
Abstract
Keywords
Projected population prevalence of disability among older people makes it a major public health concern (Khaw, 1999; McMurdo, 2000). It is, therefore, important to identify modifiable risk factors that could facilitate prevention and recovery from disability in middle and old age (Ebrahim, 1999). Recent health policy suggests that “there are few public health initiatives that have greater potential for improving health and well-being than increasing the activity levels of the population” (Chief Medical Officer, 2004, p. 20). Physically active people are at lower risk of developing a wide range of major chronic diseases including coronary heart disease, stroke, diabetes, some cancers, and of premature death (American College of Sports Medicine, 1998). Given the relationship between chronic illness and disability onset among older people (Adamson, Beswick, & Ebrahim, 2004; Adamson, Lawlor, & Ebrahim, 2004), factors which are likely to reduce the prevalence of these diseases are also likely to improve disability outcomes. In addition, there is an increasing body of literature demonstrating a relationship between increased physical activity and maintenance of functional ability and mobilty disability ( Brach et al., 2003; Hillsdon, Brunner, Guralnik, & Marmot, 2005; LaCroix, Guralnik, Berkman, Wallace, & Satterfield, 1993; Singh, 2002; Stuck et al., 1999; Visser, Pluijm, Stel, Bosscher, & Deeg, 2002) as well as recovery from disability (Wannamethee, Ebrahim, Papacosta, & Shaper, 2005).
Previous studies have tended to measure physical activity as a composite score based on a combination of several activities from domestic, work, and leisure domains (LaCroix et al., 1993; Wannamethee et al., 2005). Although these variables often can reflect frequency and/or intensity of exercise, few are derived with policy-driven recommended levels of activity in mind. It is therefore difficult to assess the possible effects of such recommendations on the risk of developing disability. From these composite measures, it is also impossible to differentiate between physical activity related to different aspects of life, for example, work compared to leisure activities, which may have implications for any attempts to develop new health policy on activity.
In addition, there is a well-documented pattern of decline in physical activity levels across the age span, with few older adults achieving the recommended minimum of an accumulation of 30 min of moderate activity on most days of the week.
Because most adults do not pursue the team sports and activity patterns of their younger years into midlife, this means that the promotion of activities that do persist into later adult life (although continued participation varies by class and gender), such as walking, swimming, social dancing, keep fit/aerobics, and golf (Hunt, Ford, & Mutrie, 2001), is crucial to successful health promotion. It is therefore important to examine whether there is an association between particular types of sporting activity and disability onset amongst older people. Here we examine whether overall activity levels (according to recommended criteria; Pate et al., 1995) and earlier sporting activities are associated with the onset of locomotor disability (LD) in early older age in a general population sample.
Method
Participants
Participants are from the oldest cohort of the West of Scotland Twenty-07 Study, a longitudinal study of social patterning of health in three age cohorts (Benzeval et al., 2009). Participants have completed a wide-ranging nurse-administered questionnaire and undergone basic physical measurements every 5 years or so. The sample (approximately 1,000 people in each age cohort) was drawn as clustered random samples from the Central Clydeside conurbation. The samples were shown to be representative of the populations from which they were drawn, using comparison data from the 1991 census (Der, 1998).
Materials and Procedure
This study uses data from two interview waves conducted in 1991 and 1995-1996 and focuses on data on the oldest cohort (aged 58 and 63 years, respectively). Ethical approval was obtained from the Glasgow University Ethics Committee for nonclinical research involving human participants.
Exercise, sport and potential confounding variables
In 1991, when participants were aged around 58 years (n = 858), the interview schedule included questions about physical activity in work (hard physical work, stair climbing) and home and leisure settings (light and heavy housework, chores and maintenance, gardening, walking, stair-climbing, cycling). These questions gathered information on past (defined as since leaving school) physical activity and current physical activity based on the Allied Dunbar National Fitness Survey. These data contributed to summary indicators of overall activity level (Berger, Der, Mutrie, & Hannah, 2005). The total number of weekly occasions of moderate activity lasting 30 min or above and vigorous activity lasting 20 min or above were estimated. Respondents were then dichotomized to reflect whether or not they achieved an “active lifestyle,” which was defined as attaining either three occasions of vigorous activity lasting 20 min per week or five occasions of moderate activity lasting 30 min. This approach was commensurate with previous recommendations for active living from the U.S. Centers for Disease Control and Prevention and the American College of Sports Medicine, which encourages the accumulation of activity from various settings, including work, home, and leisure (Pate et al., 1995).
Respondents also answered a detailed section on past and current participation in specified games and sports (Hunt et al., 2001). These were presented on a series of cards that listed 52 activities, grouped into cards for team games, individual sports, training and fitness activities, outdoor activities, and other games and sports. Respondents indicated which sports/activities they did regularly (meaning at least once a week for 2 or more months in the year) and provided subsequent detail on indicators of intensity (makes the person out of breath or sweaty) and frequency (how many days in a year). They were also asked to indicate which of the 52 sports/activities they had done regularly earlier in their life (excluding sports/activities that they had only done while still at school) but had stopped doing regularly. For each sport done in the past, total number of years done and the age at which they gave up were recorded. Summary variables were constructed for key types of sporting activity: dance/keep-fit (social dancing, dancing for fitness, exercise/circuit training, keep-fit/aerobics), walking (walking, rambling, hiking, backpacking), swimming, golf, racket sports (tennis, squash, badminton), and active team sports (football, hockey, rugby, netball, basketball) currently (at age 58) and in the past only (during adult life but given up by age 58).
Data were also collected on a wide range of other variables including gender, occupational social class, physical measurements (taken by the nurse), severity and frequency of pain in major joints, and chronic illness (see Berger et al., 2005).
LD
At age 58, and when interviewed again around age 63, respondents (n = 723) completed a modified version of the U.K. Office of Population Censuses and Surveys (OPCS) disability questionnaire. The OPCS disability scales were based on the conceptual framework of the World Health Organization’s (1980) International Classification of Impairments, Disabilities, and Handicaps (ICIDH). These questions were used for the OPCS study of the prevalence of disability in the United Kingdom—scoring on 13 functional areas in which a person may require assistance or experience difficulty, one of which was LD (Martin, Melzer, & Elliot, 1988). LD is derived from questions pertaining to a person’s reported physical performance across a number of tasks, including, for example, “What is the furthest you can walk on your own without stopping and without severe discomfort?” and “Could you walk up and down one step on your own?” Other tasks include bending and straightening, balance, and the number of falls in the past 12 months. The minimum score for each dimension is 0 (i.e., no disability); those responding positively to any question in the locomotor section of this questionnaire were classified as having LD.
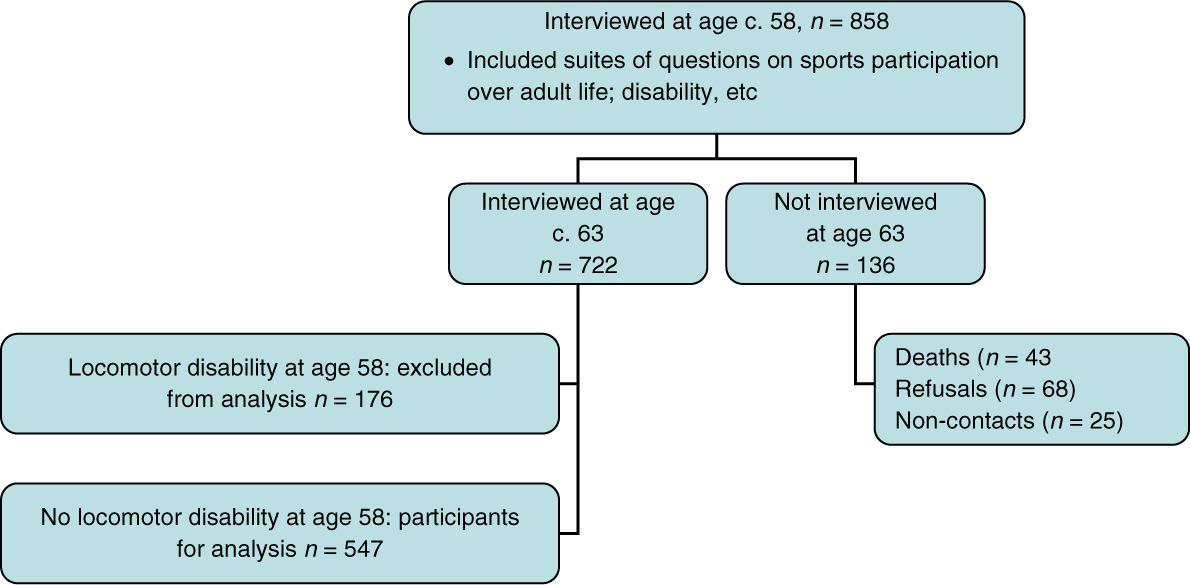
Of the 723 respondents who were interviewed at both ages, 176 (24.3%) had LD when interviewed at age 58. The analysis is based on 547 men and women as we focus on the onset of LD between the ages of 58 and 63; the 176 respondents with LD at age 58 were excluded from the longitudinal analysis (Figure 1).
Numbers of participants
Data Analysis
Data were analyzed using Stata Version 8. The associations between each of the sporting activities and LD were initially assessed using chi-square. The relationships were explored further using multivariable logistic regression, adjusting for potential confounding factors including gender, occupational social class, overall level of activity at age 58, chronic conditions at age 58 (whether has a respiratory, musculoskeletal, digestive, cardiovascular disease and/or mental health condition), experience of joint pain in lower limbs at age 58, and lifestyle factors (smoking and healthy diet).
As the physical activity measurements were based on self-report, the validity of these measures was tested by investigating associations between these variables (using t test and chi-square where appropriate) and others known to be markers of physical “fitness.” For example, increased physical activity has been associated with lower resting pulse rate, greater forced expiratory volume (FEV), higher social class, and reduced cigarette smoking in large population surveys (Lawlor, Taylor, Bedford, & Ebrahim, 2002; Smith, Shipley, Batty, Morris, & Marmot, 2000). All of these markers were associated with each of the sporting activities.
Results
Of the 547 who were free of LD at age 58, 117 (21.4%) had LD 5 years later. This did not differ for men and women (men 22.0%, women 20.8%, p = .738).
Overall, just 45% of men and 30% of women (p < .001) were achieving either 5 moderate or 3 strenuous episodes of activity. Fewer women than men achieved this level of activity across all the domains (work, nonleisure, leisure, nonwork) except home-based activity where only 3% of men and 4% of women achieved this level. More women than men participated in dance/keep-fit activities at age 58 (p < .001), but more men than women were currently regularly participating in most of the other sporting activities including swimming (p = .001) and golf (p < .001). Few (2% of both men and women) were current players of racket sports and no one was regularly involved in active team sports at age 58.
When the summary indicators of overall physical activity (i.e., achieving either 5 moderate or 3 strenuous episodes of activity across all domains) were entered into separate logistic regression models (adjusted for gender and occupational social class), there was no evidence of an association between any of the measures of overall physical activity and onset of LD (see Table 1, Model 1). This lack of evidence for an association persisted when the models were additionally adjusted for the presence of various types of chronic diseases (respiratory, musculoskeletal, digestive, cardiovascular, and mental illness), the experience of joint pain in the lower limbs (hip, knee, ankle, and foot), and lifestyle risk factors (current smoking and diet) at age 58 (Model 2).
Odds Ratios for Physical Activity and Various Types of Sporting Activity in Adult Life at 58 Years and Onset of Locomotor Disability by 63 Years
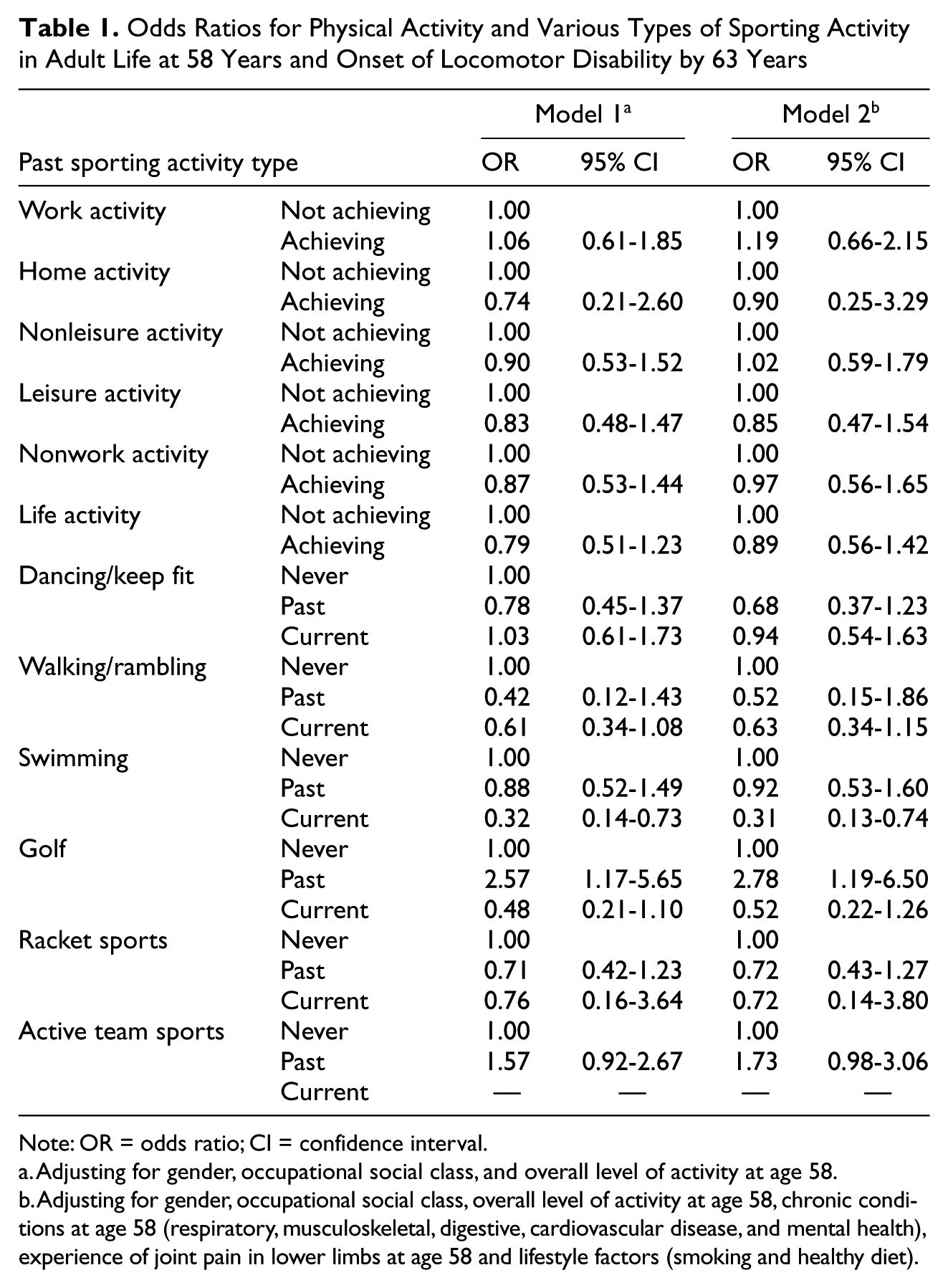
Note: OR = odds ratio; CI = confidence interval.
Adjusting for gender, occupational social class, and overall level of activity at age 58.
Adjusting for gender, occupational social class, overall level of activity at age 58, chronic conditions at age 58 (respiratory, musculoskeletal, digestive, cardiovascular disease, and mental health), experience of joint pain in lower limbs at age 58 and lifestyle factors (smoking and healthy diet).
The current sporting activities that were most prevalent among those people who were free of LD at age 58 were dancing/keep fit (16% men, 26% women), walking/rambling (22% men, 18% women), swimming (24% men, 15% women), and golf (16% men, 7% women; see Table 2). Current involvement at age 58 was unrelated to LD 5 years later for dancing. Although current walking was associated with a substantial reduction in disability onset (of 39%) and those currently playing golf at age 58 were approximately half as likely to report LD onset, these findings were not statistically significant (OR for walking = 0.61, 95% CI = 0.34-1.08; OR for golf = 0.48, 95% CI = 0.21-1.10). Swimming was the only sporting activity to show strong evidence of a protective association between current regular participation at age 58 and onset of LD within the following 5 years: those who were current swimmers at age 58 were at a substantially reduced risk of LD at age 63 (OR = 0.32, 95% CI = 0.14-0.73, adjusted for gender and occupational social class) in comparison with those who had never regularly engaged in swimming in adult life (see Table 1, Model 1). The protective effect of current swimming was not reduced by additional adjustment for the presence of chronic illness, experience of lower joint pain, and lifestyle risk factors at age 58 (OR = 0.31, 95% CI = 0.13-0.74; Table 1, Model 2).
Distribution of Men and Women Currently Achieving Recommended Levels of Physical Activity and Taking Part in Various Types of Sporting Activity at Age 58 Years
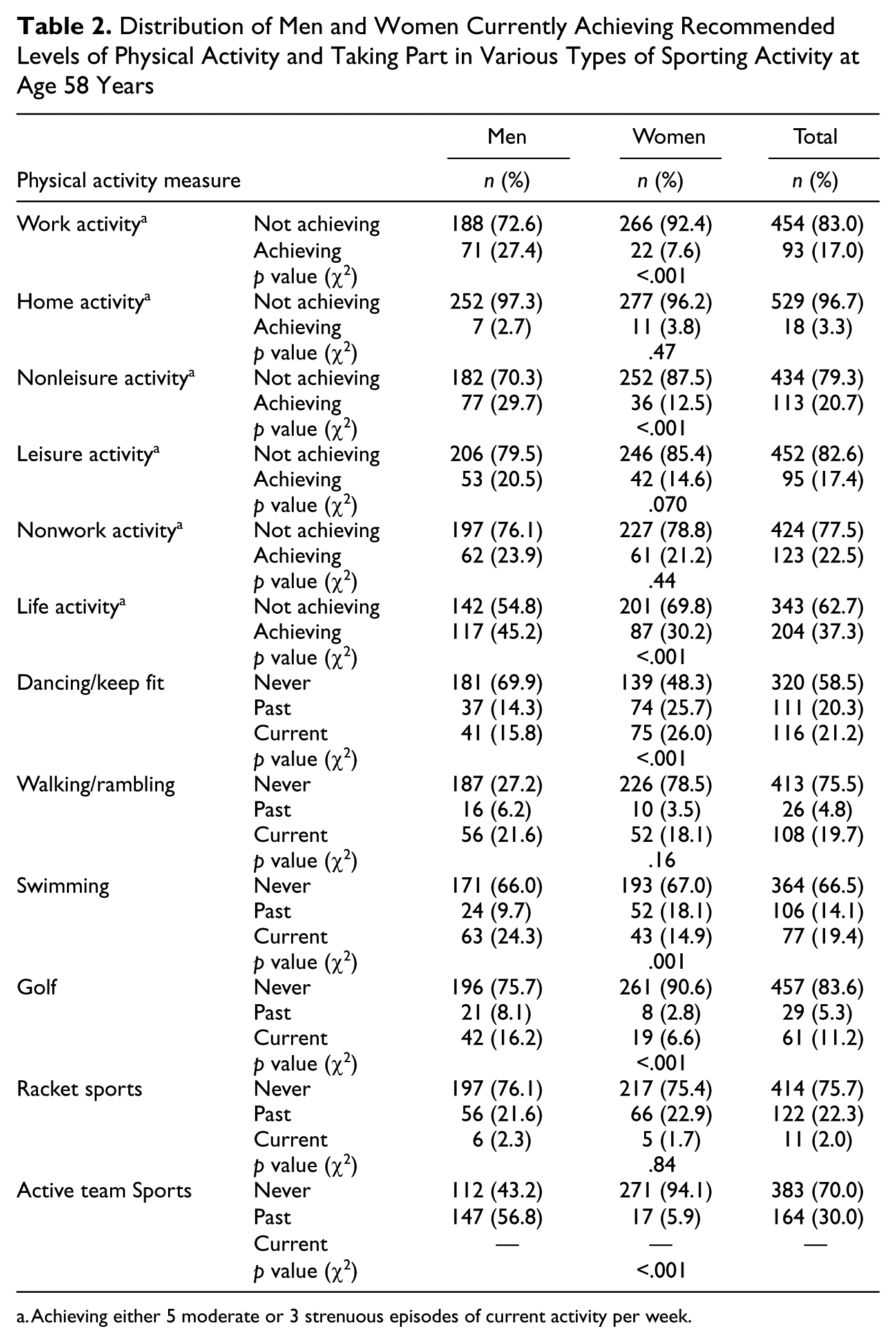
Achieving either 5 moderate or 3 strenuous episodes of current activity per week.
Of the physical activities reported to have been undertaken in the past (i.e., since leaving school but discontinued by age 58), only golf showed some evidence of an adverse relationship with LD at age 63. The risk of LD was elevated for people who had regularly played golf in the past (but were no longer playing at age 58; OR = 2.57, 95% CI = 1.17-5.65, adjusted for gender and occupational social class). Fully adjusted models showed no reduction of the odds ratio.
When the sporting activity measures were tested for validity, it was found that resting pulse rate was lower among those currently reporting physical activity (data not shown). With the exception of currently dancing, all current physical activity was associated with better lung function (as measured by higher FEV scores). These findings suggest the self-reports were valid for our purposes. As predicted, achieving current recommended levels of physical activity was more prevalent among the nonmanual social classes and prevalence of smoking was lower among those reporting any form of current physical activity. These analyses suggest that the measurements we used for physical activity reflected participants’ level of fitness and provide evidence of the construct validity of these measures.
Half (n = 68) of the 136 losses to follow-up between the two time points were due to participants withdrawing from the study, 32% (n = 43) were due to deaths, and 18% were people who were not able to be contacted at follow-up. Responders at age 63 were more likely to be current golf-players (9% vs. 4%) and less likely to be ex-golfers (6% vs. 10%) at age 58 than nonresponders at age 63 (p = .039). Similarly, responders were more likely to be current (12% vs. 5%) or ex-swimmers (19% vs. 16%) and less likely to be never-swimmers (68% vs. 79%). Responders and nonresponders did not differ on the other measures of sporting activities or of achievement of the minimum recommended levels of activity for health.
Discussion
Our analyses did not provide strong evidence to suggest that meeting the recommended targets for physical activity in early old age is associated with decreased LD onset after 4 years. This finding is contrary to the pattern emerging from other studies (Boyle, Buchman, Wilson, Bienas, & Bennett, 2007; Hillsdon et al., 2005; LaCroix et al., 1993; Lang, Guralnik, & Melzer, 2007; Stuck et al., 1999) and the conclusions drawn in the 2008 Physical Activity Guidelines for Americans, which affirms that regular physical activity reduces the risk of many adverse health outcomes (Chodzko-Zajko et al., 2009). However, the literature has not been consistent. For example, Wannamethee et al. followed 4,430 men over a 4-year period and found that, when those with mobility limitation at baseline were excluded, the development of mobility limitation was not significantly associated with physical activity after adjustment for age, lifestyle factors, and chronic illnesses (Wannamethee et al., 2005). Tager, Haight, Sternfeld, Yu, and Der Laan (2004) also failed to find clear evidence for any independent effect of leisure time physical activities for both men and women.
However, when sporting activities were examined, the data do suggest that swimming in later adult life may provide substantial protection against LD in early old age. The other sporting activities examined were not found to have consistent relationships with LD. Like other physical activities, swimming could plausibly have effects on LD via increased strength, increased stamina and flexibility, or via a reduction in risk of chronic illness. However, swimming will promote such benefits whilst placing relatively little stress on the joints of the lower limbs. The adverse effects of past golfing is difficult to explain, as this relationship was not found for other past sporting activities—however, this may reflect declines in physical capacity (3-4 hr of steady walking required) or temporary episodes of illness.
Study Limitations
Information ascertained on previous sporting activity may be prone to recall bias. Given contemporaneous public health messages at the time of data collection, which promoted increased physical activity, it is likely that respondents will have overestimated their previous physical activity, rather than underestimated this. There is no reason to suggest that this pattern would vary according to particular sporting activity. Nor is it likely that reporting of previous sporting activity will be systematically different among those reporting disability compared to not, as the physical activity questions were collected at Wave 2 (at age 58) and the disability outcome measured at Wave 3 (at age 63). These potential sources of bias would tend to lead to overestimation of the strength of association between previous sporting activity and LD, but as we found no strong evidence for such associations, this does not appear to be the case.
By using prospective longitudinal data, we have attempted to address the potential issue of reverse causality as a possible explanation for associations shown between physical activity and LD. As we restricted our analysis to those individuals who reported being disability free at Wave 2 of data collection, it is unlikely that their reporting of the independent variables were related to the LD outcome as recorded at Wave 3. This strategy has been employed in previous studies. (LaCroix et al., 1993; Wannamethee et al., 2005) However, we cannot rule out the possibility that the process of disability had started at the time of Wave 2 data collection but was not severe enough to cross the threshold we utilized to be considered as having a disability. For example, our measures of physical activity may have been, in essence, a proxy for good health and high levels of functioning rather than independent risk factors. However, currently performing any of the sporting activities considered was not associated with chronic illness, whereas there was evidence of an association between being active (5 moderate or 3 strenuous episodes of current activity per week in any aspect of life) and chronic illness. We would expect all activities to be similarly affected by this subtle reverse causality effect but because we observed different relationships with sporting and all activities, we suspect that our findings are not affected by reverse causality.
One further possibility for some of the negative findings from our data could be that the study was underpowered to detect differences in LD according to some types of sporting activity and therefore may have been prone to Type 2 errors.
Conclusion
Given that physical and sporting activities can occur in different modes, at differing frequencies, and at varied intensities, these are complex concepts to measure. However, the Twenty-07 data set provides a rare opportunity to study activity levels in the context of a detailed longitudinal social survey. In particular being able to focus on both recommended activity levels (derived from work, home, and leisure) and on specific sporting activities is unusual. The findings suggest that consideration should be given to promoting swimming in both childhood and adulthood as a form of activity that has the potential to give health benefits whilst placing relatively little stress on the joints of the lower limbs and can be pursued into old age. For example, Glasgow provides free access to swimming for older adults and this is a policy that could be adopted elsewhere. Such protection is important as most current guidelines on increasing physical activity place emphasis on activities such as walking and stair-climbing, which can be easily incorporated into daily life (Department for Culture Media and Sport, 2002; Scottish Executive, 2002) but depend on maintaining locomotor ability.
Footnotes
Acknowledgements
The authors are grateful to all the participants in the study and to the survey staff and research nurses who carried it out. The data are collected by the MRC Social and Public Health Sciences Unit. The funders had no role in the design, execution, analysis and interpretation of the data, or the writing up of the study. Thanks to Sally Macintyre for comments on an earlier draft.
Declaration of Conflicting Interests
The author(s) declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
The author(s) disclosed that they received the following support for their research and/or authorship of this article: West of Scotland Twenty-07 Study funded by the UK Medical Research Council (WBS: U.1300.80.001.00001).