversation Framework
Supplemental material, sj-docx-1-jhn-10.1177_08980101261458999 for Development and Feasibility of the Brief Care Preferences Conversation Framework by Clayton C. Clark in Journal of Holistic Nursing
Supplemental Material
sj-docx-2-jhn-10.1177_08980101261458999 - Supplemental material for Development and Feasibility of the Brief Care Preferences Conversation Framework
Supplemental material, sj-docx-2-jhn-10.1177_08980101261458999 for Development and Feasibility of the Brief Care Preferences Conversation Framework by Clayton C. Clark in Journal of Holistic Nursing
Supplemental Material
sj-docx-3-jhn-10.1177_08980101261458999 - Supplemental material for Development and Feasibility of the Brief Care Preferences Conversation Framework
Supplemental material, sj-docx-3-jhn-10.1177_08980101261458999 for Development and Feasibility of the Brief Care Preferences Conversation Framework by Clayton C. Clark in Journal of Holistic Nursing
Footnotes
Acknowledgements
The author would like to acknowledge Rae Guinan, MD, Lea Brandt PhD, and Alison Gorman for copy editing and project support.
Ethical Considerations
The project associated with this work was submitted to the Institutional Review Board of the University of Missouri and was determined not to be human subjects research, project number 2132924.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.