
Abstract
Introduction
There is extensive research that has identified a variety of key risk factors for dementia incidence; however, the majority of this research has focused on individual-level characteristics such as age, education, health conditions, and lifestyle behaviors (Alzheimer’s Association, 2021). Consequently, there is limited research investigating contextual risk factors, such as neighborhood physical and social environment (Guo et al., 2019). In fact, a systematic review on the association between neighborhood environment and cognitive function indicated that the majority of existing studies use compositional measurements such as community-level socioeconomic status and deprivation, whereas few studies investigate contextual measurements that include features of built or social environment in local areas (Wu et al., 2015).
Although measurements often vary, multiple indices for neighborhood economic disadvantage and neighborhood deprivation are frequently associated with adverse cognitive outcomes (Besser et al., 2017; Guo et al., 2019; Letellier et al., 2018). Specifically, neighborhoods with high proportion of blue collar workers, low household income, and high unemployment are significantly associated with an increased risk of dementia onset (Letellier et al., 2018). As for perceived neighborhood characteristics, one study recently identified lower neighborhood safety, lower esthetic quality, greater perceived neighborhood crime, and lower neighborhood cohesion are significant stressors associated with lower performance in spatial abilities, working memory, and executive function (Muñoz et al., 2020).
In contrast, neighborhood features that have been found to benefit cognitive health include greenspace and parks (Chen et al., 2022), accessibility to libraries, school campuses, and arts/cultural sites (Finlay, Yu, et al., 2021; Guo et al., 2019), and high sidewalk coverage (Tani et al., 2021), which are likely attributed to an increased engagement in physical, social, and intellectually stimulating activities. This is in line with studies that have documented positive associations between cognitive function and a neighborhood’s density of physical and institutional resources. Residing in a neighborhood with a greater density of physical resources such as recreational centers and parks, fitness/sports amenities, walkable destinations, proximity to public transit, and business density are associated with lower rates of cognitive decline (Clarke et al., 2015; Finlay, Esposito, Li, Colabianchi, et al., 2021). Furthermore, living in neighborhoods with greater availability of institutional resources such as eateries, senior centers, and civic/social organizations are associated with higher levels of cognitive function (Finlay, Esposito, Li, Kobayashi, et al., 2021). These findings indicate the critical role of both neighborhood physical and social infrastructures in buffering cognitive decline among older adults aging in place.
It is also well-documented there are persistent racial and ethnic disparities in dementia risk. In particular, previous research has indicated that Black and Hispanic older adults have disproportionately higher prevalence and incidence rates for dementia. Several studies have indicated that compared to White older adults, Black and Hispanic older adults have approximately a 2 and a 1.5 times increased risk for dementia, respectively (Alzheimer’s Association, 2021). Despite this disparity, there is no consensus on the key causes and pathways accounting for these racial and ethnic differences in dementia risk (Steenland et al., 2015).
Linked to social position and ethnicity, place of residence has drawn an increasing scholarly interest toward understanding inequalities in health (Diez Roux & Mair, 2010); however, the socio-contextual determinants for such disparities in cognitive health are not well understood for minority older adults. Among the limited research examining how neighborhood characteristics contribute to cognitive health in diverse samples of older adults, one study reported greater perceived neighborhood problems (e.g., low social cohesion, low safety from crime) were associated with lower global cognition and memory in Hispanic/Latina women (Estrella et al., 2020). Another study found that unfavorable perceived neighborhood characteristics (e.g., unclean, low safety, low social cohesion) were associated with lower cognitive functioning among White older adults with less education, Black older adults with more years of education, and Mexican older adults with less education (Thierry et al., 2021).
Another set of studies aimed to explore the associations between neighborhood racial-ethnic composition and cognitive decline; however, mixed findings were reported. One study found that neighborhood Black composition and Black-White segregation did not have a significant influence on cognitive aging (Kovalchik et al., 2015); whereas other studies found that individuals living in neighborhoods with a higher clustering of Black residents had slower declines over time on episodic memory (Meyer et al., 2021) and non-Hispanic Black adults were the most likely to experience negative effects of neighborhood segregation on cognition and dementia (Pohl et al., 2021). Among Hispanic older adults, one study found that higher neighborhood Hispanic composition and greater Hispanic-White segregation were significantly associated with faster cognitive decline (Kovalchik et al., 2015). In contrast, another study documented lower baseline scores in highly clustered Latino neighborhoods, but slower declines on semantic memory (Meyer et al., 2021). Research elucidating disparities in dementia risk is critical given that the U.S. population is not only rapidly aging, but also becoming increasingly more diverse. According to a 2020 Brookings report, the U.S. Census Bureau estimated that the 2010 to 2020 decade was the first time in the nation’s history in which the White population declined in numbers, and nearly four in ten Americans identified with a racial or ethnic group other than White (Frey, 2020).
In summary, the review of the existing literature indicates several gaps and limitations in our current knowledge on dementia research. First, contextual risk factors for dementia risk are understudied (Guo et al., 2019; Wu et al., 2015). Second, multiple systematic reviews on the relationship between neighborhood and cognition have revealed the vast majority of this published research is cross-sectional, and recommend future research integrate longitudinal neighborhood measures (Besser et al., 2017; Chen et al., 2022; Estrella et al., 2020; Wu et al., 2015). Third, mechanisms for racial and ethnic disparities in dementia risk are poorly understood, and disparities research that includes neighborhood characteristics are especially limited (Steenland et al., 2015).
Our present study addresses these gaps by analyzing nine years of prospective longitudinal data for a nationally representative U.S. older adult sample. To the best of our knowledge, our study is the first to examine how neighborhood environment is linked to racial and ethnic disparities in dementia risk using a national longitudinal data set. Our specific objectives include the following: (1) Examine differences in neighborhood physical disorder and social cohesion by racial and ethnic group among older adults, (2) Examine how neighborhood physical disorder and social cohesion are associated with dementia risk among older adults, and (3) Examine how race and ethnicity moderates the relationship between neighborhood characteristics and dementia risk among older adults.
Methods
Data Source
Data were retrieved from the National Health and Aging Trends Study (NHATS), a longitudinal panel study that surveys a nationally representative sample of Medicare beneficiaries age 65 and older within the United States. Nine annual waves between 2011 and 2019 of the NHATS were used for this study. Our final sample included 5181 community-dwelling older adults without a prior dementia diagnosis and self-identified as either non-Hispanic White, non-Hispanic Black, or Hispanic.
Dementia Diagnosis Measure
The dependent variable was incident dementia diagnosis, which occurred during the eight-year period between 2012 and 2019, after the removal of pre-existing dementia diagnoses at baseline (2011). Dementia diagnosis was derived from an NHATS algorithm (Kasper et al., 2013) that uses three cognitive measures: (1) AD8 Dementia Screening Interview (Galvin et al., 2005) that assesses memory, temporal orientation, judgment, and function, (2) Cognitive tests that evaluate the respondents’ memory (e.g., immediate 10-word recall), orientation (e.g., date), and executive function (e.g., clock drawing test), and (3) Self-report of an AD or dementia diagnosis by a doctor.
From these cognitive measures, respondents were categorized into three groups: no dementia, possible dementia, or probable dementia. We collapsed these categories into a binary variable for a broad definition of dementia (possible or probable diagnosis), which the NHATS has tested to have a high sensitivity of 85.7% when compared to dementia diagnoses in a consensus expert panel from the Aging, Demographics and Memory Study (ADAMS) (Kasper et al., 2013).
Neighborhood Measures
The two independent variables related to neighborhood characteristics were physical disorder and social cohesion, which were each measured with separate composite scores. The neighborhood physical disorder composite score was developed from a three-item home environment questionnaire: litter, graffiti, and vacancies. For each item, the NHATS interviewer was asked, “When standing in front of the sample person’s home/building, and looking around in every direction, how much of the following did you see?” (None, A little, Some, or A lot). Litter was defined as, “Litter, broken glass, or trash, on sidewalks and streets.” Graffiti was defined as, “Graffiti on buildings and walls.” Vacancies was defined as, “Vacant or deserted houses or storefronts.” After combining these three measures, physical disorder composite scores ranged from 0 to 9, with higher values indicating neighborhoods with more physical disorder.
Similarly, the neighborhood social cohesion composite score was developed from a three-item community environment questionnaire: knowing, helping, and trusting. For each item, respondents were asked to rate their agreement (Do not agree, Agree a little, or Agree a lot). Knowing was asked as, “People in this community know each other very well.” Helping was asked as, “People in this community are willing to help each other”. Trusting was asked as, “People in this community can be trusted.” After combining these three measures, social cohesion composite scores ranged from 0 to 6, with higher values indicating neighborhoods with more social cohesion.
These composite scores for physical disorder and social cohesion were constructed at baseline (2011), follow-up (year before death, drop-out, or dementia diagnosis), and change (follow-up compared to baseline). The regression models included only the baseline and change composite scores to limit multicollinearity due to follow-up composite scores.
Race and Ethnicity Measure
The NHATS constructed a race and ethnicity variable with several categories: non-Hispanic White (hereafter, White), non-Hispanic Black (hereafter, Black), Hispanic, other, or multiracial. This variable was derived from questions that included “What race do you consider yourself to be?” and “Do you consider yourself Hispanic or Latino?” We restricted our sample to older adults who self-identified as either White, Black, or Hispanic.
Covariates
Regression models were adjusted for sociodemographic and health variables. Sociodemographic variables included age, sex (male or female), highest level of education (less than high school, high school, or college), total income, marital status (married or unmarried), total number living in household, and metropolitan residence (metro or non-metro). Health variables included self-rated health (poor to excellent), body mass index, limitations for activities of daily living (no ADL limitations or at least one ADL limitation), proxy respondent, major depressive disorder, generalized anxiety disorder, history of heart attack, history of hypertension, history of diabetes, and history of stroke.
Analysis Plan
Descriptive statistics for continuous variables were reported as mean and standard deviation, whereas categorical variables were reported as frequencies and proportions. Racial and ethnic differences in average neighborhood physical disorder and social cohesion were analyzed using ANOVA tests. We used Cox proportional hazards models to analyze time (number of years) to dementia diagnosis starting from baseline (2011). All regression models applied complex survey sampling weights and adjusted for sociodemographics and health. Statistical analyses were performed in Stata statistical software version 16 (StataCorp LLC, College Station, TX, USA) with two-tailed tests at a 0.05 significance level.
Results
Sample Characteristics
Among the 5181 respondents in the sample, most self-identified as White (74.7%) followed by Black (20.4%) and Hispanic (4.9%). During the nine-year study window from 2011 to 2019, about 27.5% (n=1423) of the sample met the criteria for an incident dementia diagnosis. The highest incident cases were among Hispanic older adults (42.4%, n=108), followed by Black (33.2%, n=351) and White (24.9%, n=964) older adults.
Baseline Sample Characteristics.
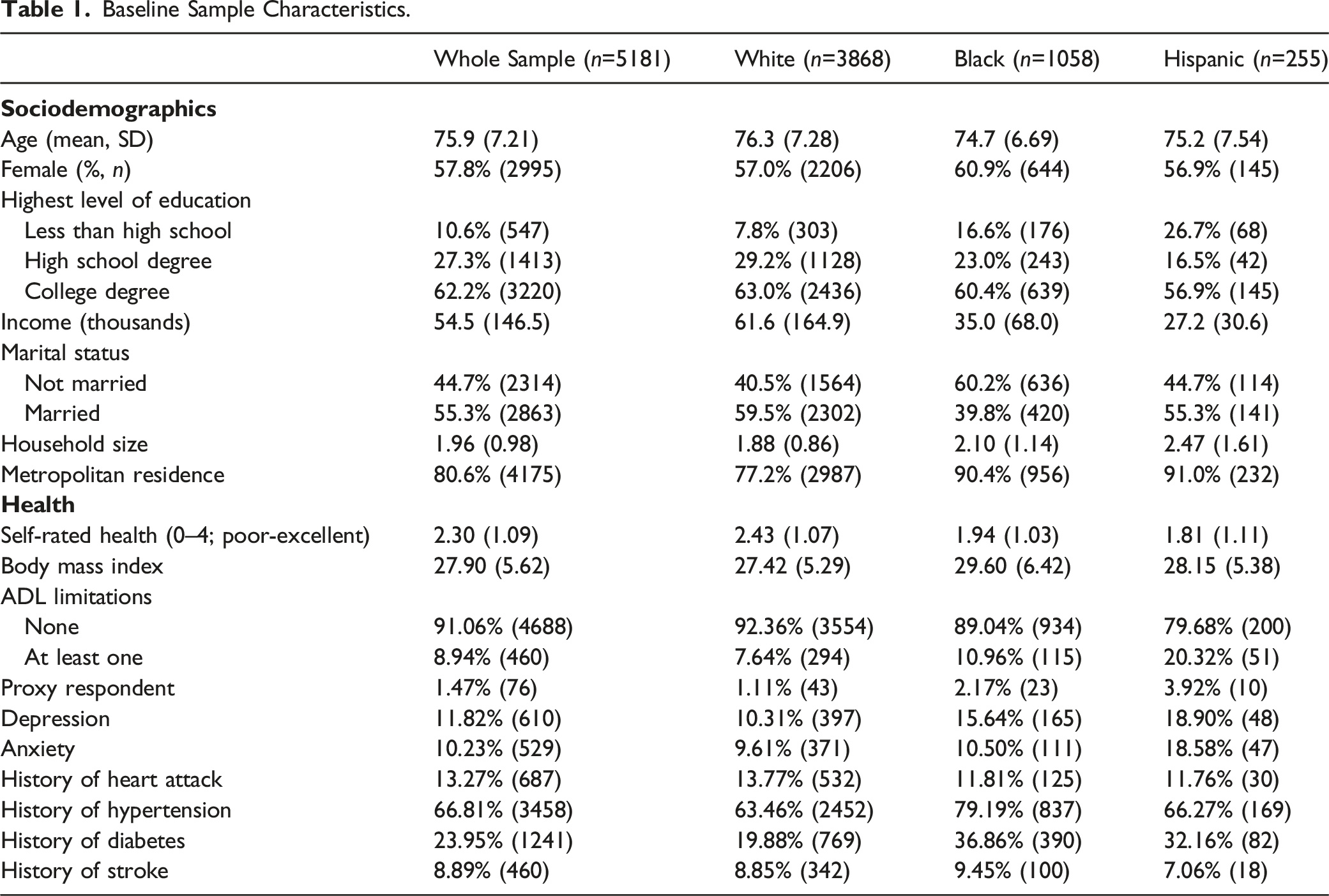
In terms of their health, the average self-rated health was 2.30 (SD=1.09), which is between “good” (2) and “very good” (3) health. The majority (91.1%) did not have any functional impairments in ADLs and had an average BMI of 27.9 (SD=5.62), indicating most respondents were overweight. For mental health, approximately 11.8% had major depressive disorder and 10.2% had generalized anxiety disorder. The most common chronic diseases were history of hypertension (66.8%) and diabetes (24.0%).
Bivariate Results
Physical disorder
Neighborhood Physical Disorder and Social Cohesion by Race and Ethnicity.
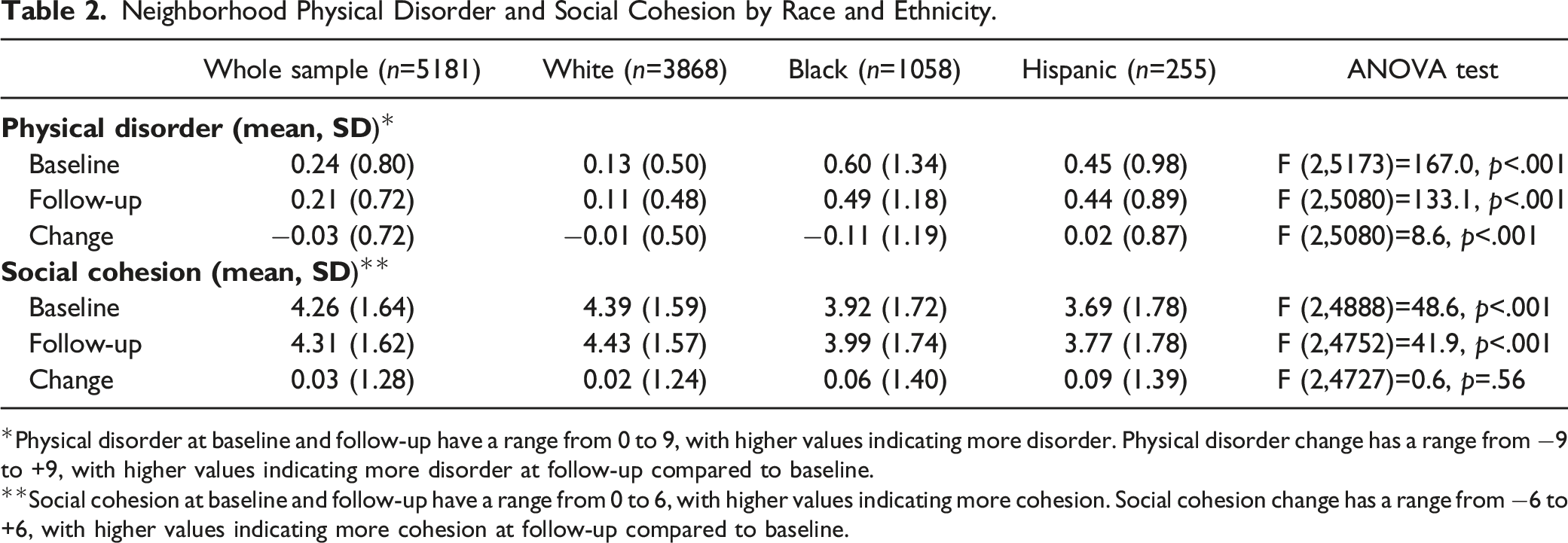
*Physical disorder at baseline and follow-up have a range from 0 to 9, with higher values indicating more disorder. Physical disorder change has a range from −9 to +9, with higher values indicating more disorder at follow-up compared to baseline.
**Social cohesion at baseline and follow-up have a range from 0 to 6, with higher values indicating more cohesion. Social cohesion change has a range from −6 to +6, with higher values indicating more cohesion at follow-up compared to baseline.
Social Cohesion
Among the three racial and ethnic groups of interest, Hispanic older adults resided in neighborhoods with the lowest levels of social cohesion at baseline (mean=3.69, SD=1.78) and follow-up (mean=3.77, SD=1.78) (Table 2). Compared to White older adults, Black older adults resided in neighborhoods with elevated levels of social cohesion at baseline (mean=3.92, SD=1.72) and follow-up (mean=3.99, SD=1.74). Relative to White and Black older adults, Hispanic older adults had the highest increased positive change for neighborhood social cohesion at follow-up compared to baseline on average. These racial and ethnic differences in neighborhood social cohesion were statistically significant only for composite scores at baseline and follow-up, but not for change at follow-up compared to baseline.
Cox Regression Results
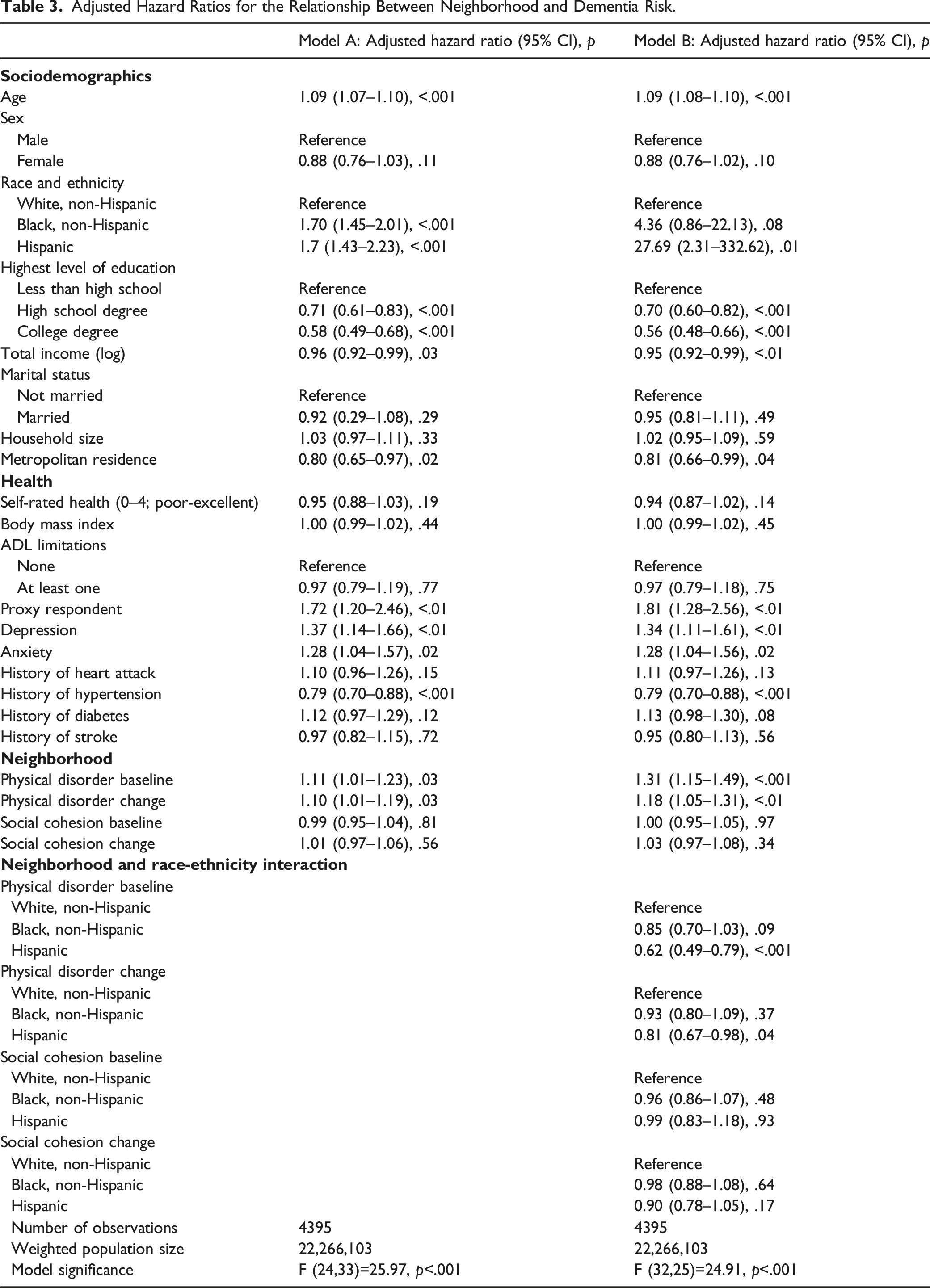
Adjusted Hazard Ratios for the Relationship Between Neighborhood and Dementia Risk.
Moderation Effects
When examining the moderating effect of race and ethnicity on the relationship between neighborhood characteristics and dementia risk, there was only a significant interaction for neighborhood physical disorder (Table 3, Model B). Figure 1 visualizes the results for the moderating role of race and ethnicity between baseline physical disorder and dementia. Each of the three racial and ethnic groups (White, Black, Hispanic) are displayed with survival curves for the two most extreme baseline physical disorder scores (zero physical disorder, and maximum physical disorder). Compared to White older adults, Hispanic older adults living in neighborhoods with high physical disorder at baseline had a significantly lower dementia risk (aHR=0.62, 95% CI=0.49–0.79, p<.001) after adjusting for sociodemographics and health. Interaction Between Race-Ethnicity and Baseline Physical Disorder on Dementia-Free Survival. Notes. PD=Physical Disorder. Zero PD indicates no physical disorder and Max PD indicates maximum physical disorder in a neighborhood.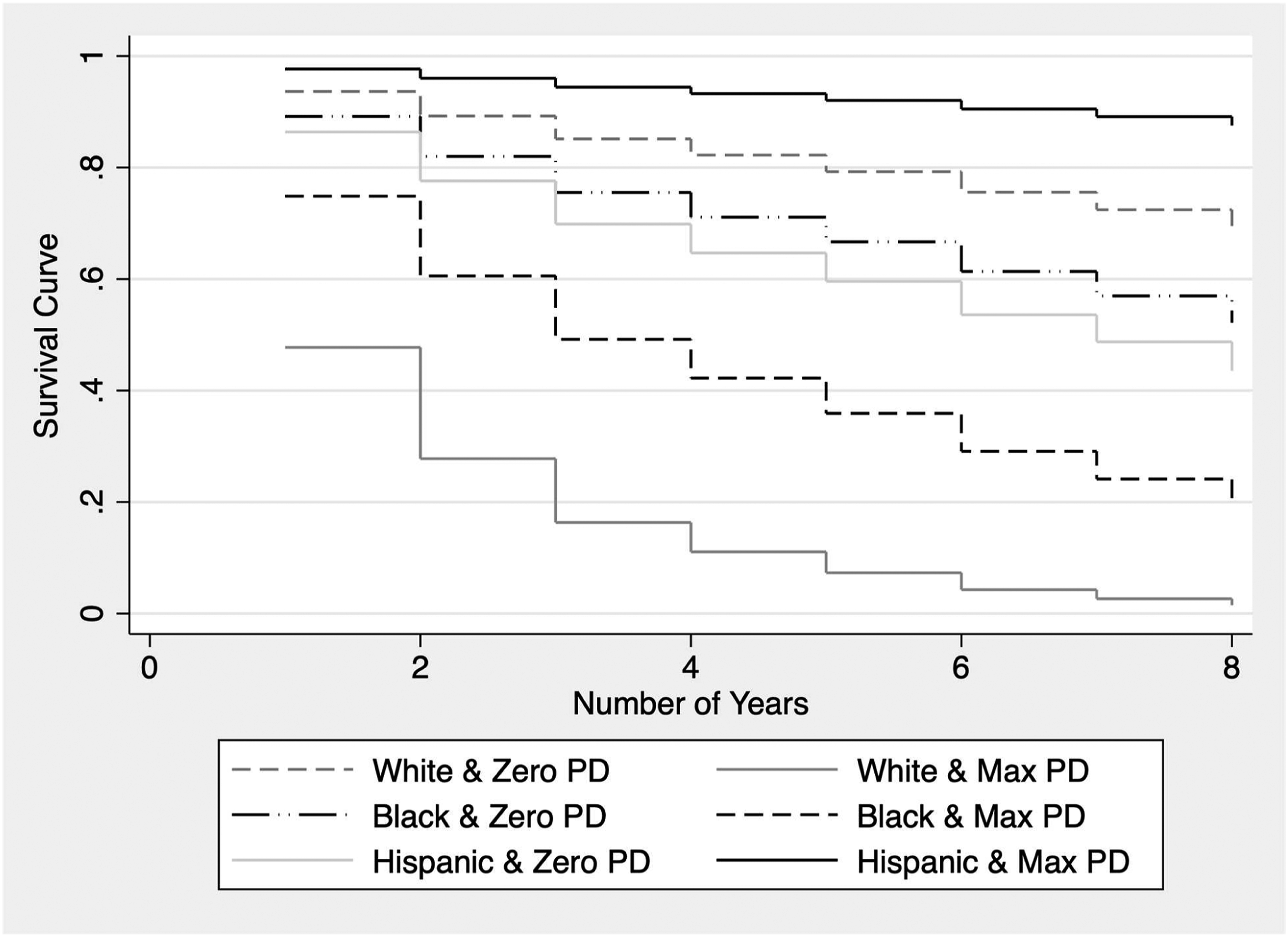
Similar to Figures 1 and 2 visualizes the results for the moderating role of race and ethnicity between physical disorder change at follow-up and dementia. Each of the three racial and ethnic groups (White, Black, Hispanic) are displayed with survival curves for the two most extreme changes in physical disorder (no change in physical disorder, and maximum increase change in physical disorder). Compared to White older adults, Hispanic older adults living in neighborhoods with higher physical disorder at follow-up compared to baseline had a significantly lower dementia risk (aHR=0.81, 95% CI=0.67–0.98, p=.04). There were no significant interactions for Black older adults based on physical disorder at baseline (aHR=0.85, 95% CI=0.70–1.03, p=.09) and change in physical disorder (aHR=0.93, 95% CI=0.80–1.09, p=.37). In addition, there was no significant interaction between race-ethnicity and social cohesion, for both baseline and change in neighborhood social cohesion. Interaction Between Race-Ethnicity and Change in Physical Disorder on Dementia-Free Survival. Notes. PD=Physical Disorder. Zero PD Change indicates no change in physical disorder and Max PD Change indicates maximum physical disorder at follow-up compared to baseline.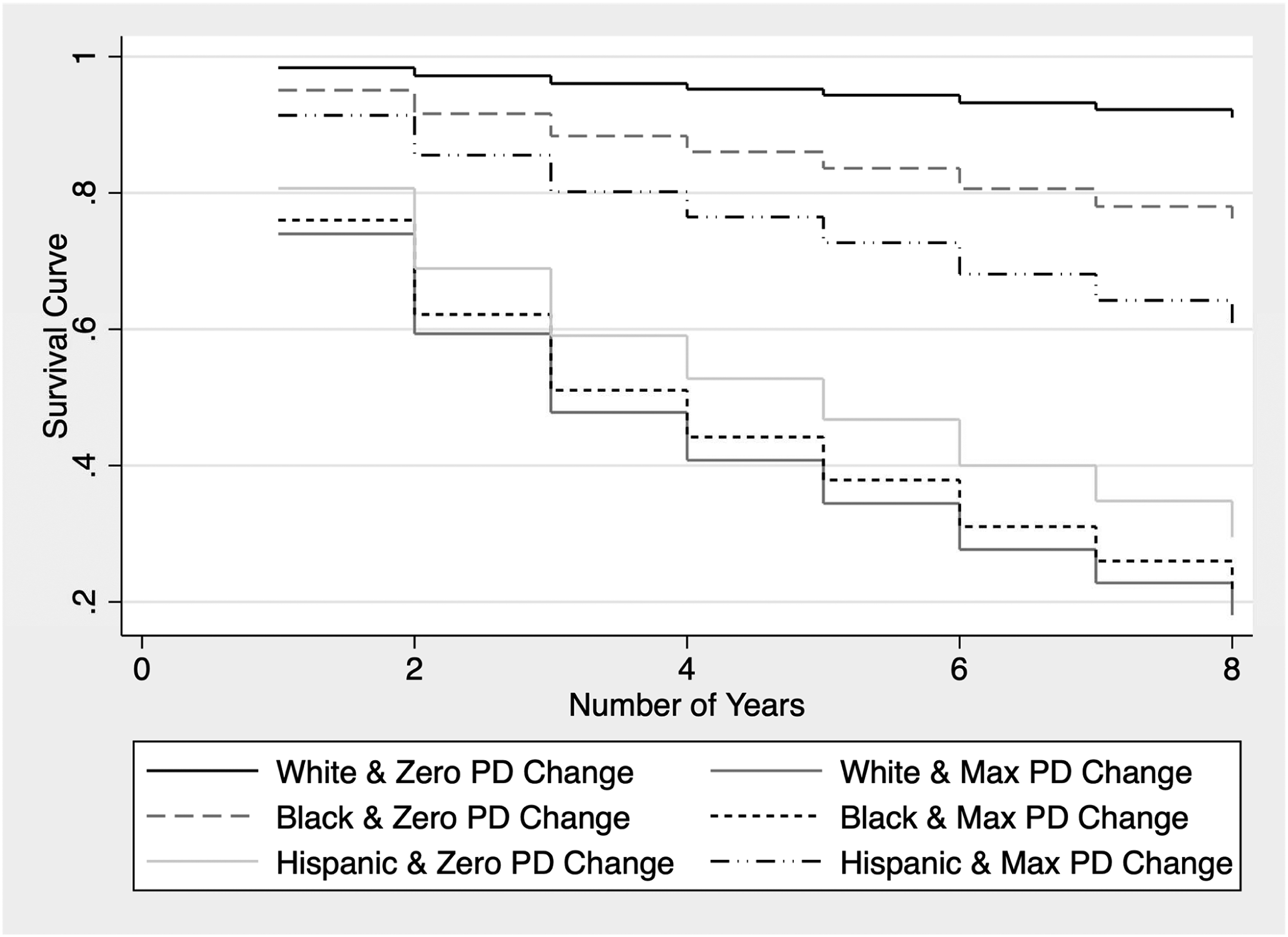
Discussion
Our study found that physical, but not social characteristics of a neighborhood are significantly associated with dementia risk. Specifically, for both baseline and change (follow-up compared to baseline), higher physical disorder in neighborhoods were associated with an increased dementia risk. This finding is consistent with previous studies that have found older adults living in neighborhoods with high physical disorder was significantly associated with worse episodic memory (Zaheed et al., 2019) and lower verbal fluency cognitive scores (Sharifian et al., 2020). Neighborhood built environment provides the foundation for active, healthy, socially engaging, and cognitively stimulating activities. Therefore, one frequently proposed mechanism for our finding is that neighborhoods with high levels of physical disorder may create fear, anxiety, and psychological stress, which further prevents older residents from meaningful engagement and worse cognitive function over time (Sharifian et al., 2020).
As for the social domain, our findings showed no significant associations between neighborhood social cohesion and dementia risk. This was unexpected because theoretically, neighborhood social environments, such as social capital and social cohesion, have benefits such as greater perception of control, increased sense of mastery, and positive mental health outcomes, which all protect or improve cognitive health in later life (Wu et al., 2015). Our null finding, however, is similar to prior research that argues that the inconsistent or null findings on the relationship between neighborhood social climate and cognitive function are likely attributed to cross-sectional study designs (Estrella et al., 2020). Despite analyzing nine years of longitudinal data in our present study, we still found no meaningful relationships between neighborhood social cohesion and dementia.
Other studies that reported mixed findings have also considered the influence of neighborhood racial-ethnic composition and separation. Several studies indicate racial-ethnic composition and segregation may be differentially associated with cognitive outcomes depending on individual race/ethnicity, and such disparities in cognitive outcomes may be attributed to the downstream effects of structural racism (e.g., unequal distributions of wealth/resources) (Meyer et al., 2021; Pohl et al., 2021). In contrast, another study suggests Black neighborhood composition and Black-White segregation does not significantly influence cognitive aging (Kovalchik et al., 2015). Based on these conflicting findings, neighborhood racial and ethnic composition is a complex factor needing further exploration in the literature.
Compared to White older adults, we found Hispanic older adults in neighborhoods with high physical disorder at baseline, and high physical disorder at follow-up compared to baseline, had a significantly decreased dementia risk. This surprising finding may be due to unique protective effects from cultural factors, such as multilingualism and multigenerational households. Unlike other racial and ethnic groups, Hispanic adults in the United States typically speak more than one language (Krogstad & Gonzalez-Barrera, 2015). Previous research indicates that multilingualism is associated with enhanced executive function and may thus prevent cognitive decline and reduce the risk of dementia (Hack et al., 2019). In addition, Hispanic Americans tend to have larger, multigenerational households compared to White adults (Marquez-Velarde, 2020). Likewise, our research found a higher average household size among Hispanic older adults (2.5 people) compared to White (1.9 people) and Black (2.1 people) older adults in our sample. The multilingual ability and larger support network among Hispanic older adults could increase cognitive reserve and thereby decrease dementia risk (Stern et al., 2020).
Given that Hispanic adults in the United States are more likely to be immigrants and older immigrants may opt to live in neighborhoods with high ethnic concentrations, another explanation for this finding could be that such ethnic neighborhoods, despite the physical disorder, may provide access to economic, social, and cultural resources for coping and adaptation (Yang et al., 2020). The physical and mental health benefits of living in ethnic enclaves among immigrants have been well-documented (Aranda et al., 2011; Gerst et al., 2011; Osypuk et al., 2009; Zhang et al., 2020), and such benefits may offset the disadvantages in the neighborhood physical domain and be extended to cognitive health.
Ultimately, further research is needed to understand the protective mechanisms for dementia risk among Hispanic older adults residing in neighborhoods with high physical disorder. Likewise, future research should explore potential pathways linking neighborhood to cognitive health disparities, such as through the mediating role of physical and social activities. Although the focus of our study was on racial and ethnic disparities in dementia, prior research has also indicated that neighborhoods with higher physical deprivation and physical disorder have a greater adverse impact on women, by significantly increasing dementia risk (Letellier et al., 2018) and decreasing global cognition and memory (Estrella et al., 2020). Therefore, the interaction between sex, race and ethnicity, and neighborhood on dementia risk would be worthwhile to explore in future research.
There were three limitations for our study. First, the physical disorder measure was collected by the NHATS interviewers, which could have limited inter-rater reliability due to differences when assessing the physical characteristics of neighborhoods. Second, our composite score for physical disorder and social cohesion were each comprised of three measures, which may not each weigh equally for their respective constructs. Third, our dementia diagnosis variable is limited by the short battery of neuropsychological tests administered in the NHATS, which had an average completion time of about 7 minutes compared to other national data sets such as the Aging, Demographics, and Memory Study (ADAMS) with a neuropsychological test completion time between 90 and 100 minutes. The NHATS dementia variable has been tested to demonstrate high sensitivity and sufficient specificity compared to dementia diagnosis based on the ADAMS consensus expert panel. In addition, dementia prevalence rates are similar between the NHATS and the Health and Retirement Study (HRS), particularly for older adults above age 70 (Kasper et al., 2013). Despite these limitations, to the best of our knowledge, this study presents the first examination of the relationship between neighborhood, race and ethnicity, and dementia using a prospective, nationally representative older adult sample.
Conclusions
Our study indicates that physical characteristics of neighborhood communities are an important social determinant of health linked to dementia. Residing in neighborhoods with high physical disorder has been shown to increase mental health disorders and decrease the ability to engage in healthy lifestyle behaviors (Barnett et al., 2018), which may ultimately elevate dementia risk. We also found racial and ethnic minority older adults more frequently reside in neighborhoods with higher physical disorder and lower social cohesion. Despite these unfavorable environments, additional research is needed to understand mechanisms that may be reducing dementia risk for racial and ethnic minorities, particularly among Hispanic older adults residing in neighborhoods with high physical disorder.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgments
National Health and Aging Trends Study (NHATS) is sponsored by the National Institute on Aging (grant number U01AG32947) and was conducted by the Johns Hopkins University.
Ethical Approval
This study was ethically approved by the Institutional Review Board for the Protection of Human Subjects at SUNY Upstate Medical University under project number 1,771,240–1.