
Abstract
Introduction
Dementia is surrounded by stigma associated with memory loss particularly in older adults which results in social isolation. It is also associated with long-term care placement, high health care costs, functional dependency, serious behavioral problems, mortality, and reduced quality of life (QoL). Almost 42% and 40% of people with dementia (PwD) in the United States and in the United Kingdom, respectively, live in assisted living facilities (limited assistance with daily activities), long-term care facilities (LTCFs; skilled nursing care with daily activities), and residential care facilities (nonmedical care in home-based setting); (Alzheimer Disease International, 2018). A distinct form of memory care, which can be found in dementia special care units, specifically focuses on long-term skilled nursing care services not only for activities of daily living (ADL) but also for serving people with Alzheimer’s disease, dementia, and other types of memory problems or cognitive impairment. Globally, the number of PwD is expected to rise to 65.7 million in 2030 and 115.4 million in 2050, and more than 90% of all cases are diagnosed over the age of 65 years (Carrillo, Thies, & Bain, 2012). Improving QoL has become the focus of dementia care outlined by the Alzheimer’s Association (Fazio, Pace, Maslow, Zimmerman, & Kallmyer, 2018), so identifying factors associated with QoL such as positive social interaction is essential. The environmental design research literature has established the importance of social interaction and social network as one of the therapeutic goals to maintain QoL in PwD (Fleming & Purandare, 2010; Garcia et al., 2012).
When caregivers are unable to take care of a family member who is suffering from dementia, it is common to transfer the patient from home to a care institution. This transition can impact the QoL of PwD mainly because of the changes in the physical environment and associated social interaction (Moyle, McAllister, Venturato, & Adams, 2007). To successfully improve the QoL of PwD via interventions, positive social interaction is considered a relevant outcome. For elderly PwD, changes in their social or physical environment or manifestations of dementia may influence their QoL, and it is therefore imperative to understand the relationships between physical environment and social interaction (Figure 1).
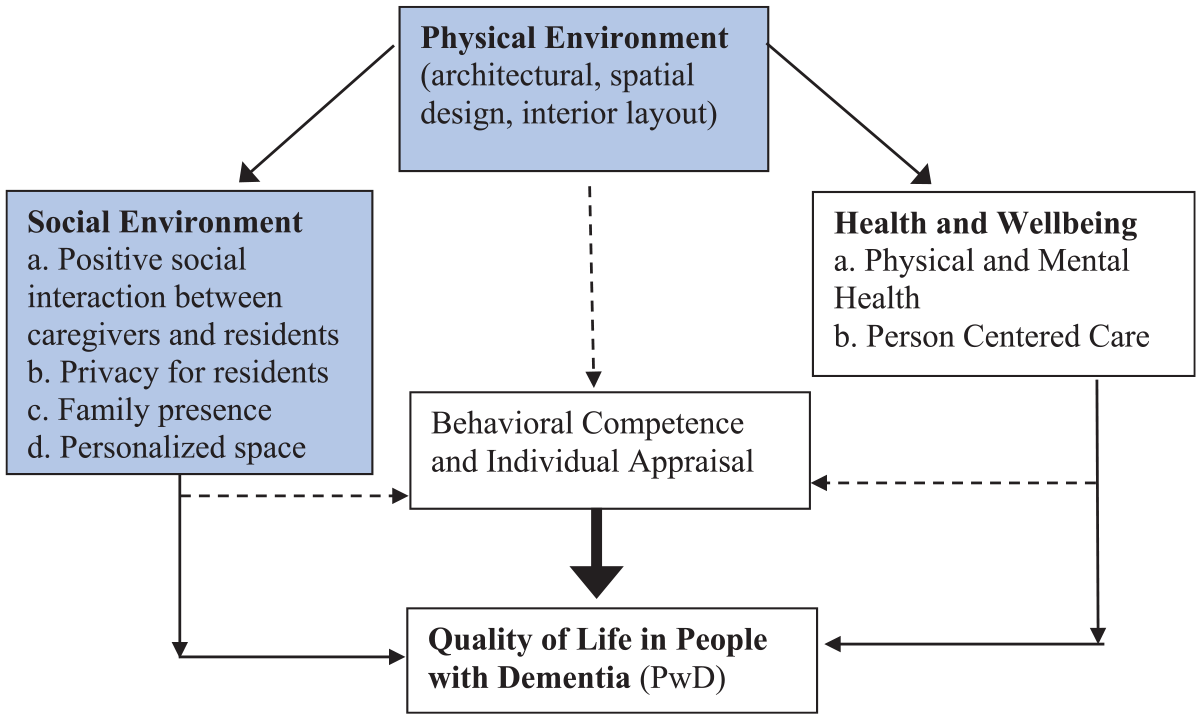
A causal model of factors influencing quality of life in people with dementia (highlighted factors are addressed in this study).
Memory, psychosocial need, comfort, desires, and time spent indoors with family members are different aspects of the human condition upon which architectural design are largely influenced. This holds true for PwD, and the design of memory care or LTCFs for PwD ought to be considered from a social justice perspective with a desire to give voice to marginalized older adults and mentally frail populations. The design of such care facilities needs specialized knowledge, professional experience, person-centered approaches, and careful consideration of the inhabitants’ lifestyles. By keeping in mind the personal experiences and lifestyles of dementia residents, the design of care facilities could be more interactive and engaging where space could facilitate better social interaction.
A growing number of studies are examining the relationship between the different physical characteristics of spatial design and social interaction, confirming the importance of these factors in memory care facilities for PwD. The objective of this systematic review is to comprehensively outline a set of factors related to the spatial design of LTCF that may influence positive social interaction and subsequently QoL in PwD. More specifically, this study aimed to systematically review the factors influencing positive social interaction that could be affected by changes in architectural design, interior layout, and physical environment of the facility. Although several reviews of the empirical literature have been conducted previously to understand the physical environment and associated QoL in LTCF of PwD (Chaudhury, Cooke, Cowie, & Razaghi, 2018; Chaudhury, Hung, & Badger, 2013; Chaudhury, Hung, Rust, & Wu, 2017;Forsund & Ytrehus, 2016; S. Lee, Chaudhury, & Hung, 2016a, 2016b; Nordin et al., 2017), no single study concentrated on the role of spatial design in positive social interaction. Therefore, this review also aimed to fill this gap and contribute to a better understanding of how “positive social interaction,” one of the most important determinants of QoL for PwD, could be influenced by different spatial designs and environmental characteristics.
Method
A “systematic review” uses systematic methods to collect secondary data from research studies (such as quantitative, qualitative, or experimental studies and randomized controlled trials) and synthesize findings both qualitatively and quantitatively (Armstrong, Hall, Doyle, & Waters, 2011). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009 guidelines (Moher, Liberati, Tetzlaff, Altman, & PRISMA Group, 2009) were employed for this systematic review. PRISMA is an evidence-based set of guidelines for reporting systematic reviews and meta-analyses specifically assessing health care interventions; the guidelines consist of a 27-item checklist and a four-phase flow diagram.
Search Strategies and Study Selection
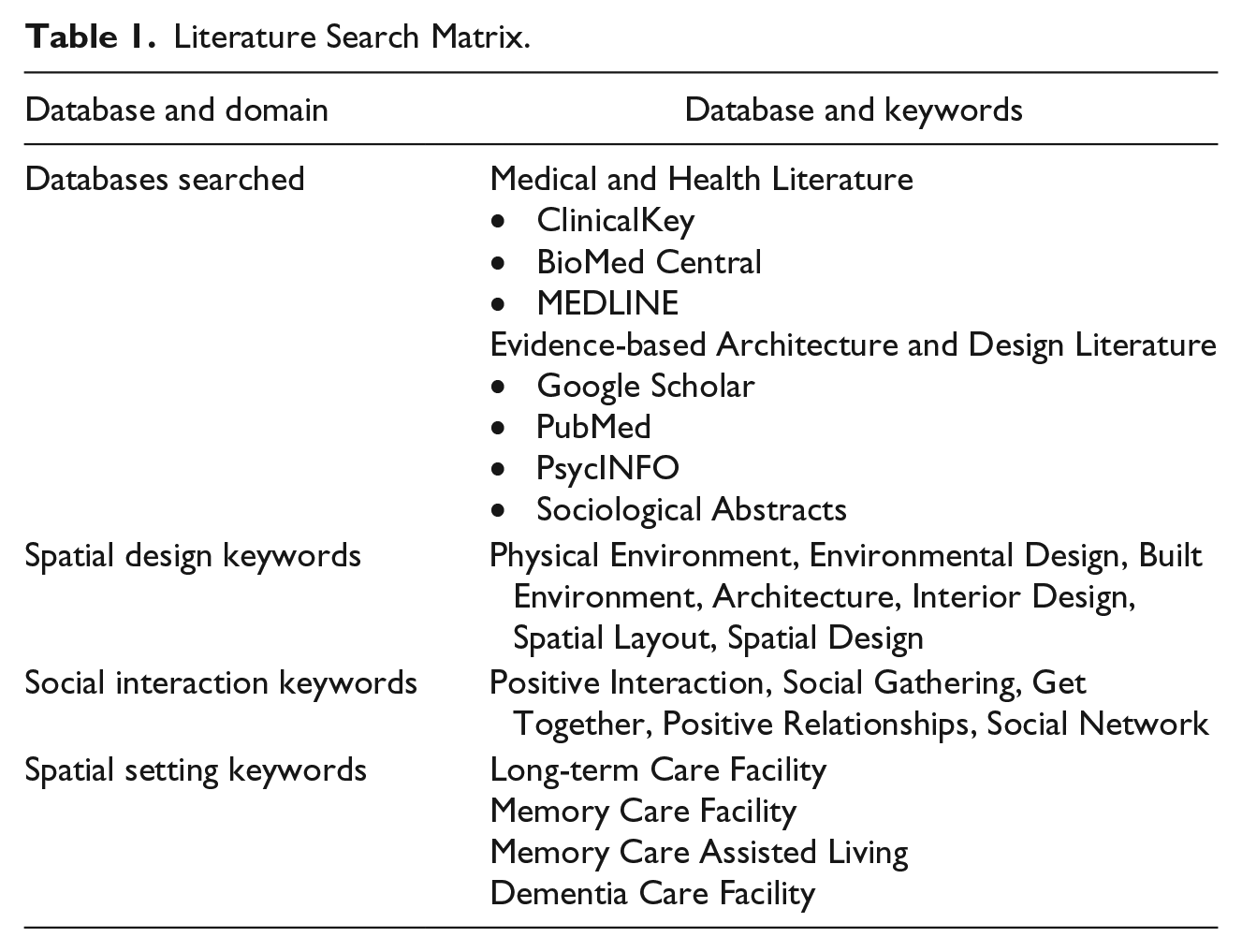
To identify spatial design factors potentially influencing positive social interaction for elderly (i.e., more than 65 years of age) PwD, the author conducted a systematic keyword search within major research databases to identify the relevant studies. Seven databases from two distinct disciplines, medical and health literature or evidence-based architecture and design literature, were included in the search strategy (Table 1). The keywords used to search for relevant articles were categorized into three different domains: spatial design, social interaction, and spatial settings (i.e., care facility; Table 1). Each search included one keyword from each domain so that results reflected all relevant aspects for the review.
Literature Search Matrix.
A total of 988 articles were initially identified from the database search (Figure 2). The inclusion and exclusion criteria were used for screening and eligibility, respectively (Table 2). A total of 51 full-text items were identified for inclusion in the systematic review (Figure 2).
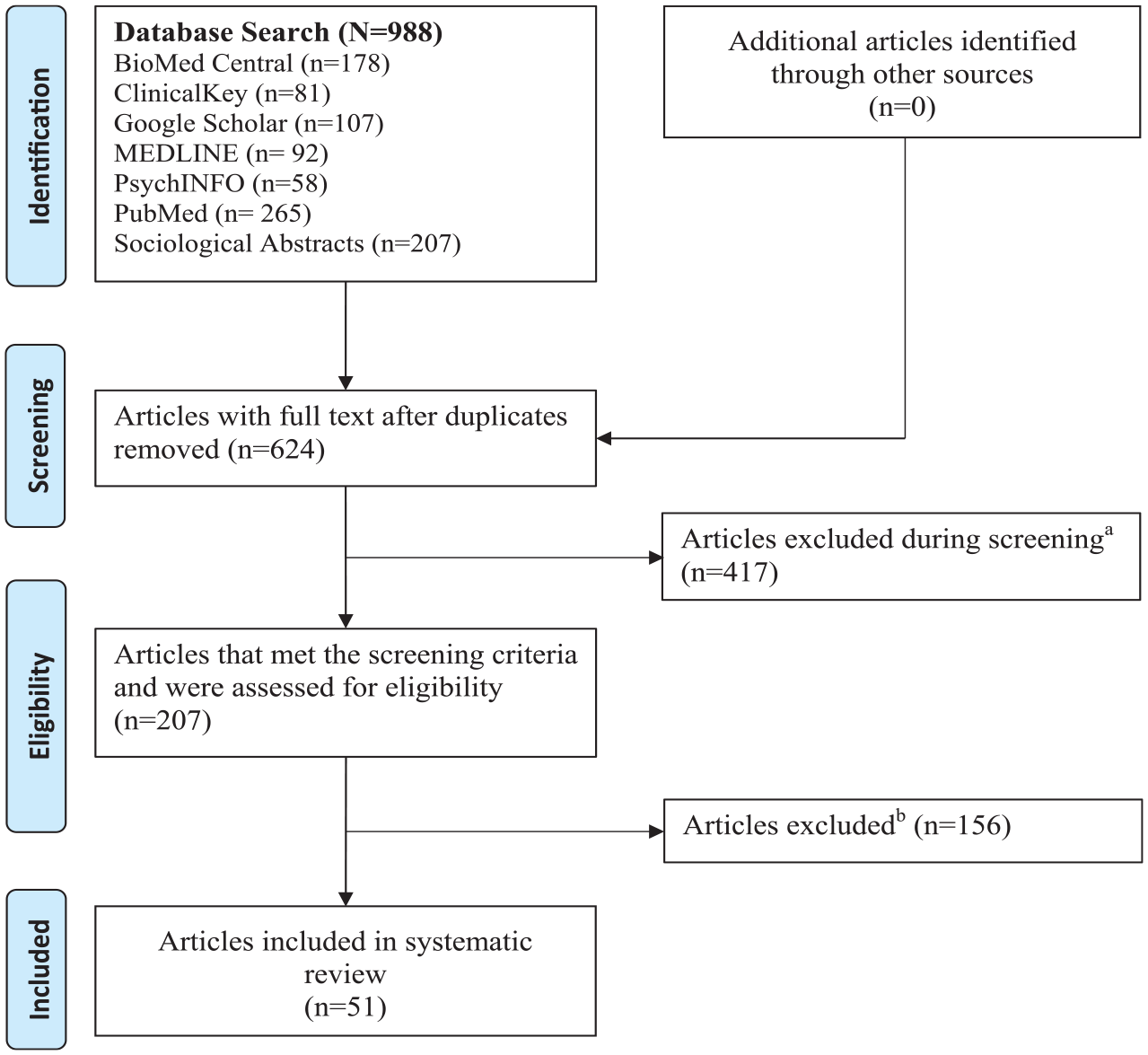
Screening flow diagram.
Screening and Eligibility Criteria for Articles.
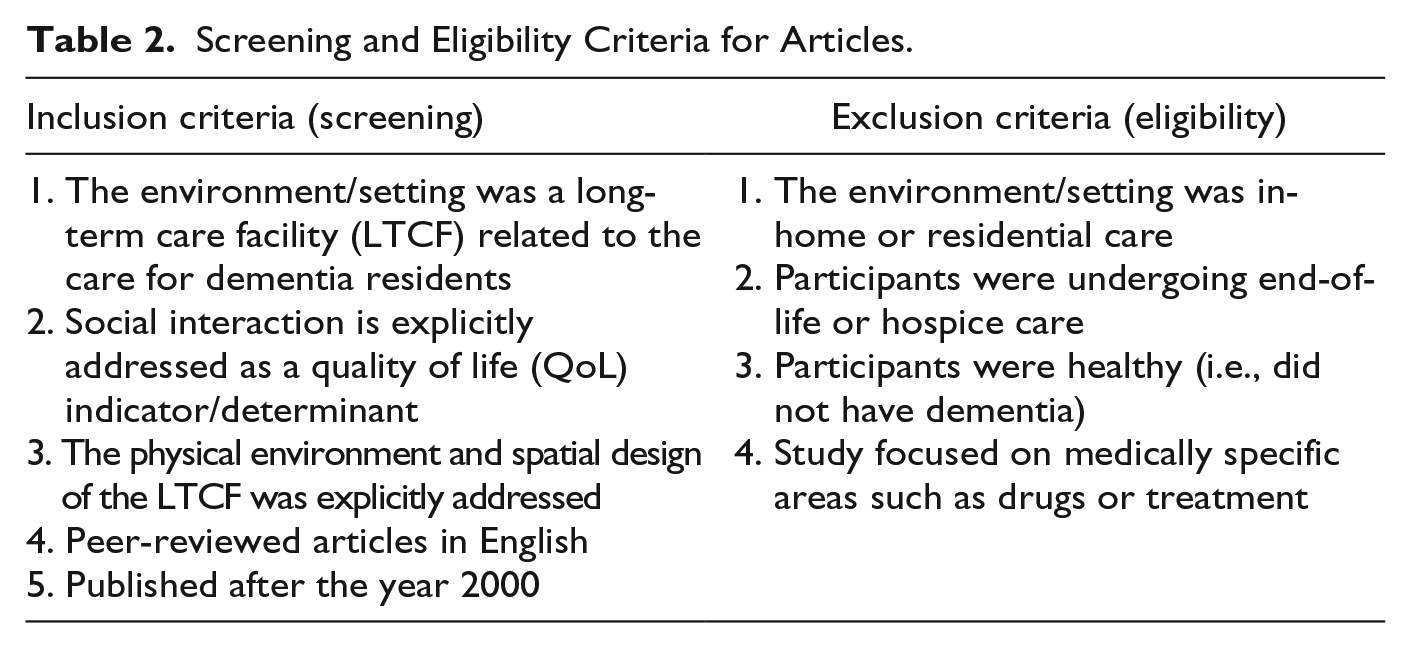
All studies included in this review explored factors potentially influencing social interaction in elderly PwD living in LTCF (Table 2).
Data Extraction and Study Classification
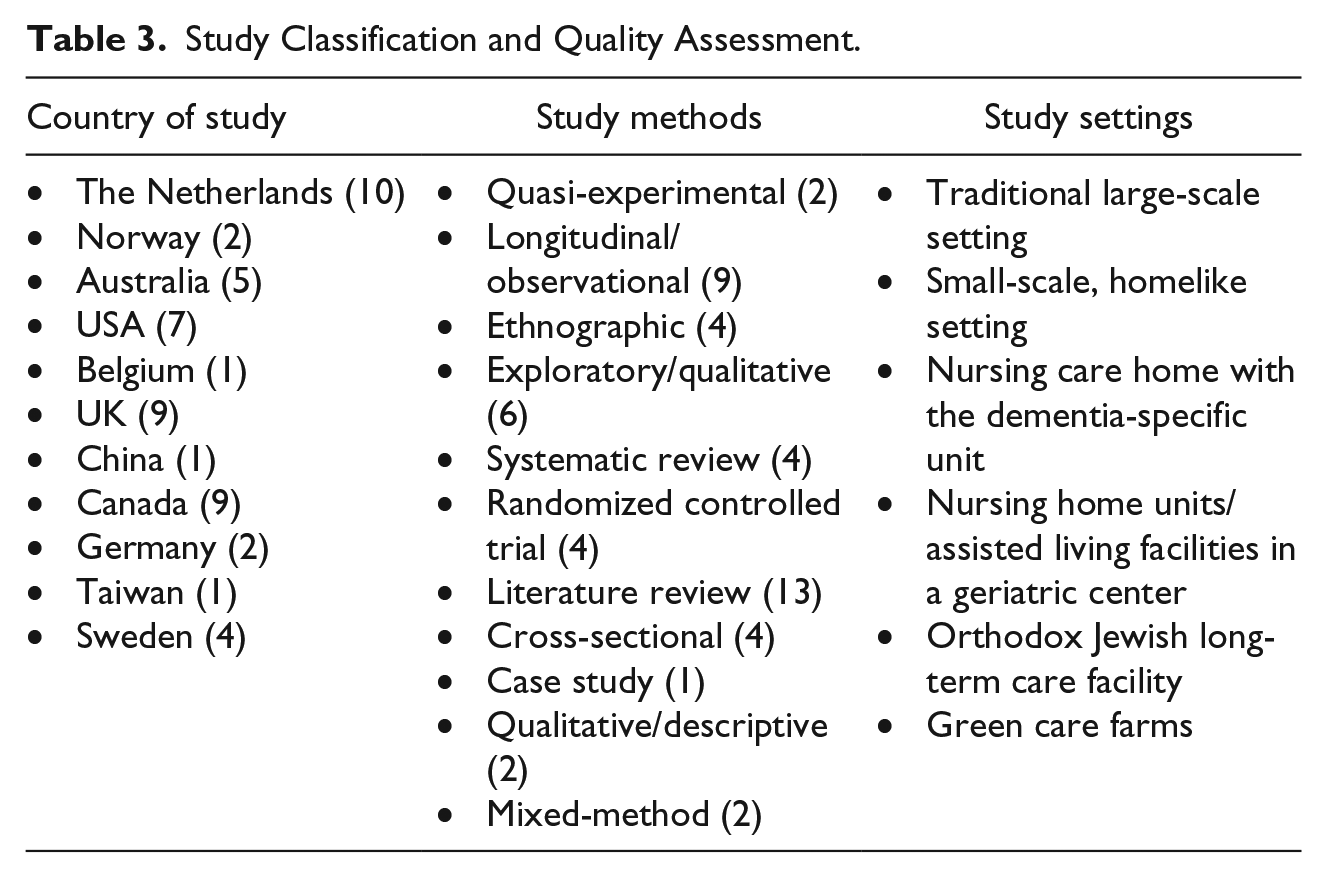
An Excel spreadsheet was created to record key information extracted from each study, including the location of research, research design, study setting, sample age and size, design intervention, inclusion criteria, outcome measures including use of scale or tool, and major findings and results of the study (Table 4 in Supplementary Material). The reviewed literature was also classified based on country of study, study methods, and study settings (Table 3).
Study Classification and Quality Assessment.
Rigor and Quality Assessment
The quality of each study was evaluated based on five assessment criteria: research design, sample size, design intervention, outcome measure, and interpretation of major findings (see Table 4 in Supplementary Material). This checklist is based on critical appraisal tools from Zaza et al. (2000), which also follow the PRISMA 2009 checklist and flow diagram. In this review, more than half (26) of the reviewed articles employed systematically sound qualitative and longitudinal research design, 17 used systematic literature review with a large number of articles (minimum 11, maximum 103), and the remaining eight studies used quantitative mixed-method research design (Table 3). The articles are also globally distributed and have study settings in many regions including Australia, the United States, the United Kingdom, Scandinavia, Europe, Canada, and different countries of East Asia (Table 3).
Results
After careful examination of the 51 studies included in this systematic review and synthesis, four major spatial design features that could directly or indirectly influence social interaction in PwD were identified and are outlined below. The results from this synthesis have been categorized into those four features and their subcategories, although there is understandably substantial overlap between many of these factors.
The Physical Environment/Setting of the Facility
When considering the physical environment of care facilities, unit size, scale, and other environmental characteristics are considered principal design elements. Although residents of care facilities value the care services most (Digby & Bloomer, 2012), the importance of the physical environment is simultaneously identified as a leading factor in potentially influencing social interaction. Spatial design features such as ambience in the environment, the use of familiar objects, furniture type and arrangement, inclusion of kitchen and residential scaled dining room, white noise, connection to nature, access to outdoor areas, privacy, use of bright light, color, temperature, wayfinding, use of smaller spaces or landmarks with simple decision-making points, and, above all, homeliness can significantly affect a patient’s mood and behavior (Barnes, 2002; Calkins, 2009; Digby & Bloomer, 2012; Fleming & Purandare, 2010; Mitchell et al., 2003; Werezak & Morgan, 2003) which can further influence social interaction and QoL. Dementia-friendly outdoor design features are also important aspect in designing care facilities. When designing the outdoor environment, bright colors such as yellow can be disruptive or agitating to the homeliness of the environment; instead, landmarks could be used as wayfinding cues, and street lighting that illuminates the pavement edge without creating glare or changes in texture or identifiable color of paving can be used to avoid potential hazards (Mitchell et al., 2003).
Mealtime intervention and dining environment
Mealtime interventions were categorized into four types: music, changes to food service, dining environment alteration, and group conversation (Whear, Abbott, et al., 2014). Mealtime intervention aims to indirectly alter nutrition or hydration status such as food, drink, or nutrient intake; increase meaningful activity by altering aspects of the physical environment or food service, such as verbal prompting or relaxing music prior to a meal; or provide education or training to PwD or their caregivers about the importance of mealtime (Bunn et al., 2016).
Mealtime intervention is considered a significant factor in improving behavioral and psychological symptoms of dementia (Chaudhury et al., 2018; Chaudhury et al., 2013; Chaudhury et al., 2017; McGilton, Rivera, & Dawson, 2003; Whear, Abbott, et al., 2014). During mealtime, small number of residents in a dining area that conforms to the family style could enhance QoL in PwD (Malderen, Mets, & Gorus, 2013). Several studies considered music, food service, dining environment, and group conversation as the most important determinants of improving social interaction during mealtime (Chaudhury et al., 2013; Whear, Abbott, et al., 2014). PwD display more agitated behaviors when they feel anxious, and quality mealtimes can be particularly distressing. One systematic review that reported on 11 articles suggests that mealtime interventions can improve behavioral symptoms in elderly PwD living in small residential care facilities (Whear, Abbott, et al., 2014). A supportive dining environment can foster functional ability, maximize orientation, provide a sense of safety and security, create familiarity and homeliness, provide optimal sensory stimulation, provide opportunities for social interaction, and support privacy and personal control (Chaudhury et al., 2013; Chaudhury et al., 2017).
Gardens on dementia
Access to the outdoor environment is also widely considered to be likely to initiate social interaction. Residents of LTCF with dementia who spend time in a garden experience lower levels of agitation (Whear, Coon, et al., 2014). Specific attention should be paid to the physical environment, design, and access to the outdoor courtyards and gardens by incorporating the independence and safety of PwD. Gardens, courtyards, and the natural environment may be strong elements of future care for dementia that not only provide outdoor access but also improve the feeling of independence. A continuous wandering path bounded by a high wall, surrounded by scented but nontoxic plants, and without any ambiguity in walking route could be effectively incorporated in a garden design for PwD to allow for independence while minimizing hazard.
The design of the garden might also include viewing platforms, a mixture of flooring (grass, concrete, and decking), raised beds of flowers or vegetables, gazebos, and fish ponds. Outdoor therapeutic environments can provide an opportunity for multisensory stimulation through reminiscence and/or social interaction, thus proving perceived competence and improving self-esteem and relaxation (Fleming & Purandare, 2010). Views of the garden and large windows allowing natural daylight allowed residents to complete ADL efficiently (Nordin et al., 2017). A 20-year prospective cohort study on social activity, cognitive decline, and dementia risk identified that people who engage in solitary activities, such as traveling, gardening, doing odd jobs, word finds, knitting and sewing, watching movies, also have increased engagement in social, physical, or intellectual pursuits that result in decreased risk of dementia (Marioni et al., 2015).
Green care farms or natural settings
Green care farms are a specific type of small-scale, homelike care environment for PwD that combine agricultural activities with care services as an alternative to traditional nursing home care. A few studies explored the daily lives of residents at green care farms in comparison with other traditional nursing home care environments and found that the daily lives of PwD living in the green care farms are based on attractive activities, sensory physical-social environment, and psychological well-being (Boer et al., 2015). Previous research has shown that residents in small-scale, homelike care environments have better cognitive and functional abilities compared with residents in traditional large-scale nursing home wards, and green care farms provide an added benefit for residents due to the close proximity to nature. By comparing four types of nursing home care environments (large-scale nursing home ward, small-scale homelike living facility, stand-alone small-scale living facility, and green care farm), the research identified that the unique features of green care farms such as the presence of animals, stables, gardens, and outdoor areas may be important interventions for dementia (Boer et al., 2015; Boer et al., 2017). Residents living at green care farms are significantly more active, more often participating in domestic activities and outdoor/nature-related activities, and significantly less often engaged in passive or purposeless activities than the residents of a traditional nursing home. The research suggests that green care farms can be a valuable alternative to traditional nursing homes, which can provide an attractive, homelike environment with activities that positively influence engagement and social interaction.
Small-scale/homelike settings
Almost every study focusing on the physical environment and design guidelines for dementia care settings recommended more homelike character, which includes furniture, wall covering, family pictures, wall décor, a cozy living room with a sofa or armchair, and a small-scale dining layout next to the kitchen (Barnes, 2002; Boer et al., 2015; Calkins, 2009; S. Lee et al., 2016a, 2016b; Smit, Willemse, de Lange, & Pot, 2014). QUALIDEM is a measuring instrument used to assess the QoL of residents living in dementia/memory care facilities; QUALIDEM scores and results repeatedly demonstrated a small-scale, homelike setting and social interaction as the main determinant of residents’ QoL (Rooij, Luijkx, Declercq, & Schols, 2011). Self-contained dwellings for a small number of residents and a dining area that represents a family style could enhance the QoL (Malderen et al., 2013). One cross-sectional study observing residents in 38 care homes in the United Kingdom measured QoL and well-being used a measuring matrix and found that the overall QoL and well-being score was larger in small homes compared with large-scale homes (Torrington, 2006) and suggested that physical environment should be designed to support activity by providing good physical support. In a longitudinal study conducted in Canada, Lee et al. concluded that residents in small-scale, homelike facilities experience more positive effects on mental health and behavior compared with residents living in a traditional large-scale unit (i.e., LTCF). The physical environment of the small-scale care unit also had more positive design features, including quality of lighting and varied stimuli (visual, tactile, acoustic), and offered a more homelike atmosphere to PwD as compared with the physical environment of a traditional large-scale setting (S. Lee et al., 2016b).
Accessibility, Legibility, and Layout
Accessibility, legibility, and layout are strong determinants of positive social interaction that can enhance residents’ well-being and independence and are highly influenced by both organizational factors and environmental design aspects (Moyle, Fetherstonhaugh, Greben, Beattie, & AusQoL group, 2015; Nordin et al., 2017). Design of both the indoor and outdoor environments influences the residents’ activities and interactions. PwD are not just passive receptors of their environment; they may actually respond to it in a very outspoken manner, if proper opportunity to interact to the environment is provided. Synthesis of building-related solutions can help designers and building service engineers to create optimal environmental conditions inside the living environments for PwD that are considered significantly important for maintaining social interaction (Hoof, Kort, Duijnstee, Rutten, & Hensen, 2010).
Point of decision and wayfinding
When navigation of the physical environment is straightforward using either point of decision landmark or wayfinding signage, it is easier for the residents to attain orientation. An architecturally legible environment, or an environment where the function of each room is evident through the size, proportion, materiality, and furnishings, is important for designing any LTCF (Marquardt & Schmieg, 2009). The floor plan design of a nursing home, in particular, has a significant influence on residents’ spatial orientation and wayfinding (Calkins, 2009; Marquardt, 2011). Environmental interventions that promote wayfinding can be implemented at two levels: (a) the design of the floor plan typology and (b) environmental cues comprising signage, furnishings, lighting, colors, and so on. Residents’ orientation also depends on the quality of the physical environment. All areas, including hallway and circulation space, should have access to natural sunlight with proper navigation and visual signage. Decorating residents’ bedrooms and doors with personal items, the length–width ratio of the corridors, lighting location and intensity, views of the outside, and other sensory stimulation and use of landmark to navigate are important point of decision design features. Architectural guidelines include a straightforward layout of the circulation system without any changes in direction, the provision of a family-style living/dining room, and a small number of residents per unit of living area (Geboy, 2009; Torrington, 2006).
A study of nursing home’s architecture on residents’ wayfinding abilities identified five characteristics or routes within the living areas of the home: (a) live-in kitchen, (b) resident’s individual bedroom, (c) location of the toilet, (d) access to the outside, and (e) layout of the common room (Marquardt & Schmieg, 2009). Architectural design guidelines suggest various strategies to enhance orientation, including improvements for wayfinding using signage and by choosing a supportive organization of the building (Hoof, Kort, Waarde, & Blom, 2010; Marquardt, 2011). Marquardt and Schmieg (2009) also identified five types of circulation systems: (a) straight circulation system, (b) L-shaped circulation system with a change in direction, (c) continuous path around an inside courtyard, (d) corridor divided by an intermediate element, and (e) corridor ending element or design. The above-mentioned circulation system highlights access to the outdoor area or balcony that should be located in a central area within the living space.
Privacy and autonomy
Social environment, privacy, sense of belonging, autonomy, and communication are important determinants of social interaction (Barnes, 2002; Marquardt & Schmieg, 2009; Torrington, 2006). The strongest evidence supports the positive benefits of private bedrooms on outcomes such as the satisfaction of families and staff, residents’ QoL, and reduced neuro-disability (Calkins, 2009). The individual room is an important feature in maintaining spousal contact and interaction throughout all phases of dementia, from early to the final phase. Ideally, bedrooms should be located close to the community space to allow for social interaction but with substantial privacy for the resident. Although economically reasonable and to some extent beneficial for social interaction, shared bedrooms are not popular in care facilities due to noise, spread of diseases, and lack of privacy. Personalized doors and inviting interior that includes memory boxes, family pictures, and achievement certificates are considered top priority by residents (Parker et al., 2004).
Furniture layout of social spaces
When designing the interior layout, furniture arrangement plays an important role in social interaction (Campo & Chaudhury, 2011; Digby & Bloomer, 2012). Seating areas in the hallways can maximize visual access in a dementia care unit, and furniture should be arranged in a conversational pattern to stimulate social interaction. Design recommendations also include homelike decorations and furniture, adequate lighting, and a layout that minimizes ambient noise to ensure congruence between the physical and social environments. Homelike décor and furniture may include the presence of meaningful objects and visual stimuli such as colors, carpet, wall decorations, photographs, fish tanks, mood lamps, walking paths, and other occupational stimuli such as books, papers, magazines, games, or stuffed animals (Smit et al., 2014).
Geboy (2009) identified 10 design principles for residents and staff of dementia care facilities, where furniture arrangement and spatial organization were particularly emphasized. Geboy recommended placing seating at right angles rather than in rows or along the periphery of the room (against the wall) and suggested planning to accommodate space for seating individuals in wheelchairs. Geboy (2009) also recommended using flexible space as a resource by personalizing and accessorizing the space with activity “props,” conversation groupings, and decentralized dining. However, further detail design recommendations should be outlined in a guideline matrix when designing such care facilities.
Social Environment and Network
Frequent social interaction is associated with higher QoL, and research clearly describes the importance of social interaction and positive mood in promoting QoL. In one study, dementia residents with higher QoL were more engaged in active, expressive, and social activities and less engaged in passive/purposeless activities compared with PwD with lower QoL (Beerens et al., 2016). By looking at 1,704 interactions over the course of 143 hr, Abbott et al. highlighted five factors to characterize interaction: (a) location of interaction, (b) context of interaction (e.g., social, care-related, or re-direction), (c) type of interaction (verbal or nonverbal and with whom), (d) frequency and duration of the interaction, and (e) quality of interaction (Abbott, Sefcik, & Van Haitsma, 2017). The results found that interactions were brief, verbal, and social in nature and occurred in public areas. Casual living and activity areas in close proximity to bedrooms or kitchens enhanced the social environment and integration through both design and staff involvement. The socio-human environment was perceived to be more important than the physical environment. Specialized physical design features can be useful for maintaining the QoL to reduce disruptive behaviors. In 2012, Garcia developed a mnemonic—C.A.R.E.F.U.L.—as a design recommendation tool for the social environment, identifying design elements from the physical and social environment that hinder or improve the disruptive behaviors and QoL of residents in LTCF (Garcia et al., 2012).
Therapeutic environment for interaction
The therapeutic physical environment is repeatedly identified as an important design element for positive social interaction (Chaudhury et al., 2018; Geboy, 2009; Hoof, Kort, Waarde, & Blom, 2010; Marquardt, 2011). Legibility, familiarity, autonomy, sensory stimulation, and social interaction are a few criteria for creating a therapeutic physical environment (Marquardt et al., 2011). Get-togethers with family, friends, or neighbors were associated with a higher level of QoL for elderly PwD. Having a window to view nature and receive fresh air could improve the level of QoL. A dementia-friendly spatial therapeutic environment, such as one that provides a familiar and comfortable living environment for elderly persons, is significantly important (Jing, Willis, & Feng, 2016). The psychosocial environment is closely related to positive social interaction, and the resultant effect on psychological and emotional well-being is critical to high-quality institutional dementia care (Werezak & Morgan, 2003).
Active participation as an aspect of QoL
QoL is a multidimensional construct that includes social relationships, active participation, and positive association with the physical environment (Parker et al., 2004). Reminiscence, leisure, expression, and vocational occupation had the greatest potential to enhance well-being. The physical environment and care organization might play a role in doing the same, but the key factor seems to be equipping staff with skills to integrate well-being-enhancing occupation into care practice. LTCF with more active atmospheres supported social interaction via the environment, and having more activity programs is preferable (Smit et al., 2014). Care in the facility are preferable that involves letting residents make their own choices and encouraging social interaction and participation in spontaneous activities. One meta-analysis shows that people with less social participation, less frequent social contact, and more feelings of loneliness have an increased risk of developing dementia. Although the results were not statistically significant, low satisfaction with social network seems to be associated with incidence of dementia (Kuiper et al., 2015).
Level of interaction in improving QoL
It is evident that frequent social interaction is associated with higher QoL. Social environment factors such as the role of staff, resident group size, and time of day the interactions take place are equally important to the other physical environmental attributes as discussed before. Social factors such as staff roles, resident group size, and physical factors, such as a noninstitutional character of the environment, nursing station location, adequate seating, and informal social interaction in care facilities, are important determinants (Campo & Chaudhury, 2011). A supportive work environment is very important for staff interaction, and the level of nursing staff interaction in any LTCF may facilitate or impede healthy transition processes for older residents (Eika, Dale, Espnes, & Hvalvik, 2015). Among experimental studies, the largest proportion of interventions includes the physical activity levels or the psychological factors of the residents to determine the level of interaction and QoL.
Staff–Resident Ratio and Care Philosophy
Quality staff interaction with residents plays an important role in promoting the psychological well-being of PwD in a psycho-geriatric setting (K. H. Lee, Boltz, Lee, & Algase, 2017). The physical environment, the care philosophy, and the culture of care play major roles in the daily lives of the residents at the Residential Care Facility (Nordin et al., 2017). The quality of residents’ relationships and quality staff interaction with residents plays an important role in promoting the psychological well-being of persons with dementia (Garcia et al., 2012). Positive interactions (regardless of whether they were verbal or nonverbal) were significantly associated with more positive emotional expression, whereas negative interactions were not (K. H. Lee et al., 2017).
Person-centered care (PCC) approach
Evidence from the literature review supports that appropriately designed physical settings play an important role in creating a PCC approach for the residents. PCC focuses on independence, selfhood or having an individual identity, well-being, and abilities of residents to feel supported, valued, and socially confident within their surrounding environment. Dementia and Alzheimer’s disease change a person’s ability to think, act, and interact with the surrounding social environments, and a PCC approach may reinstate the confidence of the residents. Sociability is an embodied dimension of selfhood (the state of having an individual identity) in person-centered dementia care, and both sociability and selfhood in dementia are equally important in comparison with other factors. Empathy, social etiquette, and the power of gesture are major aspects of selfhood. Person expressed empathy through kind words, touch, and attentiveness and responded to others’ presence and feelings of sadness, loss, and fear (Kontos, 2011). A gesture is a phenomenon that often passes without notice, yet in face-to-face interaction, it is an important resource for communication and residents do not communicate with each other with words alone (Kontos, 2011). In a qualitative descriptive study using in-depth semi-structured interviews, participants described that the care received was more important than the physical environment, but participants also valued homeliness and privacy (Digby & Bloomer, 2012). However, small-scale homelike settings with comfort, familiarity, and organized space gives dementia care homes more opportunities to improve QoL for residents and a more supportive work environment for staff (S. Lee et al., 2016a).
PCC and dementia care mapping both seem to reduce agitation and increase social interaction in PwD. The most promising treatments seem to be individually tailored behavioral interventions. The implementation costs of PCC mapping are lower than those of dementia care mapping, which requires more intensive training (Chenoweth et al., 2009). Chaudhury et al. (2013) identified the role of the physical environment in supporting person-centered dining, and the evidence indicates that well-designed physical settings can play an important role in creating a person-centered dining environment to support the best possible mealtime experience.
Empowering residents
Empowerment and collective decision-making enhances social interaction, QoL, and well-being among older adults (Knight, Haslam, & Haslam, 2010). Empowered residents feel more engaged with their environment and the people around them, and they are generally happier and have better health. The design of communal living space had several substantial positive consequences for both residents and care staff. One longitudinal experiment explored empowering residents to make collective decisions about the décor of communal space, which positively impacts the following: (a) identification with others in their home, (b) well-being and QoL, and (c) social interaction with fellow residents (Knight et al., 2010).
Sense of coherence (SOC) is a person’s way of viewing their own life. It is also a global orientation of experience that reflects the capacity to respond to stressful situations (Eriksson & Lindström, 2005; Koelen, Eriksson, & Cattan, 2017). SOC consists of three elements: comprehensibility, manageability, and meaningfulness. To measure SOC, Antonovsky (1979, 1987) developed the SOC scale with 29 items (SOCS-29), titled the “Orientation to Life Questionnaire,” with 11 items measuring comprehensibility (the cognitive component of the SOC), 10 items measuring manageability (the instrumental/behavioral component of the SOC), and eight items measuring meaningfulness (the motivational component of the SOC; Eriksson & Mittelmark, 2017).
LTCF residents in Taiwan had relatively low SOC scores (measured with Chinese version of Antonovsky short 13-item SOC scale) compared with their counterparts in Western countries. Among personal and environmental factors, it was discovered that education level, ADL score, and number of LTCF staff were significantly associated with the SOC status. Higher education level and higher ADL scores with more LTCF staff had a stronger SOC (Jueng, Tsai, & Chen, 2016). In an observational longitudinal study of 176 residents in a nursing care home, the study findings suggest the provision of autonomy for residents, letting them make their own choices and encouraging social interaction and participation in activities (Boer et al., 2015). By creating a more homelike dining atmosphere with appropriate interior design, one study of pre- and post-renovation of physical environment of the dining room has suggested five notable themes from the renovations: (a) autonomy and personal control, (b) comfort from a homelike environment, (c) conducive to social interaction, (d) increased personal support, and (e) effective teamwork among residents (Chaudhury et al., 2017). From the literature, it is evident that empowering the residents is an effective approach in care facilities.
Staff–resident ratio
Across all studies, continuous and spontaneous staff collaborations were key activities in supporting quality care. The interaction between staff and residents heavily was influenced by the staff–resident ratio, and the interactions also helped new residents to settle down by engaging in more positive, meaningful interaction during the transition process (Eika et al., 2015). Staff interaction during the older adults’ transitions was influenced by three main themes: (a) the significance of formal and informal organizational activities and interactions, (b) interpersonal relationships and cultures of care, and (c) professional hierarchy and different scopes of practice (Eika et al., 2015). Low ratio of staff to residents and disturbing noise were identified as two of the most important factors influencing behavior and QoL of residents (Garcia et al., 2012). An observation study by Edvardsson et al. identified staff presence and absence as the core concept influencing the psychosocial climate and the well-being of people in dementia in a psycho-geriatric setting. Staff were catalysts for the psychosocial climate, and when present or engaged, they could create a climate interpreted by the residents as homely, which supported patient well-being. When staff were absent, the climate quickly became anxious, and this was associated with patient ill-being (Edvardsson, Sandman, & Rasmussen, 2012).
Both the physical environment and staff care are important design aspects that influence the residents’ activities and interactions (Nordin et al., 2017). PwD with higher levels of education, higher ADL scores, and exposure to more LTCF staff had a stronger SOC (Jueng et al., 2016). The result suggests older adults in LTCF with more staff have a stronger SOC than those who stay in LTCF with fewer staff. Environmental factors such as outdoor public space may moderate the relationship between education level and SOC. More educated residents who stay in LTCF with outdoor public space may have a stronger SOC than those who stay in LTCF without outdoor public space (Jueng et al., 2016).
Discussion
It is evident that one in eight baby boomers will be diagnosed with dementia of the Alzheimer’s type once they are 65 years old. In 2016, the first baby boomers turned 70 years, and it is projected that by 2031 nearly one in two baby boomers more than the age of 80 years will be diagnosed (Bredfeldt, Rice, & Alecxih, 2015). Dementia of the Alzheimer’s type is a disease that does not have any cure or prevention, so the focus of care should be to improve social interaction and thereby QoL, and this may be done through environmental design. The objective of this literature review was to provide guidelines for designing better memory care facilities by highlighting the spatial design features for positive social interaction and ultimately better QoL.
Four key spatial design characteristics were identified as important criteria in affecting positive social interaction: (a) The Physical Environment and Setting; (b) Accessibility, Legibility, and Layout; (c) Social Environment and Network; and (d) Staff–Resident Ratio and Care Philosophy. The study identified that both physical and social environment are equally important aspects in maintaining positive social interaction between peers and caregivers. Staff also plays a key role in socialization given that the increased staff–resident ratio on the unit is an important contributing factor to initiate a positive social network. The following design intervention guidelines related to environmental factors may improve the psychological, social, and physical well-being and/or QoL of caregivers, staff, and residents:
Spatial layout of the physical environment: The design of the physical environment in supporting dementia residents has been mentioned in the research literature for more than 40 years. The configuration of the spatial layout should be open, compact, connected, visually and physically interactive, legible, and easily understandable by the residents, caregivers, and users to promote positive social interaction.
Consider size and scale of the facility: When designing care facilities, mid-size to small-scale are considered the best sizes for promoting social interaction. To maintain the homelike environment and to facilitate social interaction, the facility should not be designed for more than 10 residents.
Promote mealtime intervention: Mealtimes are considered the most important times for residents to have the opportunity to interact and ideally occur 3 times/day. Mealtime interventions, including altering the physical environment of the dining room, can have several benefits such as reduced agitation, reduced anxiety, improved food intake, and improved social interaction.
Foster ambient indoor environment: Adequate lighting, soothing sounds, appropriate temperature, reduced noise, and other ambient features of the indoor environment should be in favorable conditions to maximize the comfort and social interaction between residents and caregivers. Positive interventions such as white noise, soft music, aromatherapy, visual artworks, indoor plants, and soft/mood lighting can significantly improve the ambient environment and atmosphere, in turn promoting positive social interaction.
Access to therapeutic garden or outdoor environment: Therapeutic outdoor environments can provide opportunities for multisensory stimulation through reminiscence and social interaction, resulting in improved physical/cognitive competence, self-esteem, and relaxation. Gardens should be designed with safe outdoor access to both minimize hazard and improve independence by providing continuous wandering paths, scented but nontoxic plants, viewing platforms, a mixture of flooring (grass, concrete, decking), raised beds (of flowers or vegetables), gazebos, and fish ponds to promote sensory experiences.
Exposure to natural settings: Natural settings such as green care farms can be a valuable alternative to traditional nursing homes. They provide an attractive, homelike environment and activities that can positively influence engagement and social interaction while allowing residents to be in close contact with nature.
Foster homelike décor and personalized space: By accommodating the family members and customizing/personalizing the immediate environment with the homelike décor in both public and private spaces, care facilities can foster relationships between residents, family members, and caregivers.
Facilitate point of decision and wayfinding: The floor plan of a nursing home, in particular, has a significant influence on residents’ spatial orientation and wayfinding, both of which are required for PwD to feel comfortable engaging in social interaction. Environmental interventions that promote wayfinding can be implemented through environmental cues. Decorating residents’ bedrooms and doors with personal items, architectural differentiation, and use of color, texture, landmark, signage, and other sensory stimulation are important design features for point of decision and wayfinding.
Promote privacy for residents and support family presence: The individual room is an important feature in maintaining privacy, spousal contact, and social interaction throughout all phases of dementia. Strong evidence (i.e., from randomized trials) supports the benefits of private bedrooms on positive outcomes such as the satisfaction of residents, families, and staff, improved QoL, and reduced neuro-disability.
Provide appropriate furniture layout and seating arrangement: Furniture layout and seating arrangements are the most important interior design guidelines. Small group seating at right angles is ideal to stimulate social interaction. Chairs should be arranged in a conversational pattern, while “theater-style,” periphery seating against the wall should be avoided.
Provide an opportunity for social interaction: Social/human environments are sometimes perceived to be more important than physical environments. By keeping that in mind, some facilities offer shared bedrooms to reduce isolation and loneliness among residents. Although this can impede privacy and facilitate the spreading of infectious diseases, a shared bedroom option could also initiate social interaction not only between residents but also among family members.
Emphasize the care philosophy: PCC, individually tailored behavioral intervention, or approach to care philosophy seems to reduce agitation in PwD in LTCF. The adoption and intervention of social network analysis to facilitate PCC among residents in LTCF may significantly improve their well-being.
Empower the residents through autonomy: Valuing residents’ choices and collective decision-making related to simple design to improve indoor and outdoor environments can enhance social interaction, QoL, and well-being among older adults. The care facility can involve and value the residents’ opinions on simple but meaningful aspects such as landscaping, placement of artworks, indoor plants, home décor, and interior layout or furniture layout in common spaces or bedrooms.
Provide ample staff–resident ratio: Staff–resident ratio is frequently identified as an important determinant for social interaction and is even often valued as more important than the physical environment. Quality staff interactions with residents are valued as the core concept influencing and promoting the psychological and psychosocial well-being of PwD. Staff are catalysts for the psychosocial climate, and their presence or absence can facilitate residents’ well-being or ill-being, respectively.
Conclusions and Future Directions
One important objective of this review was to identify gaps in knowledge in the existing research literature to give directions for future research. There is a strong need for evidence-based design solutions to accommodate the personal, social, and psychological needs of the residents, staff, caregivers, and family members. There was very little research addressing the importance and key design features of the spatial configuration and ambient environment as they are proportionately related to the physiological and psychological health and well-being of the immediate users. Effective layout of the facility, clean air, cross ventilation, reduced glare, indirect natural light, soothing sound, white noise, aromatherapy, visual paintings are a few areas of concern that need further research specifically in long-term care settings for cognitively impaired people.
Among the reviewed literature, many studies had small sample sizes, without describing the quality assessment, cross verification or triangulation in study design, insufficient inclusion criteria, and control of the environment or settings, these all are considered as limitations in this synthesis study. Moreover, this article only addressed “people with dementia” in long-term memory care settings as opposed to healthy older adults or other forms of cognitive impairment for older adults in different settings such as a home or residential care, end of life, hospice care; thus, generalizability is limited. By highlighting the design intervention guidelines, this systematic review could be used as a resource for all LTCF administrators and health care design professionals and researchers to understand the gaps and opportunities in designing future care facilities to provide a positive social environment for PwD.
Positive social interaction is a strong determinant in improving QoL, even in PwD. The physical environment and spatial design of care facilities for PwD likely have a large role to play in promoting social interaction and thereby improving QoL in PwD. However, more high-quality experimental studies (i.e., randomized controlled trials) are required to confirm causational relationships between these factors. This research will prove very useful, as the incidence of dementia is growing and interventions to improve QoL are sorely needed.
Supplemental Material
Supplemental_material – Supplemental Material for Positive Social Interaction by Spatial Design: A Systematic Review of Empirical Literature in Memory Care Facilities for People Experiencing Dementia
Supplemental Material, Supplemental_material for Positive Social Interaction by Spatial Design: A Systematic Review of Empirical Literature in Memory Care Facilities for People Experiencing Dementia by Farhana Ferdous in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Toyota Foundation Individual Research Grant and Academy of Architecture for Health Foundation (AAHF) research grant.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.