
Abstract
Keywords
Introduction
Boosting cognitive performance has implications for successful cognitive aging and neurodegenerative disease. An Alzheimer’s disease prevention program delaying onset by only 1 year would cut the prevalence by more than a third by 2050 (Brookmeyer, Johnson, Ziegler-Graham, & Arrighi, 2007). In support of the search for such a program, the National Institute of Aging and National Institute of Nursing Research have supported a multisite randomized controlled trial of cognitive training: the ACTIVE study (Advanced Cognitive Training for Vital and Independent Elderly) since 1998. ACTIVE tests the effectiveness of community-based training in three areas of cognitive functioning (logical reasoning, memory, and speed of visual processing) in improving cognitive performance, performance of everyday activities, health-related quality of life, mobility, and health-service utilization (Jobe et al., 2001).
In this article we attempt to characterize the impact of ACTIVE training interventions by evaluating differences between trained and nontrained participants in the slope associated with aging of performance decrements in trained cognitive abilities. Recently, Salthouse (2006) illustrated that the pace of cognitive change over time following the ACTIVE intervention was accelerated for persons who had participated in training. The goal of the current study is to probe this observation. Specifically, we address what Salthouse called the critical question:
The critical question in the current context is therefore not the magnitude, nor the durability, of training effects, but rather the influence of the relevant experience on the rate of change in measures of cognitive functioning over time. (p. 74)
We address this question using multiple group growth curve models that decompose change over time into four distinct sources of change. Two of these are theoretically at work in both the intervention and control groups, include a retest or practice effect and age-related or maturational effect. The practice effect describes gains due to familiarity of the testing situation or content caused by repeat testing. Maturational change describes normal aging-related changes. The remaining three sources of change we characterize are evident in the ACTIVE-trained group only. These include ACTIVE’s symptomatic effect (initial boosting of performance of trained abilities), the pace at which these initial gains are lost with increasing time from the initial training (a loss of training gains effect) and an age modifying effect (altering the trajectory of performance declines with age). The extent that ACTIVE modifies the aging effect is evident from differences in the maturational effect for control and trained participants. Our analytic approach is an extension of latent growth curve models for evaluating randomized trials (Curran & Muthén, 1999; Muthén & Curran, 1997) and longitudinal cognitive performance data (Ferrer, Salthouse, McArdle, Stewart, & Schwartz, 2005; McArdle & Epstein, 1987). Our modeling is a direct test of Salthouse’s challenge.
Most studies of cognitive training are not comparable to ACTIVE for the purpose of evaluating the long-term effect of cognitive training on age trends for cognitive abilities. Smith et al. present the results of the IMPACT (Improvement in Memory with Plasticity-Based Adaptive Cognitive Training), a large randomized controlled two-arm clinical trial of the Brain Fitness Program (Posit Science, San Francisco, CA; Smith et al., 2009). They only report pre- and posttraining differences over a brief time interval. The same is true for Owen et al.’s report on their “Bang Goes the Theory” training (Owen et al., 2010) and Miller et al.’s Memory Fitness Program (Miller et al., 2011). McDougall et al. (2010) report 26-month follow-up from their SeniorWISE memory training program, but do not evaluate training-related differences in aging trends. Several other recently reported trails suffer the same lack of follow-up and/or evaluation of aging trends (Peretz et al., 2011; Pressler et al., 2011; Schmiedek, Lövdén, & Lindenberger, 2010). Perhaps the most relevant data come from observational studies of the effect of lifestyle and background characteristics on aging-related cognitive trends. The evidence for one powerful cross-sectional predictor of cognitive performance—educational attainment—is decidedly pessimistic with regard to benefits on aging-related cognitive trends (Glymour, Tzourio, & Dufouil, 2012) . In conclusion, the field is currently without a good answer to the question: can cognitive training delay the natural course of cognitive aging? Observational studies suffer important methodological limitations and biases (Glymour et al., 2012), and apart from ACTIVE, intervention trials do not have the duration of follow-up to address the question.
Therefore, our goal was to attempt to address the question of how the ACTIVE cognitive training programs influence the pace of cognitive aging. Although the impact of ACTIVE on cognitive performance has been described previously (Willis et al., 2006), previous analyses have restricted attention to total performance over time. Our approach is distinctly different because we attempt to decompose training-related effects into those that reflect immediate training gains, the loss of those training gains as time from training increases, and differences in aging-related trends.
Method
The design of ACTIVE has been described elsewhere (Jobe et al., 2001). Briefly, older adults (aged 65 to 94) were randomly assigned to one of three cognitive training or no contact control arms. Training lasted 5 to 6 weeks, and participants were assessed pre- and postintervention, and at 1, 2, 3, 5, and 10 years after posttest. This analysis considers outcomes through 5 years, as the 10-year main results are currently under analysis.
Participants
From March 1998 to October 1999, participants were enrolled across six field sites. Each field site had a different recruitment strategy. Participants were drawn from motor vehicle license or identification card rolls, clinical patient rolls, elder services rolls, congregate and senior housing sites, senior and community centers, research volunteer registries, churches, and senior citizens organizations (Jobe et al., 2001). Exclusion criteria included age less than 65 years, substantial functional impairment, Mini-Mental State Examination (Folstein, Folstein, & McHugh, 1975) score less than 23, self-reported diagnosis of Alzheimer’s disease, sensory impairment, inability to communicate in spoken English, medical conditions with poor prognosis, and previous participation in cognitive training. As reported by Willis et al. (2006), 67% of the sample was retained through the fifth annual follow-up, and retention was related to age, sex, education, health problems, and baseline cognitive function. Nevertheless, as pointed out by Willis et al. (2006), treatment group did not interact with these covariates and therefore do not affect the assessment of group differences of intervention effects. The protocol and informed consent procedure were approved by local review boards and the trial was monitored by a single Data Safety and Monitoring Board. Characteristics of persons included in our analysis are summarized in Table 1.
Baseline Characteristics of Participants by ACTIVE Intervention Group, Excluding Participants Randomized to Booster Training (N = 1,659).
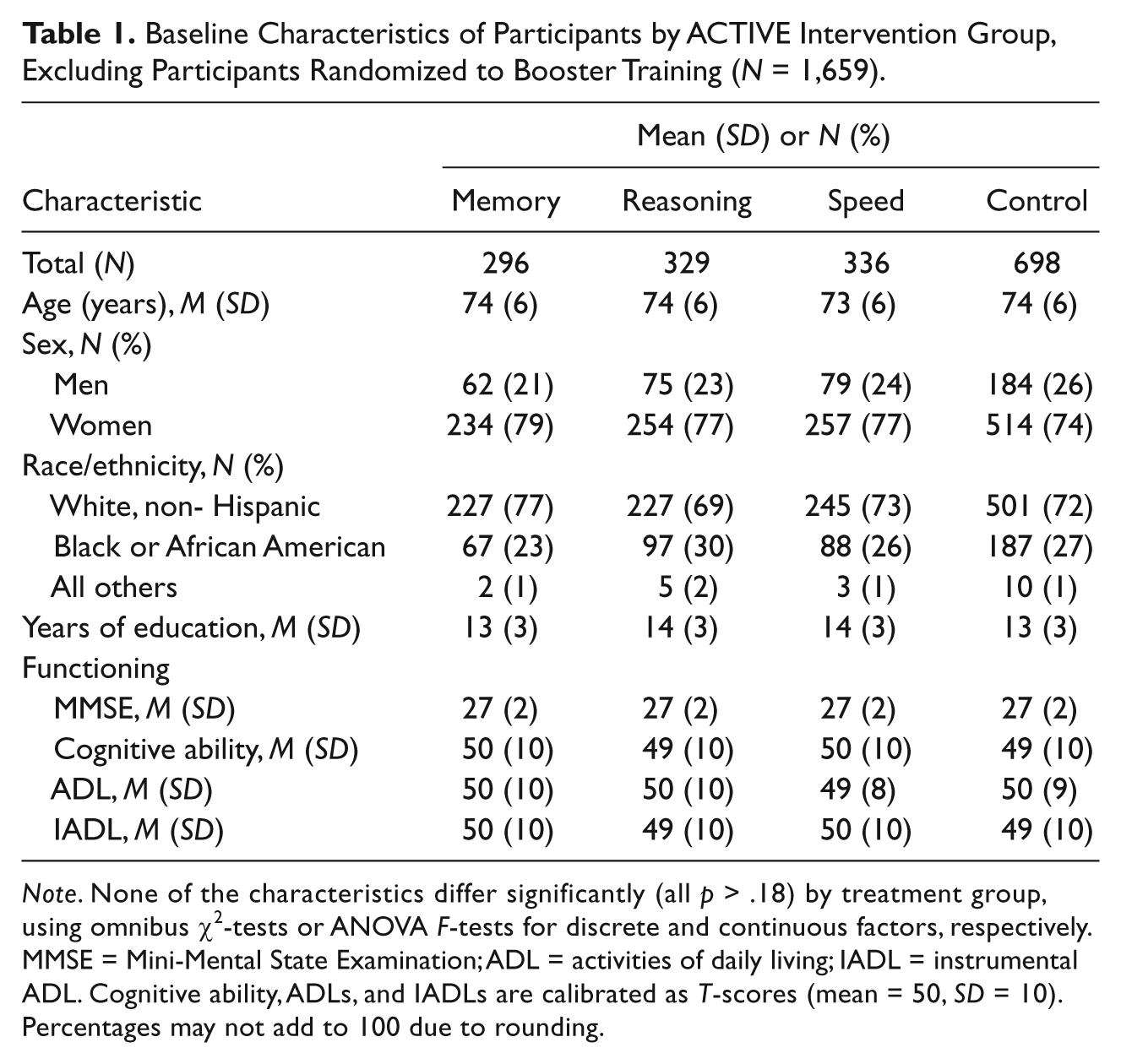
Note. None of the characteristics differ significantly (all p > .18) by treatment group, using omnibus χ2-tests or ANOVA F-tests for discrete and continuous factors, respectively. MMSE = Mini-Mental State Examination; ADL = activities of daily living; IADL = instrumental ADL. Cognitive ability, ADLs, and IADLs are calibrated as T-scores (mean = 50, SD = 10). Percentages may not add to 100 due to rounding.
Interventions
Each of the three training interventions was designed to target a specific cognitive ability—memory, reasoning, or speed of processing (Ball et al., 2002; Jobe et al., 2001). Memory training involved teaching mnemonic strategies for remembering verbal material (Rasmusson, Rebok, Bylsma, & Brandt, 1999; Rebok & Balcerak, 1989). Reasoning training involved strategies for finding the pattern in a letter or word series (Willis, 1987; Willis & Schaie, 1986). Speed of processing training focused on visual search and divided attention (identifying an object on a computer screen at increasingly brief exposures, followed by dividing attention between two search tasks; Ball & Owsley, 2000; Edwards et al., 2002; Roenker, Cissell, Ball, Wadley, & Edwards, 2003). Each training intervention involved 10 sessions. Two booster training interventions, with four sessions of content and structure similar to the initial training, were conducted at about 1 year and 3 years after the initial training. Participants who completed the initial training (having completed 8 of 10 sessions) were considered eligible for booster training, and a 60% random sample was identified and invited for boosters. The flow of participants through various stages and randomization points is illustrated in Figure 1.
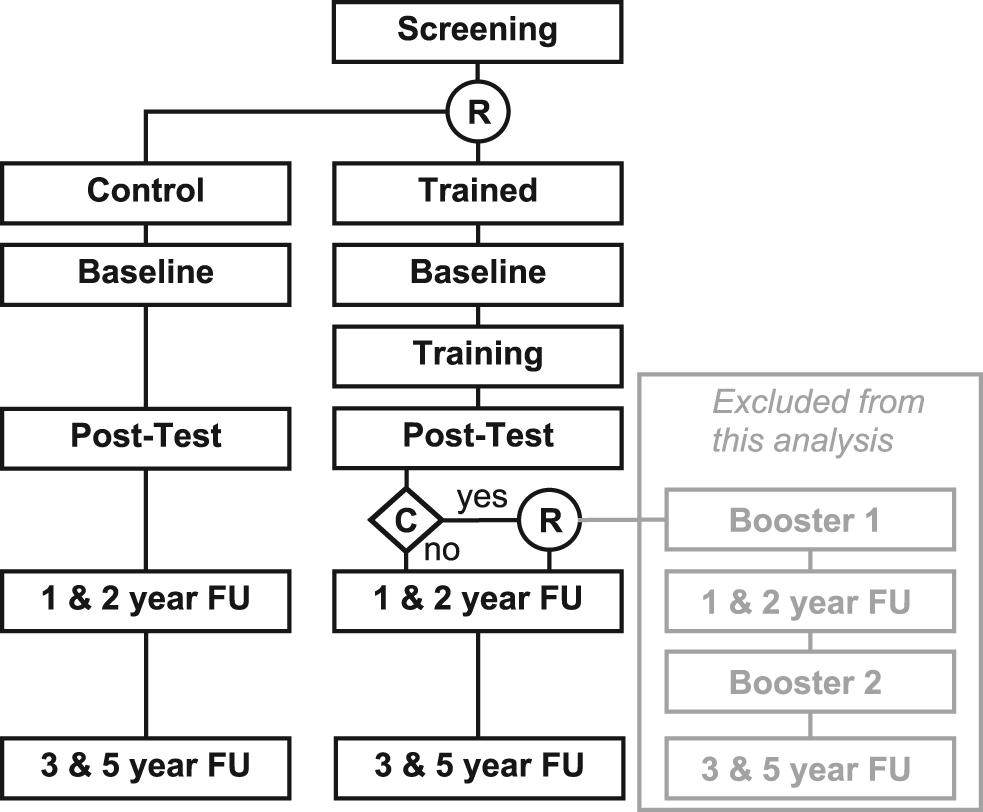
Participant Flow.
Restriction and Weighting of Participants
This analysis considers a subset of the ACTIVE participants. We exclude persons who were randomized to the booster training condition. Booster training represents an interruption into the presumed processes of forgetting initially presented training- and aging-related change. Because persons randomized to booster training had to be compliant with their initial training, the sample of persons who were initially randomized to training but not to booster is overrepresented by persons who were noncompliant with initial training (see Figure 1). We addressed this issue using propensity score methods. We used logistic regression to model compliance among those trained as a function of age (linear and quadratic functions), sex, education (less than 12 years vs. higher), race (Black or African American vs. White and All others vs. White), baseline level of general cognitive ability. General cognitive ability was included as a τ-equivalent factor score (Raykov & Marcoulides, 2000) based on three cognitive abilities: memory, reasoning, and speed (described below) and basic and instrumental daily functioning. We combined this propensity score with a propensity score for attrition over follow-up (using the same covariates) to generate a person-level weight based on the inverse probability of being compliant with initial training and not a drop out (Fewell et al., 2004). This weighting variable was used in our multivariate latent variable models, described below.
Outcome Measures
This analysis considers only the measures of the cognitive abilities targeted by the ACTIVE interventions. The ACTIVE proximal outcomes were chosen as basic cognitive abilities that had some evidence of being modifiable with focused intervention (Jobe et al., 2001).
Memory training outcomes were the Hopkins Verbal Learning Test, Rey Auditory-Verbal Learning Test, and the Rivermead Behavioral Paragraph Recall Test (Brandt, 1991; Rey, 1941; Wilson, Cockburn, & Baddeley, 1985). ACTIVE used parallel but nonequivalent forms for the memory assessment at each repeated observation to reduce retest effects. Because the forms are nonequivalent and no within-wave counterbalancing of alternate forms were used, the scale of the outcome varies across wave. We placed the alternate forms on an equivalent metric using an equipercentile equating procedure (Kolen & Brennan, 1995). An important artifact of this procedure is the removal of retest effects. Reasoning training outcomes were Letter Series, Letter Sets, Word Series (Ekstrom, French, Harman, & Derman, 1976; Gonda & Schaie, 1985; Thurstone & Thurstone, 1949). Speed of processing training outcomes were derived from the Useful Field of View (Ball & Owsley, 1993; Owsley, Ball, Sloane, Roenker, & Bruni, 1991; Owsley et al., 1998).
Following Ball et al. (2002), proximal outcomes were computed as composites and standardized by pooling and Blom-transforming (Blom, 1958) scores at all time points. We further rescaled the outcomes by standardizing to a T-score distribution based on the baseline mean and standard deviation (SD) of the referent age group among control participants (mean of 50 and SD of 10).
Age
Participants were assigned to one of four groups according to age at baseline (65 to 69, 70 to 74, 75 to 79, 80+). However, we retain use of individual time points of observation corresponding to exact years of observation (see time, below). Group indicator variables were centered using ANOVA-type centering following Kraemer and Blasey (2004). This results in an interpretation of modeled means and intercepts as averages over all age groups.
Time
We used each participant’s exact age at time of reassessment centered, at the mid-point of their age group, and divided by 5.23 (the per-protocol length of follow-up), as the time metric.
Control variables
In addition to age group, our analytic models include covariate adjustment for participant sex and race/ethnicity (Black or African American vs. all others). Because ACTIVE was a randomized trial, the treatment groups can be assumed to be equivalent at baseline with regard to observed and unobserved factors. Table 1, and previous work (Ball et al., 2002), supports this assumption.
Analytic Approach
We analyzed each of the three cognitive outcomes separately. We fit a generalization of the growth curve model (McArdle & Epstein, 1987) to multiple groups, where the grouping variable was defined by randomization to treatment arm. Our model includes a random effects growth curve model for performance differences over an age basis, and a latent growth curve on an occasion basis for design effects (treatment, retest). The multiple group approach to the evaluation of intervention studies has been addressed previously (Curran & Muthén, 1999; Muthén & Curran, 1997). A general depiction of the modeling strategy for cognitive outcomes is illustrated in Figure 2. A detailed description of the model parameterization is available in the Appendix.

Representation of the analytic model.
Missing data
Our models use all available information for model estimation. Cases with missing data in the outcome variable are included using maximum likelihood estimation under the assumption that the missing data are missing at random (Little & Rubin, 1987). Thus our missing data modeling strategies include both maximum likelihood methods and a weighting adjustment based on the inverse probability of dropout.
Results
Results are presented in Table 2 and Figure 3. The table summarizes models comparing the ACTIVE participants randomized to the control and training condition for the memory, reasoning, and speed proximal outcomes, respectively. Parameters reflect averages over all age groups and balanced for race/ethnicity and sex. Results are illustrated for the referent age group in Figure 3. Many parameter estimates are not presented (i.e., those in
Growth Model Parameter Estimates.

Note. ACTIVE cognitive intervention study (N = 1,659). All effects reflect control for baseline age group (65 to 69, 70 to 74, 75 to 79, 80 and older), sex, and race/ethnicity. Covariates are centered so that effects represent expected values for a hypothetical cohort balanced by the overall sample distribution of age, sex, and race/ethnicity (Table 1). Reasoning and speed models include weighting adjustment for the inverse probability of being compliant with initial training and completing follow-up, predicted by age, sex, race/ethnicity, education, general cognitive functioning, and ADL and IADL functioning.
p < .05 (p-values refer to test that parameter is equal to 0).
Parameter fixed to indicated value, na = not applicable.
Residual variances of observed dependent variables constrained to be equal over time and across group (results not shown).
Correction factor not estimated using MLF estimator (all other models use MLR estimator).
Comparison of model log-likelihood with correction for scaling factors (Satorra & Bentler, 1994).
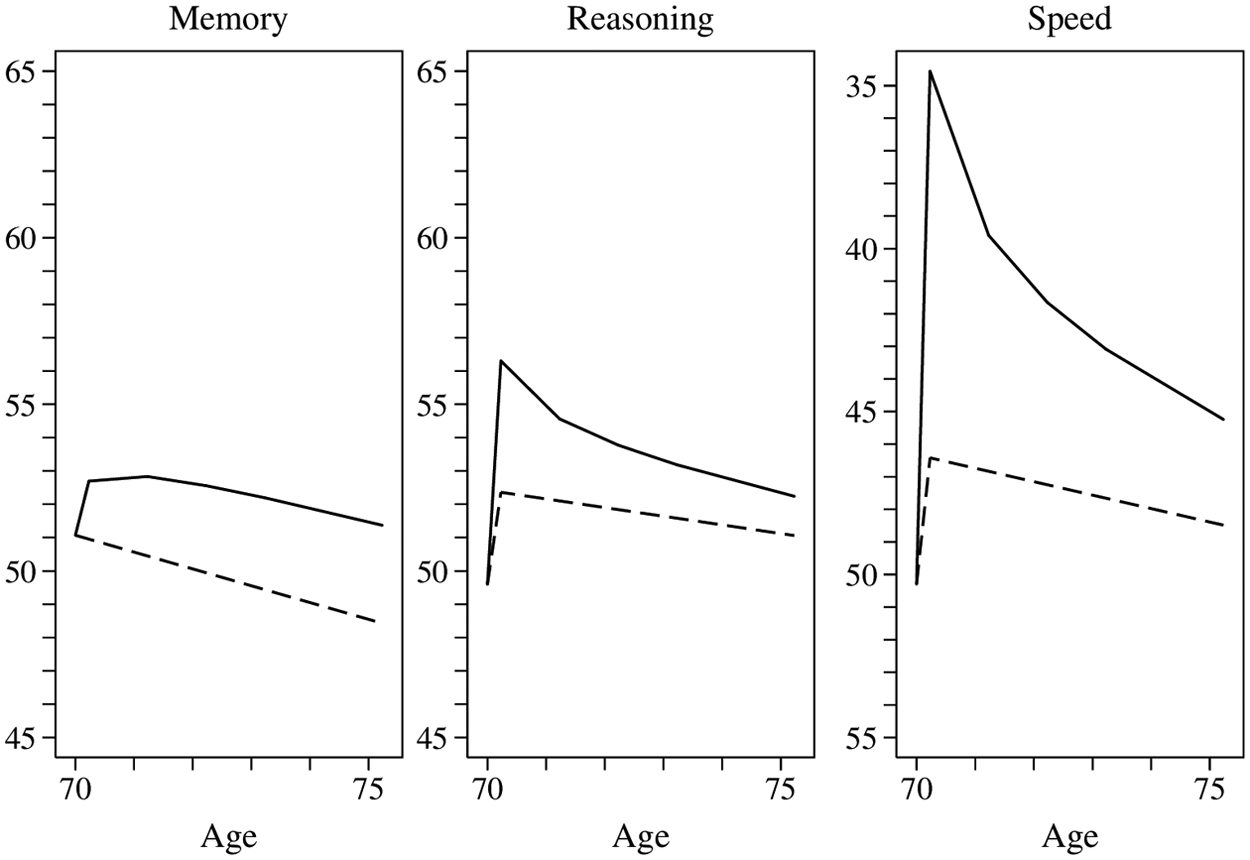
Model Implied Change in Cognitive Performance Over Time Within Four Age Groups by ACTIVE-Trained and Control Groups.
Main Model Results
Memory
Initial attempts to fit the memory model with the robust maximum likelihood (MLR) estimator and complex sampling weights failed to converge and produce standard errors. Convergence was achieved and standard errors were approximated as first-order derivatives of the model fit using the MLF estimator. The MLF estimator does not support complex sampling weights, so the memory models do not incorporate the weighting adjustment for balance of likely compliers and dropout that the other outcome models do. Therefore, the memory models include an overrepresentation of likely compliers among the controls. The implication of this is that the estimates obtained in this analysis can be considered to be biased toward the null.
The estimated memory model fit well (Table 2; overall pseudo r2 = 0.86). The normative age-related change in memory performance was estimated as −.2.5 T-score units over the period of observation (approximately 5.23 years), an effect significantly different from zero (z = parameter estimate/standard error = −8.4, p < .001). This 0.25 SD effect size for age-related change, net of retest and training effects, is assumed to be at work in both groups (control and trained). The retest effect for the memory composite (ηr) is not estimated because it is forced to be 0 due to the equating procedure. Table 2 also lists a model-implied expectation of performance level at the end of the period of observation, which for the control group 48.8.
The initial memory training effect was estimated to be 2.2 T-score units (z = 6.0 p < .001), and the loss of training-related gains was unexpectedly positive (+0.6 T-score units, z = 1.92, p = .54). Thus, memory-trained persons continued to improve beyond initial retest period. Persons trained in memory retained 125% of their initial training-related gains at approximately 5 years after training. The expected treatment effect at the end of the period of observation (i.e., the difference in the model-implied mean memory composite score at the fifth annual assessment for those memory-trained relative to controls) is 2.8, a small effect size in Cohen’s (1988) effect size taxonomy (0.28 SD units).
Reasoning
The reasoning model fit very well (overall pseudo r2 = 0.93; Table 2). Normative age-related change in reasoning performance was −1.4 T-score units over the period of observation, an effect significantly different from 0 (z = −5.5, p < .001), but of trivial to small magnitude. The retest effect for the reasoning composite is small to moderate in magnitude (2.8 T-score units, p < .001). The model-implied expectation of performance level at the end of the period of observation for persons not trained is 50.9. Comparing this to the control group intercept (49.4) reveals that persons who were not trained perform better at about 5.23 years follow-up relative to baseline (+1.5 T-score units), a consequence of a relatively large retest effect and little age-related change.
The initial reasoning training effect was estimated to be 2.8 T-score units (z = 17.7, p < .001); the loss of training-related gains was about half that magnitude (−1.5, z = −7.0, p < .001). Therefore, about 45% of the training-related gains due to reasoning training were retained over the period of follow-up. The expected treatment effect at the end of the period of observation is 1.2, a trivial effect size. Both the control group and reasoning trained group perform at a higher (better) level at the end of the follow-up period relative to baseline. In the case of controls this is because the net retest effect exceeds the net performance decrement associated with aging-related change. The balance of these effects also influence the expected performance in the reasoning trained group, which also shows a net preservation of almost half of initial training-related gains.
Speed
The speed models fit well (Table 2), with an overall pseudo r2 = 0.84. Note that the speed outcome is timed, so lower scores imply better (faster) performance. Normative age-related change was estimated at 2.2 T-score units over the period of observation, an effect that was statistically significant (z = 6.7, p < .001) and of small to moderate magnitude. The retest effect for the speed composite is moderate (−4.0, p < .001). The initial speed training effect was estimated to be −7.8 T-score units (p < .001) and the loss of training-related gains was about half that magnitude (4.6, z = 14.5, p < .001). The expected treatment effect at the end of the period of observation is −3.2 T-score units, a small to moderate effect size. About 41% of initial training-related gains were retained at the end of the observation period.
Differences in Maturational Change
Before considering models that test the difference in the pace of age-related change, we can see that the groups that received training are performing at a level that is more favorable than those of controls at the end of the follow-up period. While we have expressed these differences in T-score units in the previous section, we can also express them in terms of units of age by dividing the mean difference at the end of the follow-up period by the normative per-year change in cognitive ability. Doing so suggests that persons receiving the memory, reasoning, and speed training perform at a level about 5.8, 4.5, and 7.6 years younger than controls, respectively. 1
To test the hypothesis that training changes normative cognitive development, in each of our trained condition-specific models, we relaxed the assumption that age-related change was the same in the trained and nontrained groups. We simultaneously relaxed assumptions on the equivalence of the mean and variance of age-related change, resulting in a two degree of freedom omnibus test of statistical significance, evaluated with change in −2 × Log-likelihood with Satorra–Bentler (1994) correction for scaling factors. For only the memory-trained outcome do we see that the model modification resulted in a statistically significant improvement in model fit (p < .001). For reasoning and speed the improvement was not significant and the adjusted Bayesian Information Criterion (aBIC) favors (i.e., is lower for) the models with normative age factors constrained.
Memory
For memory training, the estimated pace of age-related change in the control group (−2.1 T-score units over 5.23 years) implied slower decline than in the trained group (−6.1). This apparent paradoxical finding is exactly the finding identified by Salthouse (2006). As mentioned above, this model modification was significant (p < .001).
Reasoning
For reasoning training, the estimated pace of age-related change in the control group (−1.4 T-score units over 5.23 years) implied a faster pace of aging than in those trained (−0.9). This aging-related change parameter was not statistically different from 0 (z = −1.3, p = .18), implying that the reasoning trained group, on average, experienced no significant age-related slowing over the period of observation. The relaxed model, however, was not better fitting overall than the constrained model (p = .921) and the aBIC favors the unconstrained model.
Speed
Speed training models, similar to memory training, revealed an estimated pace of age-related change in the control group ( +1.9 T-score units over 5.23 years) implied slower decline than in the trained group (+3.4). We interpret this counter-intuitive result as an indication that strong initial training effects coupled with rapid loss of training-related gains contaminate the estimation of aging-related change. Relative to normative aging-related change, the initial boost in the targeted ability and the loss of training gains was much more pronounced for the speed training than for memory and reasoning. The relaxed model was not better fitting than the constrained model on the basis of the improvement in log-likelihood or information criteria.
Discussion
We used growth curve models to characterize cognitive change after training implemented in the ACTIVE study. We found that the reasoning training significantly slowed reasoning ability changes due to aging. We do not show an effect of slowing aging-related declines in for speed training, and suspect this is due to the extremely powerful initial training effect and intractable confounding of the loss of training gains and maturation. We also do not show a slowing in aging-related change due to memory training.
Our analysis was an attempt to respond directly to Salthouse’s challenge to intervention studies of cognitive aging. In so doing, we were able to confirm that only one of the three ACTIVE training programs (reasoning) attenuates the pace of normal cognitive decline. Our findings repeat his observation that intervention studies (and in fields beyond cognitive aging) often find that training boosts performance but can also appear to accelerate age- or time-related change, because change over time becomes coupled with loss of training gains.
Recently, a 10-year follow-up of the ACTIVE participants has been completed. With these data, we will have more information to characterize loss functions, including identifying loss of booster training gains, which will allow approaching this analysis question with all persons randomized to one of the ACTIVE training arms. The model can be improved as well, and opportunities to do so present themselves when the additional assessment point become available. An additional data point will allow more complex functional forms for the loss of training-related gains, such as modeling a nonlinear function with a lower asymptote. Such a model modification is crucial to our general analytic approach, which relies upon our separating the profile of trainingrelated gains (initial gains and their duration) from aging-related changes. Our models may not do this well for speed and memory training, and more flexible and appropriate modeling strategies (e.g., nonlinear growth models such as structured latent curves models over the assessment occasion basis (Browne & Du Toit, 1991) coupled with piecewise linear random effect growth curve models over an age basis) may be estimable with the additional occasion data from the 10-year analyses.
Our models suggest other significant results. Although we do not demonstrate that memory training attenuates age-related change in memory performance, we do see that the albeit modest initial gains afforded by memory training are maintained at 5 years. Conversely, more than half of the initial gains in reasoning and speed are lost by 5 years. We also found that all of the training interventions attenuate the variance of age-related change in performance in trained abilities. This finding provides encouragement that the additional follow-up of ACTIVE participants will allow more time to pass and changes to accumulate and allow us to better capture the impact of ACTIVE training on change related to aging.
Limitations of this work are worth mentioning. First, as implied in our results, the 5-year follow-up period has not been sufficient to adequately characterize the effects of the ACTIVE intervention, both in terms of partialling out different aspects of the training effect (patterns of gains and maintenance for initial and booster training) and in characterizing effects on maturational change. This limitation has two further aspects. One is that as an initially healthy and cognitively intact sample of older adults, few ACTIVE participants are likely to have experienced clinically meaningful cognitive decline over 5 years. The other is that not enough time has passed to adequately characterize the magnitude and sources of change in cognitive abilities due to ACTIVE training. This is why we are forced to exclude booster participants from this analysis. To include them, we would need additional follow-up in order to identify the initial gains related to booster training and the subsequent loss of this effect.
Other forms of bias may be at work in the ACTIVE study and in our analysis. ACTIVE can best be described as a sample of convenience. The results observed may not translate to representative samples drawn from community-based populations. Characteristics of persons that cause them to be willing to participate in a long-term trial of cognitive training may influence the extent to which they are receptive to the effects of training. The detection of differences in aging-related cognitive change may be particularly challenging in ACTIVE if it is true that increasing age is associated with accelerated cognitive decline given a single eligibility threshold for baseline cognitive performance was used.
Conclusion
Our results suggest that the ACTIVE reasoning training program may slow the pace of cognitive aging, and that memory trains gains are, on average, not lost over about 5 years. Regardless, the level of performance of groups receiving the intervention are more favorable than those of controls: persons receiving the memory, reasoning, and speed training perform at a level about 6, 4, and 8 years younger than controls, respectively.
Footnotes
Appendix
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Nursing Research, National Institute on Aging, or the National Institutes of Health. Representatives of the funding agency have been involved in the review of the manuscript but not directly involved in the collection, management, analysis, or interpretation of the data.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Rebok is a consultant for Compact Disc Incorporated (CDI), which is at this time in the process of developing an electronic version of the ACTIVE memory training program. He has received no financial support from them for ACTIVE, and the relationship is managed by the Johns Hopkins University according to its established conflict of interest policies. Dr. Marsiske has received support from Posit Science in the form of site licenses for the Insight program for a different research project. Dr. Ball owns stock in the Visual Awareness Research Group (formerly Visual Awareness, Inc.), and Posit Science, Inc., the companies that market the Useful Field of View Test and speed of processing training software (now called Insight). Posit Science acquired Visual Awareness, and Dr. Ball continues to collaborate on the design and testing of these assessments and training programs as a member of the Posit Science Scientific Advisory Board.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was supported in part by the Harvard Older Americans Independence (Pepper) Center (P60AG008812). ACTIVE is supported by grants from the National Institute on Aging and the National Institute of Nursing Research to Hebrew Senior Life (U01NR04507), Indiana University School of Medicine (U01NR04508), Johns Hopkins University (U01AG14260), New England Research Institutes (U01AG14282), Pennsylvania State University (U01AG14263), University of Alabama at Birmingham (U01AG14289), University of Florida (U01AG14276).