
Abstract
Introduction
In the United States, the age structure of the population is projected to drastically change in the upcoming decades. By 2050, the older adult population in the United States is projected to increase from 43.1 million to 83.7 million (Ortman, Velkoff, & Hogan, 2014). The older adult population will also become more racially and ethnically diverse. Hispanic older adults, 65 years and older, are projected to grow from 7.3% in 2012 to 18.3% in 2050 (Ortman et al., 2014). Given the increasing number of older adults and growing diversity of the population, the prevalence of chronic disease, including cognitive impairment and dementia, is expected to increase (Alzheimer’s Association, 2018; Centers for Disease Control and Prevention, 2011). Alzheimer’s disease (AD), a neurodegenerative disorder, is the most common form of dementia. It affects approximately 5.5 million older Americans, and this number is projected to increase to as high as 13.8 million by 2050 (Alzheimer’s Association, 2018; Hebert, Weuve, Scherr, & Evans, 2013). AD is the sixth leading cause of death in the United States, and the mortality rate from AD is increasing (Alzheimer’s Association, 2018). As AD progresses, disability, decreased quality of life, and high health care costs are inevitable (Alzheimer’s Association, 2018).
Racial and ethnic minorities have a higher burden of AD compared with non-Hispanic Whites in terms of prevalence, severity, and social and economic burden (Alzheimer’s Association, 2018; Gurland et al., 1999; Haan et al., 2003; Potter et al., 2009). The term Hispanic refers to a heterogeneous population of individuals from Spanish-speaking countries; therefore, the risk of developing AD among adults who identify as Hispanic varies based on country of origin (Mehta & Yeo, 2017). High incidence and prevalence is observed among Caribbean Hispanics while a low incidence and prevalence is observed among Mexican Americans (Mehta & Yeo, 2017). This higher burden of AD in racial and ethnic minority groups is likely due to the higher burden of risk factors, including hypertension, diabetes, and socioeconomic factors (Alzheimer’s Association, 2018; Chin, Negash, & Hamilton, 2011; Mayeda, Glymour, Quesenberry, & Whitmer, 2016; Yaffe et al., 2013). Moreover, minority group members are more likely to receive delayed diagnosis and treatment for AD (Chin et al., 2011). The increasing number of individuals who identify as a racial or ethnic minority represent a growing group of individuals who are at a high risk of developing AD (Chin et al., 2011).
Reduced knowledge of AD may increase racial and ethnic disparities in disease burden by reducing risk prevention and help seeking (Ayalon & Arean, 2004). In a systematic review of literature on the public’s knowledge of AD and dementia, Cahill and colleagues found that dementia knowledge among racial and ethnic minorities was poor and included myths about the causes of AD and dementia (Cahill, Pierce, Werner, Darley, & Bobersky, 2015). Previous studies have found that Blacks, Hispanics, and Chinese are more likely than their White counterparts to believe that AD is a normal part of aging (Connell, Roberts, & McLaughlin, 2007; Connell, Roberts, McLaughlin, & Akinleye, 2009; Gray, Jimenez, Cucciare, Tong, & Gallagher-Thompson, 2009). Compared with Whites, Blacks had lower levels of factual knowledge about AD and reported fewer information sources for AD (Roberts et al., 2003). In addition, Fornazzari and colleagues assessed AD knowledge of Latin Americans and found that AD knowledge was low, specifically pertaining to the causes of AD symptoms (Fornazzari, Fischer, Hansen, & Ringer, 2009). In Latinos and Asian groups, AD knowledge was associated with level of education and the number of year speaking English, respectively (Ayalon & Arean, 2004). Furthermore, Black and Hispanic populations were more likely to be optimistic about the direction of current AD research and report lifestyle changes to prevent AD compared with Whites (Connell et al., 2007; Connell et al., 2009). Compared with Blacks and Whites, Hispanics felt well prepared to handle the AD diagnosis of a family member, which may be attributable to the cultural norm of filial piety (Connell et al., 2007).
Given the large burden of AD in Hispanics and Blacks, it is essential to assess the AD knowledge of members of racial and ethnic minority groups to inform educational interventions and increase the initiation of conversations with medical professionals about cognitive health. The AD knowledge of Hispanics has been studied less frequently than other minority groups, such as Blacks. Therefore, these analyses aim to expand the literature about AD knowledge among Hispanic populations. The objective of these analyses was to compare AD knowledge by race and ethnicity in a community sample of middle-aged and older adults in Florida. We hypothesized that non-Hispanic Whites would have more knowledge of AD compared with non-Hispanic Blacks and Hispanics.
Method
Population
We analyzed data we collected through HealthStreet, a University of Florida community engagement program which assesses the health conditions and concerns of community members in Florida through Community Health Workers (CHWs). CHWs are members of the community they serve and are trained to engage community members where they live, work, and recreate. Once consented, participants are interviewed by CHWs; information on demographics, socioeconomic status, physical and mental health, substance use, and willingness to participate in health research is obtained [Cottler, O’Leary, & Striley, 2010; Cottler, Striley, O’Leary, Ruktanonchai, & Wilhelm, 2013]. Since April 2016, participants 50 years of age and older were asked to complete an AD questionnaire. Participants who completed the AD questionnaire and who provided information on their race and ethnicity were included in these analyses (N = 842). Ethics approval was obtained by the University of Florida Institutional Review Board. Written informed consent was obtained from all participants.
Measures
Exposure
Race and ethnicity were categorized into a three-level variable: non-Hispanic White, non-Hispanic Black, and Hispanic.
Outcome
The main outcome of interest was Alzheimer’s Disease Knowledge Scale (ADKS) score. The ADKS is a 30-point, true/false assessment of knowledge of AD covering several content domains including risk factors, assessment and diagnosis, symptoms, life course, treatment and management, and caregiving (Carpenter, Balsis, Otilingam, Hanson, & Gatz, 2009). As a part of HealthStreet’s AD questionnaire, participants are asked to answer 13 items from an abbreviated ADKS covering the risk factors, assessment and diagnosis, symptoms, life course, and treatment and management domains; their number of correct answers was summed into a continuous variable ranging from 0 to 13 for individuals who provided a response for each ADKS item. Internal reliability of this abbreviated scale was reduced from the original scale (Standardized Cronbach’s Alpha = 0.71 and 0.49, respectively); however we wanted a much less burdensome measure since HealthStreet participants are asked to provide a wide variety of information during the interview.
Covariates
Age was recorded as a continuous variable and sex was recorded as male or female. Marital status was coded as currently married or not married (never married, separated, widowed, or divorced). Employment status was characterized as employed (full- or part-time) or nonemployed (not working full- or part-time). Information on education was recorded as a continuous variable “Last grade completed?” which we categorized into two groups: less than 12 years (less than high school graduation) or 12 years or more (at least general educational development [GED]/high school diploma). Participants were asked whether they have any type of medical insurance; this provided the basis for our binary insurance variable. CHWs ask participants, “Have there been times in the last 12 months when you did not have enough money to buy food that you or your family needed?” providing the basis for our food insecurity variable. Recruitment site was categorized into a four-level variable: recruitment from Gainesville, Jacksonville, Miami, or other rural counties. Participants were asked, “Have you or your parents been diagnosed with AD or another memory disorder?” If participants indicated that they received a diagnosis, they were categorized as self-reporting dementia. If either the father or mother of the participant was diagnosed with AD or another memory disorder, they were recorded as having a positive family history of dementia. Participants were asked, “Have you ever been told you had, or have you ever had a problem with [condition]?” Responses to this question for lifetime hypertension, diabetes, or depression were coded as yes or no.
Analysis
All analyses were conducted using SAS® software, version 9.4. Descriptive statistics were calculated for sample characteristics, ADKS items, and ADKS domain by race and ethnicity. Chi-square tests of independence, t tests, and ANOVA were used to test differences by race and ethnic group. Using the Proc General Linear Models Select command, a forward stepwise linear regression was conducted to identify factors associated with total ADKS score.
Results
Among the 842 participants in these analyses, 12.4% were Hispanic, and 62.3% were female. The participants had a mean age of 62.4 years old. About 1.0% reported dementia of any kind, while 20.3% reported a positive family history of AD. Hispanics and non-Hispanic Whites were significantly older than non-Hispanic Blacks. Compared with Hispanics and non-Hispanic Blacks, non-Hispanic Whites reported significantly more nonemployment (p < .05). A larger proportion of non-Hispanic Blacks reported less than high school graduation compared with Hispanics and non-Hispanic Whites; however, this difference was only significant between non-Hispanic Blacks and non-Hispanic Whites (p < .05). Food insecurity differed significantly between all three groups with Hispanics reporting the least food insecurity (26.3%), followed by non-Hispanic Whites (37.4%) and non-Hispanic Blacks (48.0%). Recruitment site also significantly differed between all three groups (p < .05). More than half of the Hispanics were recruited from Miami (62.5%), and more than half of the non-Hispanic Blacks and non-Hispanic Whites were recruited from Gainesville (56.8% and 67.5%, respectively). In addition, 20.6% of non-Hispanic Blacks were recruited from Jacksonville, while more than a quarter (26.8%) of non-Hispanic Whites were recruited from other, rural, counties. Self-reported hypertension was significantly different between all three groups; non-Hispanic Blacks were more likely to report hypertension (61.0%) while Hispanics were least likely to report hypertension (32.7%; p < .05). In addition, non-Hispanic Whites reported significantly more depression compared with Hispanics and non-Hispanic Blacks (43.5% vs. 29.8% and 26.0%, respectively; p < .05). Sex, marital status, insurance status, self-reported dementia, family history of dementia, and self-reported diabetes did not differ by race and ethnicity (Table 1).
Sociodemographic Characteristics and Comorbid Diseases of HealthStreet Participants Who Completed an ADKS (n = 842), by Race/Ethnicity.
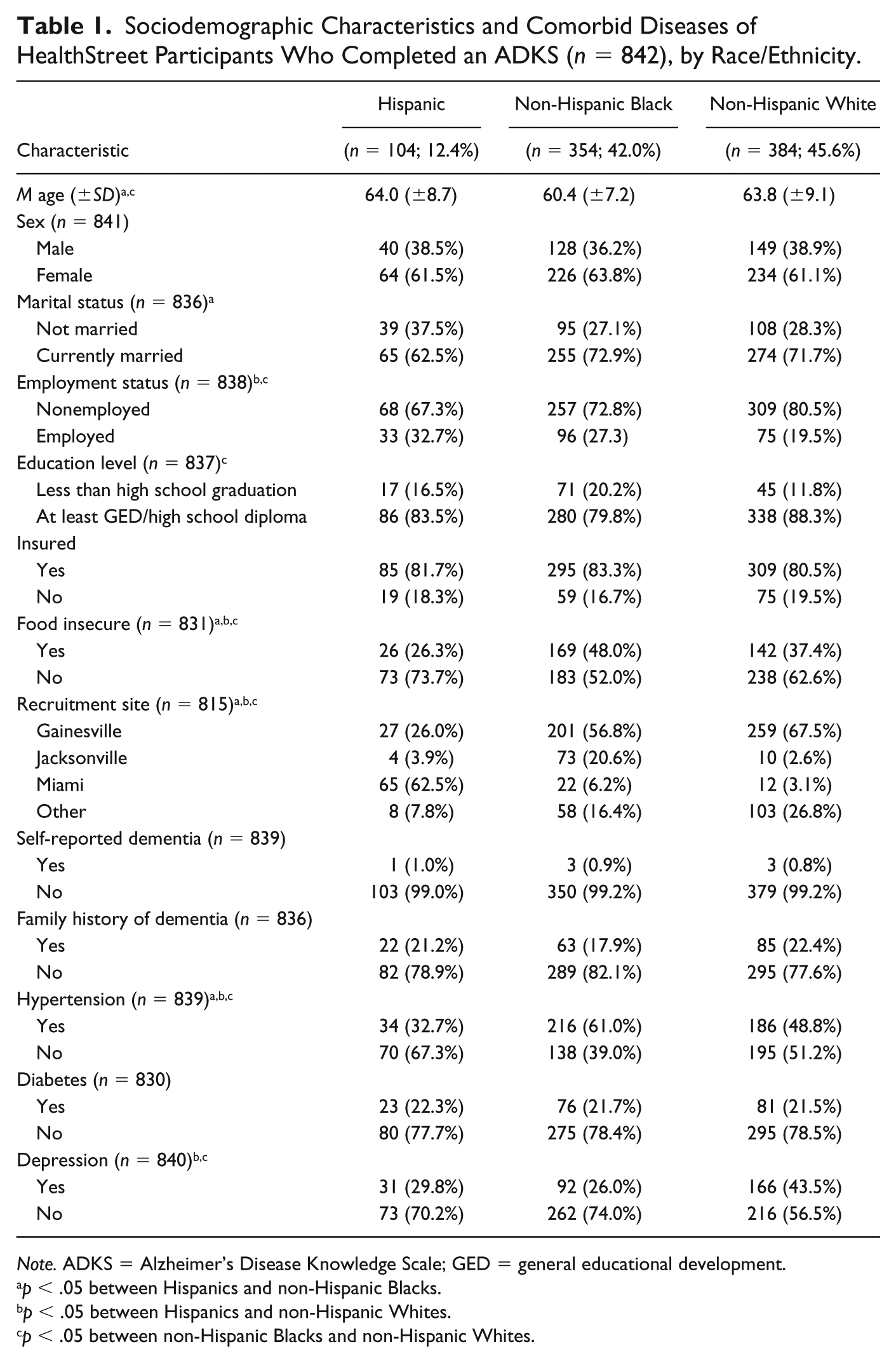
Note. ADKS = Alzheimer’s Disease Knowledge Scale; GED = general educational development.
p < .05 between Hispanics and non-Hispanic Blacks.
p < .05 between Hispanics and non-Hispanic Whites.
p < .05 between non-Hispanic Blacks and non-Hispanic Whites.
Table 2 displays the percentage of participants who correctly answered each ADKS item by race and ethnicity. Hispanics were significantly more likely to know that people with AD are prone to depression and that having either high cholesterol or high blood pressure may increase an individual’s risk of developing AD (p < .05). For other ADKS items, Hispanics and non-Hispanic Whites answered comparably; however, these two groups significantly answered more items correctly than non-Hispanic Blacks (p < .05). Table 3 displays ADKS content knowledge mean score by race and ethnic group. Significant differences were observed in each domain (p < .001). Hispanics scored better than non-Hispanic Blacks and non-Hispanic Whites on the life impact, risk factor, and course of disease domains. On the remaining domains, Hispanics and non-Hispanic Whites scored similarly but higher than non-Hispanic Blacks.
Percentage of Participants Who Correctly Answered Each ADKS Item (n = 842), by Race and Ethnicity.
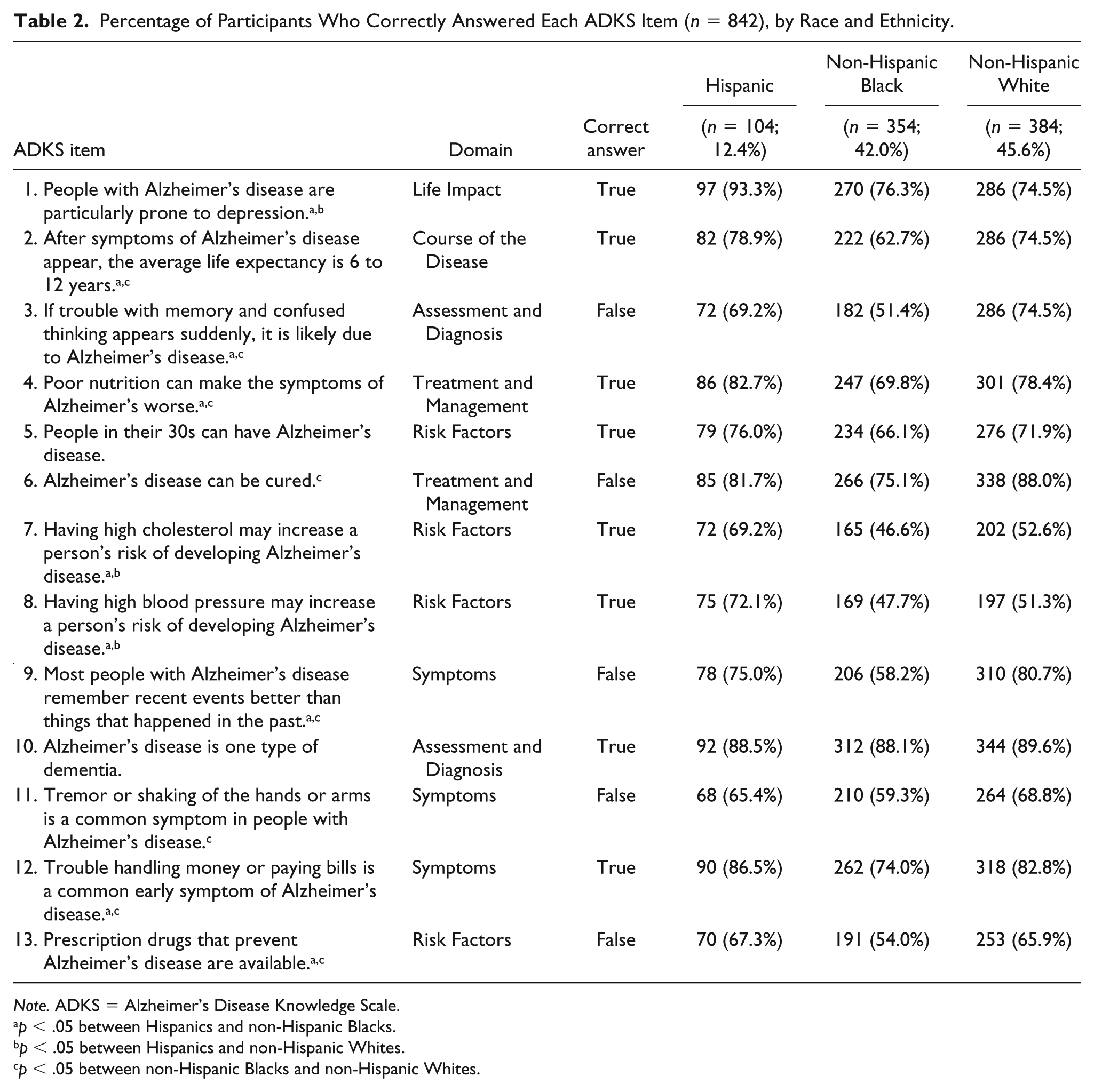
Note. ADKS = Alzheimer’s Disease Knowledge Scale.
p < .05 between Hispanics and non-Hispanic Blacks.
p < .05 between Hispanics and non-Hispanic Whites.
p < .05 between non-Hispanic Blacks and non-Hispanic Whites.
ADKS Content Domain Mean by Race/Ethnic Group.
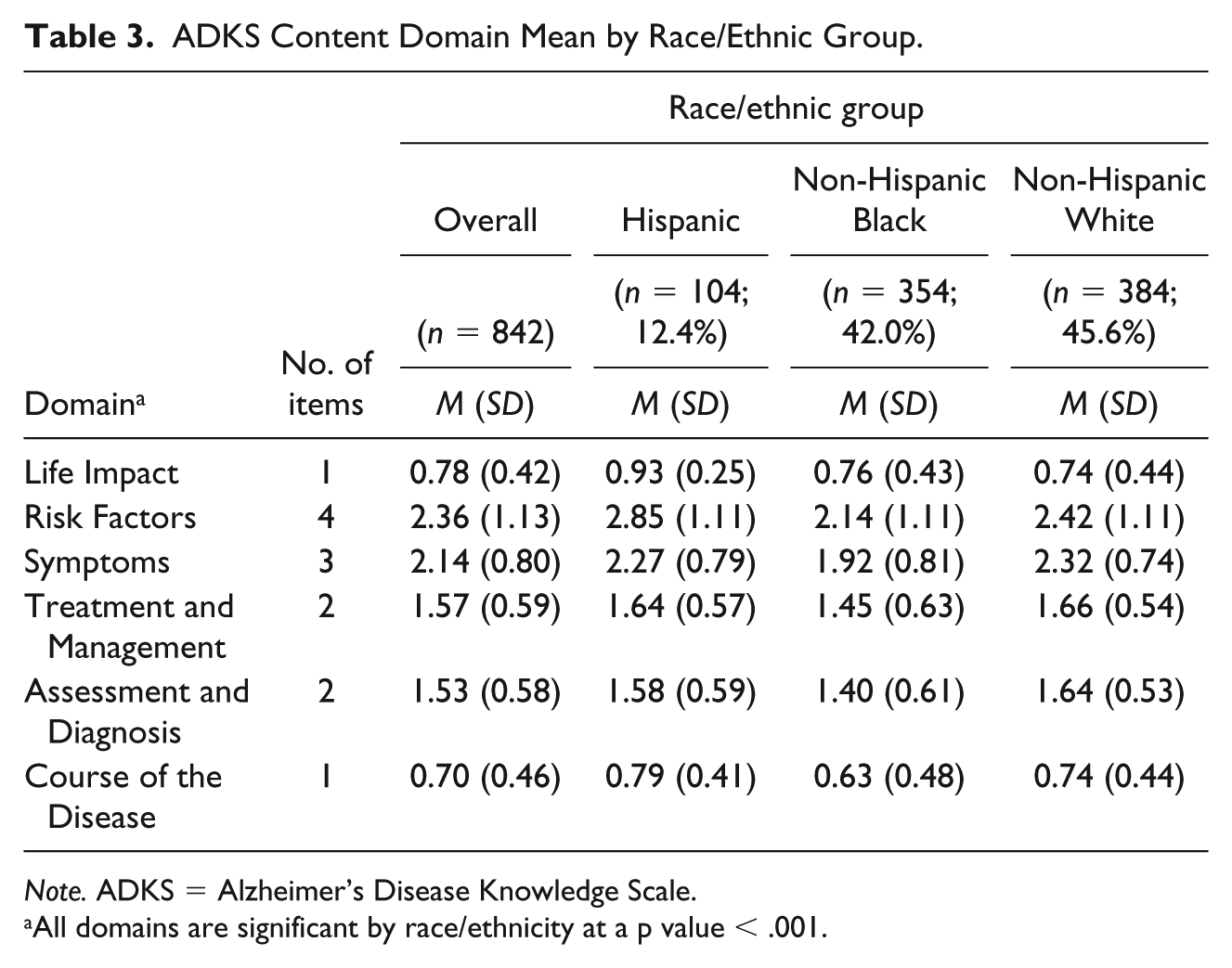
Note. ADKS = Alzheimer’s Disease Knowledge Scale.
All domains are significant by race/ethnicity at a p value < .001.
Results from the stepwise linear regression model are shown in Table 4 (adjusted R2 = 0.171). Race and ethnicity, age, sex, education, food insecurity, and recruitment site were included in the final model. Older age, recruitment from Miami, being non-Hispanic White or Hispanic, female, having more than a high school diploma, and not reporting food insecurity were associated with a higher ADKS score.
Stepwise Linear Regression Model Predicting ADKS Score (n = 819).
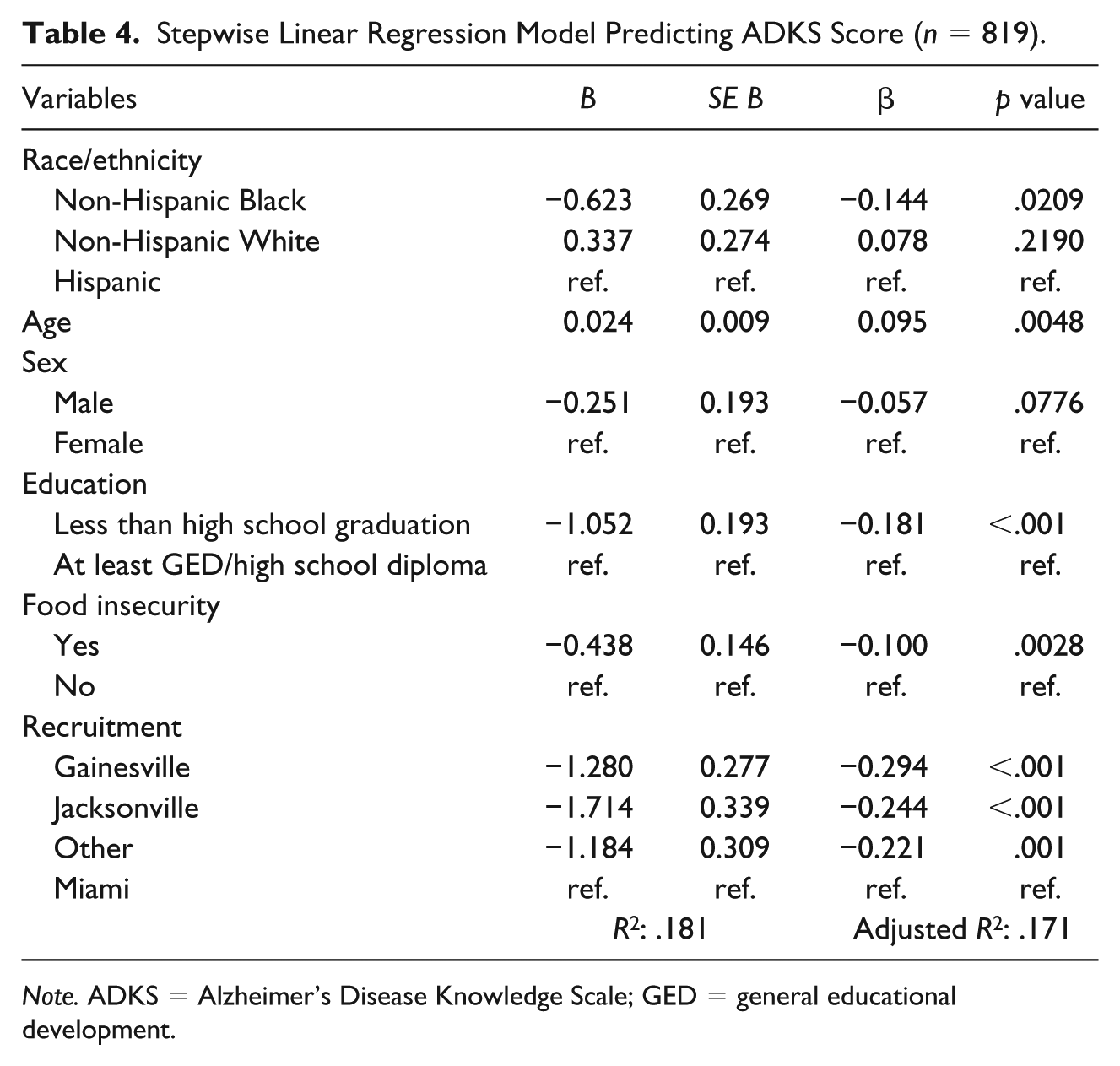
Note. ADKS = Alzheimer’s Disease Knowledge Scale; GED = general educational development.
Discussion
In these analyses, the association between race and ethnicity and AD knowledge was assessed among community-dwelling middle-aged and older adults residing in Florida. Overall, Hispanics and non-Hispanic Whites had comparable knowledge of AD. However, Hispanics were significantly more likely to be aware that there is an association between AD and depression and that high cholesterol and high blood pressure increase the risk of AD compared with non-Hispanic Blacks and Whites. As found in the extant literature, non-Hispanic Whites had a higher knowledge of AD compared with non-Hispanic Blacks. Moreover, in these analyses, AD knowledge among Hispanics was considerably higher than non-Hispanic Blacks as well.
In previous studies, results have indicated that non-Hispanic Whites have a higher knowledge of AD compared with Hispanics (Cahill et al., 2015). However, 62.5% of the Hispanics included in this sample were recruited in Miami, which has a different population of Hispanics compared with the United States. While Mexican Americans make up over half of the U.S. population, the Hispanic community in Miami mainly comprises individuals of Cuban or South American origin (Lopez, 2011). Moreover, Hispanics in this sample reported the least food insecurity, which is a proxy for socioeconomic status. Previous work has found that minorities and those in lower socioeconomic levels are less likely to seek health information from health care providers (Richardson, Allen, Xiao, & Vallone, 2012). The higher socioeconomic status among Hispanic participants compared with non-Hispanic White and non-Hispanic Black participants may be why our Hispanic participants have a comparable knowledge with non-Hispanic Whites and differ from the extant literature.
In addition, among Hispanics, country of birth differed when considering Miami recruitment. Among those recruited in Miami, a majority reported Cuba (43.1%) and Colombia (32.3%) as their country of birth, while among those who were not recruited in Miami, most reported the United States or Puerto Rico as their country of birth (57.9% and 18.4%, respectively). Hispanics from different countries may not only have various risks of developing AD (Mehta & Yeo, 2017) but also have different levels of knowledge of AD, which much be considered in future research.
Previous studies have found that racial and ethnic differences observed in AD knowledge is due to differences in educational attainment (Ayalon, 2013; Ayalon & Arean, 2004; Roberts et al., 2003). Differences in country of origin is important due to differences in educational attainment observed among these groups. A report by the Pew Research Center found that, among the U.S. Hispanic population, 13% of all Hispanics have at least a bachelor’s degree (Lopez, 2011). Within this, there are some differences by country of origin; 32% of Colombians, 30% of Peruvians, 24% of Cubans, 16% of Puerto Ricans, and 9% of Mexicans have at least a bachelor’s degree (Lopez, 2011). Most of the literature tends to focus on Hispanics as a whole, but due to the heterogeneity of this population, country of origin should be examined as well.
Although a majority of Hispanics in our sample were aware that high cholesterol or blood pressure are risk factors for AD, about half of the non-Hispanic Blacks and non-Hispanic Whites did not, indicating an area that should be targeted by public health campaigns. Norton and colleagues identified seven potentially modifiable risk factors for AD including diabetes, midlife hypertension, midlife obesity, physical inactivity, depression, smoking, and low educational attainment (Norton, Matthews, Barnes, Yaffe, & Brayne, 2014). In addition, a National Academy of Science, Engineering, and Medicine review determined that interventions for preventing onset and progression of dementia should focus on cognitive training, blood pressure management, and increased physical activity (National Academies of Sciences, Engineering, and Medicine, 2017). Therefore, education and intervention efforts should focus on hypertension prevention and control among individuals who are at risk for developing AD.
Furthermore, almost all Hispanics knew that individuals with AD are particularly prone to depression (93.3%), even though less than 30% of Hispanics in our sample self-reported depression. This is in comparison with a lower knowledge of this among non-Hispanic Blacks (76.3%) and non-Hispanic Whites (74.5%), even though non-Hispanic Whites have a significantly higher burden of depression (43.5%). Differences in the report of depression among minorities may potentially be due to disparities that exist in the recognition, diagnosis, and treatment of depression in underrepresented populations (Borowsky et al., 2000; Simpson, Krishnan, Kunik, & Ruiz, 2007).
Even though the higher knowledge observed among non-Hispanic Whites compared with non-Hispanic Blacks is consistent with the literature (Cahill et al., 2015; Connell et al., 2007; Connell et al., 2009; Gray et al., 2009; Roberts et al., 2003), it is an important area of intervention. Non-Hispanic Blacks carry a larger burden of AD and other dementias compared with Hispanics and non-Hispanic Whites (Alzheimer’s Association, 2018; Gurland et al., 1999; Haan et al., 2003; Potter et al., 2009), and interventions targeting AD knowledge are important and feasible (Fuller, Johnson-Turbes, Hall, & Osuji, 2012; Perales et al., 2018). In 2008, the Alzheimer’s Association implemented the Healthy Brain Initiative, to increase knowledge of AD among older non-Hispanic Blacks in Atlanta and Los Angeles (Fuller et al., 2012). The four core elements of the intervention included (a) developing partnerships with community organizations to promote brain health in the community; (b) conducting workshops to educate community members about brain health, risk factors, protective factors, and influence intentions to positively influence brain health; (c) holding educational community events to promote brain health and increase knowledge of protective and risk factors of good brain health; and (d) using mass media to disseminate information about brain health and relevant protective and risk factors (Fuller et al., 2012). Data were collected before, during, and after the intervention, and results showed that the intervention was effective in increasing knowledge, awareness, and intention to engage in health-promoting behavior (Fuller et al., 2012). Previous work has found that Black and Hispanic populations were more likely to report lifestyle changes to prevent AD compared with non-Hispanic Whites (Connell et al., 2007; Connell et al., 2009), suggesting that these interventions may be especially effective in racial and ethnic minority groups.
Limitations
A few limitations must be considered when interpreting the results of these analyses. The HealthStreet cohort is recruited through convenience sampling and, thus, our sample is not a representative sample of the U.S. population; however, the oversampling of African Americans and low-income populations is beneficial for these analyses given that these groups have a high burden of AD and other dementias. In addition, the country of ethnic origin is an important variable that should be included in future analyses of AD knowledge in Hispanic populations; however, the size of the study sample and the lack of a comprehensive group of Hispanic subpopulations inhibited any further analyses among Hispanics and AD knowledge. The low Cronbach’s Alpha of the abbreviated scale must also be noted. However, we wanted a less burdensome measure to reduce survey fatigue. Regardless of these limitations, HealthStreet CHWs collect real-time information on a wide variety of variables, including sociodemographic characteristics, health conditions, AD history, and AD knowledge. The HealthStreet cohort provides a unique opportunity to examine AD knowledge in a diverse community sample of middle-aged and older adults residing in Florida.
Conclusion
Given the high burden of AD in Hispanic and non-Hispanic Black populations, AD knowledge is essential to prevent risk factors for AD and to know when to seek help. The comparable AD knowledge observed between Hispanics and non-Hispanic Whites indicates that the heterogeneity of the Hispanic population in the United States plays a major role in the knowledge of AD among Hispanics. It is vital to increase educational interventions in non-Hispanic Blacks and subpopulations of Hispanics who have a lower knowledge of AD, as the number of older racial and ethnic minority group members increase in the United States.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Health Street, a community engagement program at the University of Florida, was approved by the University’s Institutional Review Board (Reference IRB201600459). Written informed consent was obtained from participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part through the National Institutes of Health’s Clinical and Translational Science Awards program, which is led by the National Center for Advancing Translational Sciences (UL1TR001427), by the Florida Alzheimer’s Disease Research Center (NIH P50 AG047266), sponsored by the National Institute on Aging, which governs Alzheimer’s Disease Research Centers through the National Alzheimer’s Coordinating Center, by the Florida Department of Health–Ed and Ethel Moore Alzheimer’s Disease Research Program (6AZ05), and by the Department of Epidemiology with funding from the College of Medicine and College of Public Health and Health Professions. Sadaf Arefi Milani was funded by the Graduate School Fellowship at the University of Florida for a portion of this work and is currently funded through the Training Grant T32AG000270 (PI Wong) from the National Institute on Aging/National Institutes of Health. Shawnta Lloyd is funded by the National Institute on Drug Abuse T32 training grant at the University of Florida Substance Abuse Training Center in Public Health from the National Institutes of Health (T32DA035167). The content is solely the responsibility of the authors and does not necessarily represent the official view of the National Institutes of Health.