
Abstract
Difficulty in hearing is a common health concern among older adults affecting about two thirds of people aged 70 years and older (Lin, Thorpe, Gordon-Salant, & Ferrucci, 2011). Hearing difficulties can hamper interaction with other people and safe orientation in the environment (Arlinger, 2003; Helvik, Jacobsen, & Hallberg, 2006), thus complicating engagement in daily life situations (Wallhagen, Strawbridge, Shema, Kurata, & Kaplan, 2001). Hearing aid (HA) use may improve hearing performance and ease the perceived negative consequences of hearing difficulties (Kochkin & Rogin, 2000), thereby supporting participation in society. However, while most HA users are likely to perceive benefit from HA use (Wong, Hickson, & McPherson, 2003), fewer than half of older adults with impaired hearing report using them (Bainbridge & Ramachandran, 2014; Hartley, Rochtchina, Newall, Golding, & Mitchell, 2010; Lin et al., 2011). Among the main reasons for not using a HA are that it is perceived to provide poor benefit, the device is found uncomfortable (Hartley et al., 2010; McCormack & Fortnum, 2013) or stigmatizing (Gagné, Southall, & Jennings, 2011), or a hearing problem is not perceived severe enough for needing a HA (Gopinath et al., 2011; Knudsen, Oberg, Nielsen, Naylor, & Kramer, 2010).
In the present study, older adults’ participation in everyday life situations in society is examined through life-space mobility. Life-space mobility refers to the size of the spatial area a person moves through in everyday life, taking into account the frequency of moving and the assistance needed for movement, thus describing total mobility (Baker, Bodner, & Allman, 2003). An individual with larger life-space has more opportunities to engage in desired activities in society (Kono, Kai, Sakato, & Rubenstein, 2004), whereas restrictions in life-space mobility may indicate more limited possibilities for participation (Rosso, Taylor, Tabb, & Michael, 2013). Maintenance of life-space mobility may help to sustain better quality of life (Rantakokko et al., 2016).
Previously, only two studies have investigated the association between hearing difficulties and life-space mobility among older adults, and the results of these studies are somewhat inconsistent (Allman, Baker, Maisiak, Sims, & Roseman, 2004; Polku et al., 2015). In both studies, self-reported hearing difficulties were found to be associated with poorer life-space mobility in community-dwelling older adults, but in the study of Allman et al. (2004), the association was not found statistically significant when adjusted for other health conditions (Allman et al., 2004). Comparison between these results is difficult because the studies differ in their sample sizes and the methodologies used to measure hearing difficulties. Moreover, neither study investigated the effects of HA use on life-space mobility. Thus, the aim of the present study was to explore whether HA use, and more specifically perceived benefit from HA use, is associated with life-space mobility among community-dwelling older adults. In this study, perceived benefit from HA use refers to the difference between unaided and aided self-rated hearing ability. We compared life-space mobility of older adults who benefit less from HA with those who benefit more from HA. In addition, we explored whether these groups differ from those who do not use HA.
Method
Study Design and Participants
This study is based on cross-sectional analyses of the data obtained from the second follow-up of the “Life-Space Mobility in Old Age” (LISPE) project, which is a 2-year prospective cohort study of community-dwelling Finnish older adults. The study design and methods, including non-respondent analysis, have been reported in detail elsewhere (Rantanen et al., 2012). Briefly, at baseline, a random sample of 2,550 older community-dwelling persons between 75 and 90 years of age was obtained from the national population register and used as the basis for recruitment. After an information letter, the persons were contacted over the telephone to enquire about their willingness to participate. Inclusion criteria were being community-dwelling in the study area, and able to communicate (i.e., able to understand the questions and provide answers to them). In total, 848 eligible persons participated in the baseline interviews during spring 2012. Of these, 761 participated in the 2-year follow-up, which consisted of a telephone interview and a postal questionnaire. If the participant was unable to answer the questions over the phone due to hearing problems, the possibility to take part in a face-to-face interview in their homes (n = 3) or, to answer the study questions via a postal questionnaire (n = 10) was offered and implemented. The 2-year follow-up postal questionnaire, which included data on HA use, was returned by 712 participants (Rantakokko et al., 2016). The LISPE project was approved by the Ethical Committee of the University of Jyväskylä. Participants were informed about the project and signed a written informed consent prior to the study.
Life-Space Mobility
Life-space mobility was assessed via telephone interview using the University of Alabama at Birmingham Life-Space Assessment (LSA) questionnaire (Baker et al., 2003). The LSA is based on self-report and contains 15 items. It measures mobility through different life-space levels (bedroom, other rooms in the home, outside home, neighborhood, town, beyond town) either by walking or using other forms of transportation, such as driving a car or using public transportation, during the 4 weeks preceding the assessment. Participants were asked how many days a week they attained each life-space level and whether they needed help from another person or from assistive devices. The life-space mobility score ranging from 0 to 120 (higher scores indicate better life-space mobility) was used in the analyses (Baker et al., 2003).
Perceived hearing ability and perceived benefit from HA use
In the postal questionnaire, the participants were asked, “How is your hearing?” Specifically, participants were asked to assess their hearing by choosing the number on a scale from 0 to 10 that best corresponded to their perceived hearing ability. Higher scores indicated poorer performance. Participants, who reported having a HA, gave two answers: one assessing their hearing with, and the other without, their HA (Figure 1).

Assessment of perceived hearing ability and perceived benefit from hearing aid use.
Perceived benefit from HA use was quantified by subtracting the aided hearing score from the unaided hearing score, a greater difference indicating greater perceived benefit. The median value of perceived benefit from HA use in the present sample was three, and was used as a cut point to categorize HA users. For the analyses, participants were divided into three groups: (a) more HA benefit (difference of 3 or more points between non-aided and aided hearing ability), (b) less HA benefit (difference less than 3 points), and (c) no-HA group (participants who reported not having a HA). HA users were also asked whether they used their HA daily (yes/no), whether they had a HA only in one ear or in both ears and, with an open-ended question, to estimate how many hours per day on average they used their HA.
Potential confounders
Factors previously found to be associated both life-space mobility decline and hearing difficulties were considered as potential confounders. Age and gender were derived from the population register. Number of years of education was used as a socioeconomic indicator. Self-reported physician-diagnosed chronic conditions were obtained from a list of 22 chronic conditions and with an open-ended question. Chronic conditions that could theoretically be linked to hearing difficulties and life-space mobility, namely, diabetes, rheumatoid arthritis, cardiac, circulatory, and neurological diseases, were chosen as potential covariates. Cognitive functioning was assessed using the Mini-Mental State Examination (MMSE; Folstein, Folstein, & McHugh, 1975). Depressive symptoms were assessed with the 20-item Centre for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977).
Statistical analyses
Of those participants who had returned the postal questionnaire (n = 712), 584 reported that they did not have a HA and, 127 reported having a HA (data on HA use were missing for one participant). Of these participants who reported having a HA, information on the perceived benefit from HA use was available for 118 participants. These participants were included in the analyses, and thus, the final sample consisted of 702 participants. Life-space mobility data were available for 699 of these participants. As life-space mobility data were missing for less than 1% of the participants, missing values were not imputed.
Characteristics of the participants are described using means and standard deviations (SDs) or percentages. One-way ANOVA was used for continuous variables and chi-square tests for categorical variables to compare characteristics between the groups categorized according to HA use and perceived benefit. Analysis of covariance (ANCOVA) was used to test the association between perceived benefit from HA use and life-space mobility. Levene’s test of equality of error variances indicated that the error variance of the dependent variable (life-space mobility score) was equal across groups. Skewness and kurtosis of the life-space score distribution were acceptable in each group.
Of the potential covariates, only age and perceived hearing ability without a HA differed statistically significantly between the groups and were thus included in the analysis. A value of p < .05 was chosen as the level of statistical significance. IBM SPSS version 22.0 (SPSS Inc., Chicago, IL) was used for the analyses.
Results
The mean age of the participants was 82 years (SD = 4.2) and 63% were women. The mean life-space mobility score was 63 (SD = 21.7), ranging from 6 to 120. Of the participants, 18% reported having a HA. The sample characteristics categorized according to perceived benefit from HA use are presented in Table 1. Among the participants who perceived more benefit from HA, 81 % reported using the HA daily and on average 9 hr/day. Among those who perceived less benefit from HA, 49% reported daily use and on average 6 hr/day. Of the 127 participants who reported having a HA, five participants (4%) reported having a HA in both ears (binaural fitting). Distributions of the unaided and aided hearing scores by categories of HA use are shown in Figure 2.
Characteristics of the Participants Categorized by Hearing Aid Use (n = 702).
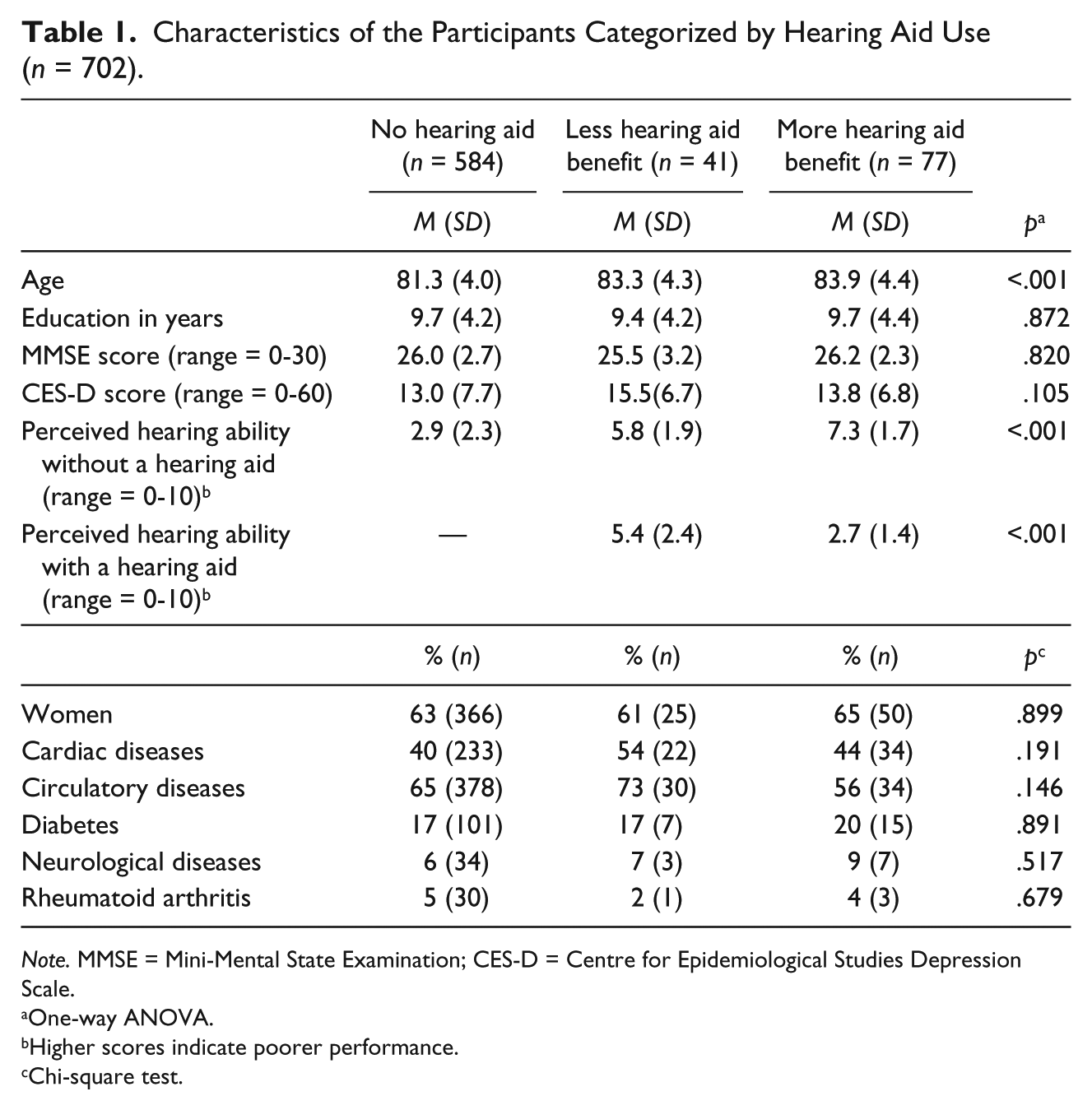
Note. MMSE = Mini-Mental State Examination; CES-D = Centre for Epidemiological Studies Depression Scale.
One-way ANOVA.
Higher scores indicate poorer performance.
Chi-square test.
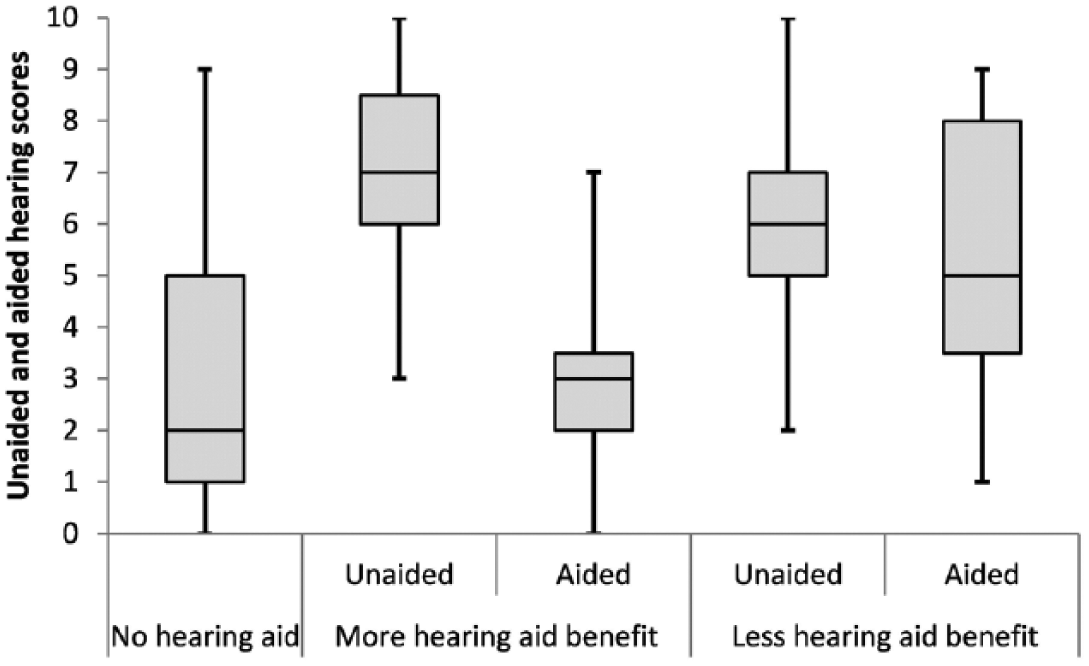
Distribution of the unaided and aided hearing scores by categories of hearing aid use.
The estimated marginal means for life-space mobility by categories of HA use are presented in Figure 3. In the crude model, the difference in the life-space mobility score was not statistically significant between participants who perceived more benefit from HA (M = 60, 95% confidence interval [CI] = [55, 64]) and those who perceived less benefit from HA (M = 51, 95% CI = [44, 57]; mean difference = 8.7, 95% CI for difference = [−1.3, 18.6]). Participants who perceived more benefit from HA did not differ from no-HA group (M = 64, 95% CI = [62, 66]) in their life-space mobility score (mean difference = −4.4, 95% CI for difference = [−10.6, 1.9]). However, no-HA group had significantly better life-space mobility score than those participants who perceived less benefit from HA (mean difference = 13.0, 95% CI for difference = [4.8, 21.3]).
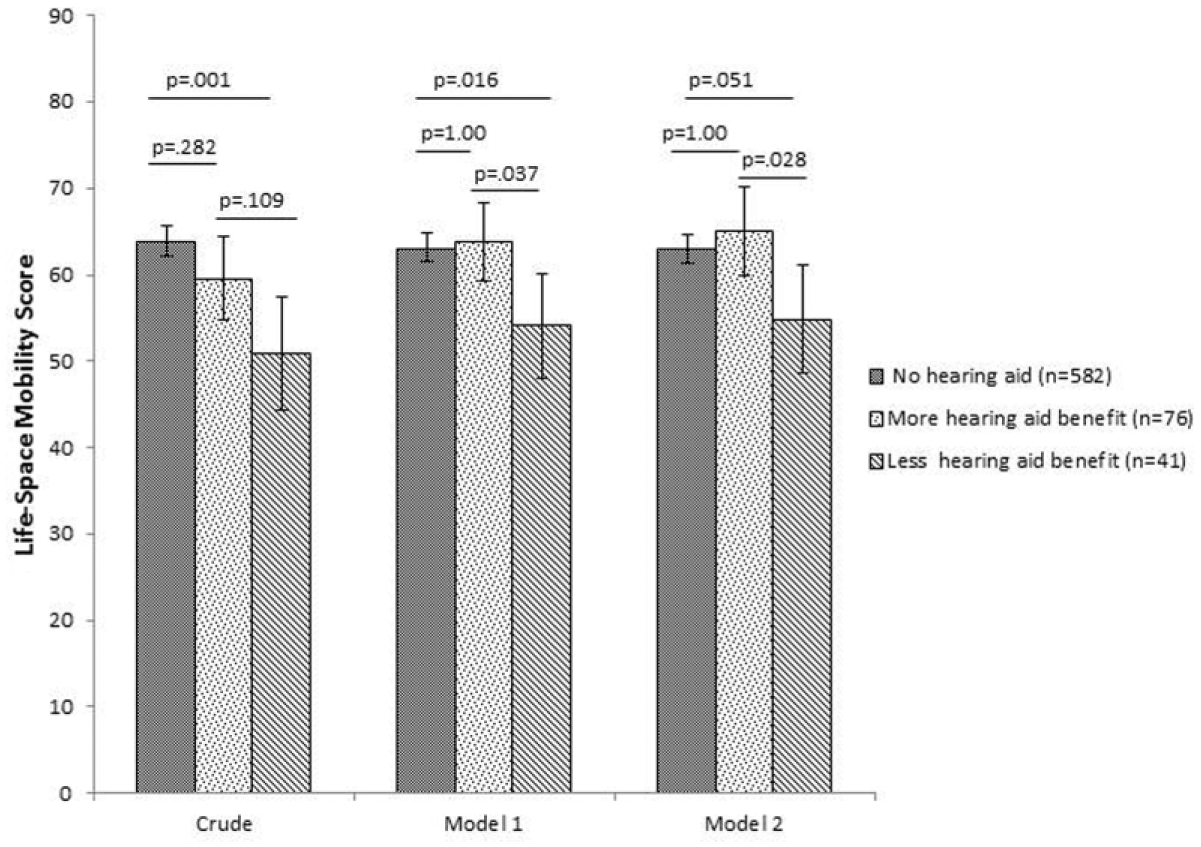
Estimated marginal means and 95% confidence intervals for life-space mobility (range = 0-120) by categories of hearing aid use.
After further adjustment for age and perceived hearing ability without a HA (Figure 3, Model 2), the difference in life-space mobility score between those who perceived more benefit from HA and those who perceived less benefit from HA maintained at the same level but became statistically significant (M = 65, 95% CI = [60, 70] vs. M = 55, 95% CI = [49, 61], respectively, mean difference = 10.1, 95% CI for difference = [0.8, 19.4], p = .028). Participants who perceived more benefit from HA and no-HA group (M = 63, 95% CI = [61, 65]) did not differ in their life-space mobility scores after this adjustment (mean difference = 2.1, 95% CI for difference = [−4.8, 8.9]). The post-adjustment difference between no-HA group and participants who perceived less benefit from HA was borderline significant (mean difference = 8.0, 95% CI for difference = [−0.03, 16.1], p = .051).
Discussion
Our study showed that persons who perceived more benefit from HA use had a significantly higher life-space mobility score than those who perceived less benefit and that their life-space mobility score was comparable with that of those without a HA.
The present study contributes novel information on perceived hearing difficulties and life-space mobility. To our knowledge, only two earlier studies have investigated this association (Allman et al., 2004; Polku et al., 2015). However, their findings were conflicting and neither of them focused on HA use. Allman et al. (2004) reported that after adjustment for other health conditions, hearing difficulty did not predict decline in life-space mobility over an 18-month follow-up. Another previous study (Polku et al., 2015) showed that life-space mobility was lower among people with hearing difficulties but declined at a similar rate over the 2-year follow-up period compared with the people who did not have hearing difficulties. The results of the present study provides further evidence for the association of poor hearing and low life-space mobility, as the perceived benefit from the HA use was associated with higher life-space mobility.
There may be several explanations for the current result. For older adults, the need to interact with others is one of the main reasons for going outside the home (Gardner, 2014). However, older people with hearing difficulties can experience communication breakdowns and avoid situations in which they might experience feelings of frustration or being left out (Arlinger, 2003; Gopinath et al., 2012). Self-stigma means that some older adults hold the same negative stereotypes about their hearing loss as those held by the society. Persons who exhibit self-stigma associated with hearing loss are more likely to reduce their activities outside the home to minimize the chances of revealing their hearing loss to others (Gagné et al., 2011). Even though a person would not withdraw entirely from situations that are challenging for hearing, they may involve in them less frequently (Mikkola et al., 2015; Polku et al., 2015). Perceived benefit from the HA may facilitate participation in out-of-home situations, thereby supporting life-space mobility.
Hearing difficulties can also impair a person’s ability to reliably detect and recognize acoustic environmental cues when moving around (Arlinger, 2003). These cues may be essential for safe orientation in space, for example, in localizing sounds of the motor vehicles. Previous studies have shown that hearing impairment is associated with walking difficulties (Viljanen, Kaprio, Pyykkö, Sorri, Koskenvuo, et al., 2009), poorer postural balance (Viljanen, Kaprio, Pyykkö, Sorri, Pajala, et al., 2009), and fear of falling (Viljanen et al., 2012). These difficulties together with impaired ability to detect environmental acoustic information may compromise safe mobility. Use of a HA may be hypothesized to reduce fear of falling and related activity restriction leading to increased out-of-home participation.
Perceived benefit from HA use is also related to the interaction between the person and his or her environment (Noble & Hétu, 1994). Listening situations differ in their auditory demands (Wong et al., 2003) and, for example, having a conversation in a group requires a lot more auditory processing than a conversation in a quiet room (Williger & Lang, 2014). A person who participates in activities that require a lot of communication is more likely to experience hearing difficulties as disturbing than a person who prefers solitary activities (Chang, Ho, & Chou, 2009). Thus, he or she may also be more likely to perceive benefit from HA use than the person who participates in fewer activities outside the home. It is probable that individuals with moderate or severe hearing impairment are more likely to use a HA and therefore, also more likely to experience more benefit from the use of a HA (Knudsen et al., 2010; Williger & Lang, 2014). For people with mild perceived hearing loss, the perceived gain from using a HA may be less. This was also supported by the current study as those who perceived benefit from HA use had lower self-rated hearing without a HA.
The strengths of this study include the use of large population-based sample, which increases the generalizability of the results. As our cohort included participants with and without hearing difficulties, the associations observed in this study likely represent those prevalent in a similar-aged general population. The study also has its limitations. Because of the cross-sectional design, the causality of the associations between the variables investigated cannot be determined. That is, we cannot say that perceiving benefit from the use of HA is a cause or a consequence of higher life-space mobility. Although we aimed to control for the effects of potential confounders, the possibility of residual confounding variables induced by unmeasured factors cannot be ruled out. Also, a few persons were excluded from the study because they were not able to communicate due to hearing problems. Therefore, it is likely that persons with severe hearing impairment were under-represented, and selection bias cannot be completely ruled out. Had these persons participated, the associations observed between HA benefit and life-space mobility might have been stronger. Further studies with larger number of HA users are needed to confirm the associations reported in this study. We were not able to use audiological equipment to quantify hearing status or to validate the appropriateness of the HAs fitted. However, previous studies support the validity of self-reported measures of hearing impairment and HA benefit (Strawbridge, Wallhagen, Shema, & Kaplan, 2000). One advantage of self-report questionnaire is that they capture information about the everyday activities and situations (Kiely, Gopinath, Mitchell, Browning, & Anstey, 2011). Moreover, subjective experiences, such as perceived benefit can be evaluated only via self-reports. In the present study, no information was collected concerning the types of HAs used by the participants. Only 4% of the HA users reported having two HAs, and therefore, it was not possible to compare the participants who were fitted with one HA (monaural fitting) and those fitted with two HAs (binaural fitting). Future investigations of the effects of the HA use on life-space mobility should take into account the role of these variables.
In conclusion, our results indicate that perceived benefit from HA use is associated with better life-space mobility. The current result serves as a justification for future studies examining whether use of a proper HA will promote life-space mobility and participation among those with difficulties in hearing.
Footnotes
Acknowledgements
Gerontology Research Center is a joint effort between the University of Jyväskylä and the University of Tampere.
Authors’ Note
This study was presented as a poster at the 23rd Nordic Congress of Gerontology in Tampere, Finland on June 19-22, 2016.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Academy of Finland (grant number 263729). The Life-Space Mobility in Old Age (LISPE) project is funded by the Academy of Finland, the Future of Living and Housing program (ASU-LIVE; grant number 255403 to T.R.) and Finnish Ministry of Education and Culture (to T.R. and E.P.). M.R. is funded by the Academy of Finland (personal grant number 285747). H.P. is funded by the Juho Vainio Foundation and the Finnish Federation of Hard of Hearing (FFHOH).