
Abstract
Mental health is a challenging public health issue for Southeast Asians, who represent one of the most rapidly growing populations in the United States. (Hinton, Chhean, Pich, Hofmann, & Barlow, 2006; S. Lee & Chang, 2012). National estimates suggest that as a whole, Asians in the United States have rates of mental illness that are lower than those observed among members of the White population. However, trauma, low income, language barriers, and service obstacles may produce far higher rates of mental distress among some subgroups than others (Office of Minority Health [OMH], 2017). The pan-ethnic “Asian-American” group includes populations that are highly heterogeneous with respect to these attributes, and to health outcomes overall. For example, health outcomes are less favorable for the Hmong and Cambodian groups compared with other Southeast Asians, as well as in comparison with most other ethnic groups in the United States (Cho & Hummer, 2001; Yang, Burr, & Mutchler, 2012).
One of the least advantaged Asian American groups is the Hmong, a preliterate, agrarian ethnic group with multiple origin points. Those from highland Laos are among the most recent U.S. immigrant groups, arriving in the United States in large numbers beginning in 1975, after experiencing widespread trauma during the war in Vietnam (Mollica, Wyshak, & Lavelle, 1987; Westermeyer, 1987). Many of these refugees spent long periods of time inside refugee camps prior to entering the United States. Upon arrival in the United States as refugees, the Hmong encountered policies that dispersed them geographically throughout the United States. For many Hmong refugees, geographic dispersion resulted in cultural isolation and posed challenges to their mental health (Westermeyer, 1987). Thus, U.S. Hmong’s experiences are shaped by their traumatizing experiences in Laos, their refugee status, and their experiences in the United States. These experiences may be directly related to depression symptoms in later life.
Recent estimates suggest that currently, about 300,000 individuals reporting Hmong background live in the United States (U.S. Census Bureau, 2016). Although the Hmong population has been in the United States for more than 35 years, it is still a relatively unfamiliar group of people among health providers and other health professionals. Existing research on the older Hmong is limited, especially relating to mental health, and research on the mental health status of older Hmong populations in the United States is virtually absent. Although very limited evidence is available about their mental health characteristics, previous studies have reported higher disability prevalence among older Hmong compared with non-Hispanic Whites and to other Southeast Asians with a similar migration background (Cho & Hummer, 2001; Yang et al., 2012).
Prevalence of Depression and Mental Health Status Among Older Asian Americans
More than 30 extremely heterogeneous subgroups are embedded within the pan-ethnic “Asian American” category. These groups bring diverse histories, cultures, religions, languages, educational profiles, and immigrant stories to the United States (Kuo, Chong, & Joseph, 2008; Mui & Kang, 2006). Although diversity within Asian American communities is recognized, what minimal research exists tends to focus on the larger groups within this population. Specifically, research on older Asian Americans often examines health concerns among the five largest subgroups: Japanese, Filipinos, Chinese, Koreans, and Vietnamese Americans (B. J. Kim, Sangalang, & Kihl, 2012; G. Kim et al., 2010; Kuo et al., 2008; Mui, 1996; Mui & Kang, 2006). Consequently, little is known about health issues affecting smaller groups, like the Hmong.
Nonetheless, available literature illustrates that risk of depression varies substantially within segments of the older Asian American population. For example, one study based on data from California reports that older Korean immigrants report the highest rate of experience with severe psychological distress (4.5%) compared with older Asian immigrants from other origins (Filipino 3.1%, Vietnamese 2%, Chinese 1.9%, and Japanese 0.3%; G. Kim et al., 2010). A study that focused on Asian groups in Texas found a depression rate for middle-aged adults 55 years and older of 12.6% (Leung, Cheung, Kao, & Gulati, 2017), with substantial differences across Asian groups observed (Chinese 18.5%, Vietnamese 14%, and Taiwanese 6.8%). Differences in mental health status between Asian groups and non-Hispanic Whites have also been documented. Specifically, older Filipino and Korean Americans were more likely to self-report psychological distress compared with older non-Hispanic Whites; however, older Japanese Americans reported lower levels of psychological distress than non-Hispanic Whites (Sorkin, Nguyen, & Ngo-Metzger, 2011). Data from the Centers for Disease Control and Prevention (CDC) for adults similarly suggests that among Asian American origin groups, rates of serious distress are highest among Filipino and Vietnamese adults (OMH, 2017). Yet, rates of distress among “Other” Asian American adults—a catch-all category that includes the Hmong along with many other small populations—are even higher than the rates reported for Filipino or Vietnamese adults.
Factors Contributing to Depression Among Older Immigrants
Aside from the characteristics known to shape depression risk in general, including gender (Alexopoulos, 2005; Unützer et al., 2003) and marital status (Bell et al., 2005), older immigrants face additional risk factors relating to stresses associated with their status. Older adults with limited education and lower income have a higher risk of depression (Bell et al., 2005), and immigrants are exposed to these risks at elevated levels. Older immigrants are less likely to have had jobs that provided a pension or a sufficiently long work history in the United States to receive Social Security (Mui, Nguyen, Kang, & Domanski, 2007; Mutchler, Prakash, & Burr, 2007) and a consistent link between immigrant status and low income has been established (Mui et al., 2007). Indeed, poverty has been shown to be a serious and harmful stressor for older immigrants (Cuellar, Bastida, & Braccio, 2004).
As well, older Asian immigrants are at high risk for experiencing poor health and disability outcomes that may be stressful. For example, several cross-sectional studies suggest that poor health is associated with depression among older community-dwelling Chinese immigrants (Dong, Chang, Wong, & Simon, 2012; Leung et al., 2017; Mui, 1996, 1999). In a disability prevalence study among middle-aged and older Southeast Asians groups in the United States, Hmong and Cambodian groups were shown to be more likely to suffer from sensory deficit, functional limitation, and disability compared with Vietnamese immigrants (Yang et al., 2012), potentially placing this group at high risk of the negative mental health consequences associated with poor physical health.
Vulnerability relating to exclusion and lack of social support may also impact risk of depression among older immigrants. Many older Southeast Asian immigrants have limited English proficiency, which may contribute to depression risk. In the absence of having proficient English, older immigrants may be reliant on an adult child for interpretation, be socially excluded, and be linguistically isolated. Research has demonstrated repeatedly that older Asian immigrants who have limited English proficiency were more likely to be depressed (Casado & Leung, 2002; Mui & Kang, 2006).
As well, collectivism is often considered to be a key value among immigrants and refugees (Park & Bernstein, 2008), and in Asian American communities, many older adults are expected and prefer to live with an adult child, often preferably a son (E. Lee, 1996; Mui et al., 2007; Park & Bernstein, 2008). Although social support norms in Asian American communities have begun to resemble that of the Western culture, with networks increasingly extending to friends and neighbors (Diwan, Jonnalagadda, & Balaswamy, 2004; Pang, Jordan-Marsh, Silverstein, & Cody, 2003), older immigrants may experience intergenerational conflicts through living arrangements or may be disappointed by their unmet filial piety expectations from their children (Leung et al., 2017; Mui, 1999). The contours of social support in this population are constantly evolving and may serve as stressors leading to depression for older refugees and immigrants, especially those who still hold a strong tie to their culture or have a more recent immigration history.
Depression Among Aging Hmong Immigrants
Existing research on depression among Hmong immigrants to the United States was conducted primarily in the 1990s (Kinzie et al., 1990; Kroll et al., 1990; Westermeyer, 1987), focusing on this population at midlife. At the time that research was conducted, the typical Hmong adult had lived in the United States for about 15 years, and high levels of depression were observed. Most Hmong refugees are now elderly, yet no literature exists on their current mental health status. This may be related to the small size of the population in the United States, coupled with additional barriers such as low literacy (e.g., many are unable to fill out questionnaires on their own), and culturally related barriers such as attitudes toward suffering and beliefs toward illness (Uba, 1992). Attitudes and beliefs about seeking mental health services prevalent in the Hmong population are influenced by ideas that illness is an unavoidable part of life, and one’s life and time of death are predetermined (Uba, 1992). Thus, these culturally related barriers negatively impact mental health utilization for Hmong immigrants (Leong & Lau, 2001; Uba, 1992).
This study offers updated information on the mental health status of aging Hmong immigrants, based on original data collected in Minnesota and California. This exploratory study has two goals. First, given the literature documenting high levels of depression and posttraumatic stress disorder at midlife in this population, we seek to determine whether elevated depression symptoms are observed among later life Hmong in the United States. Our second goal is to determine whether characteristics typically associated with depressive symptoms among older Asian immigrants in general account for variability in risk within this population. Based on prior literature focusing on older Asian immigrants, we expect that literacy levels, English language skills, education levels, gender, marital status, living arrangements, and physical health status would be associated with depressive symptoms.
Method
The Hmong population is heavily concentrated in California and Minnesota. California is the most densely populated, with 34% of the Hmong population residing in that single state, and Minnesota (26%) has the second largest number of Hmong residents (U.S. Census Bureau, 2016). These two states served as the data collection sites for this study, which was conducted in 2016 from March to August. To maximize recruitment, within each state, the researchers sought to recruit participants from counties identified as “high-density” with respect to the Hmong population, based on the 2010 Census (U.S. Census Bureau, 2010). High-density counties were targeted because, in general, locally organized Hmong organizations are prominent fixtures where a large proportion of Hmong exist. Subject recruitment was facilitated by contact with these Hmong organizations. In each of the identified counties, the first author reached out to the Hmong organization leaders, who served as cultural brokers, trusted authorities in the community, and the voice of the community.
Sample
The lead author contacted households that were identified by community leaders as including older Hmong residents. Community leaders also suggested public local events and community centers as places for participant recruitment. All individuals identified as meeting the screening eligibility (55 years of age or older and self-identifying as Hmong) were invited to voluntarily participate in the study (no compensation was given). In addition, the researcher sought permission from each community leader to administer the questionnaire at his or her community center to eligible participants. Participants who were not available to be interviewed at their local center, or who did not wish to be interviewed there, were interviewed in his or her home. Participants were first asked about their demographic information and then the HSCL-10 inventory. Interviews ranged in length from 5 to 10 min. About 40 individuals who were asked to participate refused to be interviewed for the study, but a total of 130 individuals agreed to participate. The final N for this study was 127.
Although the HSCL-10 is a self-administered inventory, rates of literacy in both English and Hmong are low in this population. Consequently, the lead researcher gave participants the option to fill the inventory out on their own or with the researcher’s assistance. Nearly all of the participants required assistance, which was provided by the lead researcher; only three participants completed the inventory on their own. All of the assistance was provided in the Hmong language.
Measures
Depressive symptoms
A depression scale specifically for the Hmong population has not been established. The Hopkins Symptom Checklist–25 (HSCL-25) has been previously validated in the Hmong population, but is not readily available to the public (Mouanoutoua & Brown, 1995). The HSCL-10 inventory instrument is a widely used condensed version of the HSCL-25 and is considered to represent a strong balance between ease of administration and accuracy of assessment (Kleppang & Hagquist, 2016). The HSCL-10 questionnaire has been validated in various populations and is actively used in the medical and social science fields (Syed, Zachrisson, Dalgard, Dalen, & Ahlberg, 2008). Given the Hmong population’s low literacy levels, the time burden required for these older individuals to fill out the HSCL-25 would be excessive; a short form is therefore beneficial (Yeung et al., 2008). Accordingly, in this study, the researchers used a Hmong-language HSCL-10 instrument that was developed based on standard practice (translated from English to Hmong and then backward translated to English) by researchers from University of California, Davis and University of California, Davis Medical Center. Although this Hmong-language instrument has yet to be validated, the items included have been shown to be valid in many other studies and languages.
The dependent variable used in this study was the mean response on the HSCL-10, calculated for each respondent by summing item responses and dividing by 10. Eleven people declined to respond to between 1 and 4 of the HSCL-10 inventory; for these individuals a modified mean score was created by summing their scores across the questions that were answered, and dividing by the total number of answered items. An additional three respondents declined to answer at least five of the HSCL-10 inventory; these individuals were omitted from the study. In this sample, the Cronbach’s alpha was .77, suggesting that the HSCL-10 was reliable.
Demographics
A number of social, demographic, and culture-specific indicators were collected as potential correlates. State of residence is a dichotomous variable in which 1 = California and 0 = Minnesota. Age was based on reported age in years. Gender was based on the following question: “What is your gender” (1 = female, 0 = male). Marital status was based on the following question: “What is your current marital status?” (1 = married, 0 = widowed, separated, divorced, or never married). As well, household size was assessed based on this question: “Including yourself, how many people are currently living in your home?”
Socioeconomic status was measured with reference to education and employment status. The participants were asked, “What is your highest level of education?” As very few participants had more than a nominal level of school, a dummy variable was coded as 1 = no school, 0 = 1 or more years of formal schooling. Employment status was assessed by asking participants “Which best describes your employment situation?” (1 = not in labor force, that is, retired, homemaker, disabled, or other; 0 = in labor force, that is, employed, self-employed, looking for work, or unemployed).
Adaptation to the United States was assessed based on immigration timing, capacity to speak English, and literacy. Location of birth was measured from the following question: “Where were you born?” All of the participants were born in Laos. This question confirms the immigrant status of all participants but was not used in the analysis. Age at which the respondent entered the United States was identified by response to “How old were you when you first came to live in the U.S.?” Participants’ abilities to speak and read English were measured based on two questions: “How well do you speak English?” and “How well do you read English?” with response options including “Not at all,” “Poorly,” “Average,” or “Well.” Thirteen participants indicated they could speak English “average” or “well,” but more than 90% of the sample spoke English poorly (n = 22) or not at all (n = 92). An overwhelming majority reported their English literacy level was poor (n = 11) or that they could not read at all (n = 103). Only a small number of participants reported that they could read English either at an average level (n = 9) or well (n = 4). Because an overwhelming share of the participants indicated their English language skills were poor or absent, these variables were each coded as 1 = not at all, 0 = poor, average, or well. Thus, the coding represents those having any English language skills (0) compared with those with none (1).
As noted above, the literature identifies a strong association between physical health and mental health, including depression. In this study, self-reported physical health was assessed to determine the extent to which measured depression levels are associated with health status. Self-reported health was measured with the following question: “How would you rate your overall physical health?” (1 = poor, 0 = good, excellent).
Imputed Variables
Three demographic variables had missing responses, including current age, age entered the United States, and household size. Multiple imputation methods were used to impute values in these cases. Following Graham, Olchowski, and Gilreath (2007), this study conducted 20 iterations of imputed data; the imputed value used in analysis was the average across the 20 iterations (further information on our imputation approach is available upon request).
Statistical Analyses
An ordinary least squares multivariate regression model was estimated. The model included variables for state of residence, age, gender, marital status, education, labor force status, age entered the United States, English literacy and speaking abilities, number of residents in the household, and self-reported physical health. We also conducted a sensitivity analysis based on a dichotomous coding of depression, using a cutoff of 1.85 or higher HSCL-10 score as being symptomatic of depression (see Haavet, Sirpal, Haugen, & Christensen, 2011, and Syed et al., 2008) for discussion of this cutoff. Logistic regression results based on that analysis were similar to the multivariate regression models (further detailed results can be shared upon request). In addition, we also looked at self-reported mental health status for sensitivity analysis. We found self-reported mental health was a significant association, suggesting that self-assessment aligned with the formalized measurement using the HSCL-10.
Results
Descriptive findings suggest that older adults in this sample have high levels of depressive symptoms on average. Previous studies with the HSCL-25 items instrument used a cut point of 1.75 to indicate being symptomatic for depression and/or anxiety (Winokur, Winokur, Rickels, & Cox, 1984). Studies using the HSCL-10 have used thresholds of 1.6 to 1.85 to indicate being symptomatic for depression (Haavet et al., 2011; Hoxmark, Nivison, & Wynn, 2010), and a cutoff score of 1.85 on the HSCL-10 has been shown to be valid among adolescences and young adults (Hoxmark et al., 2010; Strand, Dalgard, Tambs, & Rognerud, 2003). In this study, we follow past practice and consider a score of 1.85 or higher to indicate being symptomatic for depression.
As shown in Table 1, the sample mean on the HSCL-10 is 2.23, considerably higher than the conventional benchmark of 1.85 to indicate being symptomatic for depression (Haavet et al., 2011; Hoxmark et al., 2010). Sociodemographic and cultural characteristics of the sample make clear that this sample has low socioeconomic status, few English language skills, and poor health. A majority of the sample has no formal education (87%), is not in the labor force (91%), has no literacy (81%), has no English language skills (72%), and reports poor physical health (68%). The average age for this sample is 71 (SD = 11.89) and mean time lived in the United States is 29 years (SD =11.69). The average age when entering the United States is 43 (SD = 15.09). Half of the sample are married, most are female (76%), and just more than half live in Minnesota (56%).
Descriptive Characteristics of the Sample.
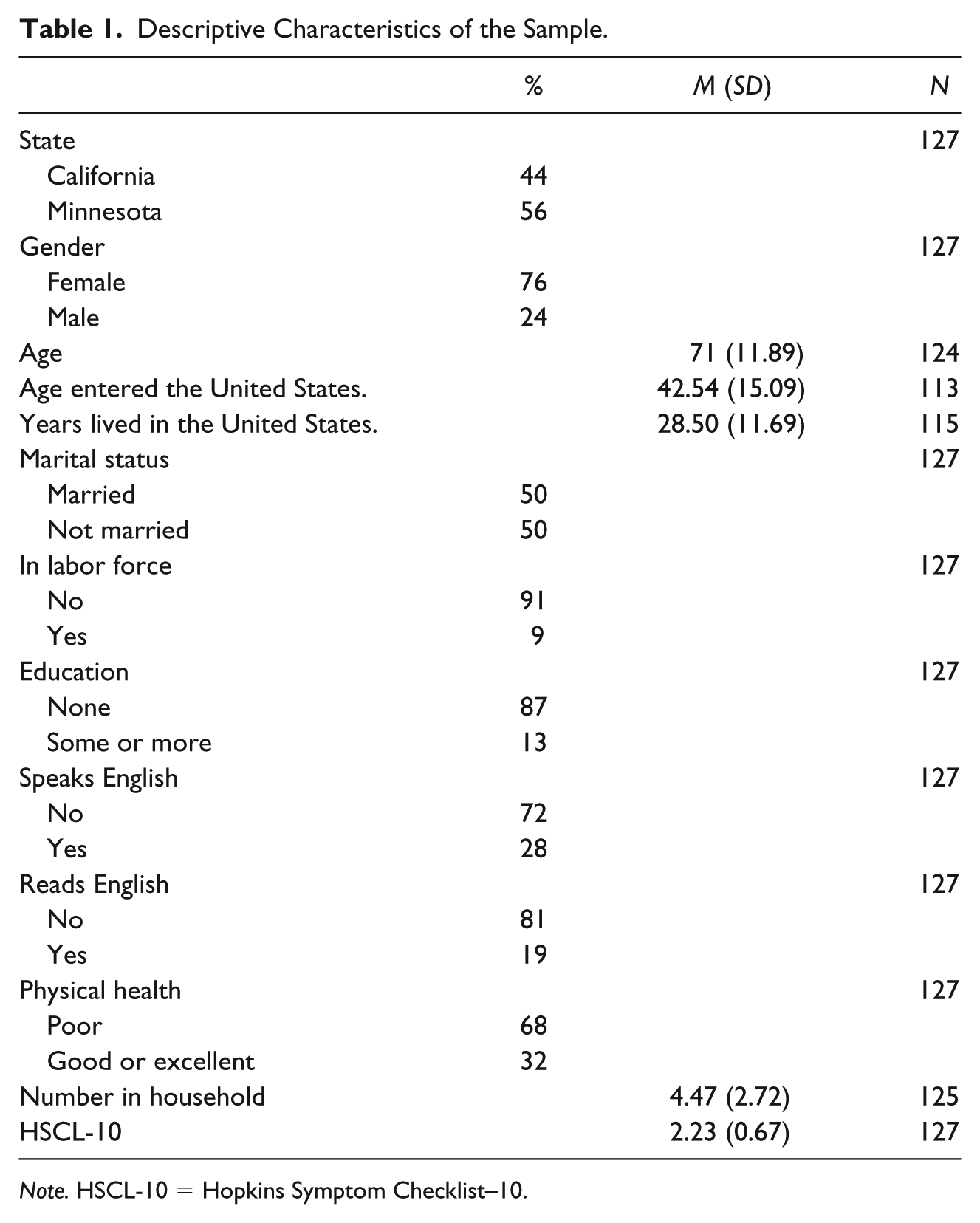
Note. HSCL-10 = Hopkins Symptom Checklist–10.
HSCL-10 Scores and Correlates
Table 2 describes the scores calculated for the HSCL-10 scale, along with the mean scores for each of the HSCL-10 inventory. Some items yield scores below the HSCL-10 mean, including feeling “suddenly scared” or “fearful,” reflecting lower endorsements on these items. In contract, considerably higher average scores were observed for other items, including “feeling tense or keyed up,” “difficulty in falling asleep or staying asleep,” “feeling everything is an effort,” and “feeling hopeless about the future,” suggesting that these aspects may reflect special aspects of strain or depressive symptoms in this population.
Means of HSCL-10 Inventory.
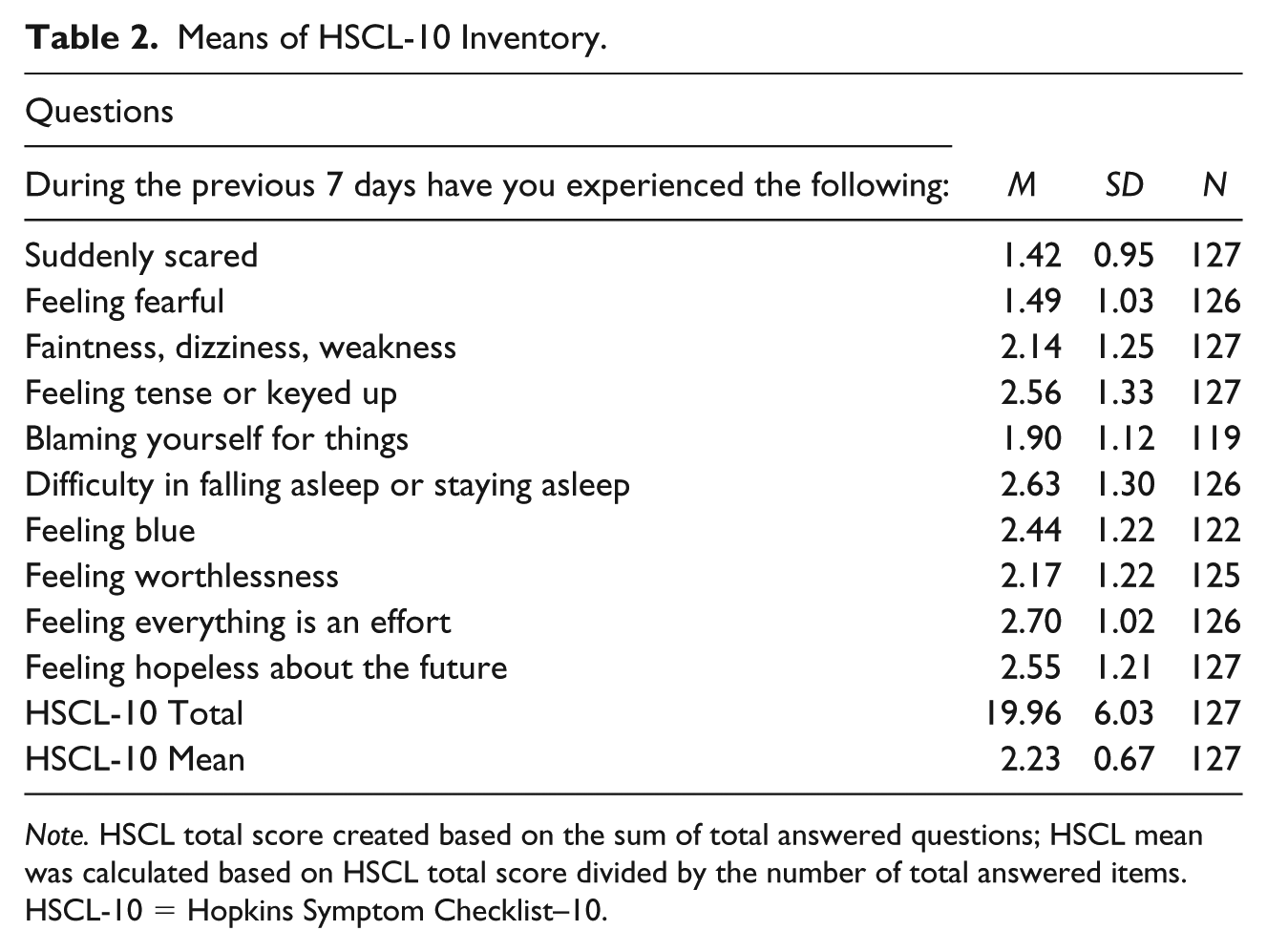
Note. HSCL total score created based on the sum of total answered questions; HSCL mean was calculated based on HSCL total score divided by the number of total answered items. HSCL-10 = Hopkins Symptom Checklist–10.
Table 3 presents the mean HSCL-10 scores for subgroups along with statistics describing independent sample t tests. Continuous variables were categorized at the mean for this illustration. Statistically significant group differences in depression levels were found based on gender (with females reporting significantly more depressive symptoms), formal education (with those having no formal education reporting more symptoms), labor force status (respondents not in the labor force reported significantly more depressive symptoms), age entering in the United States (with respondents above the mean age at entry reporting fewer depressive symptoms), ability to speak English (with those who speak any English having more depressive symptoms), literacy skills (those literate in English have significantly more depressive symptoms), and physical health (respondents reporting poor health have significantly more depressive symptoms). No zero-order differences in depression were established for state of residence (California vs. Minnesota), age, marital status, and household size. Most of the effect sizes, based to Cohen’s d, are small (Cohen’s d below 0.50), with gender, literacy, and physical health having moderate effects (Cohen’s d of 0.5-0.79) (Cohen, 1988). For this study, only the labor force status had a high effect (Cohen’s d of 0.8 or greater).
Mean Depression Score Significance of Differences, Older Hmong Refugees.
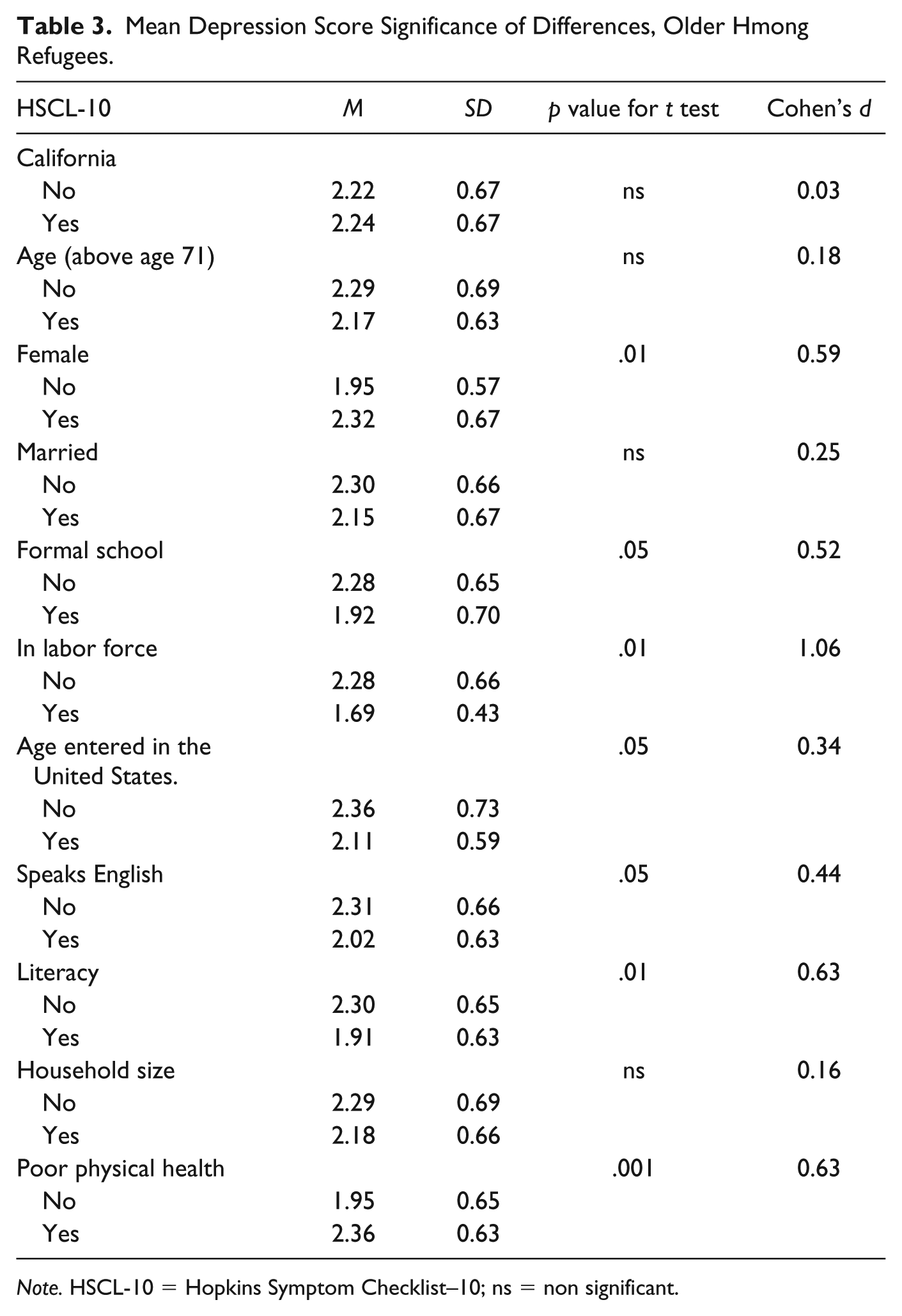
Note. HSCL-10 = Hopkins Symptom Checklist–10; ns = non significant.
Multivariate Regression Results
A multivariate analysis suggests that sociodemographic differences among members of this sample were largely not impactful in explaining variability in depressive symptoms, all else held constant (see Table 4). Some significant findings are notable, however. Age when respondent entered into the United States had a negative impact (b = −.01, p < .05), suggesting that those who entered the United States at an older age had slightly lower scores on the HSCL-10. Having more household members was also significant as a protective factor from depressive symptoms (b = −.04, p < .05). Respondents who are not in the labor force reported more depressive symptoms (b = .40, p < .10). As well, those who evaluated their physical health as poor reported significantly more depressive symptoms (b = .34, p < .01). These findings suggest that with a few exceptions, the characteristics of the older Hmong sample captured in this study largely do not account for variability in number of depressive symptoms; variability which, as discussed above, is fairly low.
Regression Analysis for Depression (N = 126).
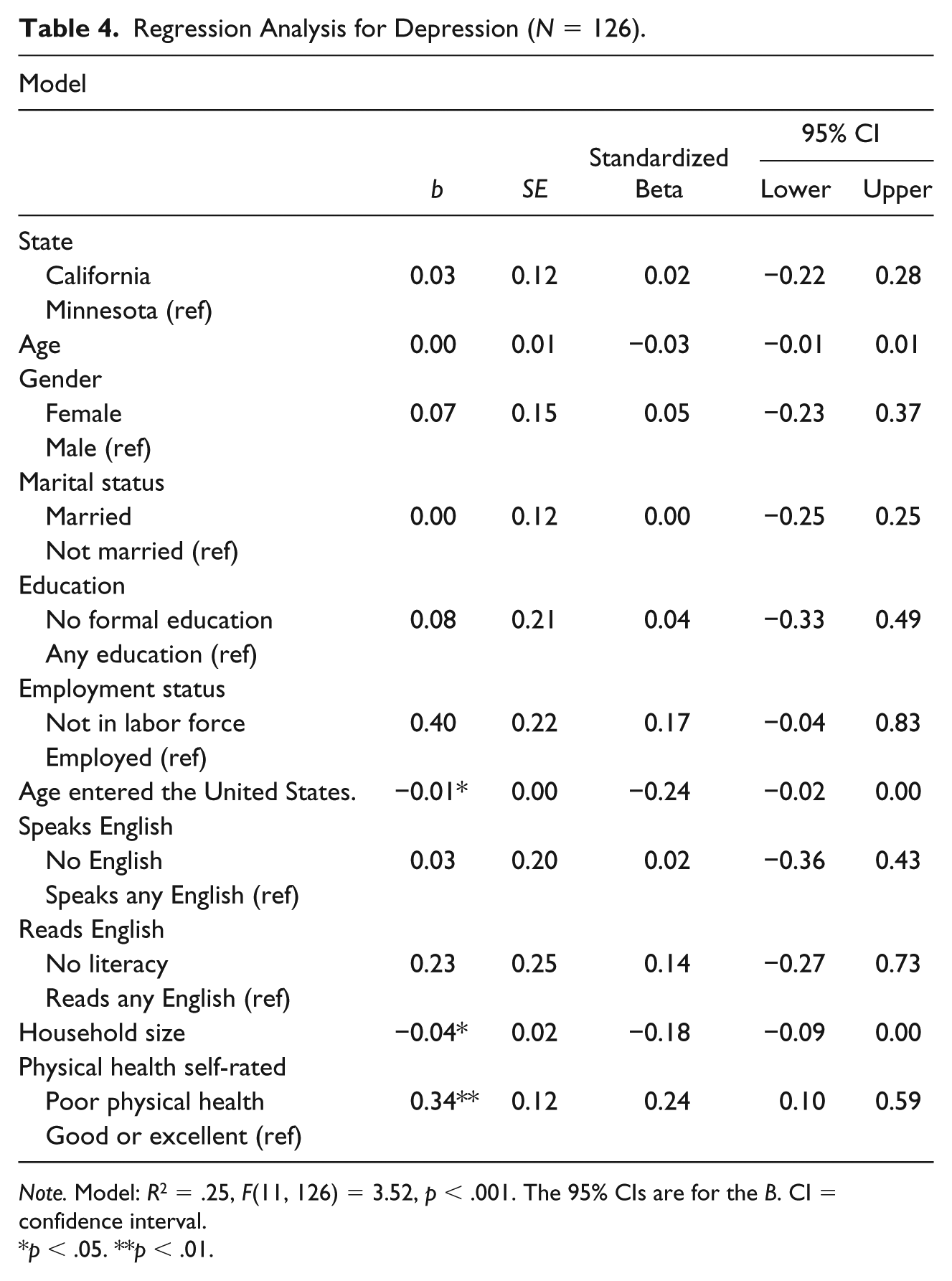
Note. Model: R2 = .25, F(11, 126) = 3.52, p < .001. The 95% CIs are for the B. CI = confidence interval.
p < .05. **p < .01.
Discussion
This study’s goal was to examine levels of and factors relating to depression among older Hmong immigrants. The most important finding of this study may be our estimation of very high levels of depressive symptoms in this sample. According to this study, and based on the HSCL-10 cutoff score of 1.85, as has been used in previous studies, nearly three quarters of participants had scores symptomatic of depression. Previous studies assessing the Hmong refugees’ mental health status suggest that this population was characterized by high rates of depression earlier in life, when this population was in their mid-30s during the 1980s (Kroll et al., 1990; Westermeyer, 1987). Our study suggests that in later life, depressive symptoms remain at similarly high levels. This finding is noteworthy as mental illness is often underreported or poorly assessed for the Hmong population. Based on the research conducted for this study, we conclude that this refugee population continues to experience a high risk for depression.
We find that a protective factor from high depressive symptoms is having membership in a large household. Having a large household may reflect having a social network and social support. Thus, these factors may serve as a buffer against endorsing depression in later life within this sample of older Hmong refugees. In this sample, the households are large (more than four members on average) even though the average age of the respondents is 71, suggesting that the households are multigenerational and likely include multiple adults, as well as perhaps grandchildren. Limited research has focused directly on the association between household size and depressive symptoms, specifically in later life; instead the focus is often on either living alone or living with another adult, for example, spouse/partner, adult child(ren). Thus, we cannot determine whether our finding on the positive effect of larger household size is comparable with previous studies. However, we know that multigenerational families are valued among Hmong and other Asian elders, so we may expect that this finding could hold more generally among other ethnic groups that share strong familistic norms.
The findings on age entering the United States suggest that coming at an older age was a protective factor from depressive symptoms in later life. This finding is in contrast to previous studies on other Asian immigrant groups; for example, one study looked at age at immigration and mood disorder among Asian immigrants and found those who entered after age 25 were more likely to suffer from a mood disorder compared with those who arrived at younger than 25 years old (Leu et al., 2008). Notably, all respondents in this study entered the United States as adults, with an average age at entry of 42 years. Thus, the discrepancy between our findings and those reported elsewhere may be a function of the older age at which these study respondents arrived. As well, differences associated with age at entry could reflect family reunification processes or other factors resulting in reestablished family ties, which may impact risk of depressive symptoms in our sample.
Our findings also suggest that older Hmong who self-assess being in poor physical health are also at risk for depressive symptoms. This finding is similar to other studies on older Asian Americans (Dong et al., 2012; Leung et al., 2017; Mui, 1999; Mui & Kang, 2006) and on the general older adult population (Alexopoulos, 2005). This finding is important because it strengthens the current literature on the association between poor health and depressive symptoms among the Asian immigrant population in later life, and specifically updates the current mental health status and presenting associations of depressive symptoms among older Hmong immigrants.
In addition to the very high levels of depressive symptoms observed, perhaps the most striking finding is that relatively few of the characteristics of the older Hmong refugees included in this study are statistically related to depressive symptoms. The mean score of the HSCL-10 was 2.23 with a low standard deviation (.67) suggesting that the depressive symptoms are high with low variability. The low level of differentiation associated with these characteristics may be a result of the sample sharing in common a high risk of depressive symptoms, along with common life experiences and characteristics that place most of the study participants at risk. As a result, identifying factors that influence depressive symptoms may have been hard to detect within this sample, which was quite homogeneous in many respects. Yet the high estimated level of depressive symptoms, in combination with the high percentage of limited English proficiency characterizing members of this sample, suggests that effectively meeting the mental health needs of this population requires language-appropriate provision of mental health services.
Limitations
As with any study, this study had limitations. First, data from this study are focused on older Hmong adults from California and Minnesota. Hmong refugees residing in other parts of the United States may have different experiences and characteristics. For example, California was more advanced in passing bills and creating policies that were culturally appropriate for the Hmong community once they started arriving in California, which might have resulted in more appropriate services for this population. However, it is noted that in the study, no significant differences in HSCL-10 score were found between California and Minnesota participants. Hmong who do not live in either of these high-density states may be exposed to factors producing higher, or lower, risks of depression.
Another limitation of this study is the potential selectivity in response. Those who declined or did not complete the survey may differ in meaningful ways from those who participated: For example, they could have especially high depression levels or, alternatively, could have a strong Hmong community connection and better mental health status. The data collection process itself posed another limitation as the majority of the respondents were literate in neither Hmong nor English and the primary researcher administered the survey. This strategy, although unavoidable, may have resulted in a potential response bias.
These data were collected at a single point in time and therefore cannot inform our understanding of causal relationships leading to depression. While some of the variables have clear causal order (e.g., age at arrival in the United States precedes our assessment of depressive symptoms), the causal ordering of some other variables is unclear. For example, it is possible that those who self-reported as having higher depressive symptoms were more inclined to perceive their physical health as poor. Thus, some effects could be bidirectional and causality was not established in this exploratory, cross-sectional study.
A final limitation of the study is that the items reflected a Western understanding of mental health concepts. As noted above, no depression scale specifically for the Hmong population has been developed. Indeed, a few of the participants did have difficulty understanding some of the items. Several items required further explanation, such as “feeling worthlessness” and “feeling blue.” The item “feeling worthlessness” was often repeated twice and apparently understood by some respondents as “feeling that you have no value,” with the word “value” in this context perceived as having net worth. The question “feeling blue” was difficult to convey as the concept “blue” is not a common expression for this population. In a forthcoming paper, we examine in-depth how older Hmong adults experience and understand depression in later life.
Conclusion and Future Direction
To date, no study has reported on depression among older Southeast Asian refugees, let alone among older Hmong. Findings from this study contribute to the much-needed literature on aging minorities and mental health, and establish the extraordinarily high levels of depression among members of this population
Currently, there is no fully validated instrument for mental health status or depression for the older Hmong population. Thus, a future goal would be to fully validate the HSCL-10 on a larger sample including older Hmong refugees living in different states. This study did not measure trauma but one could assume that given their refugee status, much of the sample would have been exposed to significant trauma. The experiences of adversity and trauma have been found to be associated with poor subjective well-being in later life (Barnes et al., 2012). A future direction for this study is to measure the association between trauma and subjective well-being for older Hmong immigrants. In addition, future study could focus on the importance of family and intergenerational household structure for this population on later-life mental health, as family is a primary social network and a key mechanism by which cultural structure and roles are maintained.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this study was supported by the National Institutes on Aging—National Institutes of Health under award number: R36 AG049059-01A1.