
Abstract
Objective
Despite a growing body of research, the effects of retirement on health are not clear. The study explores the role played by the path out of the labour market (formal retirement vs. unemployment or family reasons), accounting for individual heterogeneity.
Introduction
At first sight, the abundant literature about the effects of retirement on health seems inconclusive: the retirement-health relationship appears to be sometimes positive (retirement leading to better health), sometimes negative (retirement leading to worse health) and sometimes not significant (e.g. Van Der Heide et al., 2013).
Several reasons lie behind these contradictory findings. Some are substantive because contrasting mechanisms may be at play. On the one hand, retirement may lead to a sudden break with support networks, colleagues, and friends, and may constitute a sort of shock. Besides, once out of the ‘productive chain’, individuals may lose the sense of belonging and usefulness they (probably) felt when they were employed, and they may also stop investing in intellectually engaging activities, with negative consequences on cognitive functions (Bonsang et al., 2012; Lee et al., 2019; Mazzonna & Peracchi, 2012). Adverse effects on chronic conditions and physical health have sometimes been found, as a consequence of reduction in physical activity and social interactions after retirement (Dave et al., 2008; Behncke, 2012). On the other hand, retirement may instead prove beneficial: it is a relief from work-related stress, increases leisure time, and may encourage health-enhancing behaviours and lifestyles (Eibich, 2015; Insler, 2014) although the outcome may depend on individual or pre-retirement job characteristics (Celidoni & Rebba, 2017; Zantinge et al., 2013). This may improve physical and mental health (Syse et al., 2017), whether it is measured objectively (Coe & Zamarro, 2011; Kolodziej & García-Gómez, 2019), subjectively (e.g. self-perceived health; Hessel, 2016), or indirectly, via questions on life satisfaction (Horner, 2014).
The decision to stop working, and when, may imply a complex evaluation of costs and benefits, opportunities, and constraints (Whitley & Popham, 2017): its consequences in terms of health and wellbeing may vary. This highlights the role of heterogeneity: individuals differ in their socio-demographic profile, behaviours and preferences, and they retire from different occupations. All these characteristics contribute to shape both retirement decision and post-retirement health – incidentally, this joint determination complicates the search for a true causal effect.
The contradictory findings of the literature depend also on the research design. For instance, the health outcome that one selects is not neutral, because health has several dimensions, and no single indicator suffices (Pirani, 2017; Voss et al., 2020). Retirement may prove beneficial in some respects and detrimental in others (e.g. triggering depression while improving physical conditions), and in both cases, these effects work through the mediation of several other dimensions, family circumstances and institutional settings. The time since retirement is also very relevant: little is known on the mid- or long-term development of objective and subjective health after retirement, a path that may itself be causally linked to the change of status, for instance, through an adaptation process. In empirical analyses, time since retirement is typically short, for lack of long panel data (a limitation that affects also our results, incidentally; for an exception, see Westerlund et al., 2009).
The contradictory findings of the literature depend also on definitions and analytical strategies. As for the former, the term ‘retirement’ is often used loosely, and its meaning may range from acquiring the formal status of a retiree to the simple fact of leaving the labour market, past a certain age. In turn, this choice is linked to life histories – for example, in terms of income, or individual’s family situation – probably the true underlying causes (Halleröd et al., 2013; De Preter et al., 2013). Data availability rarely permits researchers to keep these long-term factors under control, unless they reverberate in some observable variable around the time of retirement, or shortly before it. This connects to the thorny methodological issue of endogeneity (Nishimura et al., 2018). Retirement is not independent of previous health conditions (for instance, see Behncke, 2012; Bonsang et al., 2012; Eibich, 2015; Mazzonna & Peracchi, 2012) and ‘reverse causality’ (health affecting retirement, rather than vice versa), if not properly controlled for, may invalidate all conclusions.
The purpose of this paper is to clarify three of the issues at stake in this field of study. As for the endogeneity problem, we adopt a propensity score matching (PSM) approach, a suitable way of estimating effects in observational contexts (e.g. Caliendo & Kopeinig, 2008; Crown, 2014). Relying on this technique, whose limits and potentialities we also discuss, we pursue our second aim, an analysis of the relevance of the path out of the labour market (see also Blomqvist et al., 2020; Halleröd et al., 2013; Whitley & Popham, 2017). Finally, we deal with heterogeneity, stratifying our analyses by several individual characteristics.
While in this article we focus on the individual level, the general picture should not be overlooked. Delaying retirement has become crucial for the survival of pension systems in most developed (and formerly developing) countries, which are ageing rapidly (OECD 2019). This strategy, in conjunction with others (such as adjusting contributions and benefits), is practically forced and has in fact been pursued and periodically reinforced in all OECD countries. Besides, it seems consistent with the development of clerical occupations, the constant increase in life expectancies and the possible, although not so clear, expansion of healthy life expectancy (ibidem). Determining by how much retirement can be delayed without (major) negative consequences on people’s health appears to be of paramount importance: this paper aims to shed additional light on some of the relevant issues in this domain.
Between Theoretical Considerations and Technical Difficulties
On the definitions of retirement
Strictly speaking, retirement is a formal passage from employment to the status of retiree, receiving a pension benefit. Usually, this happens because people have reached a specific age, possibly in combination with a certain seniority (through old age retirement schemes), or because they have become ill or unable to work, and in this case one can usually count on invalidity or sickness pension schemes. However, there are also other reasons that may push people out of the labour market: people may lose their job, or may decide, or need, to do something else, such as taking care of sick relatives. Indeed, in recent decades, similarly to what happened in the labour market, also the phase of retirement has been characterized by an increasing level of complexity (Voss et al., 2020). For instance, more than half of the workforce in Europe leave their occupation through pathways other than formal retirement, with men generally exploiting disability or unemployment benefits, while women become economically inactive (e.g. to take care of family members, OECD 2011). The boundaries between these situations are frequently blurred, and the transition may have more than just one cause: for example, unemployment frequently drives relatively old people out of the labour market, because re-employment perspectives are scarce.
The variety and indeterminacy of paths leading to labour market exits at later ages are recognized in the literature (e.g. Denton & Spencer, 2009), but not always accounted for in empirical research, where several studies equate retirement with the end of the working life past a certain age (e.g. 60 or 65 years). For instance, a frequently used definition is the simple ‘not working for pay’ (e.g. Coe & Zamarro, 2011; Eibich, 2015; Kolodziej & García-Gómez, 2019; Oi, 2019; Zhu, 2016), sometimes refined with the intention of staying out permanently (e.g. Bonsang et al., 2012). The downside of this broad definition is that the observation group becomes heterogeneous because individuals who formally retire and receive a pension benefit get mixed up with those who leave the labour market for other reasons, such as unemployment, sickness or passage to economic inactivity – and health consequences may differ.
While transition from work to retirement (broadly defined) has led to ambiguous results (e.g. Van Der Heide et al., 2013), transition to unemployment, especially late in life, has consistently been found to generate depression and anxiety (Blomqvist et al., 2020), diminished social engagement and self-esteem (Whitley & Popham, 2017) and lower psychological wellbeing and mental health (Voss et al., 2020). Studies on people – generally women – leaving job to take care of family and home are scarce, but a reduced mental engagement has generally emerged in these cases (Whitley & Popham, 2017). These negative health consequences tend to be long lasting: returning to work, when possible, usually improves wellbeing, but fails to bring it back to its initial levels (Voss et al., 2020).
In short, leaving the labour market may have different consequences. To investigate which prevail, in what circumstances, we formed different groups of ‘mature’ people (aged between 50 and 70 years) who were formerly employed, distinguishing those who formally retired from those who exited the labour market for unemployment or family reasons, and we measured the health effect of all of these paths.
Heterogeneity issues
Some authors claim that individual heterogeneity accounts for differences in research results (e.g. Blomqvist et al., 2020; Halleröd et al., 2013; Grøtting & Lillebø, 2020). Retirement decisions result from the subjective evaluation of a number of push and pull factors, acting both at individual and institutional level (De Preter et al., 2013); on the one hand, socio-economic circumstances, family situation, and health all play a role, as well as job-related characteristics such as job satisfaction, fatigue, labour market attachment, and income. On the other, push and pull factors can also be defined at institutional level (Whitley & Popham, 2017), considering, for example, public pension schemes, with their penalties or incentives for early retirement, or other welfare programs (e.g. unemployment or invalidity schemes).
For example, education and socio-economic status may differ between individuals in different occupations, the highly educated and well-off typically occupying prestigious positions, less physically demanding, and less likely to deteriorate one’s physical or mental health. In turn, education affects what may be labelled ‘cognitive investment’ before and after retirement (Mazzonna & Peracchi, 2012), and changes in lifestyle, such as smoking or physical activity (Celidoni & Rebba, 2017). Also family networks have been found to be correlated to health in late life (Siegel et al., 2004; Pirani & Salvini, 2012) although empirical evidence on the link with labour market exit is scarce. Considering job-related characteristics, dropping physically demanding or unpleasant jobs has been found to be a relief (Celidoni & Rebba, 2017; Eibich, 2015; Mazzonna & Peracchi, 2017; Zantinge et al., 2013), and the same applies to jobs that create stress (Van Den Bogaard et al., 2016). Conversely, abandoning a prestigious and stimulating occupation may be experienced as a loss. Not surprisingly, the consequences on health differ in the two cases (e.g. Kolodziej & García-Gómez, 2019; Westerlund et al., 2009).
In this article, we take this heterogeneity into account, by estimating the effect of leaving the labour market across different subgroups of individuals.
Methodological perspectives
Another reason behind the contradictory findings of the literature on the health–retirement relation lies in the methodology of analysis. This is perhaps the main conclusion of Nishimura et al. (2018) in their systematic review of studies based on Global Aging data (SHARE, ELSA, HRS, HSE, JSTAR), where they also considered alternative definitions of retirement. The biggest challenge is to account for selection and for the possible endogeneity between retirement and health, which is one of the drivers of the decision to retire or just leave the labour market. To circumvent these problems, an instrumental variable (IV) approach is often adopted, combining age-, country-, and gender-specific incentives for retirement, together with the statutory retirement age (e.g. Behncke, 2012; Coe & Zamarro, 2011; Fe, 2020; Kesavayuth et al., 2018; Kolodziej & García-Gómez, 2019). Individual fixed-effects are sometimes also kept into account (e.g. Bonsang et al., 2012; Celidoni & Rebba, 2017; Oi, 2019; Zhu, 2016).
However, a valid instrument, such as the frequently used ‘statutory retirement age’, must be correlated with the ‘cause’ (retirement) but not with the ‘effect’ (health), not even indirectly, for instance, through some unobserved variables that affect health. Unfortunately, this is an assumption that cannot be empirically tested, and it turns out to be very difficult to find a conceptually valid instrument (Crown, 2014). A tempting solution, in these cases, is to add as many control variables as possible, to avoid the omitted variable bias. However, all these controls should be unrelated to health and should not be themselves affected by retirement, which is rarely the case (Kolodziej & García-Gómez, 2019; Mazzonna & Peracchi, 2012). Finally, even studies that account for socio-economic heterogeneity in the relationship between retirement and health do not always consider that the statutory age at retirement employed as instrumental variable may vary by type of job and employment sector, as in Italy, for instance, or because of other factors, such as (for women) the number of children, as in some Eastern European countries (OECD, 2019). In other cases, a statutory age at retirement simply does not exist (Eyjólfsdóttir et al., 2019).
In this paper, we opted for the Propensity Score Matching (PSM) approach. While rarely used in this field of study, and typically applied only to a reduced set of countries (i.e. Behncke, 2012; Coppola & Spizzichino, 2014; Eyjólfsdóttir et al., 2019; Radó & Boissonneault, 2018), the PSM can produce an unbiased estimate of the causal effect using observational data sets, if the underlying assumptions are satisfied (Crown, 2014; Li, 2013). The most important of these is that that assignment to treatment is strongly ignorable, or unconfounded: in other words, that there are no observed or unobserved variables that influence treatment selection (retirement). This risk can never be altogether eliminated, but if the set of observed variables is large and appropriately selected, and if it can itself be interpreted as a proxy of other unobserved variables (think, for instance, of how telling education and income are of socio-economic status in general), the degree of confidence in the results of the analysis increases considerably. In particular, this approach allows to control for health prior to retirement, one of the most important factors for the selection into retirement itself.
Another reason to prefer the PSM approach to IV lies in the type of effect to be estimated. After the match based on the propensity score, one can compute the so-called Average Treatment effect on the Treated (ATT), or the treatment effect averaged over the subpopulation of treated people, a measure of the difference in the outcome (health) between those who stop working (treated) and those who do not (controls). Conversely, the IV approach leads to estimate the so-called LATE, or locale average treatment effect, which corresponds to the average of the treatment effect over the individuals whose behaviour would be different if the instrument (generally the statutory retirement age) were changed (Newey, 2007). Our aim is to study whether and to what extent exiting the labour market, for whatever reason, triggers ill health, and this exit can take place not only for retirement strictly defined. We do not intend to evaluate the effect of a given policy measure (for instance, the increasing in statutory retirement age): instead, we assess the average health effect attributable to leaving the labour market, differentiating by possible routes of exit.
Data and Method
Data and Sample
For our study, we used data from the longitudinal Survey of Health, Ageing and Retirement in Europe (SHARE) (Börsch-Supan et al., 2013), especially waves 1, 2, 4, 5 and 6, carried out respectively in 2004–2005, 2006–2007, 2010–2011, 2012–2013 and 2014–2015. We excluded waves 3 and 7, the retrospective SHARELIFE surveys. In each wave, SHARE data cover several key areas of life (health, socio-economic status, social and family networks, etc.) of more than 60,000 individuals aged 50 or over.
We focused on respondents aged between 50 and 70 years in the period between 2004 and 2015 and on a subset of the SHARE countries: those that participated in at least two consecutive waves – spanning 2 years from each other, except for waves 2 and 4 which span instead 4 years – and for which we had all the information that we needed for the analysis. Our transitions are those observed between waves 1 and 2; waves 2 and 4; waves 4 and 5; or waves 5 and 6. This means that each individual concurs to the sample with two consecutive observations: respondents must be employed at wave w and no longer employed (cases) or still in employment (controls) at wave w+1. We thus focus on the short-term effect of labour market exit on health (for a discussion, see Limitations and Strengths).
The countries included in the analysis are 15: Austria, Belgium, Czech Republic, Denmark, Estonia, France, Germany, Greece, Italy, the Netherlands, Poland, Slovenia, Spain, Sweden and Switzerland. Unfortunately, due to the limited dimension of our sample, we could not perform country-specific analyses.
Analytical Strategy
In our study, we applied a propensity score matching approach (paragraph Method), to identify the causal effect of leaving the labour market on various measures of health (paragraph Healt Outcomes), using a large set of individual information (paragraph Propensity Score Matching Variables). Very briefly, under a few assumptions, we estimate the effect of discontinuing one’s work (‘treatment’) on health by comparing two groups of individuals who are as similar as possible in all observed respects, except for the fact that, between two consecutive waves of the SHARE survey, some leave the labour market (treated individuals, or cases) and some do not (matched individuals, or controls). Any systematic difference in the health outcome between the two groups can therefore be interpreted as statistically ‘caused’ by the change in status.
In the first step of the analysis, we included all those who left the labour market, or leavers. These are those who stopped working between two consecutive waves, for any reason: they were employed at wave w, but not at wave w + 1.
Then, to investigate possible differences in the routes to retirement, we broke this group down into three subgroups, as follows (Table 1): Retirees: those who formally retired between two consecutive waves: they were employed at wave w, and formally retired at wave w + 1; Drop-outs: those who stopped working between two consecutive waves, but did not formally retire: they were employed at wave w, and either unemployed or looking after home/family, at wave w + 1; Sick and disabled: those who stopped working between two consecutive waves, but did not formally retire: they were employed at wave w, and permanently sick or disabled at wave w + 1. Cases (Three Types) and Controls Considered in this Analysis, Overall and by Sex (Aged 50 to 70 years, Several EU Countries, between 2004 and 2015). * Due to reduced sample size, we merged these two types, ignoring the differences between them. Source: SHARE data.
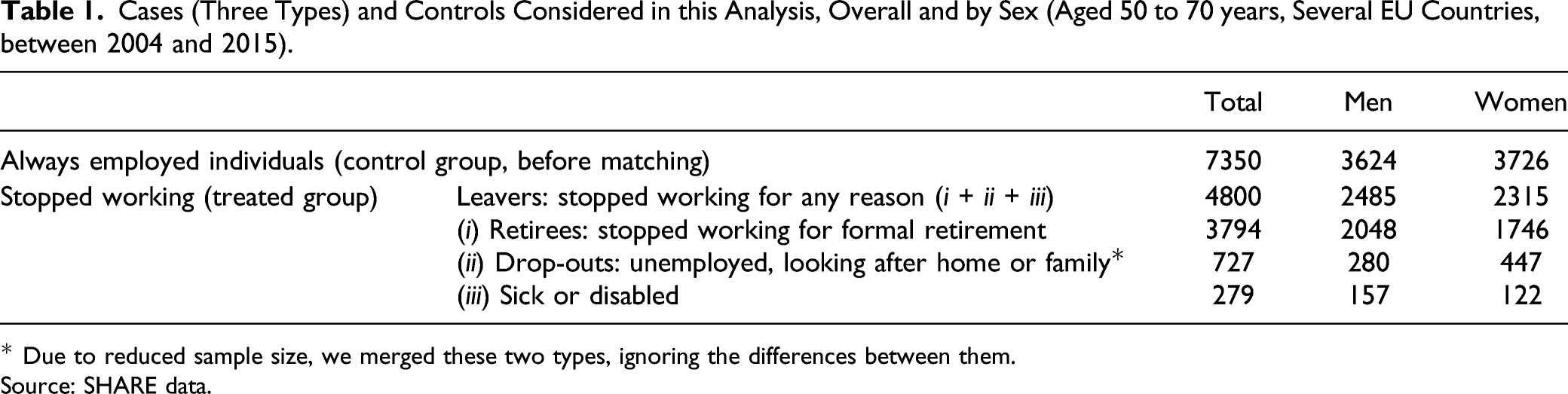
As the last group – the sick and disabled (3) – is small and highly selected, we decided to drop it. For the other groups instead we estimated the short-term health effect of leaving the labour market, keeping as a reference group those who remained in employment.
In the second step of our analysis, we estimated the health effect of ‘retirement’ highlighting the role of a few in our opinion relevant stratification variables.
Method
To estimate the effect on people’s health of exiting the labour market, we followed the potential outcome approach (e.g. Imbens & Rubin, 2015). For each individual i (1, …, n), we observed a vector X i of characteristics measured at wave w (pre-treatment characteristics). Let T i denote the treatment variable indicator, equal to 1 if individual i leaves the labour market between two consecutive waves of the survey, zero otherwise. Under the Stable Unit Treatment Value Assumption (Rubin, 1980, see Supplementary Appendix), for each individual i observed in employment at wave w there are two potential outcomes at wave w + 1, Y i (1) and Y i (0), if i does or does not leave the labour market, respectively.
A comparison of these potential outcomes, typically their difference, gives a measure of the causal effect of the transition out of the labour market. We consider the ATT, that is the average effect of this transition on those who actually leave the labour market
As we use observational (not experimental) data, we need two assumptions on the treatment-assignment mechanism. First, unconfoundedness, or ‘selection on observables’. Formally, this requires that, conditioning on observed covariates, the treatment assignment (leaving or not leaving the labour market) must be independent of the potential health outcomes ‒ T i ⊥ (Y i (0), Y i (1))|X i . Second, the overlap assumption requires that there is sufficient overlap in the distribution of the covariates between treated and control units, 0 < P(Ti=1|X i =x) < 1 for each i, which basically means that both come from overall comparable groups and that for each treated individual, a ‘corresponding’ control individual (with similar background characteristics) can be found.
This comparison is made through the propensity score, or the probability of leaving the labour market, estimated through a probit model in this case, conditional on the observed covariates. The propensity score is a balancing score: conditional on the propensity score, the distribution of the covariates is similar between treated and controls, and therefore independent of the treatment. If the unconfoundedness and the overlap assumptions hold, matching on the propensity score is sufficient to remove confounding, and what emerges (health effect) can be safely attributed to the treatment (exiting the labour market, in this case; Rosenbaum & Rubin, 1983).
In our case, we considered a large set of covariates covering demographic, social, economic, family and job-related aspects, thus capturing very many observed (and proxying also several unobserved) characteristics. We checked that the distributions proved comparable between treated and controls, and we also ran a sensitivity check (see Supplementary Appendix). Finally, with PSM, we selected a sub-group of controls, that is a group of individuals who remained in the labour market between two subsequent waves and who were as similar as possible to the treated, those who left it. The variables used to calculate the propensity score are listed in paragraph Propensity Score Matching Variable and in the Supplementary Appendix.
In selecting controls, we opted for a 1-to-1 nearest neighbour matching (Abadie & Imbens, 2011) with replacement. Among the potential controls (first row of Table 1), for each individual exiting the labour market we selected the closest control (still in the labour market at wave w+1, and with the closest propensity score), allowing a non-treated individual to be used more than once as a match. More details on the technical aspects of the matching procedure (i.e. caliper, common support and balancing before and after matching) are discussed in the Supplementary Appendix.
Health Outcomes
We evaluated the health differences between treated and control units – or between those who did and did not leave the labour market – considering three health outcomes measured at wave w + 1. First, we used the frailty index, a 40-item index validated on the SHARE dataset, measuring the number of accumulated health deficits (Romero-Ortuno & Kenny, 2012). It summarizes individual frailty both in objective (e.g. grip strength and body mass index) and subjective terms (e.g. self-reported health and mood). The count of deficits for each person is divided by 40 (total number of possible deficits considered), so that individuals in good health score 0, while individuals in the worst possible health conditions score 1.
Next, we used a composite indicator of depression constructed from the 12 basic items of the EURO-D scale (Prince et al., 1999): depressed mood, pessimism, suicidality, guilt, sleep, interest, irritability, appetite, fatigue, concentration, enjoyment and tearfulness. This scale, ranging between 0 (not depressed) and 12 (severe depression), was developed to derive a common scale of depression symptoms, especially in late life, on different indicators in several European countries. We divided this count by 12, so that individuals with good mental health score 0, while individuals with severe depression score 1.
Finally, as is commonly done in this area of research (e.g. Voss et al., 2020), we considered also a general measure of health, self-perceived health, dichotomizing the original 5-point scale into 0=good (excellent, very good or good) and 1=poor (fair or poor).
Propensity Score Matching Variables
A critical issue in the design phase of an observational study is the choice of the pre-treatment variables conditional on which unconfoundedness and overlap assumptions are reasonable. To this end, a large and representative set of pre-treatment characteristics – all measured at wave w, prior to retirement to avoid the endogeneity problem – has been accurately selected. We based this selection on a priori substantive knowledge of the phenomenon (e.g. Caliendo & Kopeinig, 2008) derived from the literature on retirement-health relationship. Below, we list the variables used for the probit estimation of the propensity score: more details about the coding of these variables and the balancing of the propensity score are reported in the Supplementary Appendix.
First, in the specification of the propensity score we included various measures of health. Accounting for the health status prior to retirement is fundamental to control for potential selection, as bad health itself can push individuals out of the labour force. We included the same three health measures used as outcomes in the subsequent wave w + 1: self-perceived health, frailty index and depression. In addition, to account for other possible aspects linked to physical health, we also considered self-reported hearing and eyesight difficulties, limitation in activities of daily living (ADL) and in instrumental activities of daily living (IADL), mobility limitations, the global activity limitation indicator (GALI), the presence of chronic diseases, grip strength and obesity. We added controls for smoking and physical activity, two important health-related behaviours.
Second, we considered several socio-demographic characteristics, potentially linked to both health and labour market exit: gender, age and age squared, education and subjective evaluation of one’s own economic situation. We kept into account the country of residence, to capture, at least roughly, unobserved characteristics differentiating individuals in our sample.
Third, we introduced the family network, controlling whether the respondent had a partner, if at least one parent was still alive, the number of siblings, children and grandchildren, and the household size.
Job-related characteristics form the fourth set of variables included in the estimation of the propensity score, as these are possible confounders in the link between labour market exit and health: type of contract and job satisfaction as declared by the respondent. To account for a potential anticipatory element, we also included the preference, expressed in wave w, to retire as early as possible from the current job.
Results
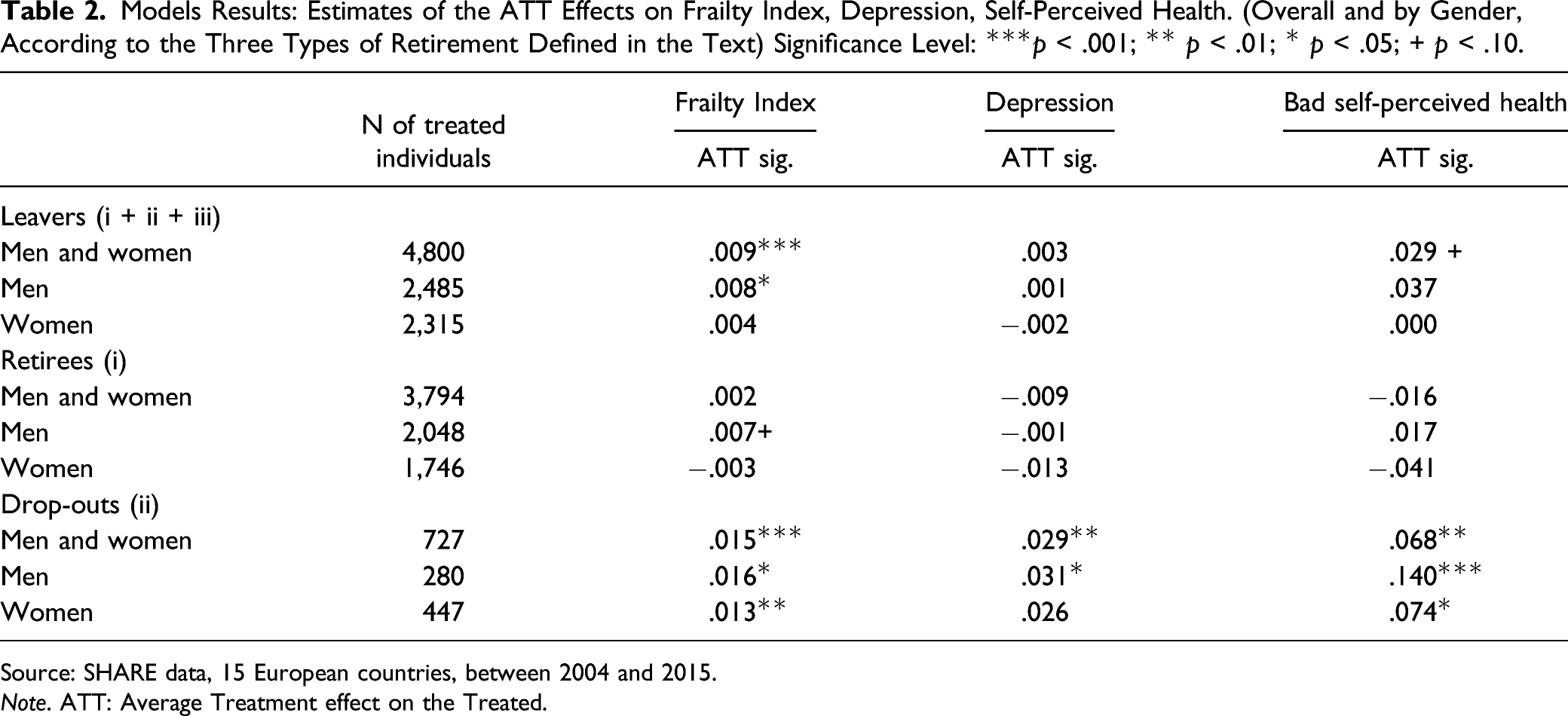
Models Results: Estimates of the ATT Effects on Frailty Index, Depression, Self-Perceived Health. (Overall and by Gender, According to the Three Types of Retirement Defined in the Text) Significance Level: ***p < .001; ** p < .01; * p < .05; + p < .10.
Source: SHARE data, 15 European countries, between 2004 and 2015.
Note. ATT: Average Treatment effect on the Treated.
First, let us consider the more comprehensive group of leavers. Leaving the labour market, at least between 50 and 70 years of age, seems to cause a general deterioration of health, especially in terms of frailty, although the magnitude of the effects is small.
This negative effect, however, depends on the route to labour market exit. Formal retirement (i) does not appear to affect health in our sample, in either way (a slightly worsening effect, significant at 10% level, can be detected only for the frailty index of men). Conversely, those who leave their job not because of formal retirement but for other reasons, the drop-outs (ii), later suffer from worse health conditions, for all the three health indicators considered here. In this case, the magnitude of these ATT effects is far from negligible, equalling .015, .029 and .068 respectively for frailty, depression and self-perceived health, with even higher values for men. Those who stopped working because of unemployment and family reasons, generally showed higher frailty levels, a higher number of depressive symptoms, and more frequently declared to be in poor health. This finding confirms what has generally been found in the literature: when discontinuing work is not a (totally) free decision, as it probably happens in these cases, distress, depression and a deterioration of both objective and subjective health may ensue (e.g. Daly and Delaney 2013).
These results bear, we believe, two relevant implications. The first is that a precise definition of ‘retirement’ is necessary to determine the direction and magnitude of the health effects of an interruption in one’s labour activity because of the different mechanisms behind this passage. The second is that remaining at work, even at relatively high ages, is not detrimental for health – and this is particularly important in an epoch when raising retirement ages seems to be one of the necessary tools to preserve the viability of pension systems.
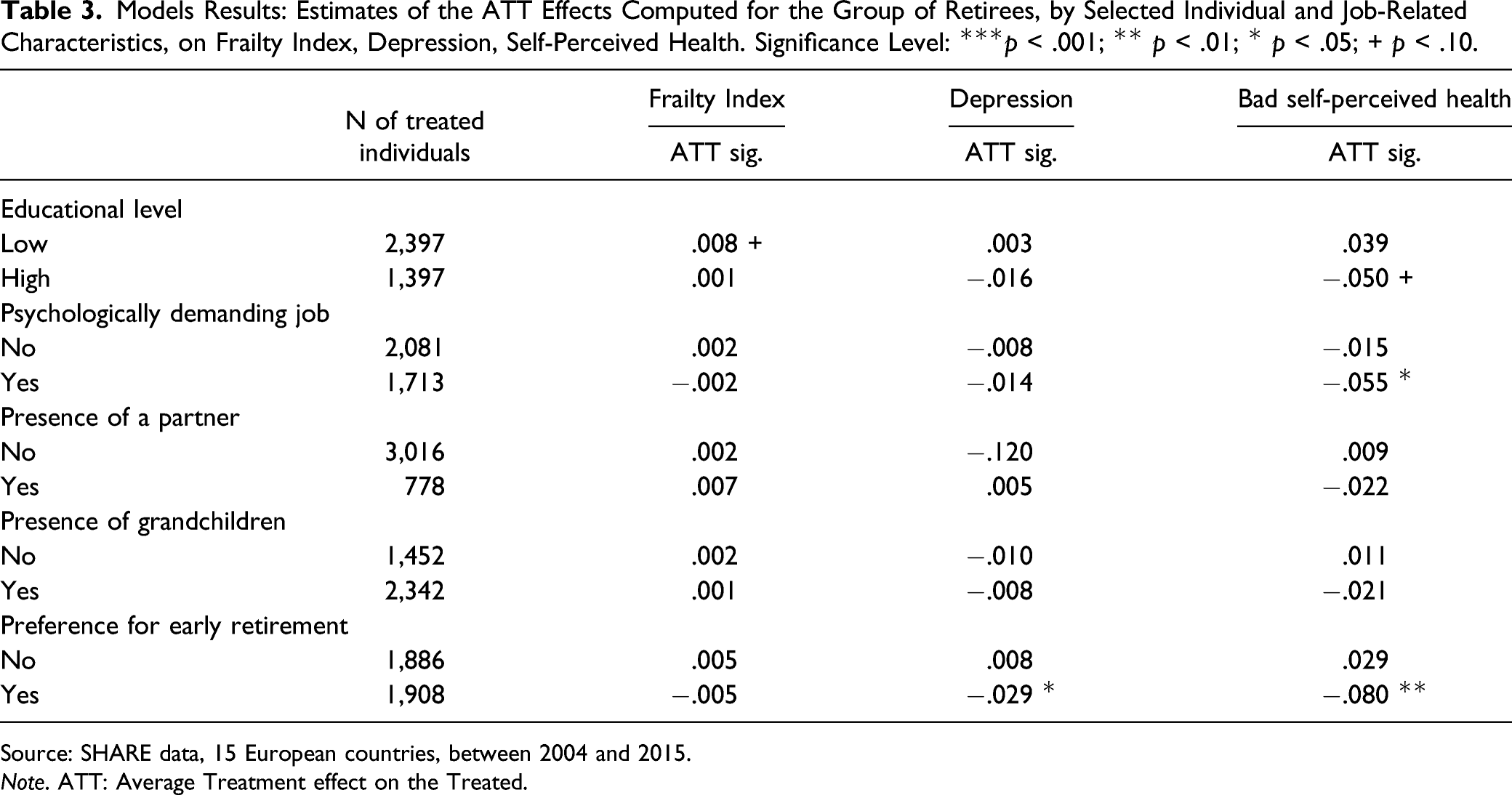
Models Results: Estimates of the ATT Effects Computed for the Group of Retirees, by Selected Individual and Job-Related Characteristics, on Frailty Index, Depression, Self-Perceived Health. Significance Level: ***p < .001; ** p < .01; * p < .05; + p < .10.
Source: SHARE data, 15 European countries, between 2004 and 2015.
Note. ATT: Average Treatment effect on the Treated.
Some differences emerge by educational level: lower education is associated with slightly worse health conditions after retirement (i.e. .008 for the frailty index), even if this is not significant for depression (.003) or self-perceived health (.039). Instead, a beneficial effect of retirement on perceived health emerges for the highly educated (−.050), and for those who had a psychological demanding job (−.055). These results are slightly more robust for women (not shown). The presence of a partner or grandchildren has positive effects on the self-perceived health of women (not shown), but these effects disappear when considering simultaneously men and women. Finally, as expected, those who longed for retirement improve after reaching it, both in terms of depression (−.029) and self-perceived health (−.080).
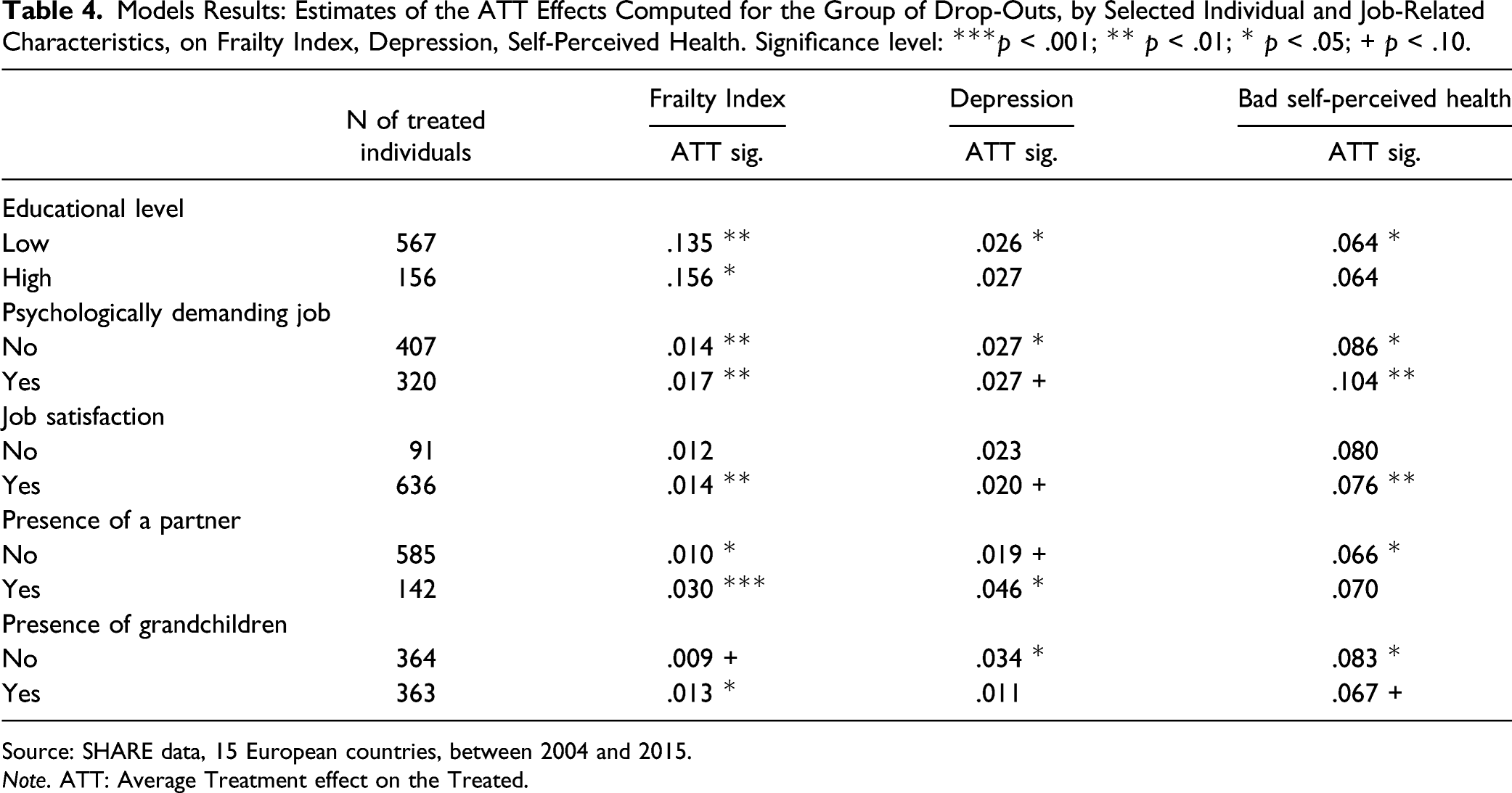
Models Results: Estimates of the ATT Effects Computed for the Group of Drop-Outs, by Selected Individual and Job-Related Characteristics, on Frailty Index, Depression, Self-Perceived Health. Significance level: ***p < .001; ** p < .01; * p < .05; + p < .10.
Source: SHARE data, 15 European countries, between 2004 and 2015.
Note. ATT: Average Treatment effect on the Treated.
The results about the presence of a partner reported in Table 4 are interesting, but they hide remarkable gender differences. In particular, health deteriorates for the men who do not have a living partner, while for women it is the presence of a partner that is linked to worse health. The presence of grandchildren does not have relevant impact on health, for either sex.
Discussion
In this study, we analyzed the health consequences of leaving the labour market in a group of European countries in recent times. Our purpose was to clarify three main issues. First, we applied a propensity score matching approach, a relatively rare technique in this field of study, which the rich set of pre-treatment variables available in the SHARE data made possible. These refer to health, lifestyle behaviours, demographic, social and family traits, and job-related features, and enabled us to minimize the possible influence of ‘confounders’ on the relation of interest. Second, we considered different pathways out of the labour market because, as we suspected and as it turned out, results depend on the very definition of ‘retirement’. Third, we estimated the health effect of exiting the labour market differentiating by various individual and job-related characteristics.
We considered three different measures of health: the frailty index (a composite measure including objective and subjective aspects); a common and reliable measure of depression, the Euro-D scale; and self-perceived health, the quintessential indicator of subjective health.
Our results highlight the importance of considering the routes that lead a mature worker out of the labour market. Loose definitions of retirement, such as ‘all those who, past a certain age (e.g. 50 years), leave their occupation for whatever reason’ may lead to wrong conclusions. In fact, formal retirement itself has virtually no effect on health, either good or bad. This is good news, in our opinion: health concerns cannot be used as an argument against postponing the retirement age in case of need, for instance, for the safeguard of pension systems. Rather, increased effort should be put in keeping mature people at work, even when difficulties emerge, either in the labour market (unemployment) or in the family sphere: those who quit their job for these reasons are worse off – at least, shortly after retirement, the only effect that we could measure. Our findings are essentially independent of the health indicator considered: all of them signal a worsening of health when the labour market is abandoned for reasons other than formal retirement.
Our results also emphasize that individual and job-related characteristics may shape the relationship between labour market exit and health, highlighting the need for a research strategy that accounts for pre-retirement characteristics – including pre-existent health conditions – and workers’ heterogeneity. In line with previous literature (e.g. Zantinge et al., 2014), a modest positive health effect emerges for the highly educated and for those who found their job demanding, according to the idea that retirement may represent a relief for workers ‘under pressure’. Not surprisingly, those who expressed a preference for early retirement report lower depression and improved self-perceived health after retirement. Focusing on the subgroup of drop-outs for unemployment or family reasons, the negative effect – which is generally present – is stronger for the low educated, possibly because their possibilities of re-employment are lower. The family context, especially the presence of a partner, matters as well, with gender differences. Health worsens for men without a partner and for women with a partner. A possible explanation lies in the caregiver role traditionally played by women, who may have to leave the labour market to look after family members in need (i.e. a sick or disabled relatives); conversely, men who leave the labour market before retirement suffer from the lack of a partner on whom to rely. Unfortunately, our data do not permit us to verify this conjecture.
Overall, we showed that it is not possible to identify a unique link between labour market exit and health: individual heterogeneity plays an important role in shaping health outcomes.
Limitations and Strengths
Our study has a number of limitations. First, the panel nature of our sample reduced the number of observations, which resulted in large standard errors: incidentally, this could explain why several parameters, while with the expected sign, did not prove significant. Moreover, due to the reduced sample size, we could not go into greater detail, and we were forced to ignore country differences, for instance, which may be relevant because of the specificity of their welfare and social protection systems (Richardson et al., 2019).
A second limitation of this study is its time frame: health consequences may emerge after a longer interval than we could cover here. We are aware that we focus only on the short-term health effects of retirement, and that we cannot measure the possible evolution of these effects, including, for example, the so-called ‘honeymoon phase’ for the newly retired, who are happy at first, but perhaps less so in the long run (Hershenson, 2016). On the other hand, limiting our study to a two-wave span allows us to minimize attrition, and maximize our sample size. Attrition could potentially be problematic for studies on health and retirement because of selection (people in worse health are more likely to drop out of the panel). In SHARE data, attrition is high, ranging between 30% (when two consecutive waves are considered, 2 years apart) and 50% (when the interval between waves reaches 4 years). However, if a bias were present, it would lead to an underestimation of the effects that we measure here, because people in poor health are more likely to exit the panel. Besides, the large number of variables considered in our PSM (also in terms of health) makes the two groups highly similar (cases and controls: see Supplementary Figure A1 and Supplementary Table A2 in the Supplementary Appendix), which reinforces confidence in our findings.
In our analysis we could not distinguish those who have literally just exited the labour market (a few days before the interview) from those who transitioned ‘long’ before (up to 2 years; even up to four in the passage from wave 2 to wave 4 of the SHARE rounds). For the subgroup of the retirees, however, we have the exact date of retirement: in this case, we verified that the distribution of these retirement periods is at random, and that including it in the analysis leaves the results unchanged (not shown here but available upon request).
Another potential limitation of our study, typical of the PSM approach followed here, is due to unobserved factors, which could invalidate the unconfoundedness assumption. This is something that, by definition, cannot be verified. However, we controlled for a very large set of pre-treatment characteristics, including health, precisely to minimize the risk of selection and reverse causality. We also simulated the presence of potential unobserved confounders (see Supplementary Appendix), and the results of this robustness check indirectly supports our claim that no unobserved confounders remain once controlling for the large set of observed characteristics.
Perhaps the most important lesson to be learnt from our study is the importance of distinguishing the routes out of the labour market: retirement proper vs. unemployment/family obligations. These groups differ in terms of characteristics (e.g. resources) and health consequences, which are non-existing for formal retirees, but clearly visible (and negative) for the others. We deem that this study, by using PSM technique, further contributes to a better understanding of the inconsistencies of previous findings on the influence of labour market exit on health.
Conclusion
Leaving the labour market in one’s mature years (between 50 and 70 years of age) is a more complex transition than it may seem. Formal retirement is the most frequent case, but there are several other ways out and these alternatives (e.g. unemployment and family reasons) are associated with markedly worse health outcomes. Future research should focus on understanding and combating the causes of premature exit from the labour market, a reason of concern not only in economic terms but also on health grounds in the light of our findings.
Our results suggest that labour market attachment, even at relatively high ages, does not damage health, thus reinforcing the idea that longer labour market participation is possible: all in all, this is good news in an era of rapid population ageing and endangered sustainability of pension systems.
Between 50 and 70 years, individuals are exposed to age-related exclusionary forces, such as biological health decline and the shrinking of support network, and face limited possibility of re-entering the labour market (e.g. OECD 2011, 2019). Back in 2002, the World Health Organization coined the expression ‘active ageing’ to define a policy framework for ‘optimizing opportunities for health, participation and security in order to enhance quality of life as people age’ (WHO 2002, p. 12). In addition to all actions aiming at promoting an engaged life, especially for more disadvantaged people (e.g. Lee et al., 2019), our results suggest that more comprehensive policy measures (Boudiny, 2013) are worth pursuing to reduce the risk of obsolescence and avoid age discrimination and the stigmatization of unemployment episodes. For instance, companies could offer recalibration and reshaping of workloads, time commitments, and types of tasks, according to the skills and phases of the life course of the worker. Re-training and up-skilling programs may help sustain or even improve the professional contribution, competitiveness and, in case of need, re-employability of mature workers. Besides, welfare schemes and systems of flexible working hours should keep into account the needs of those who are forced out of the labour market for family reasons (e.g. to take care of sick relatives), which could also boost female participation.
Getting back to work is sometimes possible, even if difficult: when this happens, the wellbeing of these mature workers improves (Voss et al., 2020). Some categories of workers are especially problematic: they suffer from higher risks of dropping out of the labour market, have worse health consequences in these cases, and are the most difficult to re-employ. These are cases that merit special attention.
Supplemental Material
sj-pdf-1-jah-10.1177_08982643211039637 – Supplemental Material for Retirement? Other Ways Out of the Labour Market Are Far More Worrying for Health: Results from a Matching Approach Study
Supplemental Material, sj-pdf-1-jah-10.1177_08982643211039637 for Retirement? Other Ways Out of the Labour Market Are Far More Worrying for Health: Results from a Matching Approach Study by Elena Pirani, Gustavo De Santis and Francesca Zanasi in Journal of Aging and Health
Footnotes
Acknowledgments
This paper uses data from SHARE Waves 1, 2, 3, 4, 5 and 6 (DOIs: 10.6103/SHARE.w1.710, 10.6103/SHARE.w2.710, 10.6103/SHARE.w3.710, 10.6103/SHARE.w4.710, 10.6103/SHARE.w5.710, 10.6103/SHARE.w6.710), and see Börsch-Supan et al. (2013) for methodological details. The SHARE data collection has been funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782) and by DG Employment, Social Affairs and Inclusion. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science and the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see ![]() ). We thank Alessandra Mattei for her advice on the use of the PSM technique.
). We thank Alessandra Mattei for her advice on the use of the PSM technique.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
We gratefully acknowledge financial support from the 2016 JPI-MYBL (Joint Programme Initiative - More Years Better Lives), CREW Project (“Care, retirement and wellbeing of older people across different welfare regimes”), Decree: n. 3266/2018.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.