
Abstract
Objectives
This study examines whether social engagement at the time of retirement is associated with better cognitive function and slower cognitive decline.
Methods
Data come from 10 waves of the Health and Retirement Study, linked with data from the Consumption and Activities Mail Survey (CAMS). Respondents included those who had transitioned from working full-time to partial or full retirement. Social engagement was measured across 5 social activities and grouped into 4 categories.
Results
In fully adjusted regression models, higher frequency of participation in social activities was associated with higher cognitive function at the time of retirement but not with slower cognitive decline after retirement. An increase in social activities after retirement was not associated with better cognitive function or slower cognitive decline.
Discussion
These findings do not offer evidence that higher frequency of social engagement or increases in social engagement after retirement protect against post-retirement cognitive decline.
Introduction
This paper examines whether a socially engaged lifestyle upon leaving the workforce serves as a buffer against cognitive aging or the decline in cognitive functions in late life. Retirement presents a major transition characterized by a full or partial cessation of work-related activities, providing a window of opportunity for older adults for continued or increased engagement in social activity and other lifestyle changes outside the workplace (Kahana et al., 2013; van Zon et al., 2016; Vigezzi et al., 2021). There is some evidence that higher levels of social engagement in older age are associated with better cognitive function and may provide some protection against late-life cognitive decline (Armstrong et al., 2022; James et al., 2021; Zhou et al., 2020; Krueger et al., 2009). However, the exact role of social engagement in cognitive aging, and especially the potential role of changes in social engagement around the retirement transition, remains poorly understood. Therefore, this paper is aimed at testing the association of social engagement at the time of retirement, and pre- to post-retirement changes in social engagement, with both overall level of cognition and post-retirement cognitive decline.
Retention of cognitive skills and abilities in later life is essential to ensure a high quality of life for aging adults. Although some degree of decline in cognitive functioning is usually expected as part of the aging process, there is significant variability in the rate of decline among older adults. Thus, significant efforts have focused on identifying predictors of age-related cognitive decline. Accordingly, empirical studies have identified key factors associated with varied levels of cognitive aging, such as a person’s level of education, engagement in complex occupations, genetic variations (e.g., APOE ε4), and engagement in physical, social, and cognitive activities (e.g., Cosentino & Stern, 2013; Opdebeeck et al., 2016; Reed et al., 2010; Sando et al., 2008).
Consideration of the beneficial effects of social engagement on late-life cognitive health can be conceptualized as part of more general ecological frameworks of aging and well-being. These frameworks emphasize the importance of the residential neighborhood conditions in shaping the behaviors, health, and well-being of older adults (Chaudhury & Oswald, 2019). Within this context, the concept of “cognability” has recently been proposed to represent the supportive conditions in neighborhood areas that promote cognitive health among its older residents (Finlay et al., 2022). The degree to which neighborhood conditions present opportunities for social engagement and interaction therefore links the neighborhood environment, via participation in various social activities, to better cognitive health in late life. This link is further substantiated by considerable evidence for the beneficial effects of social engagement on overall health and well-being in older adults. For example, studies have shown that people who engage in more social activity report better self-rated health (Morrow-Howell et al., 2014), fewer depressive symptoms and better subjective well-being (Baker et al., 2005; Glass et al., 2006; Luo et al., 2020; Son & Sung, 2023), and fewer functional limitations (Buchman et al., 2009; Janke et al., 2008; Mendes de Leon et al., 2003). Participation in social activities may offer individuals intellectual and emotional stimulation by serving to establish meaningful social roles, self-esteem, and increased social competence (Williams & Kemper, 2010). This stimulation can in turn help maintain cognitive reserve capacity and prevent or slow down age-related cognitive decline (Wang et al., 2002). While there is some evidence that social activity is associated with a reduced risk of cognitive decline and dementia (Armstrong et al., 2022; James et al., 2021; Zhou et al., 2020; Krueger et al., 2009), the extent to which this evidence translates to unique opportunities for intervention, such as during retirement transitions, remains unknown.
Major disruptions or transitions in the life course may result in substantial changes in activity levels, including social activities. Such disruptions or transitions may include residential relocations, divorce or widowhood, or serious illness and hospitalizations. Another major transition during the life course is the shift from full-time working to partial or full retirement. As work activities and responsibilities for many involve at least some degree of engagement in cognitively stimulating activities, cessation of work poses the risk of experiencing a significant reduction in cognitive stimulation (Hultsch et al., 1999; Lee et al., 2019). Although retirement has been linked with various adverse health effects, such as poorer perceived health and lower happiness (Behncke, 2012; Dave et al., 2008; Kim & Moen, 2002), a recent review found results mostly in the opposite direction: better perceived health and fewer depressive symptoms (Garrouste & Perdrix, 2021). There is also some evidence for an association between retirement and cognitive decline although the duration of the retirement-effect on cognition remains less well established (e.g., Alvarez-Bueno et al., 2021; Bonsang et al., 2012; Clouston & Denier, 2017; Coe et al., 2012). At the same time, retirement offers a unique opportunity to increase engagement in other types of activities such as leisure, physical, and social activities (Sabbath et al., 2015; Vigezzi et al., 2021). For our purposes, this raises the question of whether engagement in social activities can compensate for the cessation in work-related cognitively stimulating activities and buffer the effects of this cessation against cognitive aging that occurs in the post-retirement phase of life.
Therefore, the aim of the present study was twofold: we first test the degree to which participation in social activities at the time of retirement is associated with higher cognitive functioning at the time of retirement and reduced cognitive decline after retirement. Next, we test the degree to which increased participation in social activities from before to after retirement is associated with higher cognitive functioning at the time of retirement and reduced cognitive decline after retirement.
Methods
Sample
Data for this study come from the Health and Retirement Study, a nationally representative, biennial longitudinal panel study among older Americans, conducted by the Institute of Social Research at the University of Michigan. We used the RAND HRS data files version 1 prepared by the RAND Center for the Study of Aging with support from Social Security Administration (SSA) and National Institute of Aging (NIA). Beginning in 2001, a random sub-sample of the HRS was selected to complete the Consumption and Activities Mail Survey (CAMS) biennially in the years between core HRS interviews. For this analysis, we used data from waves 4 to 13 (i.e., 1998 through 2016) from the main HRS survey and linked these waves with data from waves 1 to 9 (i.e., 2001 through 2015 of CAMS) from the CAMS survey.
We selected respondents who had a shift in labor force status from working full-time (starting at Wave 4 of the HRS) to either retired or partly retired in the subsequent wave, using the Labor Force Status variable in the HRS. We began with Wave 4 (1998) since those who retired in the subsequent wave (Wave 5 of the HRS 2000) were the first sample eligible for CAMS, allowing us to examine CAMS data for the first wave that a participant retired. This process led to a total of 5392 respondents (3793 who retired and 1599 who partly retired). Of these respondents, we then identified participants who completed the CAMS in the subsequent year (e.g., Wave 5 - 2000 of the HRS was linked with Wave 1 - 2001 of CAMS) to link data on social activity levels (see below) with retirement status as reported in the main HRS survey. Then, in the next step, we excluded individuals reported being younger than 50 years of age (N = 5), who had missing CAMS data (N = 3479), or missing cognition data (N = 41). This resulted in a final analytic sample of 1867 individuals (Figure 1). In addition, we computed the change in social activity from the last wave working full time to the first wave reporting full or partial retirement. For this, respondents had to have non-missing CAMS data during both the last wave working full time and the first wave after retirement, resulting in a sample size of 1108 respondents. Sample exclusion criteria.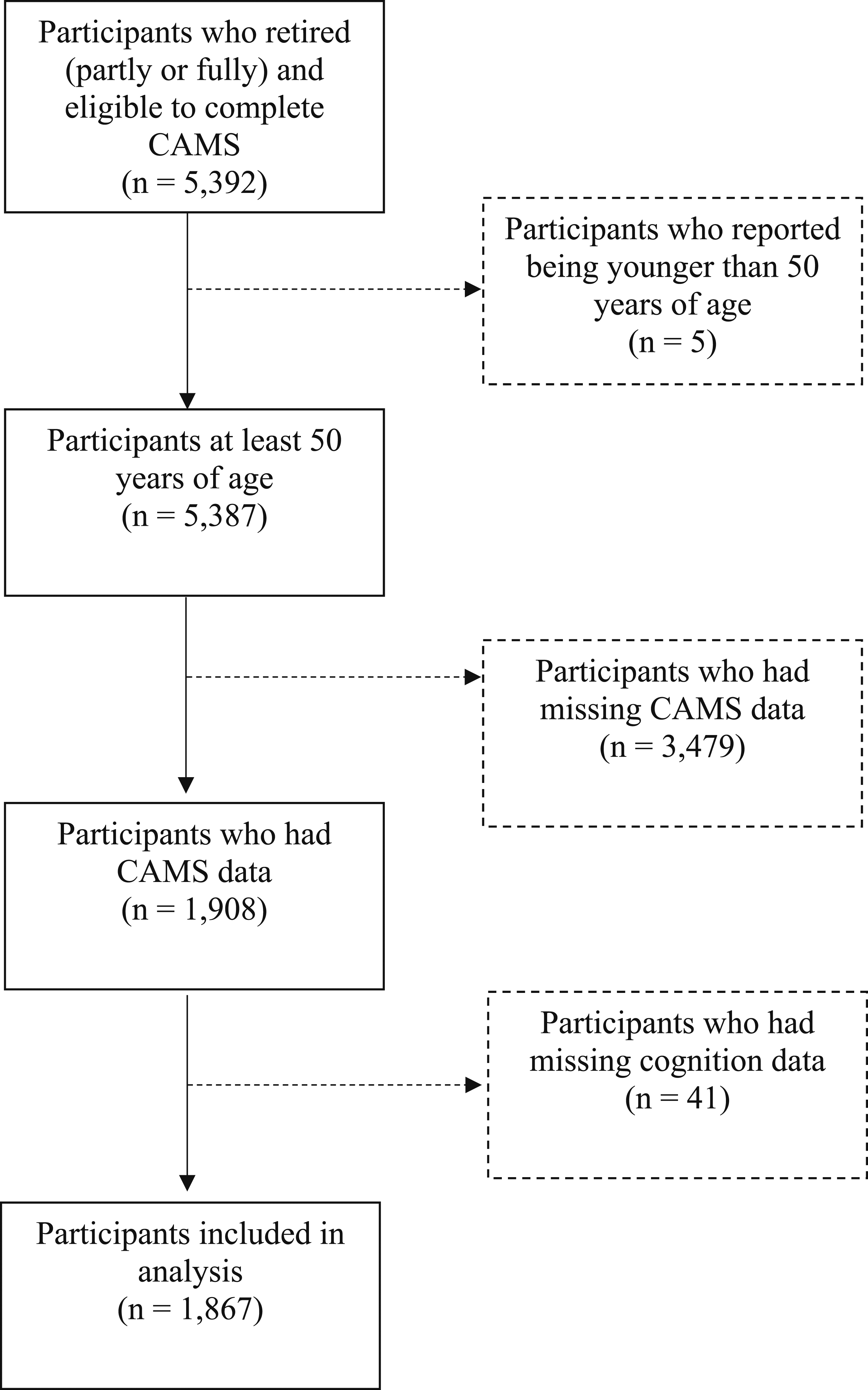
Variables
Retirement Status
Retirement status was derived from the labor force status variable, which is derived from questions included in each HRS survey. Respondents are classified as working full-time, working part-time, unemployed, partly retired, retired, disabled, or not in the labor force.
Social Engagement
The Consumption and Activities Mail Survey (CAMS) asks respondents how much time they spend engaging in a wide array of activities. For the measurement of social engagement, we followed the approach of previous studies (e.g., Armstrong et al., 2022; James et al., 2021; Zhou et al., 2020) and focused on activities that typically involve interactions with other persons: returning to working for pay after full retirement (bridge employment), visiting in-person with friends, neighbors, or relatives, informal caregiving, volunteer work (for religious, educational, health-related, or other charitable organizations), and participating in entertainment activities (attending concerts, movies, lectures, or visiting museums). Activities involving frequent participation (e.g., in-person visits with others) were assessed in terms of hours spent during the previous week, whereas activities involving less frequent participation (e.g., volunteering and attending religious services) were assessed based on hours spent during the previous month. Responses expressed in hours per month were divided by four to compute hours per week of participation. A summary social engagement variable was created by adding the total number of hours per week reported across all five variables. We used two versions of this variable in the analysis: (1) the continuous variable representing the total sum of hours of social engagement per week and (2) using quartiles of the continuous variable to create a categorical variable representing four levels of social engagement: Low, Somewhat Low, Somewhat High, or High Level of Engagement. We also created a change in social engagement variable by subtracting the total sum of hours of social engagement prior to retirement from the total sum of hours of social engagement at retirement, such that positive numbers represent an increase in social engagement. We then used the median split of the total sum of hours of social engagement at retirement to create categories of high and low social engagement before and after retirement, and create the following 4 groups: low-low, low-high, high-low, and high-high.
Cognition
We created a summary cognitive variable by averaging the standardized scores for measures of episodic memory, working memory, and processing speed derived from the Telephone Interview for Cognitive Status (TICS, Brandt et al., 1988). Episodic memory is measured by an immediate and delayed word recall task. The interviewer reads a list of 10 words to the respondent and asks the respondent to recall as many words as possible from the list in any order. The respondent is asked to recall as many words as they can immediately after listening to the words (immediate recall) and after a short interval (delayed recall). The word recall score is calculated as the number of target words recalled at the immediate recall phase and at the delayed recall phase. Thus, scores range from 0 to 20 for the total word recall index. Working memory is measured through a Serial 7s test. This test asks the individual to subtract 7 from the prior number, beginning with 100, for five trials. Correct subtractions are based on the prior number given, so that even if one subtraction is incorrect subsequent trials are evaluated on the given (perhaps wrong) answer. Valid scores are 0–5. Processing speed is measured through a backward counting task. Respondents are asked to count backwards for 10 continuous numbers from 20. Respondents receive two points if they are successful on the first attempt, one if successful on the second, and zero if not successful on either attempt.
Control Variables
Drawing from the literature (see, e.g., Guo & Song, 2023; Khalaila et al., 2024; Rajan et al., 2015; Weuve et al., 2018), we included several control variables that are known to be associated with cognitive aging in older adult populations. These include the sociodemographic variables of age (years), gender (0 = male, 1 = female), self-identified race irrespective of ethnicity (0 = White, 1 = Black/African American, 2 = neither white nor black, referred to as other), and ethnicity (Hispanic/Latino). We further included variables for education (years of education completed), household wealth (total wealth after subtracting debt from assets, log-transformed to account for the highly skewed distribution), and Census region (Northeast, Midwest, South, and West/Other). Finally, we used a measure of depressive symptoms as a marker of mental health status (the 8-item version of the Center for Epidemiologic Studies Depression Scale; CESD, Radloff, 1977) and variable of physical health status based on the number of the physician-diagnosed 8 chronic medical conditions: high blood pressure, diabetes, cancer, lung disease, heart disease, stroke, psychiatric problems, and arthritis.
Statistical Analysis
We used mixed-effects regression models to test the association of social engagement at the time of retirement, and pre- to post-retirement changes in social engagement, with level of cognitive function at baseline and change in cognitive function after controlling for sociodemographic and health factors. We used 3 sets of models to test these associations. In the first model, we adjusted for the basic control variables, including age, age-squared (to account for the curvilinear association between age and cognitive function), time since retirement (number of survey waves since retirement and the interaction between age and time since retirement) sex, race, and ethnicity. In the second model we added years of education, household wealth, and Census region as additional control variables, and in the third model variables for depressive symptoms and number of medical conditions were added. We fitted the same set of 3 sequential models for the analysis of pre- to post-retirement change in social engagement and level of cognitive function and change in cognitive function. All results were based on a weighted analysis, which considered the sampling weight for each wave. The analyses were conducted using SAS software (Version 9.4).
Results
Sample Characteristics
Demographic Characteristics at the First Wave After Retirement (N = 1867).
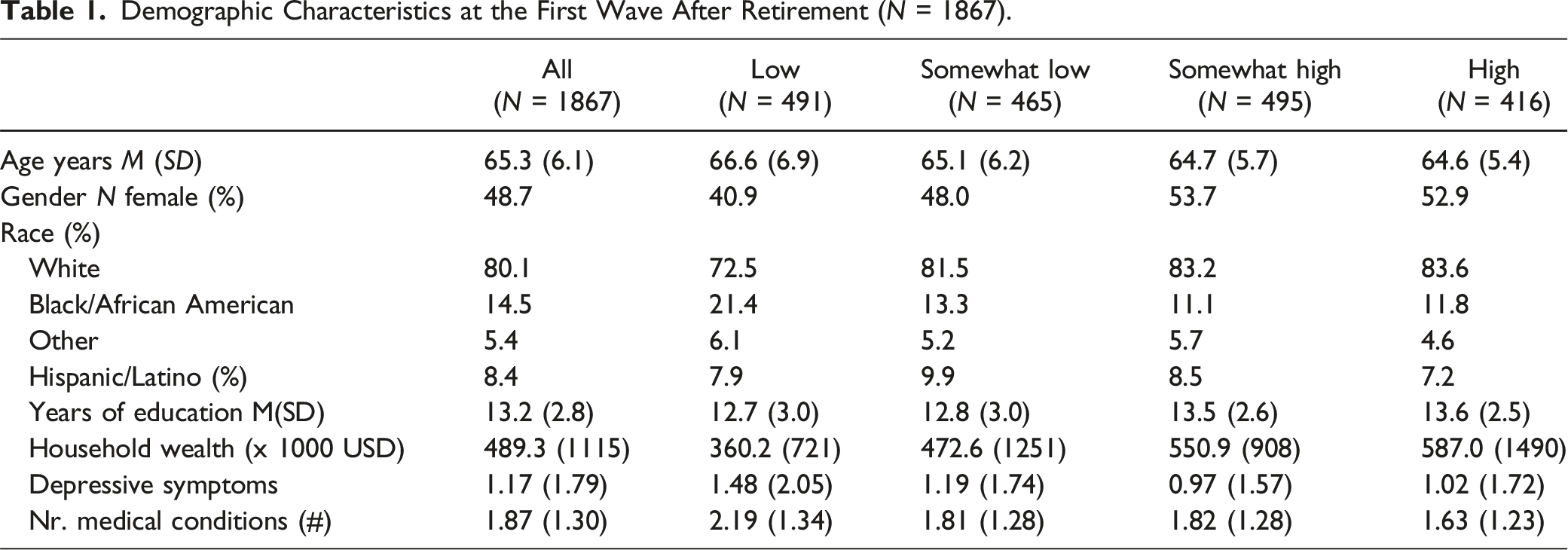
The descriptive data by the 4 social engagement groups show that younger, female, and White respondents tended to have higher levels of social engagement (Table 1). Higher levels of social engagement were also more common among those with more education and wealth, and fewer depressive symptoms and medical conditions.
Social Engagement Groups
Number of Hours/Week of Each Type of Social Activity by Level of Social Engagement.
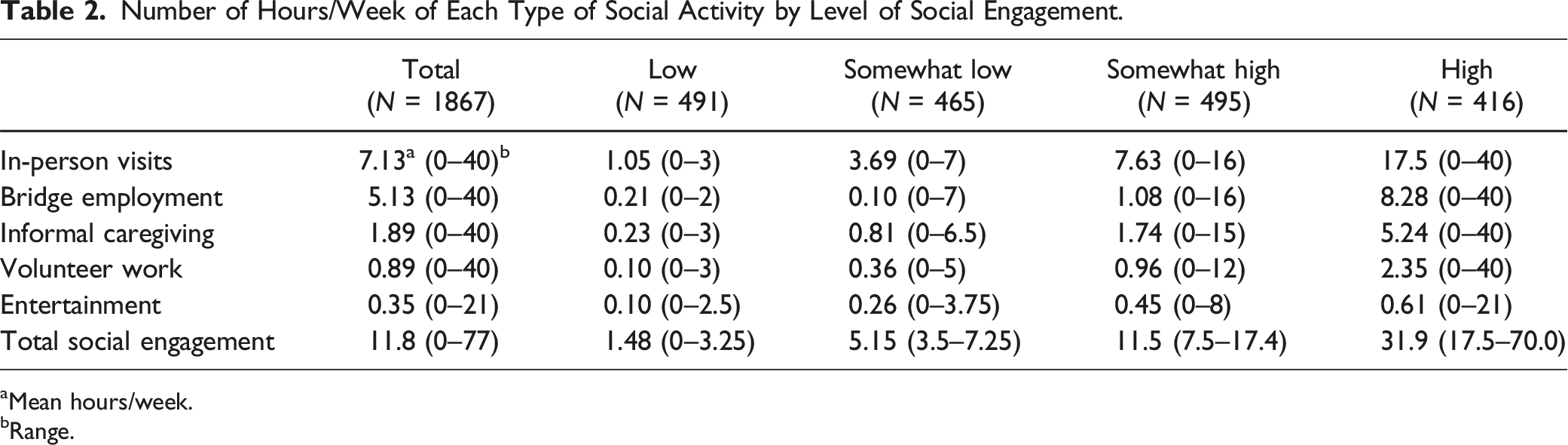
aMean hours/week.
bRange.
Social Engagement and Cognitive Function
Social engagement had a significant positive correlation (r = .10, p < .001) with cognitive function at the last wave prior to retirement. However, this correlation was considerably smaller and no longer significant at the first wave post-retirement (r = .04, p = .12).
Social Engagement at Retirement and Cognitive Function (N = 1867).
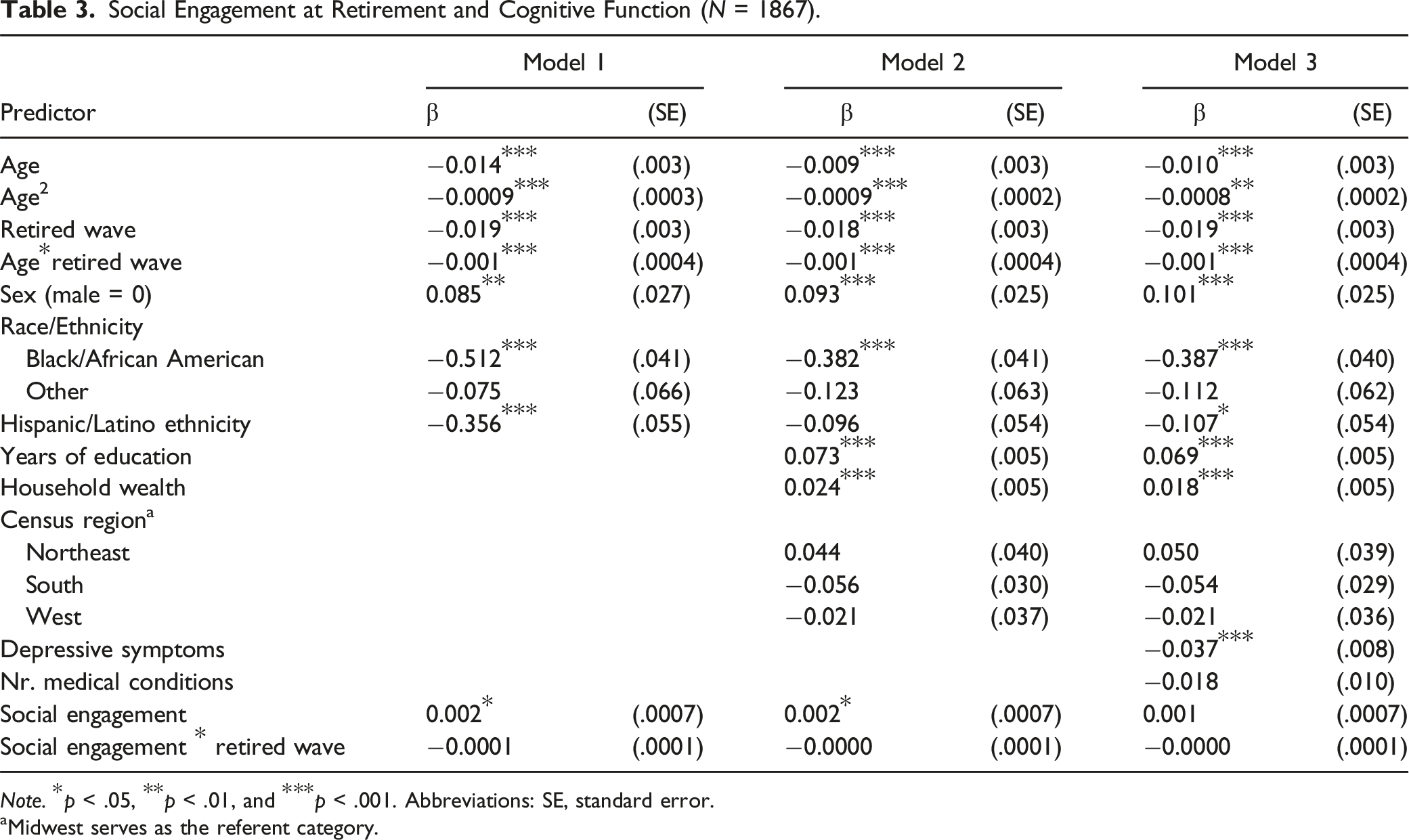
Note. *p < .05, **p < .01, and ***p < .001. Abbreviations: SE, standard error.
aMidwest serves as the referent category.
Other variables in the model revealed that cognitive function tended to decrease with increasing age in a curvilinear fashion. Cognitive function also tended to decline over time (since retirement) and tended to be higher among females and lower among Black/African Americans, people in other race groups, and those identifying as Hispanic/Latino. Education and wealth both showed a highly significant positive association with cognitive function, while Census region was not significantly associated with cognitive function. Depressive symptoms were negatively associated with cognitive function, while the number of medical conditions was not significantly associated with cognitive function (p = .06).
Using the four-level categorical social engagement variable yielded essentially the same results (data not shown). In the first model, the somewhat-low (β = 0.09, p = .04), somewhat-high (β = 0.15, p = .0002), and high level of engagement groups (β = 0.18, p < .001) were significantly associated with better cognitive function at baseline relative to the low-low social engagement group. These associations remained statistically significant with further adjustments in models 2 and 3, with exception of the somewhat-low social engagement in the third model which was no longer significantly associated with cognitive function at baseline. None of the social engagement groups showed a significant association with change in cognitive function over time (ps > .05).
We next tested whether pre- to post-retirement change in social engagement was associated with cognitive function after retirement. In the first model using the continuous variable for change in social engagement, we found no evidence for an association between this variable and either cognitive function at the time of retirement (baseline) or with change in cognitive function following retirement (all ps > .05, data not shown). Adjustment for additional control variables in models 2 and 3 yielded the same results. The same pattern of findings was also evident when we used a categorical variable for pre- to post-retirement change in social engagement (low-low, low-high, high-low, and high-high), instead of the continuous variable. There was one exception: in model 1, the high-high group (high in social engagement before and after retirement) had significantly better cognitive function at the time of retirement relative to the low-low group (β = 0.15, p < .01). This baseline difference between the high-high and low-low group was somewhat attenuated but remained statistically significant after further adjustment in models 2 and 3 (p < .05).
Discussion
This study examined whether participation in socially engaging activities at the time of retirement could serve as a protective factor for cognitive decline. To this effect, we tested the association between level of social engagement during the first wave of retirement and change in pre- to post-retirement change in social engagement with cognitive function and cognitive decline over time in a sample of retired older adults in the Health and Retirement Study who completed the Consumption and Activities Mail Survey (CAMS). The results from the present study revealed that while higher levels of social engagement were associated with better cognitive function, they were not associated with cognitive decline. In addition, when examining changes in social engagement pre- to post-retirement, the results showed that only those who remained highly engaged pre- to post-retirement had higher levels of cognitive function than those who had low levels of engagement before as well as after retirement. Pre- to post-retirement changes in social engagement were not associated with cognitive decline.
Previous research has documented the benefits of engaging in social activities for numerous aging-relevant outcomes, such as functional limitations (Buchman et al., 2009; Janke et al., 2008; Mendes de Leon et al., 2003) and mortality (Lamar et al., 2022; Thomas, 2012), as well as cognitive decline (e.g., Armstrong et al., 2022; James et al., 2021; Zhou et al., 2020; Krueger et al., 2009). Our objective was to specifically examine whether social engagement around the time of retirement would be associated with less cognitive decline in the years following retirement, based on the premise that social engagement might compensate for the cessation in work-related cognitively stimulating activities after retirement and their potentially protective effect on cognitive decline. In other words, does the retirement transition offer a unique window of opportunity to help retirees find other types of activities in their daily life that help them to ward off or delay the age-associated decline in cognitive function? Our findings, regrettably, do not provide any evidence for the merits of this hypothesis.
Our findings are inconsistent with those from previous studies which provide considerable evidence for an association between social engagement and slower cognitive decline over time (e.g., Armstrong et al., 2022; James et al., 2021; Krueger et al., 2009; Zhoue et al., 2020). While they indicate that recently retired older adults with higher levels of social engagement also tend to have better cognitive function, we can think of no obvious reasons why we failed to identify a longitudinal protective effect against declines in cognitive function, like studies of more general populations of older adults have clearly suggested. Selection bias is a possibility, due to the fact that on average, the respondents in our sample worked full time until a relatively advanced age, on average close to the official retirement age. The ability to extend work-life may have depended on other resources providing long-term protection against cognitive decline, for example, relatively good health, leaving less room for social activities to make an impact on slowing down cognitive decline after retirement. However, our data indicate that this sample was still quite diverse in many respects, such as educational level and wealth, depressive symptoms, and physical health status.
A second reason may be related to insufficient statistical power to detect a longitudinal effect of social engagement on change in cognitive function (Sommet et al., 2023). However, we note that for both the main social engagement analysis as for the change in social activity analysis, the estimated coefficient for the estimated longitudinal association was negative, and therefore in the opposite direction of a potentially protective effect, and in all instances very close to null. Thus, lack of statistical power may not have been the major reason for not finding a significant longitudinal association in our analyses. There was also substantial heterogeneity in reported participation in different social activities in the sample, reducing the possibility of restricted variance in our key independent variable as a possible explanation. In addition, our measure of social engagement followed an approach that is typical in this literature, assessing the same types of activities that are typically included in these measures, even if these measures may not capture the full spectrum of social activities in which older adults engage on a daily or weekly basis. In fact, our measure was if anything more detailed, in the sense that respondents were not asked a crude (yes, no) or generic question of frequency (e.g., ranging from never to often) of participation, but specifically asked the number of hours per week or month spent on each activity. Finally, assessments of social engagement as in CAMS are merely snapshots taken at a particular point-of-time, which may not represent engagement levels across longer periods of time for each person. However, that same limitation applies to most other studies of the relationship as well, and therefore may not explain the discrepancy between our findings and those from previous studies.
In spite of these limitations, which arguably may be insufficient to account for our null findings, our study also possessed several notable strengths. First, these data come from a large nationally representative cohort of older adults from across the United States. Second, it included longitudinal data to model changes in cognitive function with sufficient precision, although admittedly, the average of 5.5 years of follow-up may not have been long enough to capture the long-term aging effects on cognition. Third, we used a composite measure of cognitive function that assesses a range of cognitive abilities (episodic memory, working memory, and processing speed) rather than restricting to one measure, which decreases measurement error. Finally, in conducting our analyses, we controlled for several important factors that might have influenced the association between level of social engagement and cognition, including education, household wealth, depressive symptoms, and medical conditions.
In conclusion, our findings suggest that social engagement at the time of retirement and increases in social engagement immediately following the retirement transition are not associated with a protective effect against aging-related cognitive decline. While there is considerable evidence for such a protective effect in the general population of older adults, we were not able to replicate this association for the specific situation of a retirement transition. Given that the degree to which older adults are socially engaged is in theory modifiable, and therefore subject to intervention, this topic may well benefit from further exploration expanding the time frame of social engagement assessments around the retirement transition and longer follow-up of post-retirement trajectories of cognitive change.
Footnotes
Acknowledgments
The HRS (Health and Retirement Study) is sponsored by the National Institute on Aging (grant number NIA U01AG009740) and is conducted by the University of Michigan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging (grant number: NIA U01AG009740).