
Abstract
Introduction
The Hispanic Health Paradox asserts that, despite experiencing disproportionate exposure to purported risk factors for excess morbidity and mortality associated with low socioeconomic position, Mexican American immigrants generally have more favorable health outcomes compared with Mexican Americans born in the United States (U.S. born) and non-Latino Whites (Markides & Coreil, 1986). Furthermore, the longer these healthy immigrants resided in the United States and acculturated, the more likely they were to report deterioration in health status indicators compared with recent immigrants (Antecol & Bedard, 2006).
To explain immigrant health deterioration, Rogler and colleagues described “acculturation as an exogenous force shaping the conditions for the rise to psychological distress” (Rogler, Cortes, & Malgady, 1991). This phenomenon was later called the “acculturative stress” hypothesis and became widely used in mental health studies and generalized to an array of other health outcomes research with Latino populations. However, acculturation stress models have important limitations in health research because they confound cultural change effects on health behaviors with pathology, they are not temporally specific and thus inconsistent with developmental models of health. We offered the alternative “acculturation-health” hypothesis to emphasize that health outcomes are instead conditional on multiple life-course contingencies that vary in importance as determinants over the life span (González et al., 2009). The acculturation–health temporal relationships can range from negative to positive during the life span of an individual. Acculturation stress assumes a cumulative, dose-response negative linear association between acculturation and health. Acculturation-health involves interactions between endogenous (within-person) and exogenous (extra-person) factors that may affect health differentially over the life course.
The proposed acculturation-health model assumes that there are multiple points in the life course that are critical for improving health and lowering the risk of “weathering effects” seen in minority aging (Geronimus, 1992). Carefully focused research could lead to timely and effective interventions that improve health outcomes across the life course. The assumption of a constant acculturation–health relationship that is generally negative leading to declines in Mexican American health is limiting because it is overly deterministic and restricts opportunities for identifying determinants of long-range outcomes and life-course stages when they are most consequential. Although we can assume that living in a new society introduces behavioral, social, and environmental changes that may negatively influence health, there may be benefits as well, such as learning new occupational skills, greater exposure and understanding of public health and medical information, and the use of preventive medical services. Nevertheless, it is unclear how these changes are expressed in the health of older Mexican Americans in the long run.
Negative aspects of the acculturation–health relationship dominate current thinking about Mexican American health, especially regarding acculturation-related changes in risk behaviors such as diet, exercise, and substance abuse (Morales, Lara, Kington, Valdez, & Escarce, 2002). However, most of this evidence comes from studies with younger Latinos (Lara, Gamboa, Kahramanian, Morales, & Bautista, 2005). If the acculturation–health association is conditional and predicated on various endogenous and exogenous life-course factors, recent work among older adults may better inform us about the long-term acculturation–health relationship. Among older Mexican Americans and in contrast to younger adults, the relationship between acculturation and health appears positive from extant studies (González et al., 2009; González, Haan, & Hinton, 2001; Markides, Eschbach, Ray, & Peek, 2007). A limitation of much of the work on acculturation and health, including older Mexican Americans, is that outcomes are largely based on self-reports of health status that can be influenced by cultural response biases (Finch, Hummer, Reindl, & Vega, 2002). That is, objective outcomes, such as biomarkers, are generally not available. The exception is a study by Crimmins, Kim, Alley, Karlamangla, and Seeman (2007) that demonstrated that foreign-born Latinos and non-Latino Whites had similar “biological risk profiles.” They reported healthy immigrant advantages in “biological risk profiles” among aggregated Latino ethnic groups. Second, most studies use proxy measures of acculturation (e.g., years of U.S. residency or nativity), which provides little information on variations in cultural and behavioral patterns (Lara et al., 2005).
One study purpose was to examine if the “healthy immigrant” phenomenon persisted among older Mexican Americans by examining a cluster of biological markers associated with the metabolic syndrome. Obesity and metabolic disorders, including diabetes, are health problems among many Americans, particularly Mexican Americans (Flegal, Carroll, Ogden, & Curtin, 2010). As such, we believed that examining a well-recognized syndrome offers more useful information to clinicians and public health readers than an array of biomarkers. Second, we sought to evaluate the relationship between metabolic syndrome biomarkers and a measure of acculturation that provides information on more nuanced variations in cultural and behavioral patterns. For this, we used a large sample of older Mexican Americans. Based on previous work (Eschbach et al., 2007; González et al., 2001; Haan et al., 2003; Markides et al., 2007), we expected that rates of the metabolic syndrome between U.S.-born and foreign-born Mexican Americans would not differ. Second, we expected that higher acculturation would be associated with lower metabolic syndrome risk among foreign-born older Mexican Americans. Third, we examined the relationship between biomarkers and acculturation while including other factors, such as socioeconomic position and health insurance (Adler et al., 1994; Andersen & Newman, 1973; Crimmins, Hayward, & Seeman, 2004). Finally, we examined the metabolic syndrome among older Mexican Americans in the context of comparing the prevailing “acculturative stress” hypothesis and “acculturation-health” hypothesis, which assumes multiple points in the life course that are critical for improving health, to understand their utility for the study of health. As in previous work, it was anticipated that the nonlinear aspects of the acculturation-health hypothesis would be of higher utility than the prevailing acculturation stress hypothesis in understanding the relationship between culture and health at different developmental epochs.
Method
Study Participants
Participants are from the Sacramento Area Latino Study on Aging (SALSA), which is a prospective cohort study of older Latinos living in the Sacramento valley of northern California. The study was approved by the institutional review boards of the University of Michigan and of the University of California, Davis. Analyses for this report were approved by the Human Investigation Committee of Wayne State University. All SALSA participants were 60 years or older and self-designated as Latino (85.6% Mexican origin). The methods of enumeration and recruitment procedures have been previously published and produced a sample that was representative of older Latinos residing in the targeted areas (Haan et al., 2003). Briefly, surveys were conducted by bilingual/bicultural technicians in the participants’ homes to obtain demographic, health, and functional status information. Survey instruments were translated from English to Spanish and then back-translated to English to ensure the accuracy of the translations. The total baseline year (1998/1999) sample of the SALSA was 1,789 participants. In this study, we focused on participants with valid baseline biomarker data (N = 1,598). Individuals with missing biomarker data were older, less likely to own a home, and had a lower reported income and education level. They were also less acculturated and more likely to be foreign born compared with respondents with complete data.
Biomarker Outcome Measures
Cross-sectional data for these analyses came from the SALSA baseline year (1998/1999). During in-home, face-to-face interviews, study participants underwent a clinical assessment that included anthropometry, fasting blood draw, and blood pressure. High-density lipids, triglycerides, and glucose levels were assayed from fasting blood samples. Waist circumference measurements (cm) were taken at umbilicus level at mid-respiration with the participant standing erect. Systolic and diastolic blood pressure (mmHg) was measured using a standard arm cuff.
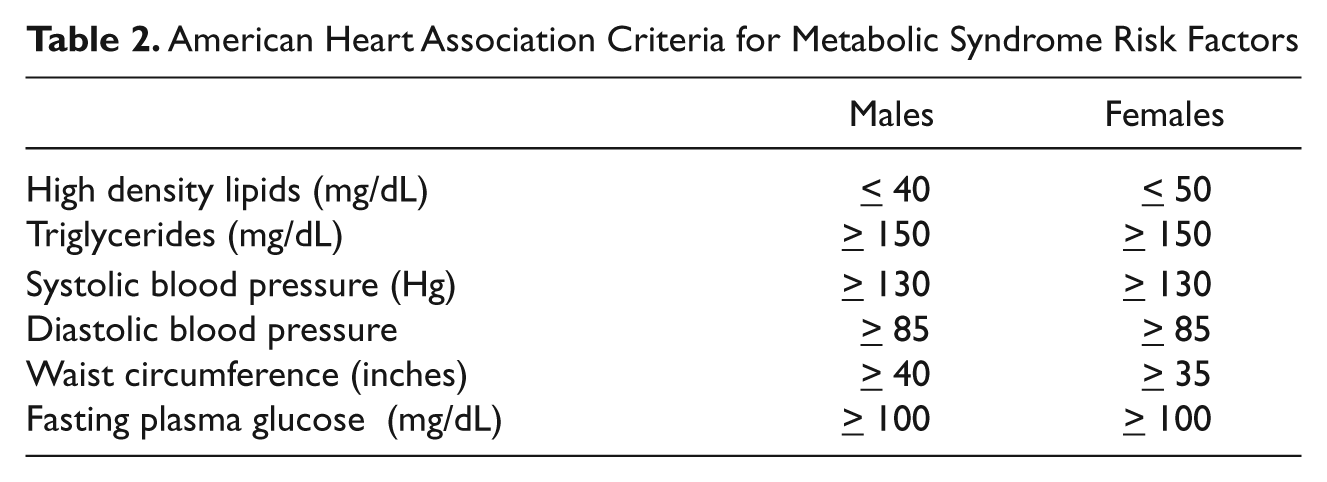
We used the American Heart Association (AHA) criteria to define metabolic syndrome biomarkers criteria and to identify study participants who met criteria (Grundy et al., 2005). Our study was focused on objective metabolic syndrome biomarkers. Therefore, antihypertensive medications were excluded in generating our outcome measure. The five AHA metabolic syndrome biomarker criteria were recoded dichotomously. Following AHA guidelines, we applied gender-specific dichotomization to all criteria. Values exceeding threshold levels were assigned a value 1, to indicate the criterion was met, and all other valid values assigned a 0. AHA metabolic syndrome criteria are shown in Table 2. A hypertension criterion was generated based on values meeting criterion for either systolic or diastolic risk classified at or above criterion levels. Furthermore, an additive risk scale (count) was created by summing total scores (range 0-5) based on the five dichotomous variables indicating criteria were met. To create our metabolic syndrome indicator, we applied AHA criteria to categorize the summed scores of three or more on our additive scale as meeting metabolic syndrome criteria with all other lesser values assigned to the reference group.
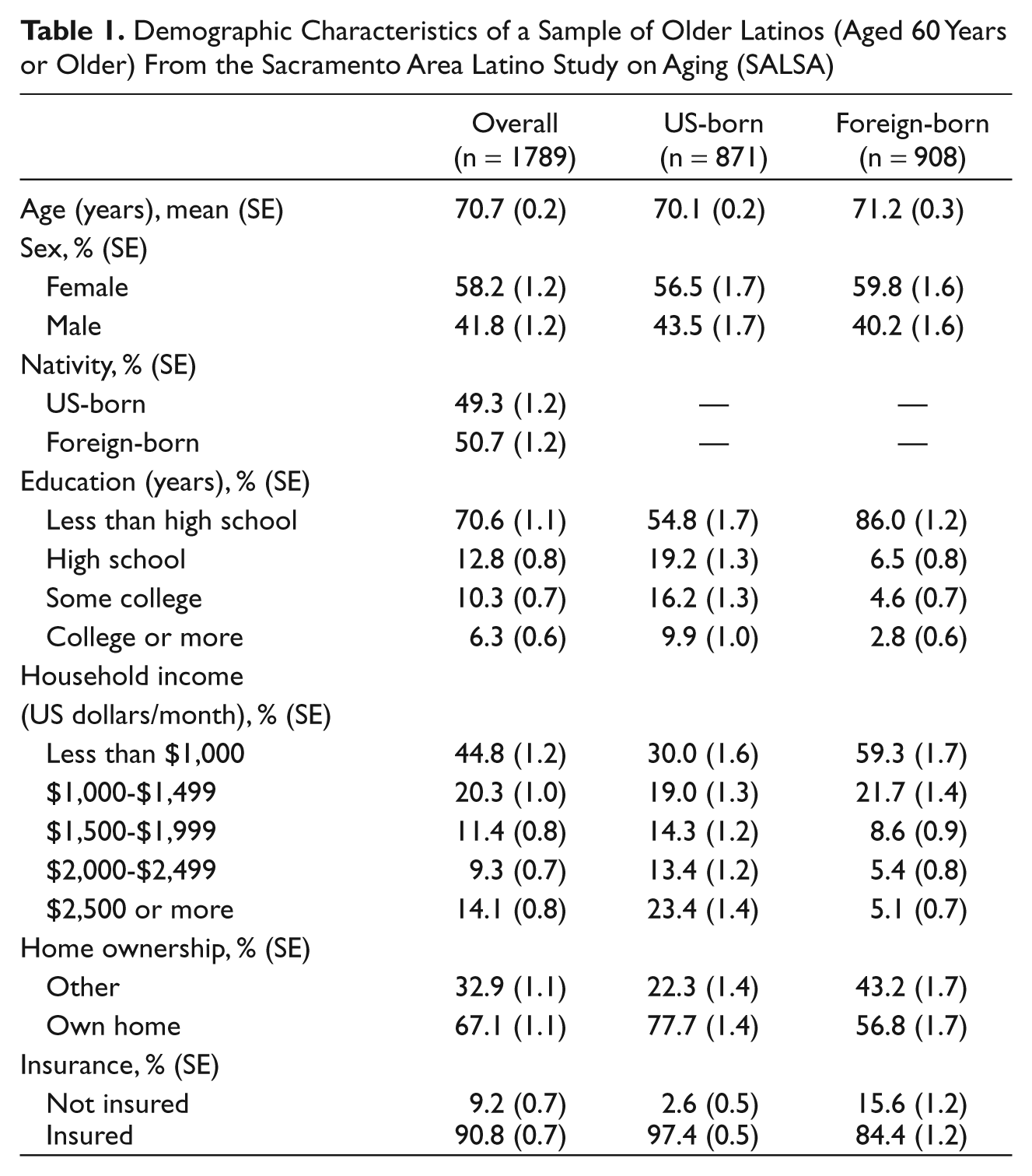
Demographic Characteristics of a Sample of Older Latinos (Aged 60 Years or Older) From the Sacramento Area Latino Study on Aging (SALSA)
American Heart Association Criteria for Metabolic Syndrome Risk Factors
Acculturation
The primary predictor variable of interest was acculturation. To assess acculturation, we used the revised Acculturation Rating Scale for Mexican Americans-II (ARSMA-II; Cuellar, Arnold, & Maldonado, 1995). Briefly, the ARSMA is a series of 17 Likert-type self-ratings on cultural practices, such as language and media use and social network contacts. The Likert-type ratings were then summed across items (range = 17-70).
Statistical Approach
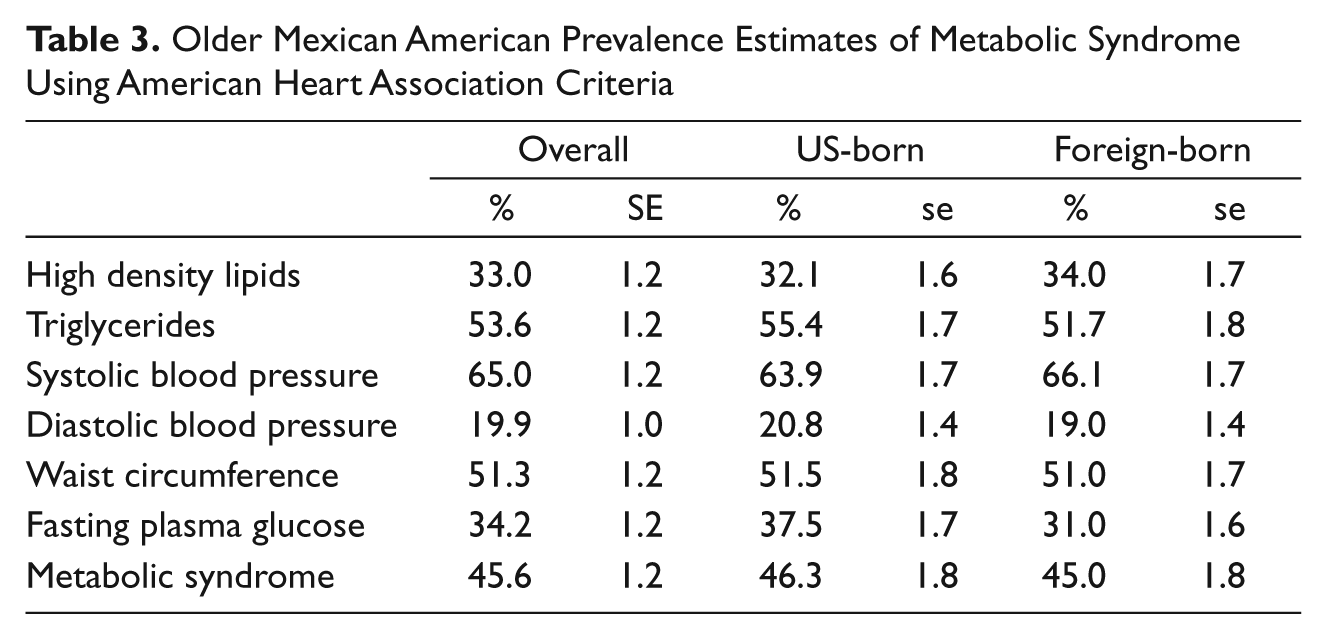
First, sample estimates describing demographic and socioeconomic characteristics including age (continuous), sex (female, male), nativity (foreign born, U.S. born), education (four categories: less than high school, high school degree, some college, and college or more), monthly household income (five categories: less than US$1,000, US$1,000-US$1,499, US$1,500-US$1,999, US$2,000-US$2,499, and US$2,500 or more), home ownership (own home or not), and health insurance coverage (insured or not insured) were calculated. Second, prevalence rates for the metabolic syndrome AHA criteria (Table 3) were estimated. These prevalence estimates were further disaggregated by nativity. Third, a logistic regression model was used to estimate the relationship between metabolic syndrome and acculturation and nativity. Of particular interest were the differential effects of acculturation on metabolic syndrome across nativity groups, which were captured using a multiplicative interaction term created between acculturation and nativity. Second, the multivariate logistic regression model was fit to account for the confounding effects of (a) socioeconomic indicators and (b) health insurance coverage. Both models were age and sex adjusted. The Stata statistical package (Release 10.1) was used for all of the analyses in this study (StataCorp, 2008).
Older Mexican American Prevalence Estimates of Metabolic Syndrome Using American Heart Association Criteria
Results
Table 1 shows selected demographic and socioeconomic indicators for the overall SALSA sample and the disaggregated U.S.-born and foreign-born groups. More than 85% of the SALSA sample was of Mexican origin, and the remainder were Central and South American, which is consistent with 2000 U.S. Census estimates for California (Census, 2000). We used the term Mexican American as this is the prevailing Latin American culture of the Sacramento valley and the number of Central Americans was very small. The sample was evenly split between U.S.- and foreign-born groups (Table 1). The foreign-born sample had significantly lower levels of education and household income, were significantly less likely to own their home, and were significantly less likely to have health insurance coverage compared with their U.S.-born counterparts.
Metabolic Syndrome
The U.S.- and foreign-born samples were evenly matched on each of the AHA metabolic syndrome biomarker criteria. With the exception of hyperglycemia, U.S.- and foreign-born respondents did not differ significantly in their metabolic risk profile. Nearly half of the sample (45.6%) met AHA criteria for the metabolic syndrome biomarkers and the two nativity groups were not statistically distinct (χ2 = .26; p = .61).
Metabolic Syndrome, Acculturation, and Nativity
Higher ARSMA-II scores indicating more acculturation were associated with significantly decreased odds of the metabolic syndrome (Table 4, Model 1). Of particular interest were the differential effects of acculturation on metabolic syndrome across nativity groups, which were captured in a multiplicative interaction term created between acculturation and nativity. The interaction term was significant, indicating that the effect of acculturation on the odds of metabolic syndrome varied by nativity (p = .045). The nonsignificant effect of nativity on metabolic syndrome, indicated at the bivariate level above, was reproduced using our multivariate results. When socioeconomic factors were introduced in Model 2, the effect (OR) of acculturation on metabolic syndrome was slightly attenuated. Accounting for the socioeconomic indicators also had an attenuating effect on the statistical significance of the interaction term (p = .053). The predicted probabilities of the metabolic syndrome by nativity groups across acculturation scores are plotted in Figure 1. The plots suggest that acculturation plays a more pronounced role for foreign-born respondents than U.S.-born ones. The effects of acculturation among U.S.-born respondents are largely uniform. Among the socioeconomic indicators considered, only the two middle-household income categories were significantly associated with lower odds of the metabolic syndrome relative to the lowest income group.
Predictors of Metabolic Syndrome Using American Heart Association Criteria Using Sample of Older Latinos (Aged 60 Years or Older) From the Sacramento Area Latino Study on Aging (SALSA)
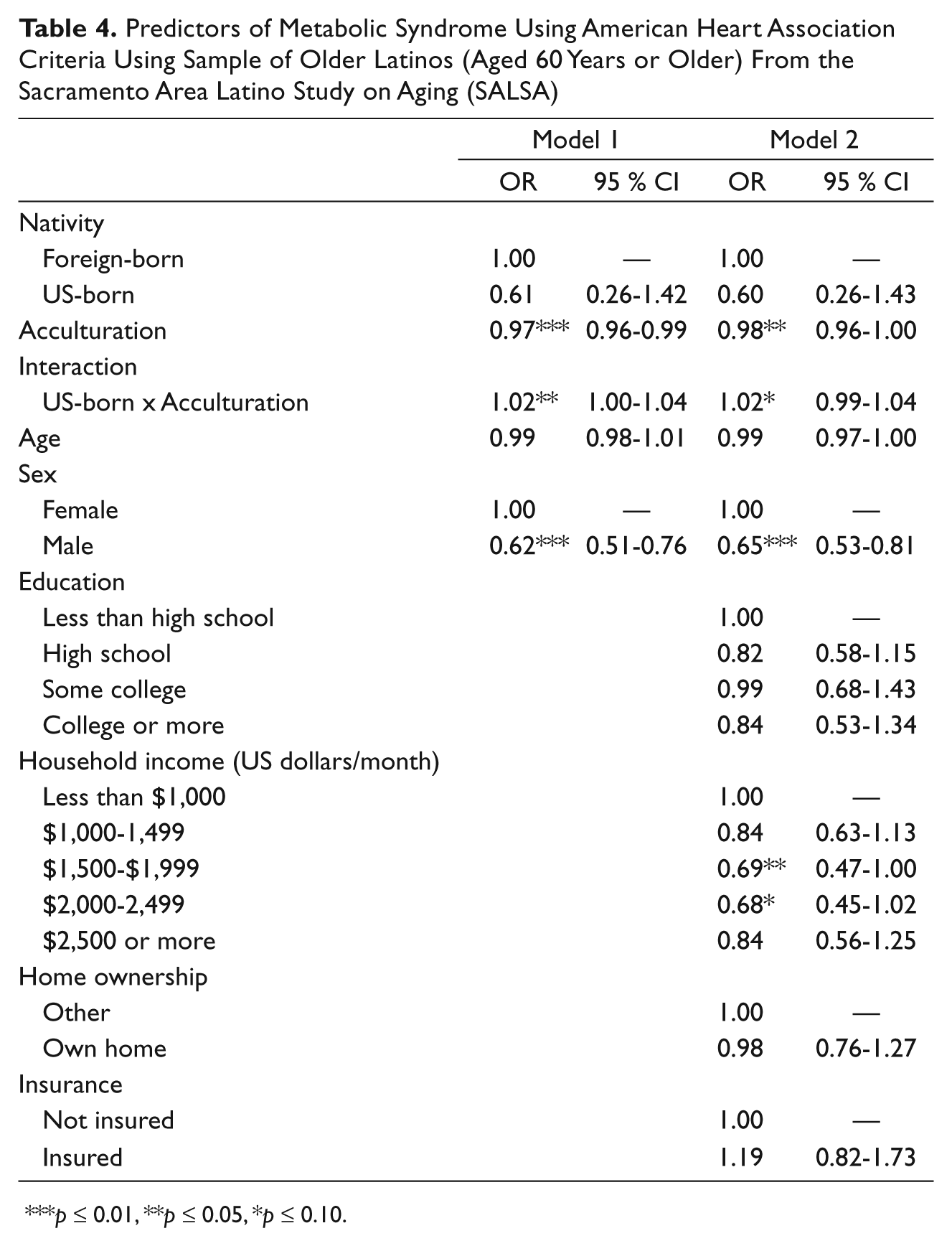
p ≤ 0.01, **p ≤ 0.05, *p ≤ 0.10.
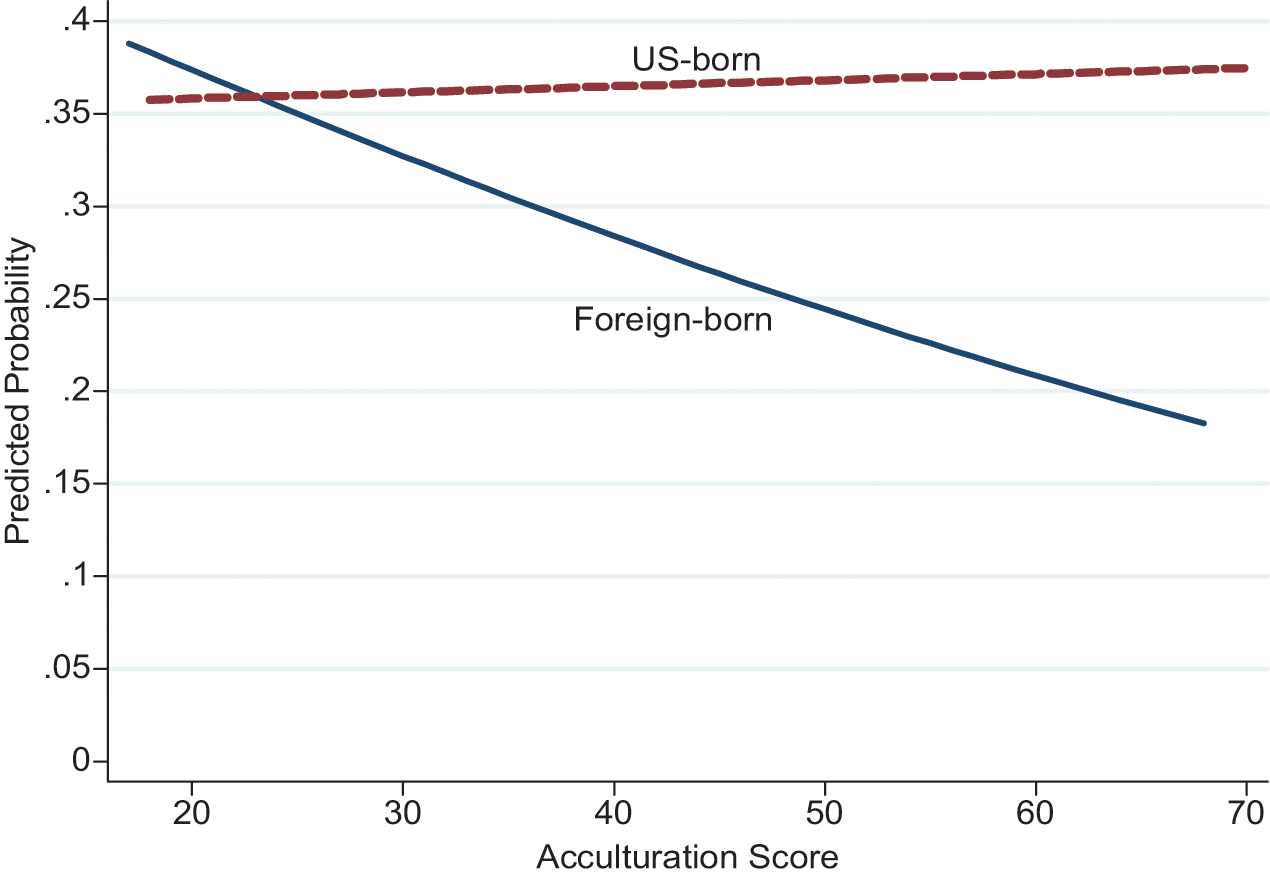
Predicted probability of metabolic syndrome using American Heart Association criteria using sample of older Latinos (aged 60 years or older) from the Sacramento Area Latino Study on Aging (SALSA)
Discussion
Two main findings emerged from our study. First, we found no metabolic syndrome biomarker evidence of healthy immigrant advantages over U.S.-born Mexican Americans. Second, higher acculturation was associated with lower risk for meeting AHA criteria for the metabolic syndrome among foreign-born Mexican Americans. The findings herein extend previous work based on self-reported functional health and proxies of acculturation with biomarkers and an acculturation measure that better characterizes cultural nuances. Our findings are consistent with previous work demonstrating that healthy immigrant advantages may not endure into older age and that acculturation is positively related with health (Crimmins et al., 2007; González et al., 2009). The study supports the acculturation-health hypothesis in that it accounts for a positive relationship between acculturation and health as opposed to a strictly negative and deleterious relationship that would be expected from the prevailing acculturative stress hypothesis. Finally, our findings are consistent with our hypothesis that the acculturation–health relationship is nonlinear over the life course; however, longitudinal information is needed to determine important developmental periods when health can be favorably modified.
To our knowledge, this is the first study to examine the relationship between acculturation and biomarkers associated with a specific health outcome. Our study is consistent with Crimmins and colleagues’ (2007) work showing no healthy immigrant biomarker profile advantages over non-Latino Whites (Crimmins et al., 2007). We extend Crimmins and colleagues’ work by examining the relationship between acculturation and a cluster of biomarkers associated with a specific and well-characterized medical syndrome. In addition, our theoretical framework allows us to test two competing hypotheses on the relationship between acculturation and health. The results support the acculturation-health hypothesis and demonstrate its utility in understanding the complex relationship between acculturation and health in later adulthood.
There is evidence that Latino immigrants lose their health advantages and converge with U.S.-born Latinos after 15 years postmigration (Alderete, Vega, Kolody, & Aguilar-Gaxiola, 2000; Antecol & Bedard, 2006). Those observations suggest that acculturative stress would continuously exert deleterious effects on immigrant health. Beyond 15 years, the long-term acculturation–health relationship is not well known. Our findings suggest that the trajectory of the long-term acculturation–health relationship may deflect positively at some point after 15 years; however, precise determination of when this change or series of changes occur could not be addressed in this work and remains to be studied.
The influential factors affecting changes in the acculturation–health relationship are poorly understood. We hypothesized that those factors enabling better health care access and patient-provider communication would explain the positive association between acculturation and health; however, the health care access enabling factors that we examined herein inadequately explained this relationship (González et al., 2009). Alternatively, the enabling factors accumulated by more acculturated immigrants might not be expected to attenuate the positive relationship between acculturation and health, but compliment it. That is, rather than attenuating the association between acculturation and health, enabling factors would be more likely to potentiate the relationship. The results from this study indicate that enabling factors very modestly attenuated the acculturation–health relationship. This is consistent with previous work and suggests that other factors may be operating to affect the trajectory of the acculturation–health relationship (González et al., 2009). Some influential enabling factors that could have affected the acculturation–health relationship may include a full spectrum of environmental conditions and additional goods and services available to more acculturated older Mexican Americans. Environmental factors may include the individual and family living in healthier and safer neighborhood and less physiological and psychological stress associated with life as an immigrant minority in the United States in perhaps the lowest socioeconomic position. In terms of goods and services, we have demonstrated that patient-provider communication is considered better and health care information (e.g., diabetes awareness and knowledge) is better understood (González, Tarraf, & Vega, 2010; González, Vega, Rodriguez, Tarraf, & Sribney, 2009). In summary, the net benefits of acculturation may confluence with improved socioeconomic position to yield better health among Mexican Americans in the long run. We were not able to address this hypothesis directly in this study. For this to be adequately addressed, prospective cohort data with younger and older may be needed.
We are not suggesting that acculturation is a cure for all ills affecting Mexican Americans. Indeed, acculturation comes at costs to one’s cultural identity and may affect both individuals and families by distancing them from family ties in Mexico. Instead, we posit that in the balance, positive aspects of acculturation may outweigh any negative factors relative to health, particularly in the later years of life when health needs change and are often more apparent. From developmental and public health perspectives, identifying deleterious and protective factors affecting health and important periods where such changes to health are probable may prove valuable in improving health and reducing the disease burden for this important population over the life course.
Study Limitations
There are several caveats to consider when interpreting the results of our study. First, we relied on cross-sectional data, which is not informative about the time-varying factors influencing health. Furthermore, we examined a small set of factors that could influence the acculturation–health relationship and other unexamined factors may be more influential than those selected for this study, such as health behaviors (Singh & Siahpush, 2002). Second, the average age of SALSA participants was relatively young, and it is unclear if our findings would be similar for older Mexican Americans. We did not examine return migration; however, previous work indicates that the influence of return migration is not substantial (Patel, Eschbach, Ray, & Markides, 2004). In addition, the SALSA is a regional study and might not be representative of the Latino population in the United States in general. Finally, missing data on the main outcome and the significant differences in nativity and acculturation between respondents with complete and missing data could have biased our findings. However, considering the fact that foreign-born and less acculturated respondents were more likely to have missing data, we believe that our findings provide conservative estimates on the relationship between acculturation and metabolic syndrome biomarker risk.
Conclusions
Among older Mexican Americans, higher acculturation was associated with lower metabolic syndrome biomarker risk among immigrants, but not U.S.-born older adults. The relationship between acculturation and health is complex and varies over time and by nativity. Understanding the acculturation–health relationship across the life span affords health scientists opportunities of identifying critical developmental periods for improving the public health of this increasingly important segment of the U.S. population.
Footnotes
The contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. All authors had access to study data and gave final approval to submit the manuscript for final publication.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health, National Institute of Mental Health (MH 084994–HMG), National Institute on Aging (AG 12975 and AG 33751–MNH, and the National Heart Lung Blood Institute (HC 65233).