
Abstract
Objectives
This study explored how coping moderates the association between discrimination and health outcomes in lesbian, gay, and bisexual (LGB) and heterosexual midlife and older adults.
Methods
This study analyzed longitudinal data from 163 LGB and 326 propensity-matched heterosexual midlife and older adults over approximately 20 years, using the Midlife in the United States study.
Results
Discrimination was associated with slower chronic condition accumulation over time for LGB individuals. Problem-focused and avoidance coping moderated discrimination’s impact on mental health in LGB participants over time, and in heterosexual participants, they moderated the association between discrimination and chronic conditions.
Discussion
The results suggest a potential “steeling” effect in LGB midlife and older adults facing higher discrimination levels. Furthermore, the findings suggest that effective coping strategies for mitigating the adverse impacts of discrimination on physical and mental health may vary by sexual orientation.
Introduction
In recent years, research has unveiled significant disparities in the experiences and health outcomes of lesbian, gay, and bisexual (LGB) older adults compared to their heterosexual counterparts. These disparities are marked by elevated rates of discrimination against LGB older adults (Fredriksen-Goldsen, 2017a; Lee et al., 2016; Lehavot & Simoni, 2011), which, in turn, are linked to higher rates of both physical and mental health challenges (Hoy-Ellis & Fredriksen-Goldsen, 2016; Jackson et al., 2019; Wallace et al., 2011). Despite these adversities, most LGB older adults in the United States are aging successfully as they report good health, engage in health-promoting behaviors, and have supportive social networks (Fredriksen-Goldsen et al., 2015; Grossman et al., 2000; Van Wagenen et al., 2013). While previous research on LGB older adults has largely been deficit-focused, an increasing number of studies have started to investigate the strengths and protective factors that may help mitigate the harmful effects of discrimination on the health of this marginalized population.
Yet, a critical gap persists. Longitudinal studies that investigate the relationship between discrimination and the physical and mental health of LGB midlife and older adults remain scarce. Existing longitudinal research in LGB health has predominantly focused on younger age groups (e.g., adolescents or young adults) (Burton et al., 2013; Hatzenbuehler et al., 2008), making it challenging to generalize findings to older LGB individuals. While a recent study noted that LGB older adults experienced fewer increases in chronic conditions over time compared to heterosexual participants (Nelson & Andel, 2020), it did not include a measure of discrimination. To our knowledge, no study has comprehensively examined the moderating effects of problem-focused and avoidance coping on the associations between discrimination and LGB health over time, particularly in comparison to heterosexual adults. Therefore, this study aims to answer the research question: Do the effects of discrimination on the health outcomes of LGB midlife and older adults differ over time compared to their heterosexual counterparts, and how do the use of problem-focused and avoidance coping strategies influence these effects?
Conceptual Framework
This study aims to fill this gap in the literature by investigating the intricate interplay between discrimination, coping strategies, and the health trajectories of LGB older adults. Drawing on the Health Equity Promotion Model (HEPM), an intersectional framework designed to foster health equity and move beyond deficit-focused perspectives, this study explores the multifaceted dimensions of this relationship (Fredriksen-Goldsen et al., 2014). The HEPM expands upon established stress and coping models such as the Minority Stress Model (Meyer, 2003) and the Psychological Mediation Framework (Hatzenbuehler et al., 2008), which primarily focus on examining stressors and psychological mechanisms (mediation), including coping, linking experiences of discrimination and stigma to health outcomes in minority populations. These models emphasize stress and its mediating effect on health. The HEPM provides a broader perspective by encompassing intersecting social positions (e.g., race, age, socioeconomic status, and gender), multilevel contexts (e.g., individual- and structural-level minority stressors), and both health-promoting and adverse pathways, making it a more comprehensive framework for understanding the intricate dynamics shaping the health of LGB individuals across the lifespan (see Figure 1). The health equity promotion model (Fredriksen-Goldsen et al., 2014).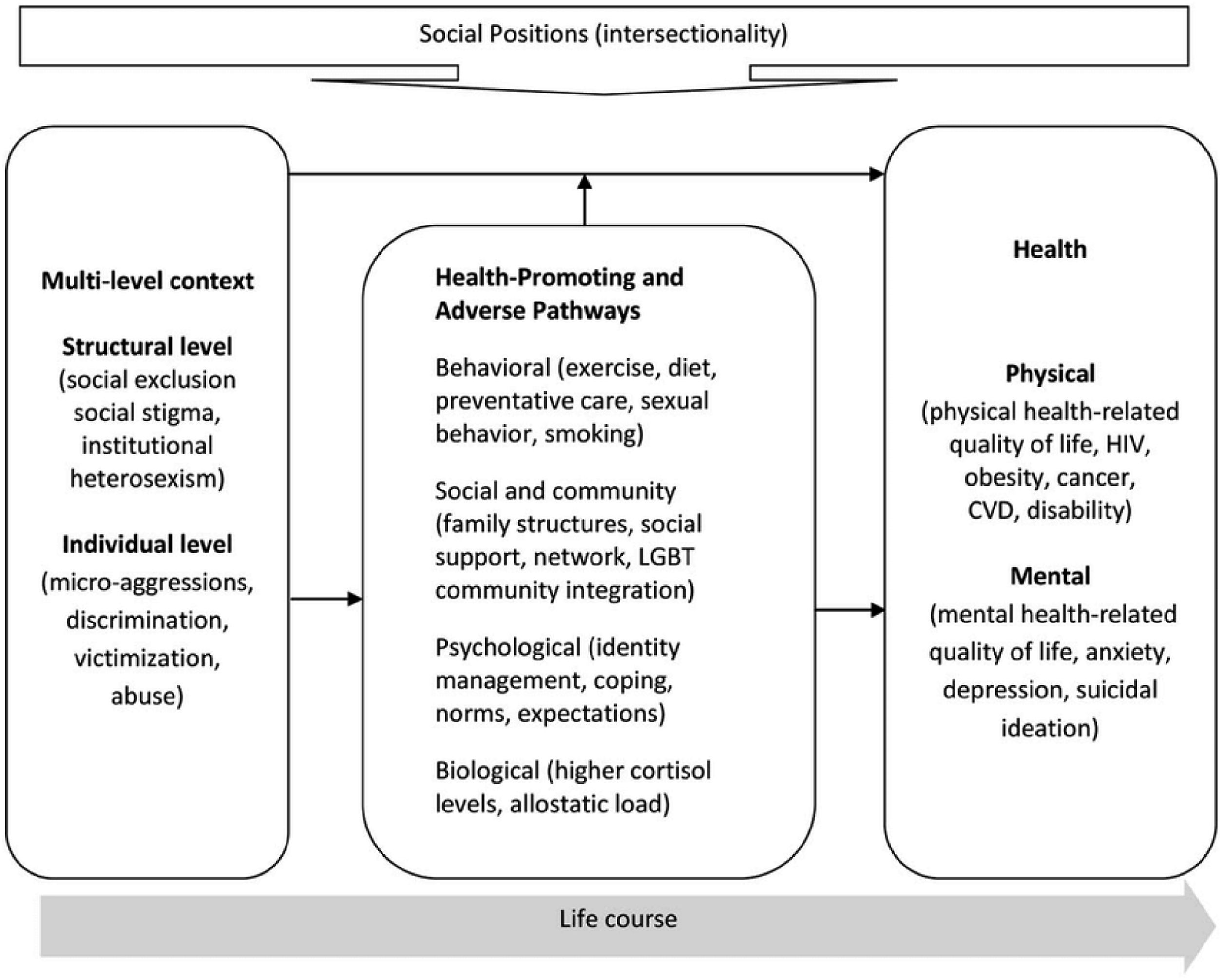
Discrimination
LGB individuals have been found to be twice as likely as their heterosexual counterparts to encounter both lifetime discrimination (e.g., denied a bank loan) and day-to-day discrimination (e.g., insulted or threatened), even when accounting for factors such as age, sex, race, and education (Mays & Cochran, 2001). In this study, discrimination is operationalized as the frequency of experiencing various forms of daily mistreatment, including being treated with less courtesy, less respect, receiving poorer service, being called names or insulted, and being threatened or harassed. While both heterosexual and LGB older adults may encounter discrimination based on various factors, LGB individuals are disproportionately affected by discrimination related to their sexual orientation. The HEPM accounts for the complexity of these intersecting social positions and life experiences in shaping LGB physical and mental health outcomes.
Existing research reveals that discrimination among LGB midlife and older adults is associated with diminished quality of life (Mays & Cochran, 2001), compromised physical health (Feinstein et al., 2022; Nelson et al., 2022), mental health challenges (Feinstein et al., 2022; Walch et al., 2016), increased risk of problematic drinking (Bryan et al., 2017), and substance use (Bränström & Pachankis, 2018). However, the HEPM acknowledge that discrimination may not always result in poor health outcomes. Some LGB individuals, despite facing discrimination, manage to sustain good physical and mental health by leveraging health-promoting processes like coping, which they have developed throughout their life experiences (Fredriksen-Goldsen et al., 2014).
Coping
This manuscript delves into the role of coping in this intricate interplay. Within the HEPM, coping is acknowledged both as a positive, health-promoting psychological process and as an adverse one, contingent upon the type of coping strategies employed (Fredriksen-Goldsen et al., 2014). Coping, broadly defined, encompasses cognitive and behavioral strategies used to navigate stressors (Lazarus & Folkman, 1984). Common conceptualizations categorize coping as problem-focused versus emotion-focused, active versus passive, and approach versus avoidance (Solberg et al., 2022). For the purposes of this study, problem-focused coping denotes actively engaging with stressors by formulating solutions or action plans, while avoidance coping involves disengaging from stressors either emotionally or cognitively.
In studies across various populations that did not assess sexual orientation, individuals utilizing problem-focused coping techniques had better physical and/or mental health compared to those employing avoidance coping techniques (e.g., Kidd & Carroll, 2007; Moos et al., 1990; Roesch et al., 2005). Among studies involving LGB adults, avoidance coping mediated the association between minority stress and mental health (Choi et al., 2016; Kaysen et al., 2014; Szymanski & Owens, 2008; Zheng et al., 2020), while problem-focused coping did not exhibit the same mediating effect (Flenar et al., 2017; Kaysen et al., 2014; Szymanski & Owens, 2008). It is important to note that the LGB studies examining coping primarily used cross-sectional designs, with Choi and colleagues (2016) utilizing a longitudinal design, but only spanning twelve months. These studies also did not include a heterosexual comparison group to examine any differences by sexual orientation and primarily included younger samples (i.e., mean age less than 30 years).
The Current Study
This study conducts a longitudinal analysis of coping mechanisms in LGB midlife and older adults to evaluate their potential as moderators in the complex relationship between discrimination and health outcomes. The study also performs a comparative analysis with heterosexual adults, offering insights into disparities related to sexual orientation and age group. Leveraging longitudinal data from the Midlife in the United States (MIDUS) study, the study investigates the distinct moderating roles of problem-focused and avoidance coping in the context of perceived daily discrimination (referred to as “discrimination”), examining their influence on physical and mental health over approximately 20 years.
Research Aims and Hypotheses
This study had two aims: (1) examine differences in the associations between discrimination and the health outcomes over time for LGB and heterosexual adults, and (2) assess how problem-focused and avoidance coping moderate the association between discrimination and health over time for LGB and heterosexual adults. For the first aim, based on previous findings, it was predicted that (1) compared to heterosexual participants, higher discrimination would be associated with a significantly greater increase in the number of chronic conditions over time and a significantly greater decrease in self-rated mental health over time for LGB participants. For the second aim, it was hypothesized that, (2a) problem-focused coping would moderate the effect of discrimination on the health outcomes for heterosexual participants only, mitigating the adverse effects of discrimination over time, and (2b), avoidance coping would moderate the association between discrimination and changes in health over time for both LGB and heterosexual participants. Specifically, higher utilization of avoidance coping would intensify the adverse effect of discrimination on the health outcomes.
Methods
Data
Data for this study were from the main survey of waves 1, 2, and 3 of MIDUS, a nationally representative, multidisciplinary study of midlife and older adults. MIDUS is one of few longitudinal studies of midlife and older adults to include a measure of sexual orientation (National Academies of Sciences, Engineering, and Medicine, 2020). For the first wave of the MIDUS study (MIDUS 1, 1995–1996), participants were chosen via random telephone digit dialing procedures, resulting in 7108 adults. Participants gave verbal consent and completed a 45-min telephone interview. After the telephone interview, participants were mailed two self-administered questionnaires. The second wave of the MIDUS study (MIDUS 2) took place from 2004 to 2006. Of the 7108 adults that participated in the first wave, 4963 continued to participate in the second wave, completing both assessments again (MIDUS 2 retention rate = 69.8%). The third wave (MIDUS 3), following the same procedures as previous waves, was conducted between 2013 and 2015, with 3294 participants completing the assessments (MIDUS 3 retention rate = 46.3%).
Sample
MIDUS participants are English-speaking adults living in the conterminous United States (i.e., 48 states, not including Hawaii and Alaska) (Radler & Ryff, 2010). For this study, only participants who responded to the sexual orientation question during MIDUS 1 were considered for the analyses (n = 6314). Participants that were missing data on the variables of interest at MIDUS 1 (baseline) were excluded (n = 387). At baseline (MIDUS 1), 94 participants identified as homosexual (gay/lesbian), 74 as bisexual, and 5958 as heterosexual. Homosexual and bisexual participants were grouped into a LGB group. In total, 163 participants with complete data identified as a LGB during MIDUS 1. A 2:1 propensity score matched heterosexual group was identified using propensity score matching as described in the statistical analyses section. The heterosexual group only included participants that identified as heterosexual and never identified as a LGB in any of the waves. The final analytical sample (n = 486) included 163 LGB participants and 326 propensity-matched heterosexual participants at baseline.
Measures
Number of Chronic Conditions
In each wave, participants were asked “In the past twelve months, have you experienced or been treated for any of the following” for 30 chronic conditions including migraine headaches, stroke, diabetes, AIDS/HIV, thyroid disease, and chronic sleep problems. The number of chronic conditions ranged from 0 to 30. However, to make this a measure of physical health only, the two chronic conditions related to mental health were excluded: “anxiety, depression, or some other emotional disorder” and “alcohol or drug problems.” Therefore, the total sum of chronic conditions ranged from 0 to 28.
Self-Rated Mental Health
For the self-reported measure of current mental health, participants were asked “Would you say your mental or emotional health is excellent, very good, good, fair, or poor?” on a scale of 1 (poor) to 5 (excellent). Self-rated mental health was treated as a continuous variable for this study with higher scores indicating better mental health.
Sexual Orientation
Sexual orientation was assessed with one measure: “How would you describe your sexual orientation? Would you say you are heterosexual (sexually attracted only to the opposite sex), homosexual (sexually attracted only to your own sex), or bisexual (sexually attracted to both men and women)?” For this study, homosexual (i.e., lesbian and gay) and bisexual participants were combined into the LGB group (coded as 1). Propensity score matching was conducted to create a propensity-matched heterosexual group (coded as 0).
Perceived Daily Discrimination
For perceived daily discrimination, participants were asked “How often on a day-to-day basis do you experience each of the following types of discrimination?” such as being treated with less courtesy than other people, being treated with less respect than other people, receiving poorer service, being called names or insulted, or being threatened or harassed. Responses ranged from 1 (never) to 4 (often). The scores were summed to create the perceived daily discrimination variable with scores ranging from 9 to 36.
Coping Styles
The moderator variables for this study were problem-focused coping and avoidance coping. In MIDUS, coping was measured using 26 items from six subscales of the COPE (Carver et al., 1989). Two subscales were used to assess problem-focused coping (active coping and planning), and two subscales were used to assess avoidance coping (denial and behavioral disengagement). Each subscale was assessed with four items that asked participants about what they generally do and feel when they experience stressful situations. Each item ranged from 1 (not a lot) to 4 (a lot). Subscales were constructed by calculating the sum of the items in each subscale. Problem-focused coping was the sum of the 8 items in the active coping and planning subscales (Cronbach’s α = .89). Avoidance coping was the sum of the 8 items in the denial and behavioral disengagement subscales (Cronbach’s α = .70). Scores ranged from 8 to 32 with higher scores indicating higher use of each coping style. Coping was not assessed in MIDUS 1; therefore, this study used coping data from MIDUS 2.
Covariates
The covariates for this study included age (in years), sex (0 = male and 1 = female), education (0 = high school graduate or less and 1 = some college education or more), marital status (0 = not married and 1 = married), employment status (0 = not currently employed and 1 = employed), and race (0 = race other than white and 1 = white). These covariates were selected as they have been found to be associated with health disparities (Adler & Newman, 2002; Hughes & Waite, 2009).
Statistical Analyses
All analyses were conducted using SAS, version 9.4 (SAS Institute Inc, Cary, NC). First, propensity score matching (Parsons, 2004) was conducted to match two heterosexual participants to each LGB participant. Propensity-score matching reduces the influence of confounding variables in nonrandomized studies (Austin, 2011; Haukoos & Lewis, 2015). Propensity scores were estimated using a logistic regression adjusted for baseline age, sex, education, and race. After obtaining propensity scores, a greedy propensity matching add-on macro in SAS was used to match two heterosexual participants to each LGB participant. Standardized mean differences were calculated to assess the balance in matching covariates (age, sex, education, and race) between LGB and heterosexual groups after propensity score matching (Baek et al., 2015). Standardized differences in the matching covariates that are <.1 indicate successful balancing between the two groups. Chi-square and t-test analyses were conducted to examine differences in the measures being used for this study that were not matching covariates between the LGB and matched heterosexual groups.
Next, using PROC GENMOD in SAS, generalized estimating equation (GEE) analyses with negative binomial distribution were conducted to assess the association between discrimination and the number of chronic conditions over approximately 20 years. Negative binomial GEE analyses are often used with count variables that are skewed due to many responses at the lower end such as having many participants with zero chronic conditions at baseline (Zeileis et al., 2008). Since the regression coefficients for the negative binomial GEE models were log-transformed, the coefficients were exponentiated to create interpretable values in the form of incidence rate ratios (IRR). To test hypothesis 1, first, a GEE model was conducted with the three-way interaction term “time x discrimination x sexual orientation” to assess if there was a difference in the association between discrimination and number of chronic conditions over time by sexual orientation. Second, additional GEE analyses were conducted separately for the LGB group and the matched heterosexual group to further examine the nature of the interaction effects by sexual orientation. The same two-step approach was applied to the hypothesis for self-rated mental health, where a mixed effects model with the three-way interaction term “time x discrimination x sexual orientation” was tested and then separate analyses were conducted for the LGB and the matched heterosexual groups, using the PROC MIXED procedure in SAS.
To test the hypotheses for aim 2, the potential moderating effects of problem-focused coping and avoidance coping were examined by adding the interaction terms (time x discrimination x problem-focused/avoidance coping) were added to the separate models for the LGB and heterosexual groups, controlling for covariates. If the interaction term had a p-value of less than .10, additional analyses were conducted to examine the nature of the moderating effect. Specifically, the continuous moderators were stratified above the median (categorized as high) and at or below the median (categorized as low) (problem-focused coping median = 26 and avoidance coping median = 12) to graph the moderated associations between discrimination and the health outcomes. Median splits are a common method of dichotomizing continuous variables to facilitate analytic ease and clarity of interpretation (Iacobucci et al., 2015).
Results
Sample Characteristics
Characteristics of LGB and Propensity-Matched Heterosexual Participants at Wave 1 of the Midlife in the United States Study.
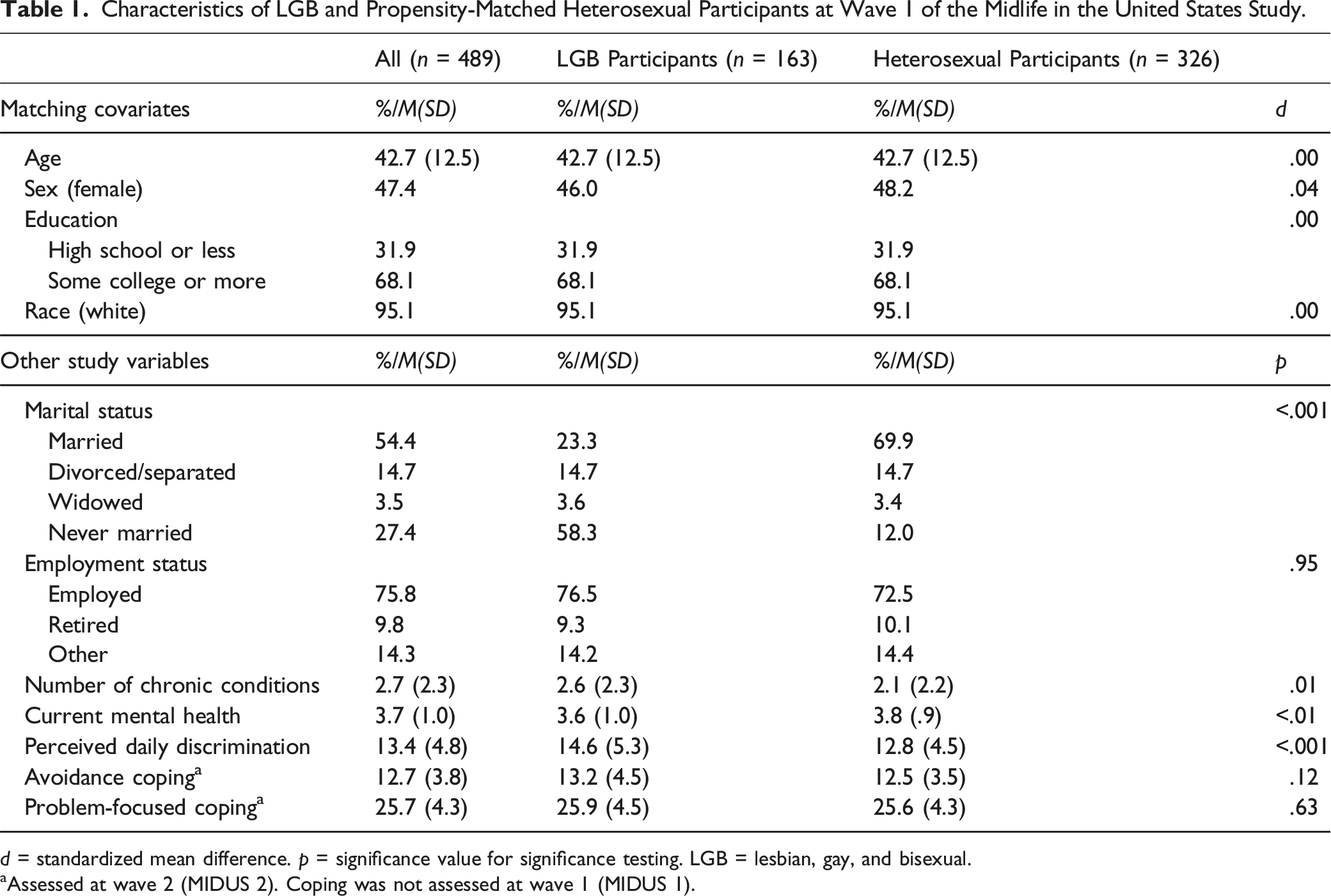
d = standardized mean difference. p = significance value for significance testing. LGB = lesbian, gay, and bisexual.
aAssessed at wave 2 (MIDUS 2). Coping was not assessed at wave 1 (MIDUS 1).
The calculated standardized mean differences were less than .1, indicating successful balancing and no significant differences between LGB and heterosexual participants in any of the matching covariates (age, sex, race, and education). The two groups significantly differed in marital status with heterosexual participants being more likely to be married than LGB participants (p < .001, 70% vs. 23%, respectively). LGB and heterosexual participants were not matched on marital status due to laws restricting same-sex marriage until 2015. LGB participants reported significantly more chronic conditions (p = .01), lower mental health (p < .01), and higher discrimination (p < .001) at baseline. There were no significant differences in problem-focused coping or avoidance coping between the two groups.
Discrimination and Number of Chronic Conditions
The negative binomial GEE model with a three-way interaction term “time x discrimination x sexual orientation” (results not reported in table format) indicated a significant moderating influence of sexual orientation on the association between discrimination and the number of chronic conditions over time (IRR = .98, 95% confidence interval (CI) = .96–.99, p = .04). The model indicated a significant increase in the number of chronic conditions over time for heterosexual participants (IRR = 1.11, 95% CI = 1.03–1.20, p = .004). LGB participants had a 34% greater accumulation of chronic conditions over time relative to heterosexual participants (IRR = 1.34, 95% CI = 1.01–1.79, p = .04). Separate analyses for LGB and heterosexual participants were conducted to further examine the nature of the moderating effect of sexual orientation on the association between discrimination and the number of chronic conditions over time.
Results of the Negative Binomial GEE for LGB and Propensity Score Matched Heterosexual MIDUS Participants.
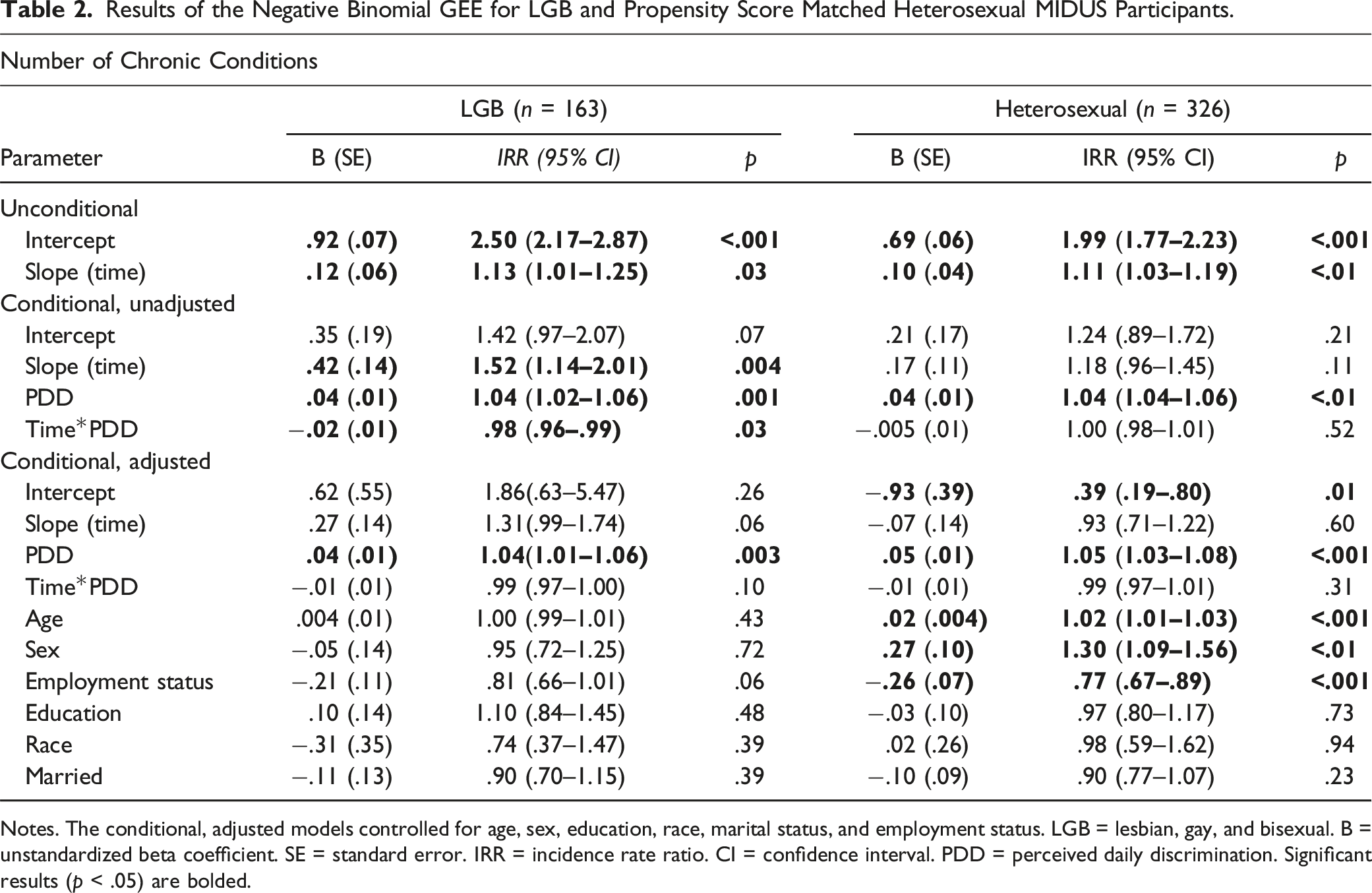
Notes. The conditional, adjusted models controlled for age, sex, education, race, marital status, and employment status. LGB = lesbian, gay, and bisexual. B = unstandardized beta coefficient. SE = standard error. IRR = incidence rate ratio. CI = confidence interval. PDD = perceived daily discrimination. Significant results (p < .05) are bolded.
For the matched heterosexual group, the change in the number of chronic conditions over time (slope) was not significant when perceived discrimination and the “discrimination x time” interaction were added to the model. After controlling for covariates, discrimination was positively associated with the number of chronic conditions at baseline (IRR = 1.05, 95% CI = 1.03–1.08, p < .001). For each unit increase in discrimination, the number of chronic conditions at baseline increased by 5%. Discrimination was not significantly associated with the change in the number of chronic conditions over time.
For heterosexual participants only, age, sex, and employment status were significantly associated with the overall number of chronic conditions. Each additional year of age was associated with a 2% additional increase in the number of chronic conditions (IRR = 1.02, 95% CI = 1.01–1.03, p < .001). Heterosexual females had 1.30 times more chronic conditions overall compared to heterosexual males (IRR = 1.30, 95% CI = 1.09–1.56, p < .01). Being currently employed was associated with 23% less chronic conditions overall relative to not being employed. Figure 2 depicts the covariate-adjusted association between discrimination (dichotomized for clarity and ease of interpretation) and the number of chronic conditions for the LGB and heterosexual groups. Dichotomized perceived daily discrimination and the number of chronic conditions over time for LGB and heterosexual participants. Note. LGB = lesbian, gay, and bisexual. Perceived daily discrimination was categorized into a high and a low group. Scores equal to or below the perceived daily discrimination score were categorized as low perceived daily discrimination. Scores greater than the median were categorized as high perceived daily discrimination. The median for perceived daily discrimination was 14 for the LGB group and 11 for the heterosexual group.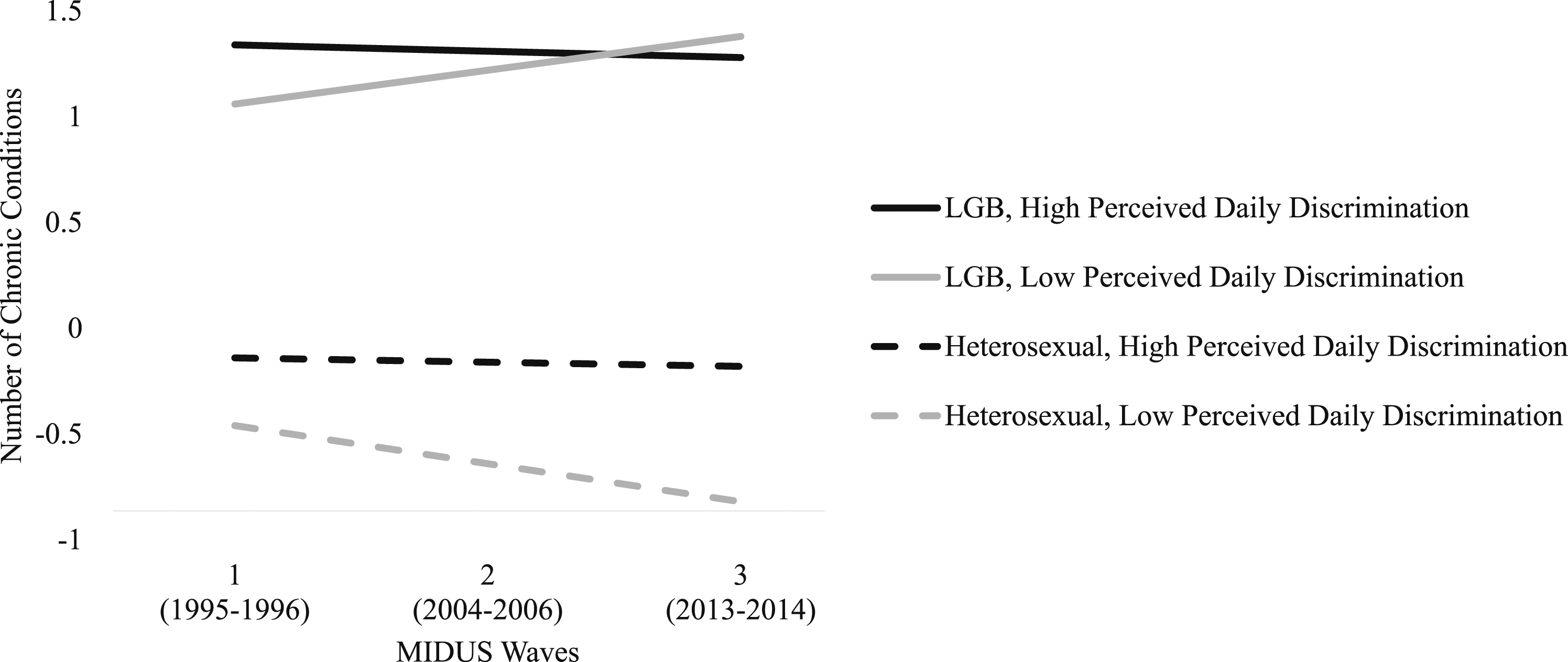
Discrimination and Self-Rated Mental Health
The mixed effects model with a three-way interaction term “time x discrimination x sexual orientation” (results not reported in table format) did not indicate a significant moderating effect of sexual orientation on the association between discrimination and self-rated mental health over time (b = .01, SE = .01, p = .15).
Results of the Mixed Effects Models for LGB and Propensity Score Matched Heterosexual MIDUS Participants.
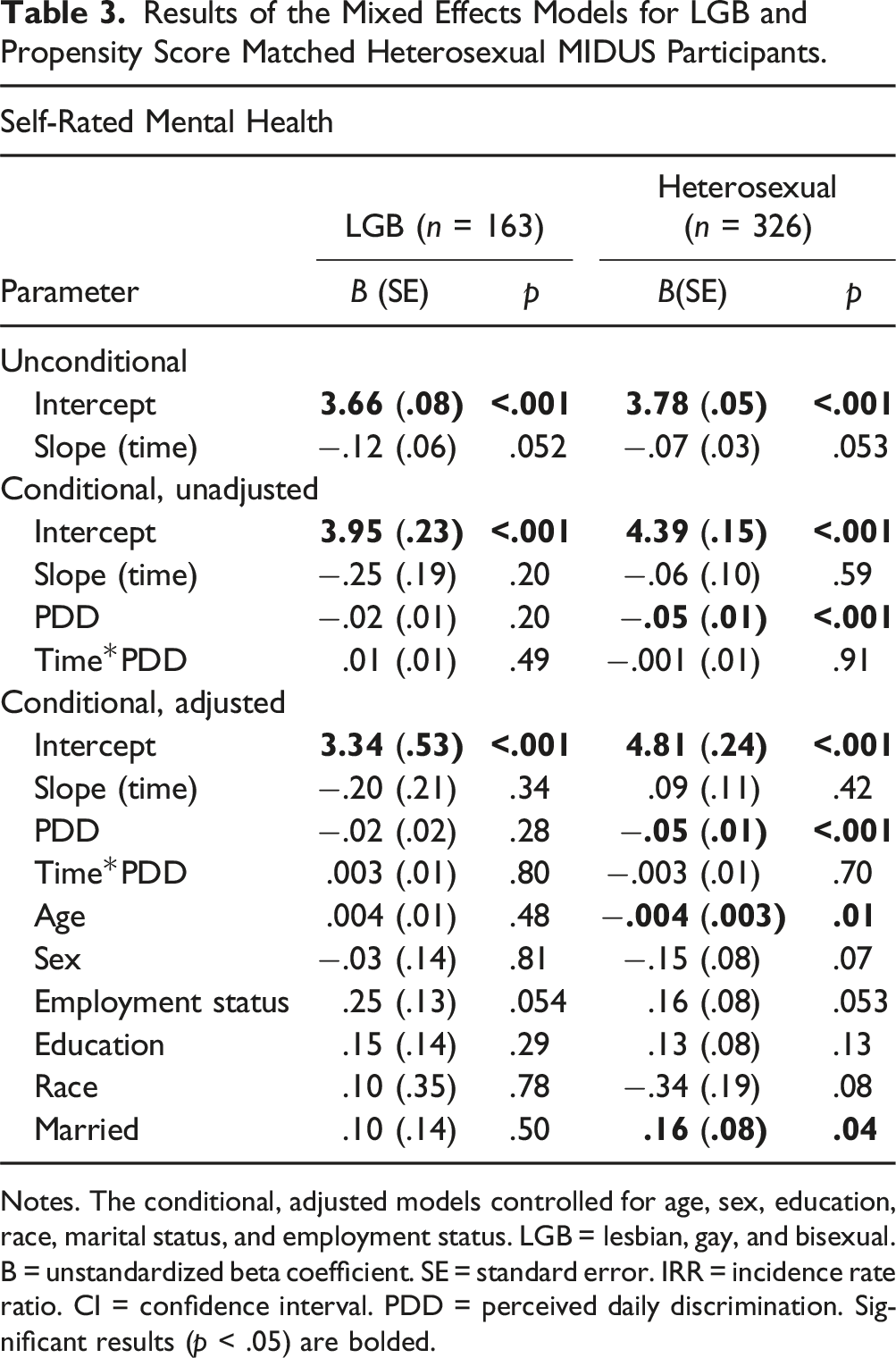
Notes. The conditional, adjusted models controlled for age, sex, education, race, marital status, and employment status. LGB = lesbian, gay, and bisexual. B = unstandardized beta coefficient. SE = standard error. IRR = incidence rate ratio. CI = confidence interval. PDD = perceived daily discrimination. Significant results (p < .05) are bolded.
For the matched heterosexual group, whereas the effect of time was not significant, discrimination was significantly negatively associated with self-rated mental health at baseline, even after controlling for covariates (b = −.05, SE = .01, p < .001). For heterosexual participants, every one unit increase in perceived discrimination was associated with a .05 decrease in self-rated mental health. For heterosexual participants only, increasing age was associated with poorer mental health (b = −.004, SE = .003, p = .04) and being married was associated with better mental health (b = .16, SE = .08, p = .04).
Moderating Effect of Coping on the Associations Between Discrimination and Health
Results of Longitudinal Analyses with Moderator Interaction Terms Added.
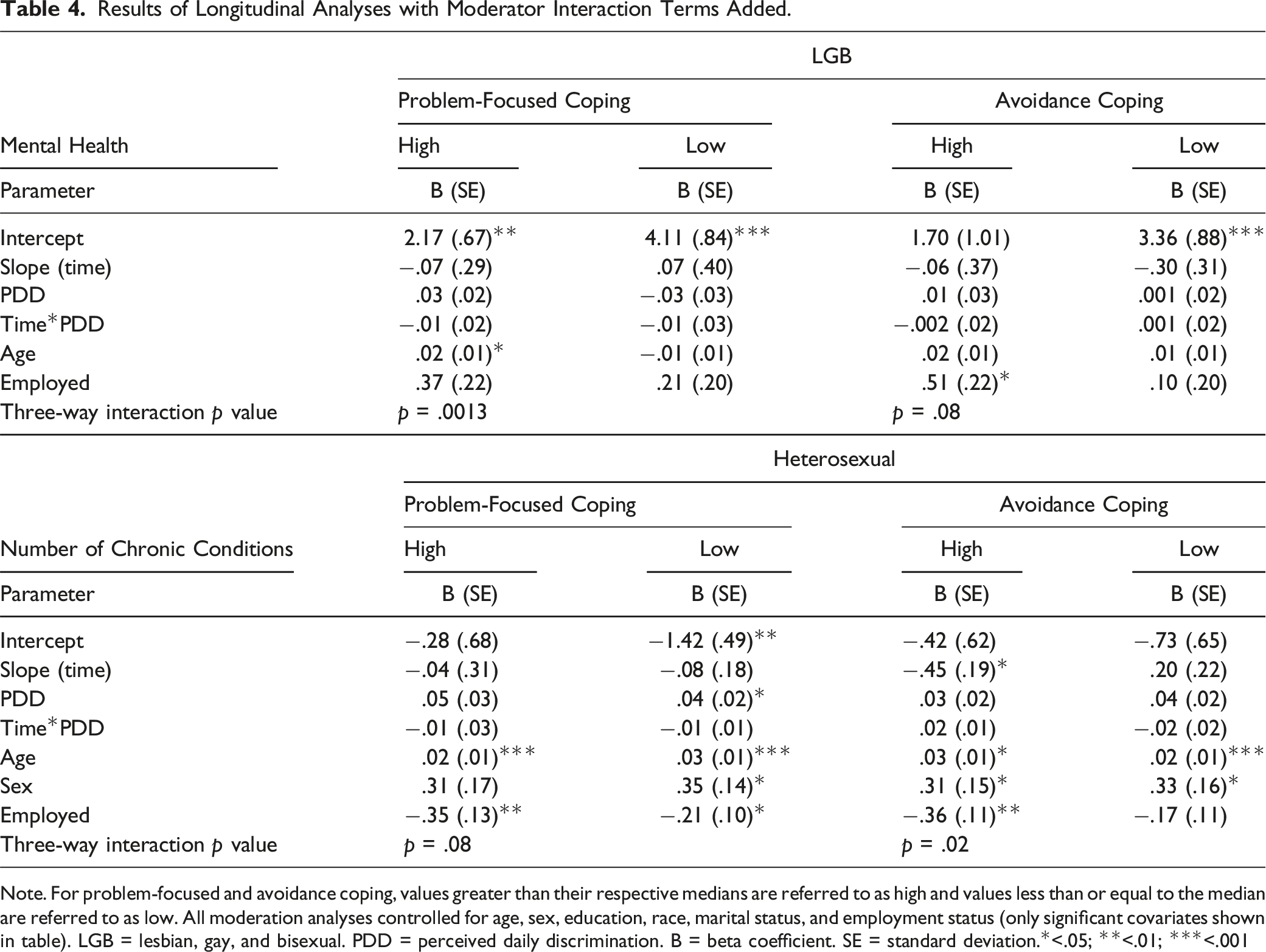
Note. For problem-focused and avoidance coping, values greater than their respective medians are referred to as high and values less than or equal to the median are referred to as low. All moderation analyses controlled for age, sex, education, race, marital status, and employment status (only significant covariates shown in table). LGB = lesbian, gay, and bisexual. PDD = perceived daily discrimination. B = beta coefficient. SE = standard deviation.*<.05; **<.01; ***<.001
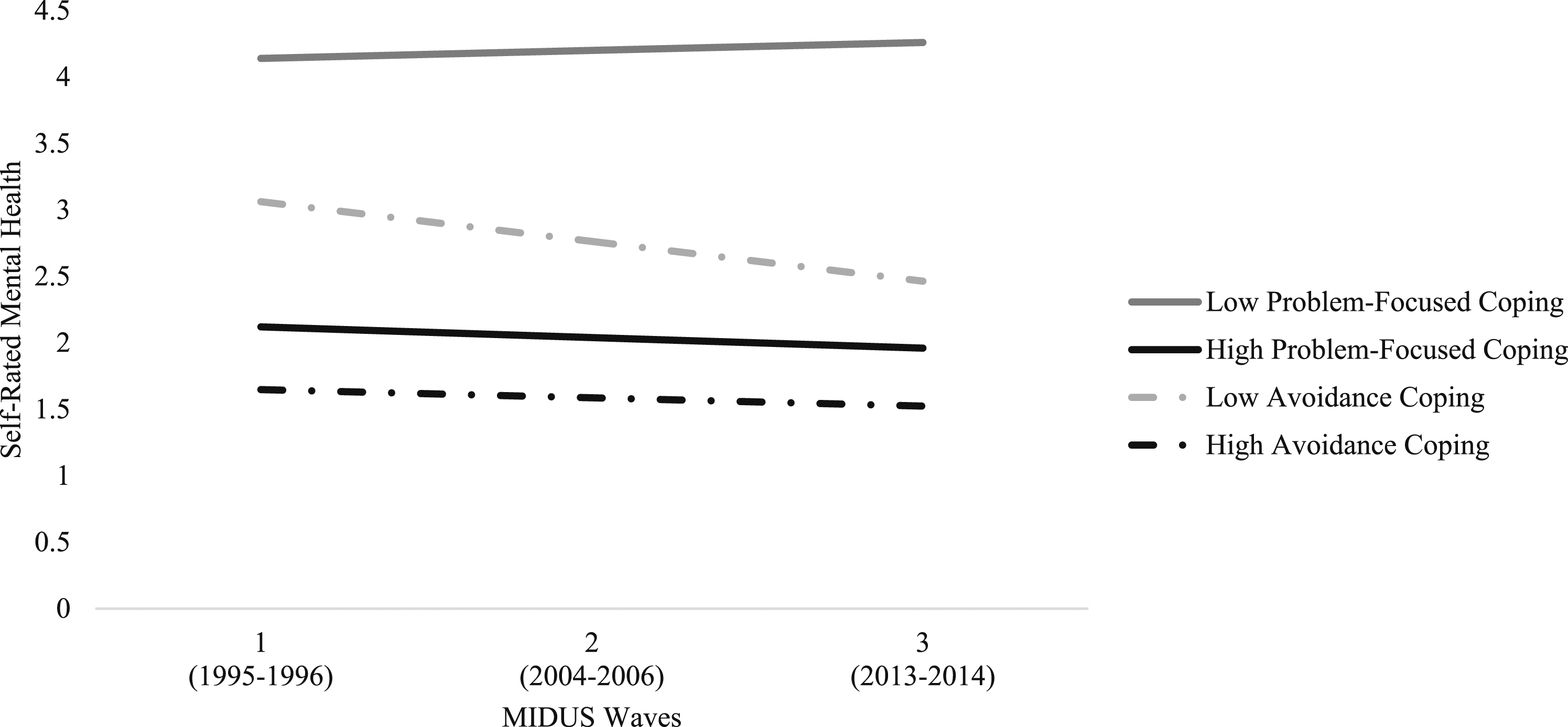
Perceived daily discrimination and self-rated mental health over time for LGB participants, moderated by problem-focused and avoidance coping. Note. LGB = lesbian, gay, and bisexual. Problem-focused coping (median = 26) and avoidance coping (median = 12) were dichotomized above and below their median. Values greater than the median were categorized as high and values less than or equal to the median were categorized as low.
For the matched heterosexual group, problem-focused coping and avoidance coping did not have a significant moderating effect on the association between discrimination and self-rated mental health (p = .71 and .60, respectively). Problem-focused coping had a significant moderating effect on the association between discrimination and the number of chronic conditions (p = .08). Heterosexual participants with low problem-focused coping had less chronic conditions at baseline (b = −1.42, SE = .49) than heterosexual participants with high problem-focused coping (b = −.28, SE = .68) but both groups declined at relatively similar rates over time (b = −.08, SE = .18 and b = −.04, SE = .31, respectively). For heterosexual participants with low problem-focused coping, discrimination was significantly positively associated with the number of chronic conditions at baseline (b = .04, SE = .02, p < .05). Avoidance coping also had a significant moderating effect on the association between discrimination and the number of chronic conditions over time (p = .02). Heterosexual participants with both low avoidance coping experienced an increase in the number of chronic conditions over time (b = .20, SE = .22), but the high avoidance coping group experienced a decrease in the number of chronic conditions (b = −.45, SE = .19). Figure 4 displays the associations between discrimination and the number of chronic conditions over time for heterosexual participants, moderated by problem-focus and avoidance coping. Perceived daily discrimination and the number of chronic conditions over time for heterosexual participants, moderated by problem-focused and avoidance coping. Note. Problem-focused coping (median = 26) and avoidance coping (median = 12) were dichotomized above and below their median. Values greater than the median were categorized as high and values less than or equal to the median were categorized as low.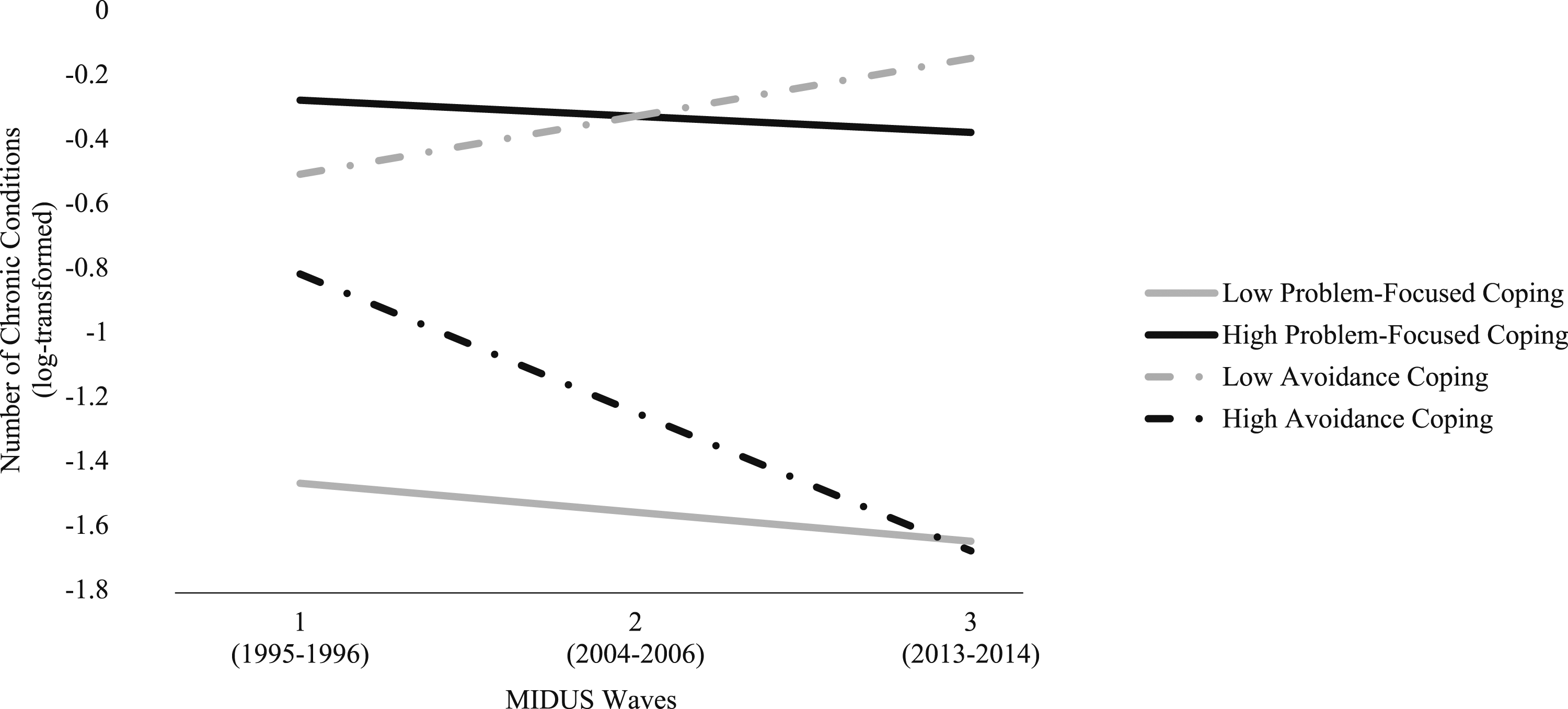
Discussion
The current study aimed to investigate how problem-focused and avoidance coping strategies moderate the associations between discrimination and physical and mental health outcomes over time in LGB and heterosexual midlife and older adults in the United States. The findings revealed distinct trends in health trajectories. Over the study period, LGB participants experienced an increase in the number of chronic conditions and a decrease in self-rated mental health. In contrast, heterosexual participants displayed a decrease in the number of chronic conditions and consistently reported higher levels of mental health. These results align with prior research indicating that LGB older adults face a greater risk of poor physical and mental health compared to their heterosexual counterparts (Fredriksen-Goldsen, 2017b; Jackson et al., 2019; Nelson & Andel, 2020b).
The study’s first hypothesis, proposing a decline in physical and mental health over time for LGB participants with higher perceived discrimination, was not supported. Surprisingly, the results revealed that although LGB participants initially reported more chronic conditions with higher discrimination, increased perceived discrimination was significantly associated with a decrease in the number of chronic conditions over time, before accounting for covariates.
Figure 2 provided intriguing insights, with LGB participants reporting discrimination levels above the median exhibiting a negative slope in chronic conditions. This suggests a potential “steeling” effect (Rutter, 2006), where repeated exposure to adversity like discrimination may lead to resilience to the harmful effects of similar stressors. High perceived daily discrimination in LGB older adults was associated with higher lifetime discrimination, indicating that those with greater lifetime exposure to discrimination may have developed effective coping strategies to manage the chronic stress associated with discrimination. This aligns with research showing that a higher number of early-life stressors can contribute to greater resilience in later life (Harris et al., 2016).
Understanding the impact of discrimination on the health of LGB older adults requires considering historical and social contexts. Fredriksen-Goldsen (2016) categorized LGB older adults into three generations: the Invisible Generation, the Silenced Generation, and the Pride Generation. These generational categories reflect distinct experiences shaped by historical events and cohort effects. For instance, the Invisible Generation (15% of this study’s sample), born in 1934 or earlier, matured during a time when sexual orientation was not openly discussed, likely due to the hardships of the Great Depression and World War II. The Silent Generation (22% of the sample), born between 1935 and 1949, faced a period when homosexual conduct was illegal and considered a severe mental disorder (Foglia & Fredriksen-Goldsen, 2014; Fredriksen-Goldsen, 2016). Approximately half of the participants belonged to the Pride Generation (born 1950–1964), who matured during the rise of the gay rights movement. An additional 16% were part of Generation X (born 1965 to 1972), who came of age during the height of the AIDS/HIV epidemic in the 1980s/1990s. These generational categories underscore the varying degrees of exposure to discrimination across their lifespans. Compared to their heterosexual counterparts, LGB older adults may have accumulated more experiences with discrimination throughout their lives, potentially contributing to their resilience to its adverse effects.
Hypothesis 2a, predicting that problem-focused coping would moderate discrimination’s impact on health outcomes for heterosexual participants, was partially supported. Problem-focused coping moderated the association between discrimination and the number of chronic conditions but not its association with mental health. Interestingly, heterosexual participants using more problem-focused coping had more chronic conditions over time compared to those reporting lower use of this coping strategy. However, employing problem-focused coping, rather than avoidance coping, was associated with fewer chronic conditions and a decline in the number of chronic conditions over time. These findings are consistent with prior research suggesting that greater reliance on problem-focused coping is associated with better health compared to using avoidance coping strategies (e.g., Kidd & Carroll, 2007; Moos et al., 1990; Roesch et al., 2005).
Unexpectedly, problem-focused coping also influenced the self-rated mental health of LGB participants. Those reporting higher use of problem-focused coping strategies had consistently reported lower mental health across the three study waves, while those with problem-focused coping scores below the median experienced a slight improvement in mental health over time. This unexpected result may be attributed to the nature of the stressor. When the stressor is perceived as uncontrollable and chronic, high use of problem-focused coping strategies may increase stress and potentially harm mental health (Folkman & Moskowitz, 2004; Ngamake et al., 2016).
Hypothesis 2b, predicting that higher utilization of avoidance coping would exacerbate the adverse effects of discrimination on health outcomes, was partially supported. LGB participants using more avoidance coping reported lower mental health across all three time points, consistent with previous research on LGB samples (Choi et al., 2016; Kaysen et al., 2014; Zheng et al., 2020). Surprisingly, higher utilization of avoidance coping was associated with improved physical health over time among heterosexual participants, even after controlling for covariates. This finding diverges from prior studies which typically link avoidance coping to poorer physical health compared to problem-focused coping (e.g., Kidd & Carroll, 2007; Moos et al., 1990; Roesch et al., 2005). It suggests that avoidance coping may have a distinct impact on heterosexual older adults experiencing discrimination, possibly due to specific factors related to uncontrollable or short-term stressors (Roth & Cohen, 1986; Suls & Fletcher, 1985).
Strengths and Limitations
This study possesses several noteworthy strengths. Firstly, its longitudinal design allows for an investigation of how discrimination affects the physical and mental health of LGB midlife and older adults over time. Secondly, the study adds robustness through its comparative analysis, incorporating a propensity-score matched heterosexual comparison group. This approach enhances the rigor of the research by facilitating a comprehensive examination of health disparities based on sexual orientation. Thirdly, the study delves into the intricacies of coping mechanisms, which is a relatively underexplored area in the context of discrimination and LGB health. By investigating the moderating effects of both avoidance and problem-focused coping, this research expands our understanding of how coping strategies may influence health outcomes for LGB individuals. Lastly, by focusing on strengths and resilience, this study steers away from the deficit-focused approach that often characterizes research in this area. It thus introduces the possibility of a “steeling” effect among LGB older adults exposed to high levels of discrimination.
However, it is essential to acknowledge certain limitations. First, the presence of missing data and attrition over time, which is not uncommon in longitudinal research, may have influenced our ability to detect statistically significant associations between perceived discrimination and changes in health outcomes. This potential limitation is exacerbated by the relatively small sample size at the study’s baseline.
Another limitation pertains to the use of a sexual orientation measure that defines sexual orientations based on reported attraction. This measure may not comprehensively represent one’s identity or affiliation, which introduces complexities that could impact the interpretation of findings related to discrimination and minority stress. Additionally, this study did not assess changes in sexual orientation between waves, which could have affected the composition of the LGB and heterosexual groups. Furthermore, the absence of data on gender identity should be acknowledged, as the study solely operationalized sex in binary terms (male or female), potentially limiting the exploration of the complex dynamics of gender diversity.
Another limitation was the lack of investigation into coping as a mediator of the relationship between perceived discrimination and health outcomes over time. Coping strategies may explain, rather than moderate, the changes in physical and mental health. Moreover, coping data were collected from one time point, preventing an exploration of how changes in coping strategies may have influenced the relationship between discrimination and health over time.
Suggestions for Future Studies
The findings of this study suggest that different coping strategies may have varying effects on physical and mental health based on sexual orientation. They also raise the possibility that excessive engagement (problem-focused coping) and excessive disengagement (avoidance coping) with stressors like discrimination could be harmful. Future research on minority stressors should consider assessing perceived control to better understand the nature of the stressor. Additionally, there are other coping strategies not examined in this study that may influence or help explain differences in the association between discrimination and health outcomes among sexual minorities. For example, research has indicated that having more social resources is a crucial protective factor among LGB individuals (Fredriksen-Goldsen, 2013; Fredriksen-Goldsen, 2017a). Investigating these effective coping strategies among LGB individuals can inform interventions aimed at reducing health disparities. Future research should continue to explore the strengths of LGB individuals rather than focusing solely on deficits. Examining how individuals effectively cope over time while experiencing higher perceived discrimination can provide valuable insights into developing interventions that promote resilience among LGB individuals at greater risk of negative health outcomes.
Intersectional research represents another crucial avenue for future studies examining the health and resilience of LGB adults. Much of the existing research on LGB older adults, including this study, primarily involves white, well-educated participants. People possess multiple social identities that intersect (Bowleg, 2012), and it is important to consider these identities concurrently with sexual orientation. Future research should investigate coping with discrimination among other sexual orientations as well as among gender diverse people. To gain a comprehensive understanding of the populations under study, inclusive and dynamic measures of gender identity and perceived discrimination should be incorporated. This approach will help develop tailored interventions to promote well-being among diverse sexual and gender minorities by addressing the complex interplay between sexual orientation, gender identity, discrimination, and health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.