
Abstract
Introduction
A sense of purpose in life refers to feeling that life has intention and direction. Maintaining purpose can inform the pursuit of values-based goals (Ryff, 1989) and is considered crucial sustenance for adults’ well-being (McKnight & Kashdan, 2009) and life satisfaction (Hill et al., 2018). Maintenance of purpose across late life can also serve multiple protective functions for health, for example by lowering the risk of developing illnesses or experiencing physical health declines. Indeed, as older adults encounter physical, cognitive, and socioemotional challenges, purpose acts as a resource to bolster health outcomes (Boyle et al., 2010; Cohen et al., 2016; Hafez et al., 2018; Kim et al., 2020). At the same time, older adults have been described as at-risk for experiencing a reduction in their sense of purpose as part of a larger constellation of declines in late life, or as a reaction to negative life events. For example, longitudinal studies have consistently described declines in reported sense of purpose as adults transition from mid-to late-life (Hill & Weston, 2019; Pinquart, 2002).
Illness events that occur in older adulthood may serve as catalysts for changes in sense of purpose, but there is limited empirical evidence of changes in purpose after diagnosis of various chronic, life-limiting illnesses in older adulthood (Hill et al., 2021). Existing research on this topic, including intervention development research, has primarily focused on populations of adults diagnosed with cancer (Park et al., 2019) or chronic disabilities (Yeung & Breheny, 2021). The current study leverages data from a national dataset to examine trajectories of purpose in life for older adults diagnosed with cognitive impairment (i.e., including Alzheimer’s Disease and related dementias; henceforth ADRD), as compared to older adults diagnosed with heart disease or with no chronic illness diagnosis. We include older adults diagnosed with heart disease as a comparison group to demonstrate that the impact of a chronic illness diagnosis on purpose may be diagnosis-specific. Like a diagnosis of ADRD, a diagnosis of heart disease is common and often precedes major lifestyle changes. However, we hypothesized that psychological, social, and functional implications of each disease may underlie diverging impacts of diagnosis on purpose. These major chronic illnesses are each associated with differences in available treatments and resources as well as personal and social expectations about living well with each condition, which may differentially influence changes in sense of purpose over time. Previous studies have examined changes in sense of purpose following heart disease diagnosis (Hill et al., 2021), but have not detected notable changes, further substantiating our selection of this comparison group.
In the context of living with ADRD, previous research has predominantly considered the protective effects of sense of purpose on delaying onset of ADRD. Cross-sectional and longitudinal research, for example, demonstrate that a lower sense of purpose is a predictor of risk of dementia onset, even after controlling for various socioeconomic and demographic factors (Kim et al., 2019; Sutin et al., 2022). However, given that millions of Americans are already living with an ADRD diagnosis, it is also crucial to investigate adults’ maintenance of sense of purpose across diagnosis of ADRD, from before to after a diagnosis is made. Sense of purpose mitigates negative consequences of chronic illness, such as ADRD, including by promoting compliance with health guidelines (Musich et al., 2018) and supporting health decision-making. Given evidence that sense of purpose can bolster life satisfaction (Hill et al., 2018), purpose may also lessen declines in life satisfaction that are associated with the development of cognitive impairment (Gotanda et al., 2023; St John & Montgomery, 2010). As such, maintenance of a sense of purpose across the trajectory of chronic illness diagnosis, particularly in the context of a diagnosis of ADRD, may be a critical health- and quality of life-promoting factor.
Receiving an ADRD diagnosis is critical to navigation of living well with disease limitations (Blinka et al., 2023). At the same time, confirmation of ADRD through a formal diagnosis can act as a potent threat to psychological well-being (Snowden et al., 2015). Indeed, receiving an ADRD diagnosis can itself bring about a reappraisal of one’s future or obscure one’s sense of self (Lishman et al., 2016; Robinson et al., 2011), altogether threatening one’s sense of purpose (Wynn et al., 2021). As such, examining the role of purpose as a protective factor to prevent or delay ADRD must be complemented with investigating changes in sense of purpose when ADRD is diagnosed (Robinson et al., 2011). Thus far, only one recent study to our knowledge has examined longitudinal change in purpose during a period of development of cognitive impairment, with results suggesting that purpose indeed declines during this span of time (Sutin et al., 2023).
The Current Study
This study utilized data from the National Health and Aging Trends Study (NHATS) 1 to establish trajectories of self-reported purpose across diagnosis of ADRD, in comparison to diagnosis of another major chronic illness, heart disease, and to no diagnosis of chronic illness using three-year (pre-diagnosis, year of diagnosis, post-diagnosis) timespans. We hypothesized that trajectories would meaningfully differ based on diagnosis type, with ADRD diagnosis participants, but not comparison group (heart disease, no diagnosis) participants, reporting decreasing sense of purpose across the disease trajectory. Our study aims were preregistered prior to data analyses and were: 1) to examine trajectories of change in purpose from before to after receiving an ADRD diagnosis and 2) to examine differences in purpose trajectories across the three diagnosis groups (ADRD, heart disease, and no diagnosis).
Method
Description of Secondary Data Source and Relevant Survey Items
The current study followed a preregistered protocol deposited at the registry of the Open Science Foundation (OSF; https://osf.io/y4kcw). This study drew from a large, national, and publicly available dataset, the National Health and Aging Trends Study (https://www.nhats.org/). NHATS provides valuable insights into the health and well-being of older adults in the United States and has been used to inform policies and programs designed to improve the lives of older adults. Annual assessments of physical, cognitive, social, and environmental data are collected to evaluate longitudinal trajectories with a holistic framework. Data for NHATS is collected by the Johns Hopkins University Bloomberg School of Public Health in conjuncture with research corporations such as Westat and is currently supported by the National Institute on Aging.
At the time of this study, public use data provided by NHATS included annual assessments from 2011 to 2021. The sample is selected from the Medicare enrollment database; older adult Medicare enrollees who do and do not initially live with chronic or serious illnesses are selected using a stratified random sampling procedure to ensure that the sample is nationally representative of the Medicare population. Participants are interviewed annually by trained interviewers who collect information on a wide range of health and social factors. The first wave of data collected for NHATS was via in-person interviews in the summer of 2011.
Grouping Variable: Illness Diagnosis
To create a sample using the larger NHATS dataset, three diagnosis groups were developed (i.e., ADRD diagnosis, heart disease diagnosis, and no diagnosis). Initially, we delineated the age and gender composition of the ADRD group. Subsequently, from a larger pool of NHATS participants, we isolated potential matches for both the heart disease diagnosis group and the no diagnosis groups, stratifying them by gender and then by age to mirror the ADRD group’s demographic profile closely. Random selection was conducted within each stratum to ensure the matched groups resembled the ADRD cohort distribution. NHATS identifies health conditions through self-reported responses (Yes/No/Previously Reported) to items regarding whether a doctor had diagnosed the participant with any of several chronic conditions since their last NHATS interview. Once a condition was reported, participants’ responses to these items were not reassessed in subsequent years. Thus, participants were sorted into diagnosis groups (ADRD diagnosis, heart disease diagnosis, no diagnosis) based on their self-reported receipt of diagnosis during the year in which they were completing the survey.
Similar to other studies (Sutin et al., 2023), we included participants in the ADRD diagnosis group if they endorsed having received a physician diagnosis of any type of dementia, Alzheimer’s disease, or cognitive impairment, and who provided relevant survey responses at least one year before and one year after diagnosis. We included participants in the heart disease diagnosis group if they endorsed having received a diagnosis of heart disease, including acute infarction, as per available options in the NHATS dataset, and who provided relevant survey responses at least one year before and one year after diagnosis. Finally, we included participants in the no diagnosis group if they reported no new or existing chronic, life-limiting diagnosis (i.e., including heart disease, dementia or cognitive impairment, diabetes, lung disease, stroke, and cancer as per options in the NHATS dataset) during the three-year period from which we drew responses. We excluded participants from each group if they reported receiving any other chronic and life-limiting diagnosis during the three-year period or managing other, existing chronic and life-limiting diagnoses during this period. In other words, for example, those diagnosed with ADRD in our final sample only reported a diagnosis of ADRD, and no other chronic, life-limiting illnesses.
Outcome Variable: Sense of Purpose
The outcome variable was self-reported sense of purpose, measured via a single item adapted from the widely used Ryff Scale of Psychological Well-Being (Ryff et al., 1989; my life has meaning and purpose) to which participants responded on a three-point scale (1 = agree a lot, 2 = agree a little, and 3 = agree not at all). Participants responded regarding how they were feeling in the last month. For our data analyses, scores were reverse coded such that higher scores indicated greater feelings of sense of purpose.
Participants
Demographic Characteristics.
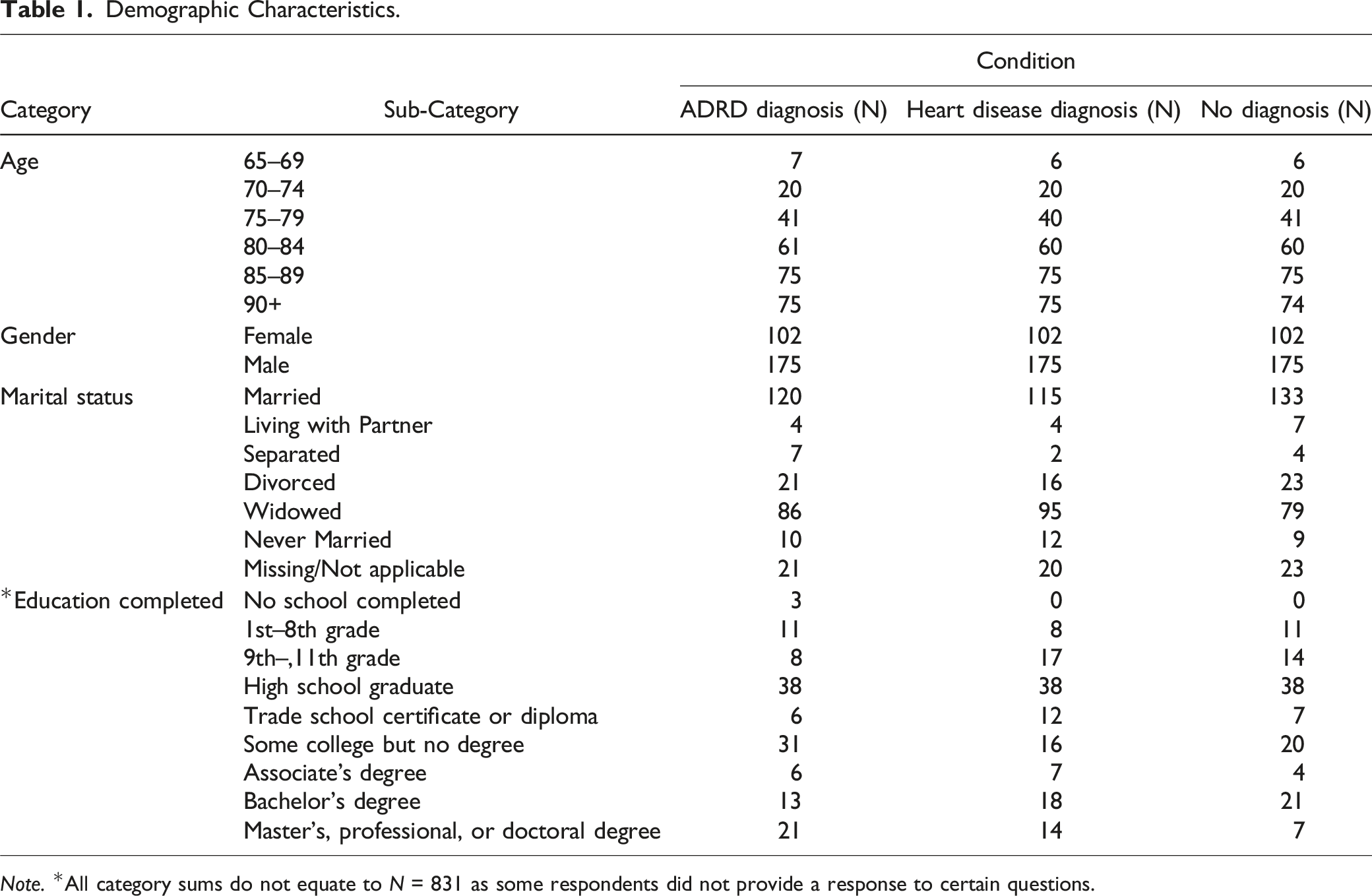
Note. *All category sums do not equate to N = 831 as some respondents did not provide a response to certain questions.
Data Transformation and Plan of Analysis
Before conducting analyses, it was necessary to isolate discrete groups based on illness diagnosis criteria described above, including by excluding those who had experienced more than one illness diagnosis within the three-year period or maintained an ADRD or heart disease diagnosis from prior to the three-year period. Data was first merged across all years into a core dataset by participant identification number using IBM SPSS v.28. Only relevant variables were kept in the final dataset. Similarly, we isolated all analyses for our outcome variable (i.e., sense of purpose) to those indicating that they “agree not at all,” “agree a little,” or “agree a lot.” Guided by our hypotheses, we only included data from participants who had clearly indicated “yes” or “no” to a diagnosis at each time point. A total of n = 1553 sample persons indicated they had received an ADRD diagnoses across all NHATS rounds. Because we were interested in the year directly prior to and directly after a reported diagnosis, we created a new variable across participants to capture their associated responses to the outcome variable (i.e., sense of purpose) at a given time point; that is, we isolated sample participants’ responses to the purpose item for the year before, during, or after a reported diagnoses. A series of “ = IF” statements were deployed using Microsoft Excel to create three variables that captured participants’ feelings of purpose 1) before diagnosis, 2) during the year of diagnosis, and 3) after their diagnosis. Thus, reported sense of purpose for each person included in the final dataset could be compared at these levels. A sample formula is available in our OSF study preregistration file. Last, a variable was created to delineate a participant’s diagnosis group. This transformation took time (e.g., calendar year of diagnosis) out of the equation.
Given the likelihood of violations of certain assumptions due to the nature of this dataset, we first conducted key preliminary checks. Mauchly’s test of sphericity showed that sphericity was violated for the within-subjects factor (W = 0.98, p < .001); as such, subsequent analyses rely on the conservative Greenhouse-Geiseser correction to compensate. Descriptive statistics were then computed for each dependent variable. A three (time: year before, during, or after diagnosis) by three (group: ADRD diagnosis, heart disease diagnosis, or no diagnosis) mixed factorial ANOVA was used to evaluate the trajectory of self-reported sense of purpose between diagnoses. Follow-up pairwise comparisons were conducted using the Holm–Bonferroni method.
We utilized G*power software version 3.1.9.7 to confirm the sample size was appropriate. This was done by considering a range of estimated effect sizes and taking into account certain factors. Firstly, we considered the lack of variability in response options for our dependent variable. In light of this, we chose a small magnitude of effect size (η2 = .01) based on Cohen’s (2016) guidelines. Additionally, we assumed a conservative correlation of r = .35 between the measures and applied a standard nonsphericity correction (ε = 1.0). Furthermore, we set the alpha level (α) at .05 and the beta level (β) at .80 based on best practices in our field. After evaluating these factors, the optimal sample size for our study was estimated at N = 261, suggesting that the current sample size is sufficiently powered to yield meaningful results.
Results
Average Scores of Sense of Purpose Across Diagnosis Groups.
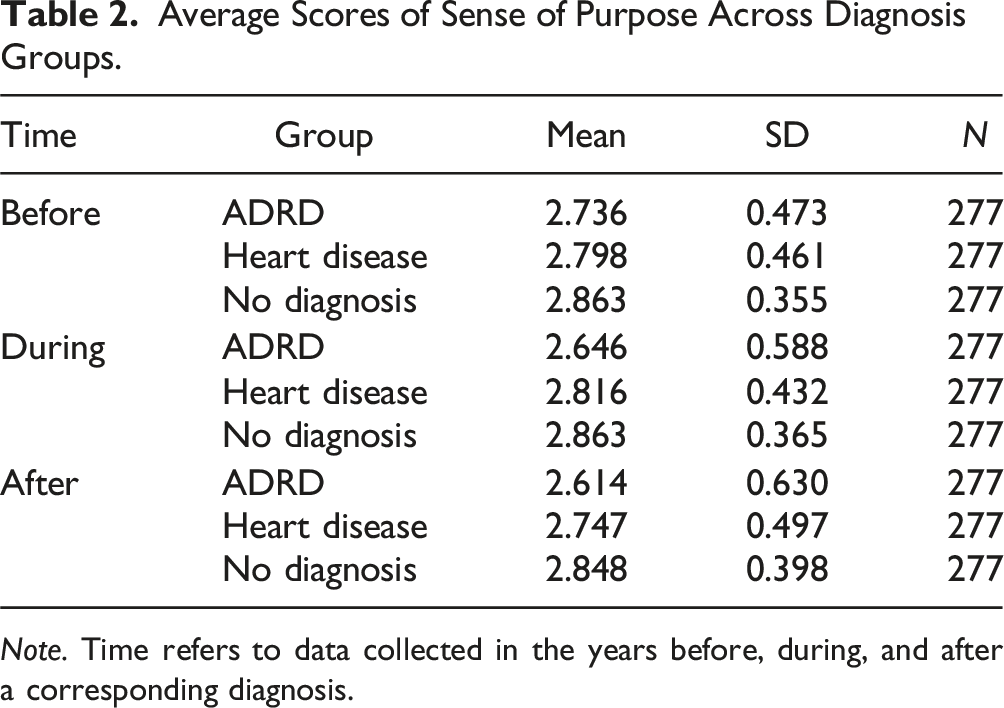
Note. Time refers to data collected in the years before, during, and after a corresponding diagnosis.
The interaction effect between time and group indicated that the effect of time on purpose differed depending on the diagnosis received. Simple main effects analysis showed that only those in the ADRD diagnosis group varied significantly in their purpose over time (F = 5.28, p = .005), with purpose in this group declining from before (M = 2.74) to after diagnosis (M = 2.61), t = 3.85, p = .003, d = −0.258. The simple main effects for both the heart disease (F = .27, p = .07) and no diagnosis (F = .24, p = .79) groups were not significant.
3
A visualization of this is displayed in the descriptive plot in Figure 1. Descriptive Plot of the Interaction between Sense of Purpose and Diagnosis over Time. Note. Error bars are displayed based on a 95% confidence interval.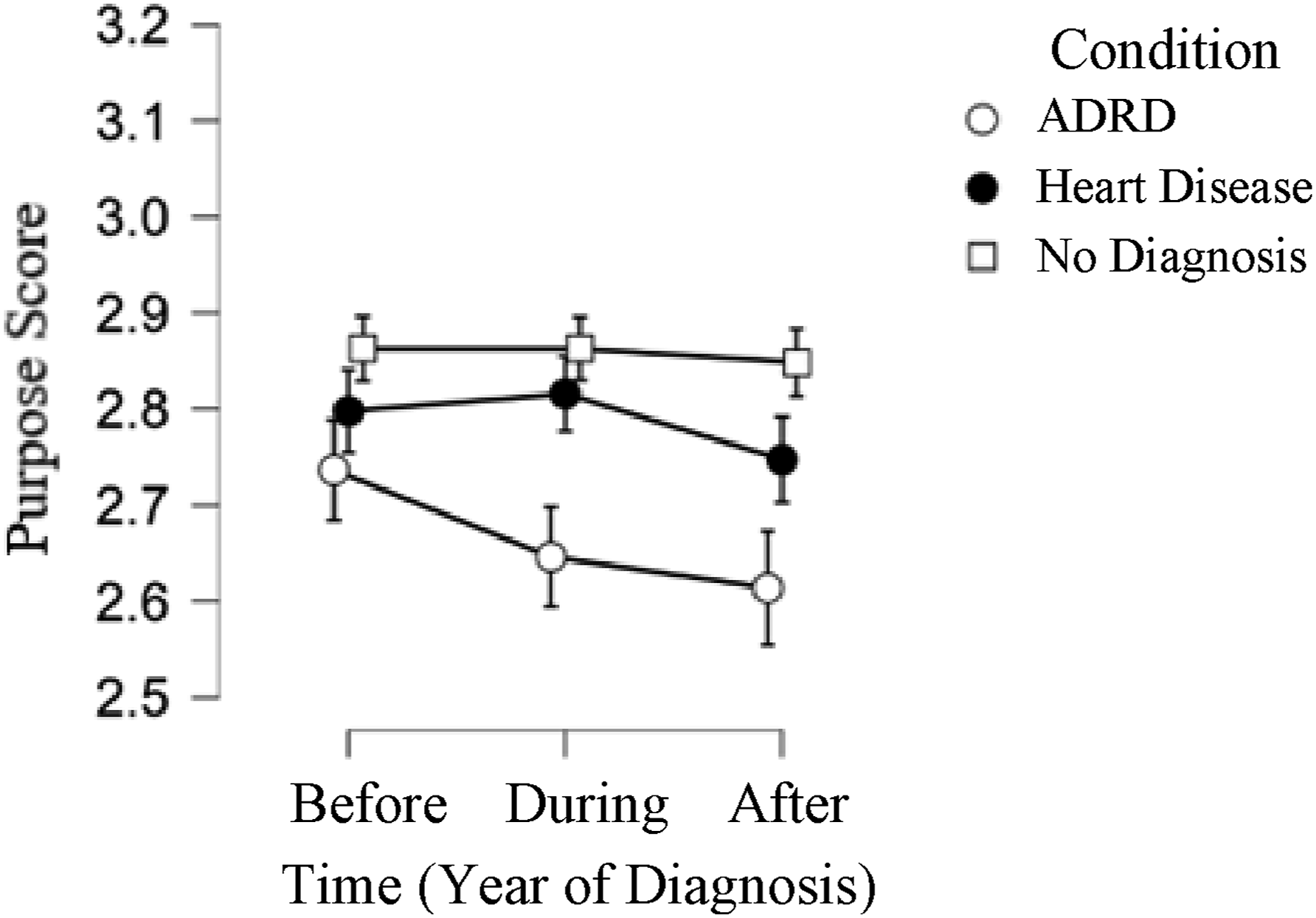
Discussion
This study demonstrates declines in sense of purpose from before to after diagnosis of ADRD in older adulthood across a multi-year period. Our results are consistent with existing observations of decreased sense of purpose from just before, to just after, an ADRD diagnostic appointment (Wynn et al., 2021) and across multi-year health declines associated with ADRD progression (Sutin et al., 2023). The current study sheds light on unique ramifications that an ADRD diagnosis poses for older adults’ sense of purpose. That is, diagnosis of ADRD specifically, and not other common chronic illnesses such as heart disease, may distinctively threaten sense of purpose. We are not suggesting that clinicians withhold diagnoses to spare patients from ramifications; on the contrary, the majority of patients want to understand their diagnoses (Blinka et al., 2023; Robinson et al., 2011), even if the experience is challenging (Yates et al., 2021). Instead, our study underscores the value of clinician communication strategies and other, complementary, post-diagnostic support, to minimize threats to sense of purpose across the ADRD diagnosis trajectory.
Through our comparison with a no chronic illness diagnosis group across a three-year period, we also demonstrated that this decline in sense of purpose is not necessarily due to changes across normal aging. Although previous research suggests that purpose declines over the many year-span of transition from mid-to late-life (Hill & Weston, 2019; Pinquart, 2002), our results indicate that, in older adults with no reported illness diagnosis events, purpose may tend to be stable across shorter longitudinal periods. Our work showcases the need for development of interventions that support care navigation, education for clinicians providing diagnoses, and increased incorporation of non-diagnosing health care teams to bolster purpose for newly-diagnosed persons living with ADRD. Our work also points to future directions for the examination of purpose as a core life construct for persons living with ADRD.
How is Sense of Purpose Impacted by Chronic Illness? Differentiating by Diagnosis
While diagnosis of both heart disease and ADRD may raise some similar types of concerns, broadly, (e.g., around new medications or lifestyle changes, care support needs, and prognosis), the threat posed to one’s sense of purpose in the months post-diagnosis appears to be disease-specific and may be related to differences in diagnosis delivery, available treatments, palliative resources, existential implications, and social stigmas about living well with each type of condition. Although heart disease is the leading cause of death worldwide, adults underestimate the risks associated with heart disease (Mosca et al., 2000), and often maintain optimism about their health after diagnosis, suggesting one pathway by which purpose is maintained following this cluster of diagnoses. In contrast, many persons living with ADRD describe internalized shame, loss of confidence, and limiting beliefs following their diagnosis which may reduce their social engagement or sense of self-worth and can delay critical help-seeking behaviors (Nguyen & Li, 2020). In tandem, declines in sense of purpose across the diagnosis experience may be driven by socially-informed fears of an inability to adapt as symptoms progress, apathy in light of a lack of available treatments, and infantilization or estrangement from individuals in support networks (Cheston et al., 2015; Dröes et al., 2006).
Compared to other chronic, progressive illnesses, there also appears to be a lack of necessary post-diagnostic supports, or limited access to existing supports, to help persons living with ADRD to adapt to new information about their health and functioning in ways that ultimately support their sense of purpose. Following diagnosis of heart disease, for example, patients also anticipate further declines, but care workers place emphasis on prevention and can help to renew patients’ motivation to “take care of their heart,” even in cases where heart disease diagnoses are irreversible and progressive. In contrast, for patients newly diagnosed with ADRD, care workers may place less emphasis brain health and well-being, potentially exacerbating worry about unavoidable further cognitive decline, dependance, and dysfunction. Expectation of the progression of these symptoms is likely to clash with pursuit of purpose-driven goals or purpose maintenance (Hartog et al., 2020). Increased accessibility of supportive resources may not only boost sense of purpose post-diagnosis; such resources may help persons living with ADRD tap into their sense of purpose as a critical guide through disease uncertainty and functional decline.
Beyond Diagnosis: Inter-individual Differences in Purpose Across the ADRD Trajectory
We note that, overall, participants in this study indicated a moderate to strong sense of purpose, regardless of disease diagnosis over time. Although outside the scope of the current study, we speculate that there is variation in reported sense of purpose between older adults within each disease diagnosis context that is driven by additional protective and risk factors. Some factors may be disease diagnosis-specific, while other factors may be non-disease specific and instead mirror known inter-individual differences in older adults with no ADRD diagnoses (e.g., educational attainment and marital status; Hill & Weston, 2019). Future research should characterize the protective and risk factors most relevant to an ADRD diagnosis context to provide guidance for intervention.
As one example, a diagnosis of ADRD is often be accompanied by depression, with previous work demonstrating high comorbidity rates between these two diagnoses (Kunicki et al., 2023). Depressive symptomatology may dysregulate neural systems, leading to abnormalities in executive functions and attention processes (Murrough et al., 2011), holding implications for sense of purpose. In contrast, other work has suggested that low purpose is itself a risk factor for depressive symptoms in individuals with advanced dementia (Sutin et al., 2022), suggesting that depression can be a consequence, rather than antecedent, of decreased purpose in an ADRD disease context. We recognize that depression and loss of purpose are distinct concepts with distinguished clinical implications for older adults (Kaneriya et al., 2023), especially those diagnosed with major chronic conditions. However, we suggest that future research further clarify the direction and magnitude of associations between depression and purpose in the wake of an ADRD diagnosis and across ADRD progression. Establishing causal pathways between these constructs could also help researchers to determine mechanisms of change to target in the development of future interventions.
Similarly, future research should present models of the directions of associations between sense of purpose, life satisfaction, and personality traits, particularly within an ADRD disease context. While studies suggest that personality traits do not predict changes in reported purpose across a multi-year period of older adulthood (Hill & Weston, 2019), other research suggests that changes in personality can manifest following onset of ADRD symptoms (Islam et al., 2019; Terracciano et al., 2023). We speculate that these personality changes could also dictate changes in sense of purpose in the wake of symptom onset or ADRD diagnosis.
Importantly, although our study demonstrates a decline in purpose in the wake of an ADRD diagnosis, individual differences allow many older adults to maintain a sense of purpose even while experiencing considerable ADRD symptoms (Sabat & Harré, 1992; Wynn et al., 2021). In contrast to our assertions that the diagnostic journey itself can pose a psychological threat to sense of purpose for people living with ADRD, recent research proposes that loss of purpose early in the disease course may be due to neurodegeneration (Sutin et al., 2023), perpetuating assumptions that early declines in purpose in this disease context are somewhat inevitable, or at least associated with intensity of cognitive symptoms. In contrast, and given the lack of evidence to support this point, we argue for a strengths-based approach (McGee et al., 2023; Warchol, 2006) to hypothesis generation. This approach spotlights changeable, external factors (e.g., the delivery of an ADRD diagnosis, support offered to individuals in the wake of the diagnosis) rather than unchangeable factors (disease symptomology or pathogenesis) to discover ways that persons living with ADRD can be supported to maintain a sense of purpose across their diagnosis experience. However, no studies have disentangled the extent to which the diagnosis itself, versus symptoms of the disease that often manifest in tandem with a diagnosis, are incremental predictors of changes in reported sense of purpose. This comparison would be a critical next step for research and ultimately inform intervention development.
Links Between Purpose and ADRD in Older Adulthood
The current study and other recent research together point to bidirectional links between sense of purpose and the development of ADRD. On the one hand, sense of purpose is described as a crucial protective factor for cognitive health and delayed ADRD onset (Boyle et al., 2010, 2012; Kim et al., 2019; Lewis et al., 2017; Sutin et al., 2022; Wilson et al., 2022). Strong sense of purpose may even negate some negative impacts of the diagnosis itself, as individuals with a higher sense of purpose show more effective emotional recovery, and lower impulsivity, after negative events (Burrow & Spreng, 2016; Schaefer et al., 2013). In contrast, according to our results, the process of receiving and adopting an ADRD diagnosis may contribute to declines in sense of purpose (Mak et al., 2021). Some researchers, in fact, assert that this association is cyclical (i.e., cognitive declines predict lower purpose, which in turn predicts further cognitive declines; (Wilson et al., 2013).
We speculate though, too, that differences in the directionality of effects may be driven by differences in how ‘sense of purpose’ is being defined and measured (Kashdan et al., 2023). For example, purpose as a conscious, changeable motivator (McKnight & Kashdan, 2009) reflects a range of goals, desires, or definable pathways and may promote self-beliefs and behaviors that protect against cognitive impairment. Persons living with dementia describe “engaging in meaningful activities,” as a core component of what matters most in their lives (Huizenga et al., 2023), suggesting that supporting the pursuit of such activities may benefit purpose post-diagnosis. Purpose, however, also exists as an existential sustenance characterized by the pursuit of one core life passion that transcends smaller goals (Cheston et al., 2015) which may be threatened by losses of self and autonomy that are anticipated in ADRD (Aminzadeh et al., 2007; Brown, 2017; Jetten et al., 2010). Existing research on sense of purpose in chronically ill adults often spans both conceptualizations (Park et al., 2019), further obscuring these constructs. Indeed, the single-item measure embedded in the NHATS dataset refers to both meaning and purpose, limiting differentiation of these constructs in this work. Building off of calls for purpose to be better defined and examined in individuals facing difficult life events (Kashdan et al., 2023; Sharma & Bluck, 2022), we assert that an important future direction is the distinction between dimensions of sense of purpose for persons living with ADRD. This distinction may help sharpen the focus of purpose-based interventions in this illness context.
Limitations
We selected heart disease as a comparison group because of the frequency of heart disease diagnoses in older adults in the US and the existing research demonstrating consistency in reports of purpose in life across this diagnostic experience. There are other chronic illness diagnosis contexts that might be associated with changes in purpose in life, and we encourage readers to review existing literature that addresses these contexts (Park et al., 2019; Yeung & Breheny, 2021). Similarly, isolating participants with no additional chronic, life-limiting conditions to create each study group somewhat compromises real-world application. Future research should explore incrementally potent effects of diagnosis of, or maintenance of, multiple chronic conditions in these disease contexts.
Other main limitations include the single-item measure to assess purpose in this publicly available dataset. Although the single-item measure was derived from a validated and commonly used assessment of purpose (Ryff, 1989) when the NHATS dataset study was designed, the item used in the current study asked participants to consider their sense of purpose and meaning, broadly, using a three-point scale. Changes in sense of purpose over time thus require participants to endorse notable differences in purpose, and more subtle changes in purpose are likely not detectable through this three-point scale. Future primary data collections could build from our findings and measure sense of purpose more robustly.
Conclusion
As the prevalence of ADRD diagnoses has increased over time, interest in bolstering psychological health, including sense of purpose, across the ADRD diagnosis process has grown substantially. This study characterizes a reality that is often discussed among recently diagnosed older adults living with ADRD: diagnosis experiences, and reactions to the diagnosis in the months following, can threaten sense of purpose, resulting in a decline in purpose over time for these individuals. By contrasting these findings to trajectories of sense of purpose following diagnosis of heart disease, we demonstrate that changes in purpose following diagnosis may be disease-specific. Results suggest new considerations for examining dimensions of purpose, imply bidirectional influences between purpose and ADRD diagnosis in older adulthood, and underscore the need for interventions to support sense of purpose in older adults following ADRD diagnosis.
Footnotes
Acknowledgments
The authors would like to thank the people who have enriched this manuscript through sharing their experiences or discussing our findings with us. This includes Rachel Bloom and Dr Sumeer Tah. We would also like to recognize the National Council of Dementia Minds for amplifying the stories of persons living with dementia, inspiring components of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr E. L. Mroz is supported by the National Institute on Aging (NIA) Institutional Training Grant (T32AG019134).
Transparency and Openness Promotion Statement
This study was preregistered at Open Science Framework: https://osf.io/y4kcw. The NHATS dataset is publicly available at https://www.nhats.org/researcher/nhats. The dataset developed from the larger NHATS dataset for this study is also available via Open Science Framework: ![]() with DOI 10.17,605/OSF.IO/FM9GP
with DOI 10.17,605/OSF.IO/FM9GP