
Abstract
Keywords
Introduction
The protective and therapeutic health benefits associated with physical activity in the older adult population, particularly engagement in walking behavior, have been extensively documented (Chodzko-Zajko et al., 2009; Taylor et al., 2004). Even among older adults with poor lower-body capacity, exercise is known to incur benefits in physical functioning in the form of improved balance, muscle strength, aerobic power, endurance, and mobility (McAuley & Katula, 1998; O’Connor, Aechenbacher, & Dishman, 1993; Rejeski & Mihalko, 2001). Physical inactivity has been linked to functional limitations and impairments, disability, and increased risk for the development of chronic illnesses such as coronary heart disease, cancer, diabetes, hypertension, and bone and joint disease (e.g., osteoporosis and osteoarthritis; Bouchard, Shepard, & Stevens, 1994; Warbuton, Nicol, & Bredin, 2006). In addition to enhancing physical health, regular engagement in exercise behavior produces numerous mental health benefits as evidenced by the outcome measures of depression, anxiety, positive/negative mood states, and health-related quality of life (McAuley & Katula, 1998; O’Connor et al., 1993; Taylor et al., 2004).
Although much of the empirical evidence derives from samples of older non-Latino white adults, the limited available evidence suggests similar positive health enhancing effects of regular exercise among older Latino adults. Unfortunately, there is indication of racial/ethnic disparities in exercise adherence as this growing ethnic minority subgroup reports the least amount of leisure time physical activity (LTPA; Crespo, Keteyian, Heath, & Sempos, 1996; August & Sorkin, 2010). Reports document the highest rates of nonengagement in LTPA among Mexican American men (33%) and women (46%; Crespo et al., 1996). Older non-Latino white adults between the ages of 70 to 79 are more physically active than Mexican Americans across all age groups (Anderson, Franckowiak, Christmas, Walston & Crespo, 2001). Across a spectrum of body mass index (BMI) categories, seniors belonging to a racial/ethnic minority group, specifically those of Mexican American and African American descent, report higher rates of no LTPA when compared to their non-Latino white counterparts (Anderson et al., 2001). Indeed, rates of regular physical activity are reported to be as low as 10% among older Latino adults. While there are a number of factors that serve as antecedents to physical activity nonadherence in the Latino community, issues relating to mental health may contribute to this disparity.
A construct that has increasingly received more attention in terms of its impact and consequence on physical activity participation rates is the psychological correlate of depression. Older Latinos are disproportionately at risk for depression with reported prevalence rates as high as 25.6% among the Latino subpopulation (Black, Markides, & Miller, 1998). Furthermore, Mexican American seniors with lower levels of acculturation display an elevated risk for depression when compared to their more acculturated or U.S.-born counterparts (Gonzalez, Haan, & Hinton, 2001). Accompanying these estimates of a higher prevalence rate, older Latino adults are less likely to receive proper mental health services (Robins, Locke, & Regier, 1991; Unutzer et al., 2003) as socioeconomic and cultural factors (e.g., stigma associated with mental illness) often serve as deterrents for seeking mental health services. As will be discussed below, this unmet mental health need, as experienced by minority older adults, may offer insight into the high rates of sedentarism.
There are two competing theories guiding the depression research in the context of physical activity. The first suggests that symptoms of depression precede sedentarism, in other words, negative psychosocial responses in the form of depressive symptomatology serve as antecedents or causal factors in the deterioration of physical activity levels (Roshanaei-Moghaddam, Katon, & Russo, 2009). The second argues that depression develops as a consequence of physical inactivity (Perrino, Mason, Brown, & Szapocznik, 2010). Most literature on this topic makes use of the latter theory known as the consequence model, which hypothesizes physical inactivity to be a risk factor for the development of depressive symptomatology, acting via social, cognitive, and neurobiological pathways (Rehor, Dunnagan, Stewart, & Cooley, 2001; Russo-Neustadt, Beard, Huang, & Cotman, 2000). After controlling for relevant covariates (e.g., age, medical problems, negative life events, etc.) and despite methodological incongruence, cross-sectional studies have consistently revealed an inverse relationship between depression and physical activity (Dunn, Trivedi, & O’Neal, 2001). Longitudinal studies show a protective effect against development of depressive symptomatology among physically active older adults (Strawbridge, Deleger, Roberts, & Kaplan, 2002; Teychenne, Ball, & Salmon, 2008). Although a recent meta-analysis suggests only short-term effects, there is mounting evidence using meta-analytic and experimental techniques establishing the antidepressant effect of physical activity among individuals with mild to moderate major depressive disorder (MDD; Blumenthal et al., 1999; Dunn, Trivedi, Kampert, Clark, & Chambliss, 2005; Krogh, Nordentoft, Sterne, & Lawlor, 2011), that is, physical activity may be an effective treatment option for major depression. Once again, and as noted in the literature examining the physical benefits of exercise, the evidence on the protective and therapeutic effects of exercise against symptoms of depression are predominantly derived from samples of non-Latino white older adults.
The understudied and competing theory, one that changes the directionality of association, proposes that depression may precede physical inactivity as a result of the affective symptoms associated with a depressive state (e.g., fatigue and decreased energy). Roshanaei-Moghaddam et al. (2009) published a review of the literature presenting the current state of knowledge on the longitudinal effects of depression on exercise adherence. Based on the eleven studies that met inclusion criteria, the authors conclude that the there is sufficient evidence linking baseline depression to sedentarism and diminished levels of physical activity across time. It should be noted that of the eleven studies included in the review, only one had participants of Latino descent. Also, this literature review did not include Perrino et al. (2010) who, using a cross-lagged panel analysis with a sample of older Latino adults (n = 273), found baseline depression levels to be predictive of low walking levels at 30 months. What may be concluded from these longitudinal studies is that baseline depression is detrimental and may diminish levels of engagement in exercise behavior across time, but intervention studies may suggest an alternative.
To our knowledge, research on the prospective effects of depression on exercise adherence levels is virtually nonexistent in the context of exercise interventions, particularly among minorities and older adults with low socioeconomic status. In one of the few studies on this topic, Nguyen, Koepsell, Unutzer, Larson, & LoGerfo (2008) examined participation rates, attrition, and patterns of participation in a physical activity program among older adults with depression. Older adults with depression were just as likely to join the health plan-sponsored physical activity program when compared to nondepressed members, but they were at greater risk for attrition over the 2-year time span. Despite knowledge that older adults with depression have higher attrition rates after enrolling in exercise programs, studies have not looked at the potential moderating effect of depression when examining the effects of an exercise intervention on physical activity level, particularly among older Latino adults.
To examine this new question, the primary aims of the current study are to (a) examine the relationship between depression and physical activity levels in a sample of community-dwelling older Latino adults, and (b) to examine whether individuals with baseline depression are less likely to increase physical activity levels during subsequent follow-up measurements (1-, 12-, 24-months) after enrollment in an exercise intervention. Given the potential for differential study attrition and the implication this presents when examining the impact of depression on future exercise participation levels, the current study also examines the factors influencing differential study dropout and the variables associated with retention among older Latino adults with self-reported baseline depression.
In addition to depression (the main independent variable of interest in the current study), comprehensive reviews have identified multiple sociodemographic, biopsychosocial, and environmental correlates that may obscure the association between physical activity and symptoms of depression. For instance, socioeconomic status has consistently shown a positive relationship with physical activity level (Sallis & Owen, 1999). Men reportedly have higher participation rates in leisure time physical activity when compared to women. In terms of psychosocial variables, in addition to the most widely studied individual-level construct of self-efficacy, additional variables associated with physical activity include factors such as social support, perceived physical activity outcomes, and so forth. (Trost, Owen, Bauman, Sallis, & Brown, 2002). The built environment also influences individual engagement in exercise behavior as characteristics associated with neighborhood aesthetics, safety, and land use, among others, may act to enhance or deter engagement in physical activity (Mier, Medina, & Ory, 2007; Taylor, Leslie, Plotnikoff, Owen, & Spence, 2008). Indeed, Satariano et al. (2010) found that seniors living in residential areas have significantly less engagement in walking behavior when compared to those living in mixed-use or commercial areas. Finally, individual health status (e.g., visual, cognitive, and physical impairments) may serve as an obstacle to the performance of physical activity. Thus, the present study considers the longitudinal role of depression on exercise adherence within the context of multiple sociodemographic, health status, psychosocial, and environmental factors in older Latino adults enrolled in an exercise intervention.
Method
Study Population and Data Source
The dataset for the current study (n = 572) comes from a randomized controlled trial (RCT) conducted between August 2005 and 2009, whose aim was to examine the efficacy of a theoretically grounded standardized exercise intervention (¡Caminemos!) on subsequent physical activity levels as measured through self-report and pedometer data (Sarkisian, Weiner, Davis, & Prohaska, 2007). The analyses for this manuscript were based on baseline, 1-month, 12-month and 24-month in-person interview and pedometer data collected from Latinos aged ≥60 years participating in the exercise intervention (¡Caminemos!). Participants were recruited and enrolled at 27 senior centers in the greater Los Angeles region. Inclusion criteria for the study participants were as follows: Latino descent, aged 60 years or older, fluent and able to communicate in English or Spanish, and sufficient cognitive functioning (measured via a 6-item cognitive screening test; Callahan, Unverzagt, Hui, Perkins, & Hendrie, 2002). Participants were excluded if they were already participating in 20 minutes or more of physical activity at least 3 days a week.
Eligible participants were randomly assigned to either the intervention group—consisting of 4-weekly 1-hour group sessions teaching attribution retraining techniques to raise expectations for aging—or the control group who instead received 4 weekly 1-hour health education lectures. As part of attribution retraining, participants were taught that sedenterism is not an inevitable consequence of aging and that older adults should attribute being sedentary to modifiable attributes rather than old age. After attending their randomly assigned 1-hour group sessions (i.e., attribution retraining vs. health education), participants in both arms of the study participated in a 1-hour exercise class taught by a certified instructor. Therefore, the study arms were as follows: (a; intervention arm) receiving the group-based “attribution retraining” sessions and a 1-hour exercise class; (b; control arm) receiving a series of health education lectures and a 1-hour exercise class (with same frequency as the intervention group). The exercise classes were a modified version of the Lifetime Fitness Program© (now called EnhanceFitness®) administered by Senior Services (Seattle), which include strength, endurance, balance and flexibility exercises, and is designed to be safe for seniors with a wide range of physical abilities. The 4-week core program was followed by monthly reinforcement sessions for 11 additional months, and sessions every 2 months for the following 12 months (total intervention duration = 24 months). Both the intervention and the control groups received equal amounts of contact from study staff. Approval for the study was obtained through the University of California Los Angeles Institutional Review Board (IRB).
Measures
All survey data including participant socio-demographic, behavioral, psychosocial, and health-related information was collected using in-person interviews conducted by trained bilingual staff. Described below are the measurement tools used in the current study. Measurement instruments previously published in the Spanish language appropriate for Latinos of Mexican and Central American origin that demonstrated acceptable reliability and validity were used in their published forms. Instruments for which there was not a previously tested published Spanish version were front and back translated by a certified translator. In terms of organization of this section of the manuscript, the outcome variable(s) of physical activity (i.e., Yale Physical Activity Survey and pedometer data) are described first. This is followed by a description of the 5-item depression measurement tool, the main independent variable of interest, and the biopsychosocial covariates.
Outcome Variable(s)
Physical activity and walking level
Physical activity was measured using the Yale Physical Activity Survey (YPAS) and pedometer data. Capturing an assortment of behaviors at varying intensity levels, the YPAS is a 40-item instrument used to assess household, exercise, and recreational components of physical activity in older adults (Dipietro, Caspersen, Ostfeld, & Nadel, 1993; Pennathur, Magham, Contreras, & Dowling, 2004). The survey tool captures three summary indices: (a) Total Time Summary Index (TTSI), (b) Energy Expenditure Summary Index (EESI), and (c) the Activity Dimensions Summary Score (ADSS). Psychometric testing of the YPAS in previous studies revealed adequate test-retest reliability with correlation coefficients in the range of 0.42 (p = 0.0002) to 0.65 (p = 0.0001) and acceptable construct validity when correlated to multiple physiological variables associated with regular engagement in physical activity (e.g., estimated VO2max, percent body fat, etc). The Spanish-version YPAS was found to have moderate to good 2-week test-retest reliability with correlations coefficients ranging from 0.424 (p<0.05) to 0.789 (p<0.01) among older Mexican American adults (Pennathur et al., 2004).
Walking level, measured via vertical acceleration, was captured using the Digiwalker (Yamax DW-500, New Lifestyle, Inc., Kansas City, MO) pedometer whose reported accuracy is within 3% of direct observation. Participants were asked to wear the small electronic pedometer over the hip at waist level at all times with the exclusion of periods associated with sleep, bathing, or swimming. Using computerized downloading methods, research staff documented the number of steps over the previous week as recorded by the digital pedometer at baseline, 1-, 12-, and 24-months. Specifically, the pedometer was worn for a full week (i.e., 7 days) at five different time points during the exercise and attribution retraining program, such that at the baseline, 1-, 12-, and 24- month assessment periods the number of steps over the previous week were recorded.
Predictor Variable
Depressive symptoms
The construct of depression was assessed using the 5-item Geriatric Depression Scale (GDS; Hoyl et al., 1999). The GDS has shown to be an effective screener for depression among frail community-dwelling older adults as it does not rely on somatic symptomatology which have been shown to be more appropriate for younger populations (i.e., pessimism about the future, weight loss). The 5-item scale consists of dichotomous (yes/no) response options to questions such as, “Are you basically satisfied with your life?” The GDS has good convergent validity with clinical diagnosis of depression as it has a sensitivity of 0.97 and a specificity of 0.85. Those endorsing two or more items on the GDS were classified as screening positive for depression.
Covariates
Additional independent variables known to be associated with physical activity and walking behavior were included as covariates, including sociodemographic characteristics, health status measures, psychosocial factors, and neighborhood characteristics.
Sociodemographic factors
The sociodemographic factors assessed were age, gender, education, income, marital status, years of residency in the United States, and acculturation. Borrowing items from the original Acculturation Scale developed by Marin, Sabogal, Marin, Otero-Sabogal, & Perez-Stable (1987), acculturation was measured using a 5-items scale inquiring about language use.
Medical comorbidities
A self-report questionnaire, modeled after the Charlson comorbidity index, was used to capture medical comorbidities (Katz, Chang, Sangh, Fossel, & Bates, 1996). Participants were asked whether they had any of the following medical conditions: high blood pressure, heart attack, congestive heart failure, stroke, diabetes, arthritis, hip fracture, fracture of wrist, arm or spine, lung disease (e.g., asthma, emphysema, etc.), liver disease, cancer, Parkinson’s disease, Alzheimer’s disease or dementia, and anxiety disorder.
Sensory impairments
Two items, with dichotomous yes–no response choices, were used to capture visual and hearing difficulties. Using dichotomous response options (i.e., 1 = Yes and 2 = No), participants were asked to report any visual difficulty (i.e., can’t see normally even with glasses) or hearing difficulty (i.e., can’t hear normally) experienced within the past four weeks.
Cognitive health
The Modified Mini-Mental State (3MS) examination was used to measure cognitive functioning. The 3MS is a modified version of the Mini-Mental State (MMS) examination. Along with measuring a wider range of cognitive functions and difficulty levels, the 3MS has greater sensitivity when differentiating among dementia patients (Teng & Chui, 1987).
Neighborhood environment
Neighborhood characteristics were captured using a shortened version of the Neighborhood Environment Walkability Scale (NEWS; Saelens, Sallis, Black, & Chen, 2002). The selected subscales capture the presence of walking facilities (e.g., presence of sidewalks), neighborhood aesthetics, pedestrian/traffic safety, and crime safety as they relate to the neighborhood surroundings. A 5-point Likert-type scale, ranging from “strongly agree” to “strongly disagree”, is used to rate statements such as, “There are many interesting things to look at while walking in my neighborhood.”
Social support for physical activity
An 18-item instrument was used to measure social support for physical activity. Using a Likert-type response scale ranging from “none” to “very often,” the participants were asked to self-report the frequency of exercise-specific social support received from family and friends. The scale included 15-items as originally developed by Sallis, Grossman, Pinski, Patterson, & Nader, (1987), with the addition of three items developed by the “¡Caminemos!” research team (i.e., During the past 3 months my family, friends, or both (a) made plans without considering my exercise schedule; (b) worried that I may hurt myself by exercising; and (c) told me I am too old to exercise).
Intrinsic religiosity and religious affiliation
Religiosity and spiritual practices were captured using items from the Systems of Belief Inventory (SBI-54; Holland et al., 1999). Participants were asked to provide a spiritual self-rating (e.g., “Religion is important in my everyday life”), and to self-report their religious affiliation (e.g., Catholic, Jewish, etc.)
Efficacy for physical activity
The Social Cognitive Theory (SCT) constructs of outcome expectancy and self-efficacy, as they relate to the performance of physical activity, were measured using previously validated instruments. The Outcome Expectations for Exercise Scale (OEE) is an 8-item survey instrument designed specifically for older adults (Resnick, Zimmerman, Orwig, Furstenberg, & Magaziner, 2000). Psychometric testing reveals adequate construct and criterion validity, internal consistency (Cronbach α of 0.87-0.89), and reliability. Respondents are asked to rate statements such as, “Exercise makes me feel better physically,” on a 5-point Likert-type scale ranging from “strongly agree” to “strongly disagree”. A modified version of McAuley’s exercise self-efficacy measure, shortened and specifically adapted to capture walking behavior, was used to capture individual confidence in the engagement of walking behavior (McAuley, 1993).
Fear of falling
A shortened version of the Tinetti Fear of Falling Scale was used to capture an individual’s self-efficacy in performing daily tasks (e.g., taking a bath or shower) without falling (Tinetti & Powell, 1993). It is a self-report survey tool with higher scores indicating lower confidence in performing daily activities with fall avoidance. Psychometric testing has revealed adequate validity and reliability (test-retest, r = 0.71).
Statistical Method
Data analysis was performed through the use of statistical software (SAS 9.1 for Windows; SAS, Inc, Cary, North Carolina). Descriptive statistics summarizing baseline characteristics for the total sample, and stratified by depression status, are reported for the sociodemographic and physical activity variables (i.e., pedometer 7 day average and the Yale Physical Activity Survey); these are presented as frequencies, percentages, and means as appropriate. T-tests and chi-square tests were also performed to identify between-group differences across the sociodemographic variables for the depressed and nondepressed subgroups.
Bivariate analyses were conducted between each physical activity measure and baseline depression status. Next, simple linear regressions were performed separately for the dependent variables of physical activity (i.e., pedometer data and YPAS subscales) with depression status as the independent binary variable. This was followed by stepwise model selection procedures to produce a parsimonious model for the purposes of running an adjusted model examining the main effects of depression status after controlling for relevant covariates. The stepwise selection technique consisted of multiple forward selection and backward elimination procedures as automated by SAS software using a conservative inclusion and exclusion p-value criteria of 0.15. Control variables included in the stepwise model selection procedure were as follows: age, gender, education, income, marital status, years in United States, acculturation, medical comorbidities, visual/hearing difficulty, cognitive fxn-global, incontinence, NEWS-environment-neighborhood, social support for physical activity, intrinsic religiosity and religious affiliation, outcome expectations for exercise scale, Tinnetti fear of falling scale, and exercise self-efficacy. Box-cox transformations procedures were used to normalize the physical activity outcome variables before fitting the regression models. Finally, only covariates with p-values ≤ 0.15 as identified in the stepwise selection procedure were included in the final regression models.
Next, generalized estimating equations (GEE) were used to examine change in physical activity across time to identify significant differences by baseline depressions status. GEE methods were used separately for each of the physical activity measures (i.e., pedometer data and YPAS subscales) to estimate the contrast between depressed and nondepressed subgroups at 1-, 12-, and 24-months. Due to the differences in physical activity level between the depressed and nondepressed subgroups, baseline values were subtracted from each follow-up estimate. Both an unadjusted model and adjusted model were constructed. The adjusted model controlled for sociodemographic characteristics, health status measures, psychosocial factors, and neighborhood characteristics.
Although GEE is the preferred statistical method for longitudinal data analysis as it uses all non-missing pairs of data in the estimates, it does have limitations. Thus multiple retention analyses were also conducted, as differential program attrition by depressions status was possible. First, the Log-Rank test was used to identify the factors associated with overall program attrition. As, differences in program retention were observed by depression status, further retention analyses were performed to examine the predictors of attrition among those with baseline depression. Eleven factors were used when examining attrition in the depressed subgroup, these included age, gender, education status, annual income, marital status, BMI, disability as measured via activities of daily living, medical comorbidities, environmental/neighborhood characteristics, and social support for physical activity.
Results
Table 1 presents the baseline characteristics for the total sample of older Latino adults (n = 572), along with a stratified summary by depression status. The sample was majority female (77.1%) and ranged in age from 60 to 93 years (M = 73.7, SD = 6.8). This subpopulation was prominently of low socioeconomic status. Overall, 59.3% had less than or equal to an 8th grade education, of which 14.5% had no formal schooling. Slightly over 80% of the older adults had incomes below US$20,000 with 17.0% reporting income below US$5,000. A total of 164 older Latino adults (28.8%) self-identified as married, this was followed by widowed (36.1%), separated/divorced (22.5%), and never married (12.6%). The majority were residing alone (36.2%), followed by living with spouse (30.2%) and friends/relatives (31.1%). Most participants were Catholic (85%). Compared to those without depression, bivariate analyses revealed that older adults classified as depressed were more likely to report low levels of income (p = 0.005) and education (p = 0.034), self-identify as never married (p = 0.009), and exhibit lower acculturation levels as measured via length of US residency (p = 0.039).
Baseline Characteristics of the Study Sample, by Depression Status.
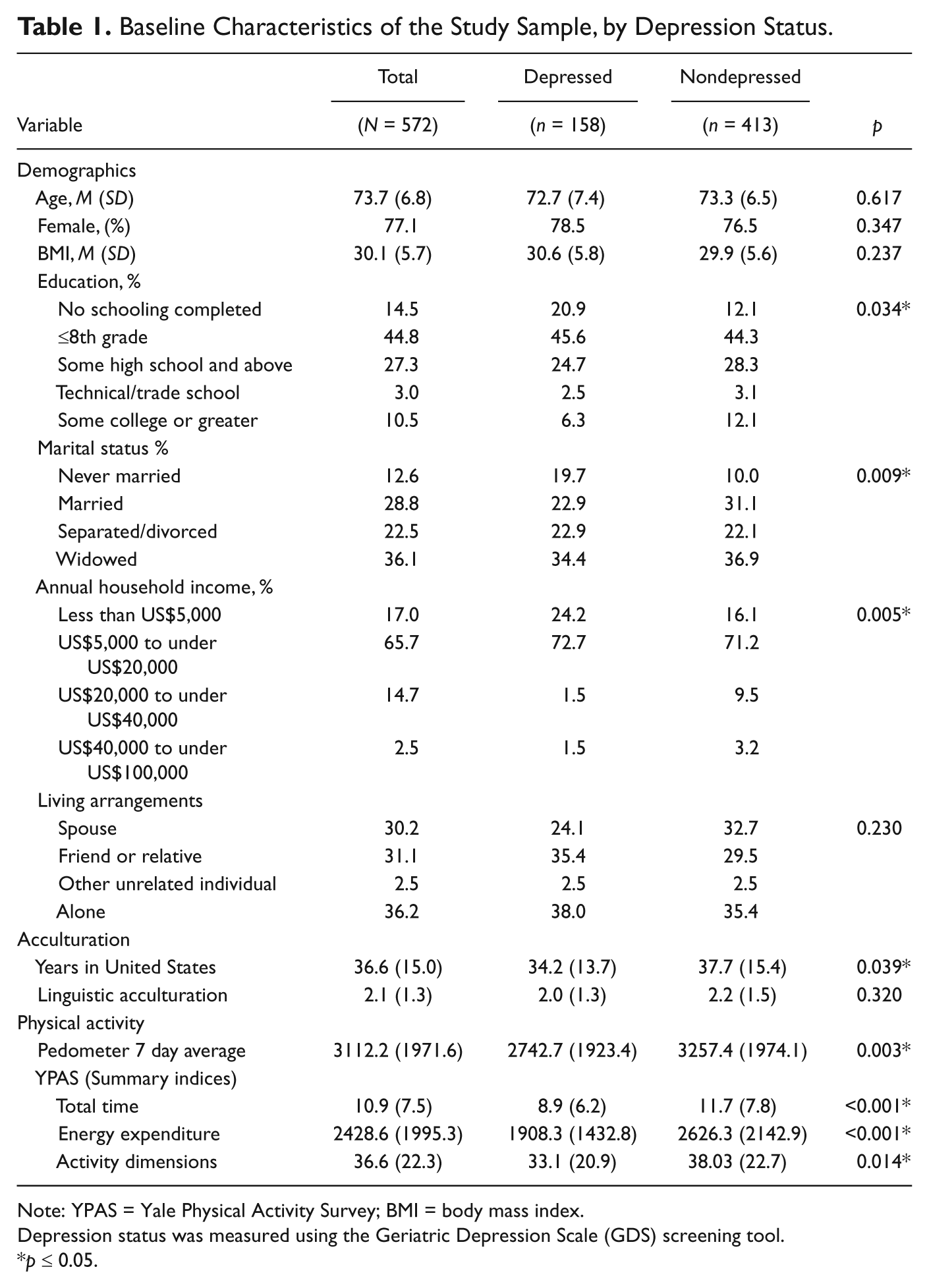
Note: YPAS = Yale Physical Activity Survey; BMI = body mass index.
Depression status was measured using the Geriatric Depression Scale (GDS) screening tool.
p ≤ 0.05.
Baseline data indicates that 27.6% screened positive for depressive symptomatology as measured by the GDS. As hypothesized, across all measures of physical activity, bivariate analyses indicate higher physical activity scores for the nondepressed subgroup (Table 1). Specifically, when using continuous pedometer data as the outcome of interest, depressed individuals recorded 515 fewer steps per day over the previous week when compared to their nondepressed counterparts (2743 steps/day vs. 3257 steps/day; p = 0.003); this represents an approximate difference of 0.2 miles per day. Those with depression also had significantly lower scores on all three summary indices of the YPAS; Total Time (p<0.001), Energy Expenditure (p<0.001), and Activity Dimensions (p = 0.014).
Using linear regression, Table 2 provides the relationship between baseline depression status and all measures of physical activity at the bivariate and multivariate level; the multivariate regression model controls for sociodemographic characteristics, health status measures, psychosocial factors, and neighborhood characteristics (NEWS). At the bivariate level, older adults with depression demonstrated significantly lower walking and physical activity levels at baseline. After controlling for relevant covariates, depression status remained significantly correlated with three of the four physical activity measures (i.e., pedometer data, Total Time Summary Index, and Energy Expenditure Summary Index).
Parameter Estimates for the Cross-Sectional Regression Models of Baseline Data Fitted With Transformed Outcomes.
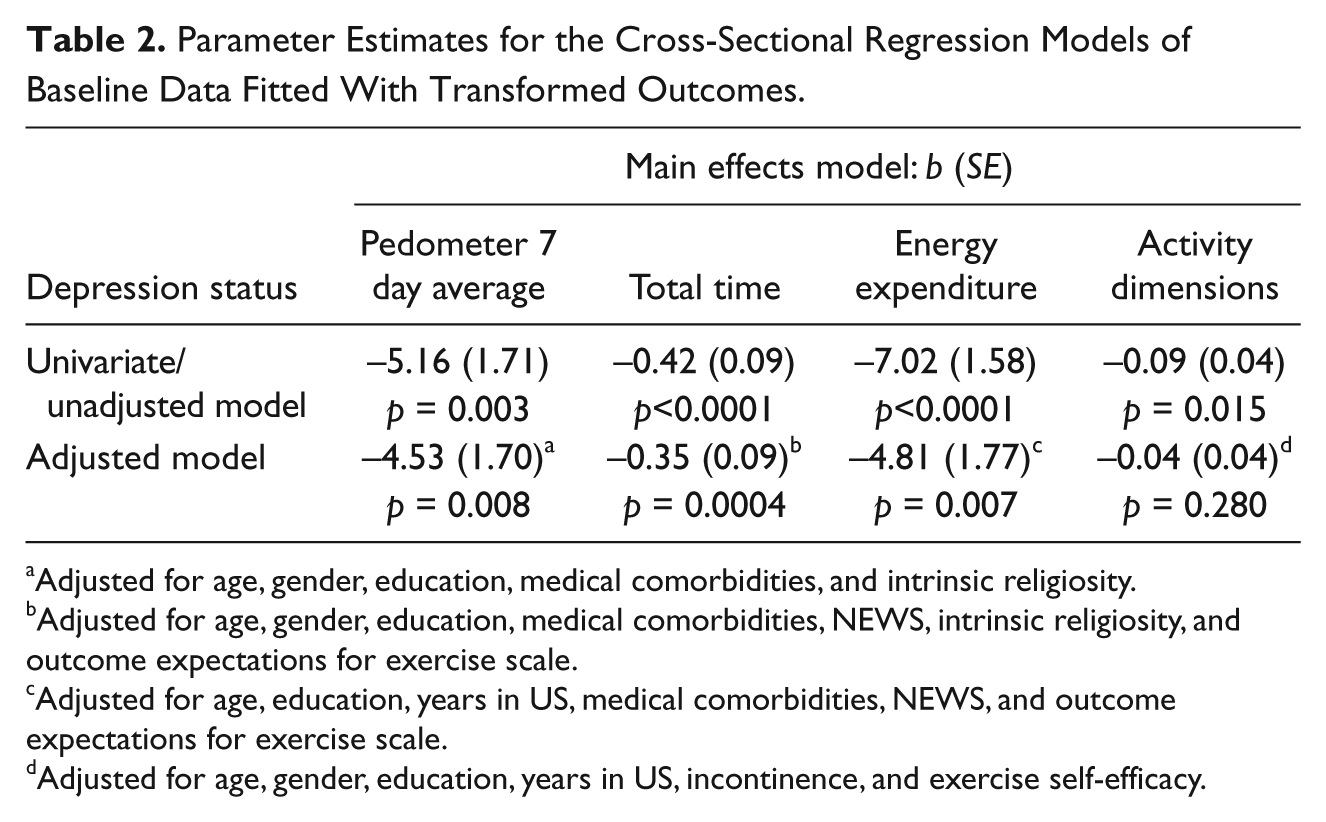
Adjusted for age, gender, education, medical comorbidities, and intrinsic religiosity.
Adjusted for age, gender, education, medical comorbidities, NEWS, intrinsic religiosity, and outcome expectations for exercise scale.
Adjusted for age, education, years in US, medical comorbidities, NEWS, and outcome expectations for exercise scale.
Adjusted for age, gender, education, years in US, incontinence, and exercise self-efficacy.
Longitudinal results of physical activity at 1-, 12-, and 24-months using GEE analysis are presented in Table 3. Significant between-group differences in the change-scores for the baseline depressed and nondepressed subgroups were not evident for any of the physical activity measures. Specifically, pedometer data and summary indices of the YPAS show no difference in physical activity level between depressed and nondepressed at any of the follow-up time points (i.e., 1-, 12-, and 24-months).
Estimates of the Contrast between Depressed and Nondepressed at Baseline With Outcomes at Each Follow-up Time Point Adjusted for Baseline Value Using Generalized Estimating Equations.

Due to the difference between depressed and nondepressed at baseline, we subtracted baseline value from each follow-up estimate. Adjusted model controlled for age (continuous), gender, education (categorical), income (categorical), marital status, years in United States, acculturation, medical comorbidities (not including item G15. which inquires about depression), visual/hearing difficulty, cognitive fxn-global, incontinence, NEWS-Environment-neighborhood, social support for physical activity, intrinsic religiosity and religious affiliation, outcome expectations for exercise, Tinnetti fear of falling, exercise self-efficacy, and study arm assignment.
Finally, retention analysis revealed that participants enrolled in “¡Caminemos!” were less likely to stay in the study if at baseline they were identified as depressed (i.e., endorsed two or more items on the GDS; p<0.0001) and if they exhibited lower levels of physical activity as measured by pedometer data (p<0.0001) and two of the YPAS subscales (i.e., Total Time Summary Index [p = 0.0041), and Energy Expenditure Summary Index (p = 0.0135]); note, results for the retention analyses are not shown in a tabular format. Retention at 24 months was 76% for the nondepressed subgroup and 50% for those with depressive symptomatology. As baseline depression was the main predictor of interest in the current study and differences in retention were observed for this construct, further retention analyses were conducted to examine the predictors of attrition among those with baseline depression. Social support for physical activity (but none of the other potential predictors) was associated with retention among the participants who had depression scores at or above the 2-point cutoff as set by the GDS. Participants with baseline depression who remained in the exercise program (i.e., those who reached the 24-month study completion date) were characterized as having higher levels of social support for physical activity.
Discussion
The current study evaluated the longitudinal relationship between depression status and physical activity among a sample of community-dwelling older Latino adults. Cross-sectional analyses with baseline data show that using several different measures of physical activity, individuals with depressive symptomatology were less likely to be engaged in walking behavior and they displayed lower physical activity levels. Upon enrollment in an exercise intervention, however, having depressive symptoms at baseline was associated with greater rates of attrition but was not associated with changes in physical activity level at any of the follow-up time points among those who stayed in the program. This suggests that baseline presence of depressive symptomatology may not serve as a barrier to engagement in future exercise behavior. Instead, encouragingly, initiation of physical activity among older adults regardless of depression status has the potential for long-term sustainability.
Cross-sectional findings of the current study are consistent with existing literature documenting the inverse relationship between depression and exercise levels, such that higher depression scores are associated with lower engagement levels of physical activity (Dunn et al., 2001; Krause, Goldenhar, Liang, Jay, & Maeda, 1993; Kritz-Silverstein, Barrett-Connor, & Corbeau, 2001; Morgan & Bath, 1998; Perrino et al., 2010). Additionally, baseline presence of depressive symptomatology was strongly associated with lower overall participation in the exercise intervention as revealed by the higher dropout rate. Higher rates of attrition among those with baseline depression is not uncommon as previous research has linked this psychological disorder to lower engagement levels in health behavior practices (Wing, Phelan, & Tate, 2002) and diminished exercise-related self-efficacy scores (Vickers, Nies, Patten, Dierkhising, & Smith, 2006). Although higher levels of attrition after enrollment in the “¡Caminemos!” exercise intervention were evident for those with baseline depression, exercise initiation and engagement among depressed older Latino adults is feasible, as 50% of this subpopulation completed the 24-month intervention and most of these individuals (80.5% based on pedometer data) increased their physical activity. The completion rate for the current 24-month study approximates that of Vickers et al. (2009; i.e., 10-week treatment completion rate of 65%), who conducted a randomized control trial examining the feasibility of an exercise counseling intervention in a population of women smokers with depression. In addition, the attrition rate among the depressed subpopulation in the current study is also comparable to that reported by Dishman and Buckworth (1997) among nondepressed adults. Specifically, they reported a stable mean exercise dropout rate of 50% among nondepressed adults after performing an extensive review of exercise programs conducted over a 20 year time span. Therefore, the current study suggests that more efforts should be placed on retaining study subjects with baseline depression while it also demonstrates that older Latino adults with depression can successfully engage in an exercise intervention and increase walking levels.
Social support for physical activity was the only construct associated with retention among subjects who endorsed 2 or more items in the GDS. Though not all the “¡Caminemos!” participants who were depressed and stayed in the study actually increased their exercise levels, these findings are compatible with the literature documenting the effectiveness of social support in enhancing motivation and adherence to an exercise program in the older adult population (Baert, Gorus, Mets, Geerts, & Bautmans, 2011; Dishman, Sallis, & Orenstein, 1985), as interpersonal relationships can be a source of encouragement in the form of positive reinforcement and tangible support (e.g., transportation to exercise facility). But, there is also evidence documenting lower levels of engagement in walking behavior among older adults with high levels of instrumental social support as a potential result of developed dependency. For instance, Perrino et al. (2011) found a lower likelihood of engagement in walking behavior in a sample of older Latino adults with high levels of instrumental social support (e.g., help with chores). This suggests that instrumental social support could hinder motivation and engagement in healthy behavior among depressed recipients. Instruments capturing the construct of social support may need to be further refined and implemented to more thoroughly distinguish between positive and negative forms of social support offered. With these new measurement tools, programs aimed at initiating and sustaining physical activity may more rigorously target older depressed adults receiving low levels of positive social support and/or high levels of dependency-promoting support.
Nonetheless, findings show that older adults who endorse symptoms of depression at baseline but who reach study completion show a significant increase in physical activity level with an associated improvement comparable to their nondepressed counterparts. This finding is not incompatible with available evidence on exercise adherence in populations with a psychiatric illness such as depression. For instance, Jette et al. (1998) found a positive association between the mood state of depression/dejection and adherence to the home-based “Strong for Life” resistance exercise program in a sample of community-dwelling older adults between the ages of 60 and 94 years. Patten, Vickers, Martin, & Williams (2003) found no significant differences in session attendance or mean number of minutes of exercise engagement between depressed and nondepressed smokers participating in a group-based exercise program. Examination of weekly exercise frequency further revealed that depressed smokers, when compared to their nondepressed smoking counterparts, reported significantly higher exercise levels. The authors hypothesize that the potential increase in positive emotional well-being associated with participation in physical activity may contribute to the higher exercise performance levels in the depressed subpopulation. Peer and researcher staff based social support and positive reinforcement if perceived to be of therapeutic benefit by the depressed subpopulation, may offer another mechanism for their high exercise adherence rates. Prohaska, Walcott-McQuigg, Peters, and Li (2000) offer yet another theory proposing that older adults with depression may intentionally opt to participate in exercise programs as a self-prescribed (or healthcare provider-prescribed) treatment method for their associated symptoms of depression. More research is needed to elucidate this phenomenon.
Given the underdiagnosis and low treatment rates for depression in older adults (Robins et al., 1991; Unutzer et al., 2003), it becomes clinically relevant to recognize that presence of depression will not necessarily serve as a barrier for initiation and maintenance to a physical activity regimen. Healthcare providers should be aware that older adults with depression are capable of joining physical activity programs with demonstrated exercise activity increases comparable to their nondepressed counterparts after initiation of an exercise regimen and among those who remain in the program. Given the substantial benefits associated with physical activity, healthcare providers should offer behavioral prescriptions and encouragement for patients with and without depression to initiate an exercise regimen.
This is one of the first studies done on this topic that does not solely rely on self-report measures of physical activity, as a more objective measure was obtained through use of a digital pedometer. Nonetheless, several study limitations should be considered in interpreting the findings. First, determination of depression status was not based on a clinical diagnosis made by a mental health provider as a self-report measure was administered (i.e., GDS), which served only as a screening tool and not a diagnostic examination. The covariates capturing psychosocial and physical health were also based on self-report measures and are therefore subject to biases (e.g., recall bias, respondent fatigue, etc). Second, not all survey instruments had a published Spanish version with previous psychometric testing. Third, the current study did not consider the potential change in depressive status across time or the initiation or use of antidepressive medication. It is plausible that initiation and engagement in physical activity (or the initiation of medication) served to alleviate symptoms of depression at 1-, 12-, and 24-months if one were to assume a continued deterioration in mental health in the absence of an exercise program. Finally, higher rates of attrition among older adults with baseline depression can operate as a study limitation, particularly since this subgroup would be more likely to report low physical activity levels.
Given the cross-sectional association between depression and physical activity, future research should explore the mechanism through which depression is associated with lower physical activity levels, particularly among older Latino adults. For instance, does depression lower physical activity level by lowering exercise self-efficacy, behavior specific knowledge, or social support? Or alternatively, perhaps the causal mechanism goes the other direction: people who do not exercise for other reasons are more likely to become depressed. Identification of the mechanisms through which depression and low level of physical activity interact has the potential to inform the development of more targeted prevention and treatment programs for older minority adults with clinically significant level of depression. The feasibility of implementing an exercise intervention among older adults with baseline depression was demonstrated by successful participant recruitment and by the fact that those with depression at baseline who stayed in the program had no difference in their increase in physical activity levels.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Number R01 AG024460-05 (C. Sarkisian, PI) and P30AG028748 (UCLA Claude D. Pepper Older Americans Independence Center). This publication was first drafted at the University of Illinois at Chicago by the lead author through funding received from the Diversifying Higher Education Faculty in Illinois (DFI) program. Editing and final submission was made possible by the National Institute of Health under Award Number 5T32 HL069771-10 (M. Daviglus, PI).