
Abstract
Background
This study examined whether patterns of relationship quality between parents and adult children were associated with the onset of ADL disability in later life.
Research Design and Methods
Using data from the Health and Retirement Study (N = 8,101), we studied whether support, strain, and patterns of relationships between parents and adult children were related to age of onset of ADL disability among parents.
Results
Greater support from adult children (based on parental report) was associated with later onset of ADL disability, and greater social strain was associated with earlier onset of disability. Compared to high-quality relationships, adverse, indifferent, and ambivalent relationships were associated with an earlier onset of ADL disability over time.
Discussion
It is important to acknowledge the complexity of relationships between parents and their adult children to understand how patterns of quality within these relationships influence ADL functioning in later life among parents.
Keywords
Individuals’ lives are shaped by the relationships in which they are engaged, and these relationships have been found to be influential for many health outcomes—including physical, psychological, and cognitive. Interest in the impact of social relationships on health has a long history, rooted in early work conducted by Durkheim. In studying suicide, Durkheim ([1897]1979) argued that those lacking social ties were less attached to society and more likely to engage in deviant behaviors. Since Durkheim’s work, other scholars have argued that the relationship between social relations and health is more complex. For example, in the 1980s Rook sparked interest in the negative dimension of social interaction, finding that negative social ties had more potent effects on psychological well-being than positive ties (Rook, 1984). This study was critical for the work on social relationships and health as it shifted the literature to acknowledge the “dark side” of social relationships and that social relationships are not “universally protective for later-life well-being; rather, the protective effects of social ties vary based on the structure, nature, and quality of the relationship” (Carr & Moorman, 2011, p. 145).
One particularly prominent relationship among adults involves their child(ren). Throughout the life course, this relationship “endure[s] with often complex patterns of interaction, support, and exchange that wax and wane around key transitions in the adult years” (Zarit & Eggebeen, 2005, p. 135). As parents’ age, the tie with their adult children may become even more influential as they lose other social ties (Milkie et al., 2008). Therefore, it is important to examine how aspects of this relationship may influence health outcomes for parents in later life.
The present study, informed by the life course perspective and solidarity-conflict framework, uses longitudinal data to enhance our understanding of how complex and multidimensional intergenerational relationships (specifically the tie between parents and adult children) influence health in later life. To do this, we first examined whether social support and social strain between parents and adult children were associated with the onset of disability as assessed by activities of daily living (hereafter, ADL disability) in later life. Then, we created four patterns of relationship quality between parents and adult children based on the average scores of social support and social strain indicators—high quality (i.e., high support and low strain), adverse (i.e., low support and high strain), indifferent (i.e., low support and low strain), and ambivalent (high support and, high strain)—and examined how these patterns were associated with the onset of ADL disability. ADL disability, also referred to as self-care disability, is identified by difficulty in performing basic, necessary, and socially defined tasks such as bathing, eating, and dressing. According to data from the 2019 American Community Survey, about four million adults 65+ years old reported difficulty with at least one ADL (United States Census Bureau, 2021). The onset of ADL disability often represents a transition to a state that has consequences for human agency, independence, and potentially quality of life (Latham-Mintus & Landes, 2023). It may also require an adult child to engage in more caretaking behaviors. As such, it is imperative to identify how the quality of relationships between adult children and parents may influence the onset of ADL disability.
Theoretical and Empirical Background
Intergenerational Social Support and Social Strain
Many studies that examine social relationships and health broadly utilize the life course perspective as a guiding framework. The life course perspective highlights the importance of “linked lives” which emphasizes that individual lives are embedded in and influenced by relationships with friends and family, that may be beneficial or harmful to health (Bengtson et al., 2012; Elder et al., 2003).
Moreover, scholars argue that the quality of a social connection is important to consider in assessing the association between social relationships and health (Antonucci et al., 2014; Song et al., 2021; Umberson & Montez, 2010). Support and strain are key dimensions of intergenerational relationship quality (Bengtson et al., 2002; Birditt et al., 2012), and past theoretical and empirical work provides reasons to expect that social relationships with adult children may influence parental health. Social support includes instrumental (e.g., transportation and help with daily tasks), informational (advice), and emotional (feeling loved and, cared for) support that may buffer against detrimental health outcomes (Thoits, 2010; Umberson & Montez, 2010). Social strain has been identified as a stressor that triggers hormones leading to the dysregulation of bodily systems and negatively influences health (Rook, 2014; Umberson et al., 2014). Social strain is measured by assessing relationships between parents and adult children that are demanding, critical, and involve conflict and tension (Antonucci et al., 2014).
Most studies examining emotional support (the domain of social support utilized in the present study) and ADL disability have found that higher levels of emotional support are often protective against later-life ADL disability risk (Mavandadi et al., 2007; McLaughlin et al., 2012; Mendes de Leon et al., 2001; Torres et al., 2018), but other studies do not support this thesis (Mao et al., 2018; Seeman et al., 1996). Fewer studies on social relationships and ADL disability have examined negative dimensions of relationship quality, but in general, these studies have observed that negative social interactions in later life were associated with higher rates of ADL disability over time (Krause & Shaw, 2002; Mavandadi et al., 2007).
Although these studies are important for the current study, we aim to build on this literature in two ways. First, most prior work on social relationships and ADL disability has examined support and strain as separate and independent dimensions of relationship quality. However, individuals may experience both support and strain within the same relationship, and it is unclear how the combination of emotional support and strain is associated with the onset of ADL disability in later life. Second, previous studies have examined the influence of social support or strain on ADL disability independent of relationship type, but we systematically examine whether relationships between parents and their adult children are associated with ADL disability.
Complexity in Relationships Between Parents and Adult Children
The solidarity-conflict framework specifies that positive and negative aspects of intergenerational relationships exist simultaneously (Bengtson et al., 2002; Bengtson & Oyama, 2010). Although many studies focus on either social support or relationship strain in intergenerational ties, recent research has highlighted the importance of addressing the positive and negative components of relationships (Gilligan et al., 2015). Intergenerational relationships are complex, thus focusing on either positive or negative features alone can mask important elements of these relationships (Bengtson & Oyama, 2010). One avenue for examining the complexity of relationships is to assess both support and strain indicators simultaneously. Another avenue is to examine patterns of relationships that combine both positive and negative aspects (i.e., ambivalent and indifferent ties).
Studying ambivalent relationships (i.e., those that can be classified as both positive and negative) takes us “beyond the dualistic view” of social relationships by emphasizing the “coexistence of contradictory sentiments, expectations, and forces” as characteristics of social relationships (Connidis, 2015, p. 77). In the solidarity-conflict framework, these ties have also been referred to as “intense ties” (Van Gaalen & Dykstra, 2006). Scholars have shown that ambivalence is a common characteristic of relationships between parents and their adult children partly because ties among family members often encourage a form of commitment and obligation, regardless of the quality of the tie (Gilligan et al., 2015; Pillemer & Suitor, 2002).
Ambivalent relationships may represent a specific type of stressor, one identified by uneasiness, unpredictability, and uncertainty in social ties. Indeed, scholars have reported that despite the positivity found in ambivalent ties, they are associated with worse health outcomes including greater psychological distress (Uchino et al., 2004), higher blood pressure (Holt-Lunstad et al., 2007), and shorter telomere length, an important biomarker of aging (Uchino et al., 2012). To our knowledge, only a couple of studies have examined the implications of ambivalent social ties on physical functioning, using cross-sectional analyses. First, Rook and colleagues (2012) found that ambivalent social ties were more strongly related to functional health limitations (a composite measure of ADLs and IADLs) than exclusively problematic ties. More recently, Brown and Rook (2022) reported that having more ambivalent ties in one’s network was related to higher levels of functional limitations (ADLs and IADLs), but diversity of ambivalent ties (i.e., the number of distinct roles in these ties) was related to fewer functional limitations. These studies examined associations at one time point; however, the current study investigates how patterns of relationship quality between parents and their adult children may influence the age of disability onset 12–14 years later.
Further, an understudied dimension of relationship quality is indifferent ties. Indifferent ties are characterized by both low support and low strain and can be considered the opposite of ambivalent ties (Ross et al., 2019). Some scholars question the importance of accounting for indifferent ties because they are loosely linked ties and thus unlikely to influence health (see Ross et al., 2019). Yet, others argue indifference in close relationships could indicate withdrawal or disengagement and thus be distressing and disadvantageous for health and well-being (DeLongis et al., 2004; Ross et al., 2019). For example, DeLongis and colleagues (2004) conducted a study on couples using daily diaries and found that low negative exchanges and low positive exchanges were associated with higher levels of negative affect the following day. To our knowledge, most of the studies that explore indifferent ties focus on marital relationships. We investigate how relationships between parents and their adult children that are low on both positive and negative indicators are associated with ADL disability in later life as this is an important lifelong tie.
Research Questions
Relationships between parents and their adult children involve a long-term tie that is associated with many expectations and commitments, affectively intense, and generally hard to exit (Thoits, 2003). The nature of this tie may shift throughout the life course as parents and their adult children transition through different stages. Thus, we examined whether social support, social strain, and different patterns of relationship quality between parents and their adult children influenced the onset of ADL disability. The life course perspective emphasizes the importance of timing and life transitions. Thus, understanding the association between the quality of the parent and adult–child tie and later ADL disability onset is important to identify a potential factor, relationship quality, that could delay the age at which the onset of an ADL disability occurs. Based on the current literature, the present study addresses the following research questions: 1. Are social support and social strain from adult children associated with the age of ADL disability onset among parents in later life? 2. Compared to high-quality relationships between parents and their adult children, are adverse, indifferent, and ambivalent relationship patterns associated with an earlier onset of ADL disability among parents?
Methods
Sample
This study used longitudinal data from the Health and Retirement study (HRS), a nationally representative, biennial panel study of American adults aged 50 years and older, with oversampling of Black and Hispanic Americans and Florida residents. More information about the design of the HRS is presented by Sonnega and colleagues (2014). Due to survey design, respondents in the HRS were randomly selected to answer questions for relationship quality in either the 2006 or the 2008 psychosocial questionnaire. To optimize the use of variables from this half-sample questionnaire, we gathered wave 1 (W1) ADL disability and most covariates in either 2006 or 2008, matching participation in the psychosocial questionnaire, and followed initial respondents prospectively through 2020.
The analytic sample was limited to respondents who met the following criteria: (a) participated and had non-zero weights (i.e., 50+ years of age, noninstitutionalized, and alive) in the 2006 or 2008 wave including the psychosocial module (N = 13,770), (b) did not report an ADL disability prior to or at baseline age (N = 9,817), (c) self-identified as non-Hispanic White, non-Hispanic Black, or Hispanic (N = 9,624), (d) reported having at least one living child (if missing or status of any child is unknown, respondent was excluded) (N = 8,368), (e) reported at least one indicator of social support and one indicator of social strain used to create the relationship quality indicators (N = 8,318), and (f) were not missing on any covariates in the study (N = 8,101).
Measures
ADL Disability
The dependent variable in this study was age of onset of an ADL disability during the study period. HRS respondents were asked whether they have any difficulty performing five tasks: bathing, eating, dressing, walking across a room, and/or getting in or out of bed. We utilized RAND’s measure of ADL disability, which summed the number of activities that respondents reported some difficulty accomplishing and identified the age at which respondents reported at least one ADL. Respondents who reported an ADL disability prior to or at their W1 age (1994 to 2006 or 2008) were excluded to ensure temporal ordering in our models. Respondents who did not develop an ADL disability were assigned their age at the last wave (2020) and treated as censored in our survival models.
Relationship Quality Patterns
In the 2006 or 2008 psychosocial questionnaire, respondents were asked seven questions to examine the perceived social support and social strain that they receive from their child(ren). Social support was gathered with three items that stated: “Thinking about all of your living children” … (1) “how much do they really understand the way you feel about things?”; (2) “how much can you rely on them if you have a serious problem?”; and (3) “how much can you open up to them if you need to talk about your worries?” An index was created by averaging across all social support items, ranging from “not at all” (0) to “a lot” (3) (α = .81). Social strain was gathered with four items that stated: “Thinking about all of your living children” … (1) “how often do they make too many demands on you?”; (2) “how much do they criticize you?”; (3) “how much do they let you down when you are counting on them?”; and (4) “how much do they get on your nerves?” An index was created by averaging across all social strain items, ranging from “not at all” (0) to “a lot” (3) (α = .77).
Following a similar approach as others (Ross et al., 2019; Uchino et al., 2001), we identified the mean of social support and social strain after applying the exclusion criteria and used these numbers to create the relationship quality patterns between parents and their adult children. High quality (reference group) were relationships that were above average in social support and below average in social strain. In contrast, adverse relationships were relationships that were below average in support and above average in strain. Indifferent relationships were below average in both support and strain domains, whereas ambivalent relationships were above average on both support and strain. No respondents had scores exactly at the means of support or strain because these numbers were not rounded. See Figure 1 for a conceptual representation of the four domains of relationship quality. Conceptual representation of the relationship quality indicators based on the mean score of social support and social strain. 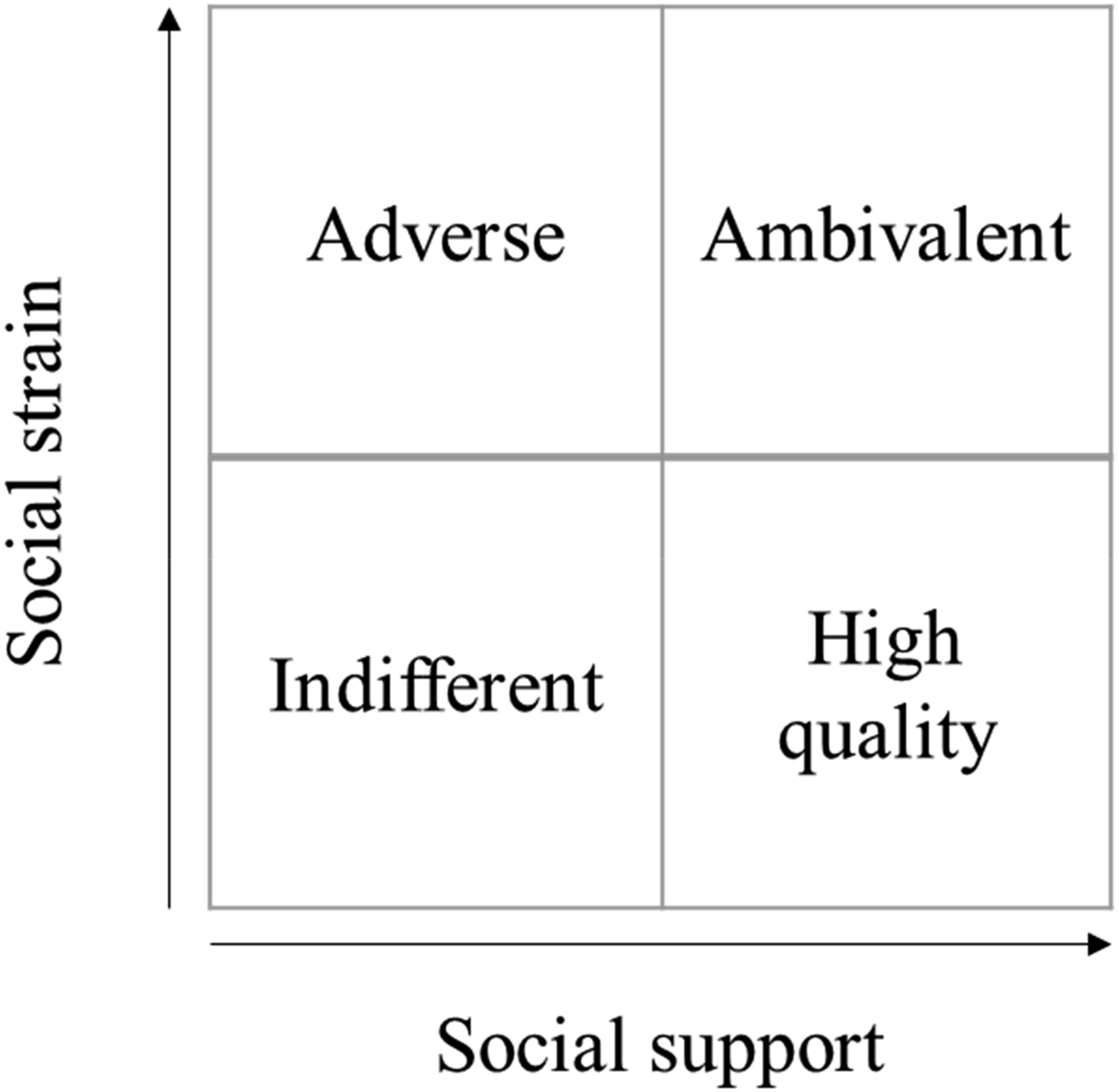
Covariates
We used a binary variable to differentiate men and women (0 and 1, respectively) and three binary variables (0,1) to assess race and ethnicity: non-Hispanic White (reference group), non-Hispanic Black, and Hispanic adults. We also adjusted for additional characteristics known to influence disability in later life. Two adult resources were included: education (years of schooling, top coded at 17+) and household wealth (tens of thousands of dollars and cube rooted to correct for skewness). In addition, we adjusted for number of living children (top coded at 11+).
Four adult health-related indicators were also included. Depressive symptoms were measured using an 8-item Center for Epidemiological Studies – Depression (CES-D) score in which a higher score indicates more symptoms. Self-rated health ranged from 0 (poor) to 4 (excellent). A self-reported physical activity scale gathered both frequency and intensity of exercise. Participants were asked how often they participated in moderate and vigorous physical activity, with five response categories: never/rarely = 0; one to three times per month = 1; once per week = 2; two or more times per week = 3; and everyday = 4. The scale was created by weighting the type of physical activity by intensity (moderate = 1.4, vigorous = 1.8) based on metabolic equivalent recommendations (Latham & Williams, 2015). Possible scores ranged from 0 (no physical activity) to 12.8 (moderate and vigorous physical activity daily). Body-mass index (BMI) was based on self-reports and categorized into underweight or normal weight (BMI < 25), overweight (25 ≥ BMI < 30), and obese (BMI ≥ 30). We combined underweight/normal due to a small number of respondents in the underweight category. In preliminary analyses, we also tested for underweight as a separate category but found that it was non-significant.
Analytic Strategy
The analysis was conducted in two steps using Stata/SE 18.0. First, we gathered descriptive statistics for all variables used in the study. Second, event history analysis was used to prospectively examine the association between relationship quality among parents and their adult children and the onset of first ADL disability (i.e., incidence over a 12–14-year study period). All event history analyses require two variables: an incidence (or censoring) variable and a duration variable. The incidence variable was whether a respondent reported an ADL disability during the study period, and the duration variable was age at onset of ADL disability (or last observed age for respondents who did not develop an ADL disability). As opposed to using survey wave as the metric of time, we used age measured as the year and month of the survey interview in which respondents experienced ADL disability onset. Age of onset was thus approximate and only accurate up to the 2-year interval of HRS waves. We used age at last report for respondents who did not report an ADL but left the sample during the study period (i.e., censored). Using age as the time metric for the longitudinal analysis enabled us to interpret the transition to disability as an age-specific incident function (Thiébaut & Bénichou, 2004).
For the event history analysis, we employed a Weibull accelerated failure time (AFT) model, a parametric survival model. Weibull AFT models are common in health and aging research (e.g., Bauldry et al., 2023; Liu et al., 2023; Sauerteig-Rolston & Ferraro, 2024) and were beneficial for this analysis for a couple of reasons. Unlike the Cox model, the Weibull AFT model does not rely on a proportional-hazards assumption. In preliminary analyses, we fit a Cox model and found the same pattern of substantive findings but noted failures to the proportional-hazards assumption for the global test and key variables. In addition, Weibull AFT models are quite flexible and can account for aging processes in which the probability of experiencing an event can increase, decrease, or stay the same over time, with the first being what we would expect for ADL disability. An increasing failure rate (i.e., time to onset) is denoted by a shape parameter (Ln_p) that is greater than one. In all models, we found a shape parameter greater than one meaning that the probability of experiencing an ADL disability increased with age. The results from the Weibull AFT models can be interpreted both in terms of the coefficient (β) and time ratio (eβ). Earlier onset of disability was reflected in a negative β (and eβ < 1) while later onset was reflected in a positive β and (eβ >1). Analyses incorporated respondents’ weights from the psychosocial questionnaire and adjusted for the complex sample design using cluster robust standard errors.
Results
Sample Characteristics
Descriptive Statistics, N = 8,101.
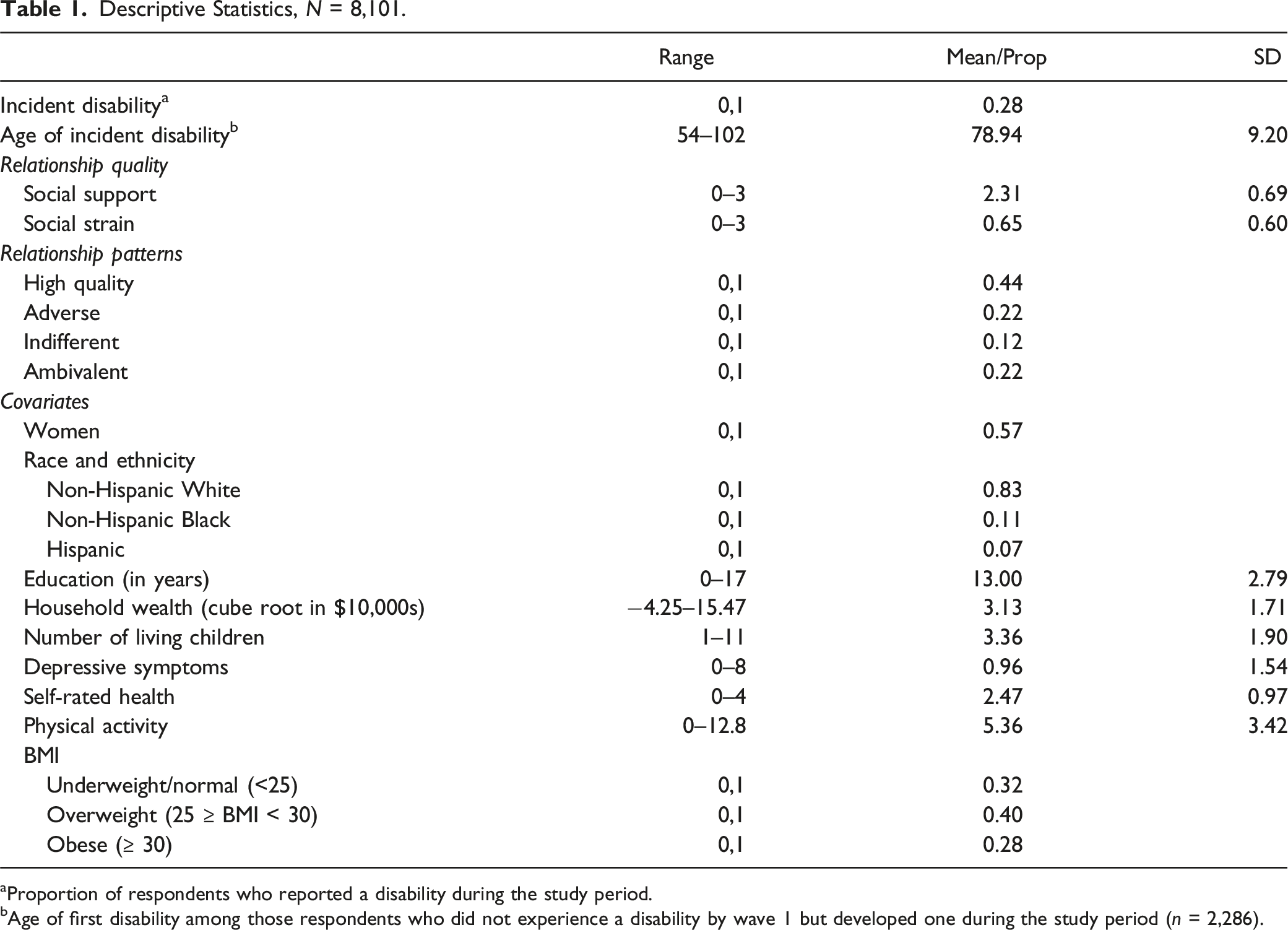
aProportion of respondents who reported a disability during the study period.
bAge of first disability among those respondents who did not experience a disability by wave 1 but developed one during the study period (n = 2,286).
Support and Strain with Adult Child and Disability Incidence Among Parents
Weibull Accelerated Failure-time Models Associated With Support and Strain Between Parents and Their Adult Children and Incidence Disability (N = 8,101).
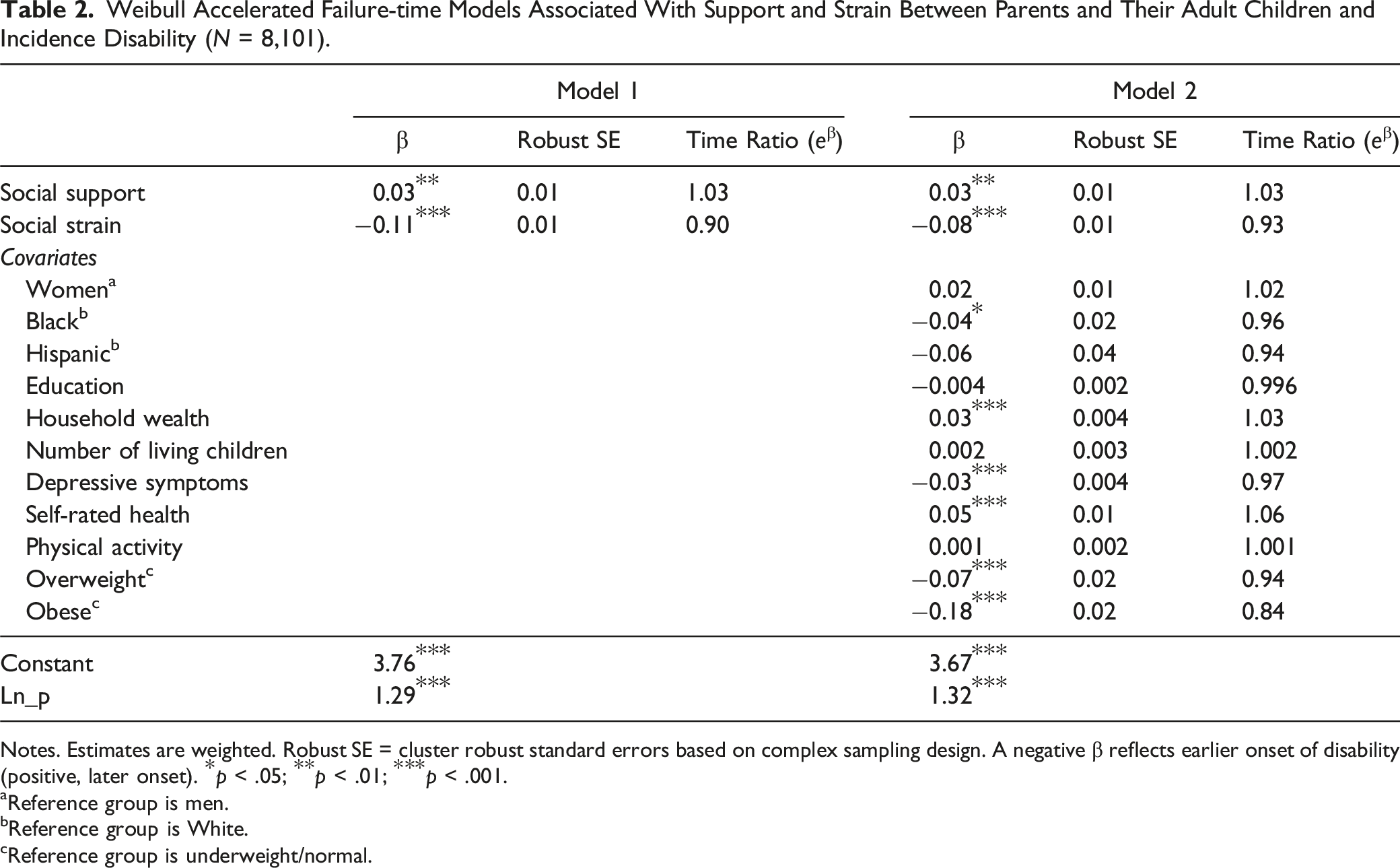
Notes. Estimates are weighted. Robust SE = cluster robust standard errors based on complex sampling design. A negative β reflects earlier onset of disability (positive, later onset). *p < .05; **p < .01; ***p < .001.
aReference group is men.
bReference group is White.
cReference group is underweight/normal.
Relationship Quality Patterns and Disability Incidence Among Parents
Weibull Accelerated Failure-time Models Associated With Relationship Patterns Between Parents and Their Adult Children and Incidence Disability (N = 8,101).
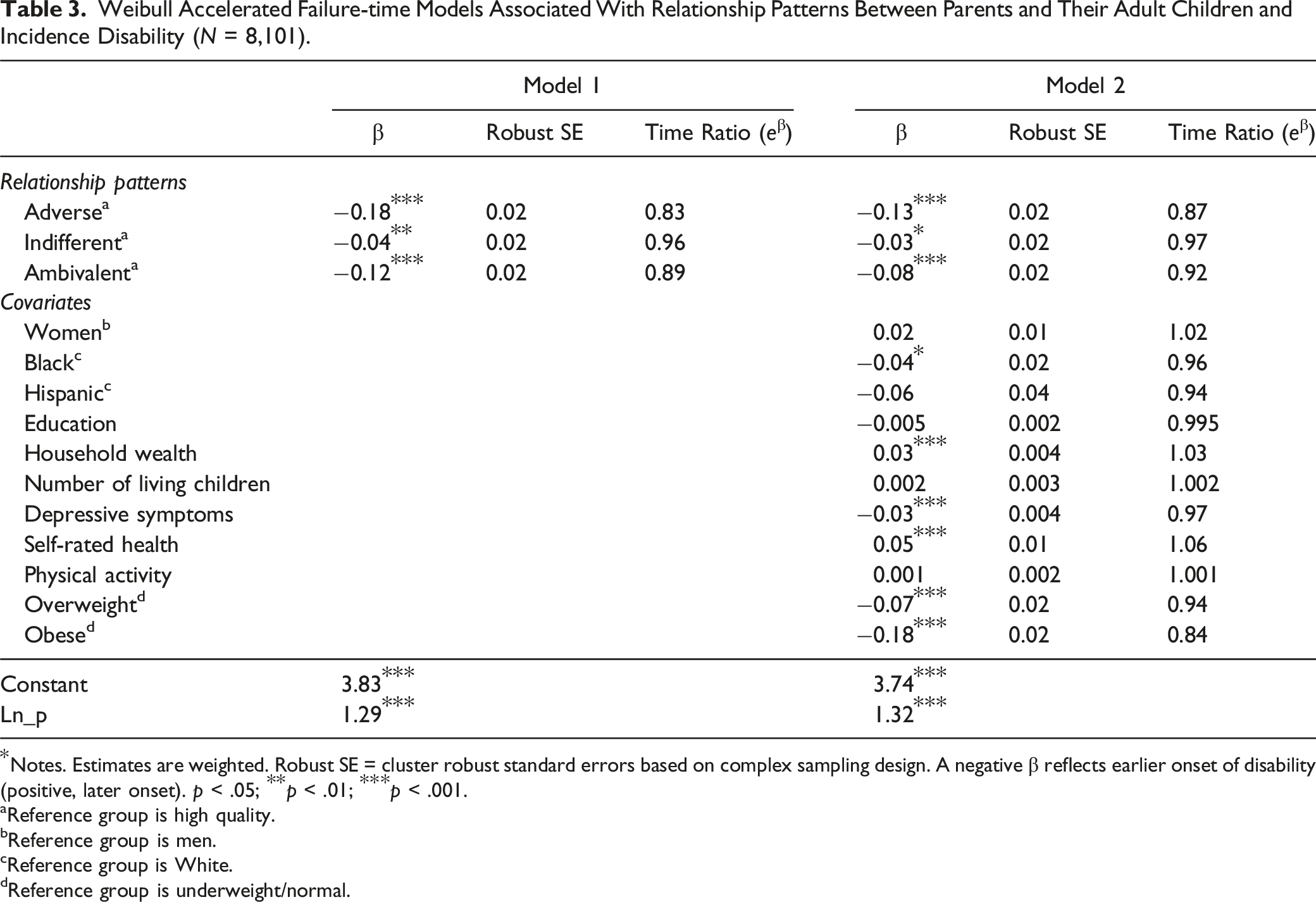
Notes. Estimates are weighted. Robust SE = cluster robust standard errors based on complex sampling design. A negative β reflects earlier onset of disability (positive, later onset). p < .05; **p < .01; ***p < .001.
aReference group is high quality.
bReference group is men.
cReference group is White.
dReference group is underweight/normal.
Model 2 adjusted for additional factors known to influence disability. The results for Model 2 revealed that respondents in adverse relationships with their adult children experienced the onset of ADL disability 12% ([1- e−0.13 X 100]; β = −0.13, p < .001) earlier than those in high-quality relationships. Respondents in indifferent relationships experienced the onset of ADL disability 3% ([1- e−0.03 X 100]; β = −0.03, p < .05) earlier than those in high-quality relationships. Moreover, respondents in ambivalent relationships experienced the onset of ADL disability 8% ([1- e−0.08 X 100]; β = −0.08, p < .001) earlier than those in high-quality relationships.
In addition, Black respondents experienced an earlier onset of disability than White respondents (β = −0.04, p < .05). Higher household wealth was associated with a later onset of ADL disability (β = 0.03, p < .001). Higher levels of depressive symptoms and being overweight or obese compared to having a normal weight were associated with an earlier onset of ADL disability during the study period (respectively, β = −0.03, p < .001; β = −0.07, p < .001; β = −0.18, p < .001), while reporting better self-rated health was associated with a later onset of ADL disability (β = 0.05, p < .001).
Weibull Accelerated Failure-time Models With Different Reference Group Comparisons for Relationship Patterns Between Parents and Their Adult Children and Incidence Disability (N = 8,101).
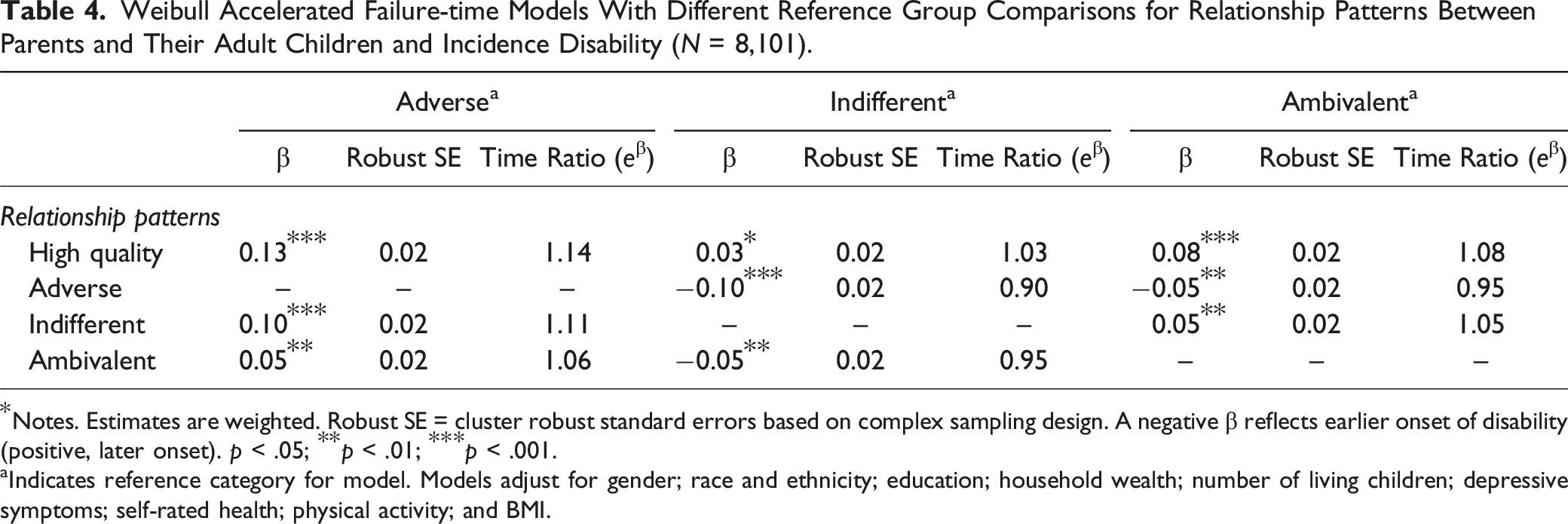
Notes. Estimates are weighted. Robust SE = cluster robust standard errors based on complex sampling design. A negative β reflects earlier onset of disability (positive, later onset). p < .05; **p < .01; ***p < .001.
aIndicates reference category for model. Models adjust for gender; race and ethnicity; education; household wealth; number of living children; depressive symptoms; self-rated health; physical activity; and BMI.
Discussion
Relationships between parents and their children are a lifelong tie that may influence parental health in later life. Informed by the life course perspective and the solidarity-conflict framework, we investigated relationship quality between parents and their adult children and ADL disability onset. Numerous studies have indicated that negative relationships between parents and their adult children are considerably less prevalent than positive ones (see Offer, 2021) and that parents, specifically mothers, and their adult children maintain a high degree of intergenerational solidarity throughout the life course (Stepniak et al., 2022). In this study, we incorporated the complex and multidimensional components of ties between parents and adult children to examine how the quality of these enduring relationships may influence the age of onset of ADL disability in later life. Consistent with prior studies, we found that high quality relationships were the most common pattern reported, followed by adverse, ambivalent, and indifferent. Further, results revealed that social support and social strain had opposite but expected associations with the onset of ADL disability. Moreover, the combination of support and strain in unique relationship quality patterns was influential for the incidence of ADL disability in later life. Being able to maintain independence, autonomy, and physical functioning in older life is an aspirational goal for many adults, yet adverse, indifferent, and ambivalent relationships between parents and their adult children represent a threat to this goal.
Relationship Quality Between Parents and Adult Children and ADL Disability
We found that social support was beneficial for later life ADL disability onset, a pattern reported by most studies examining social support across domains of relationships and ADL disability (Mavandadi et al., 2007; McLaughlin et al., 2012; Mendes de Leon et al., 2001; Torres et al., 2018). We also found that social strain was associated with an earlier onset of ADL disability, suggesting that stressful aspects of intergenerational relationships are harmful for health.
Because we found that support and strain simultaneously influenced ADL disability, we were particularly interested in exploring our typology of relationship patterns which was composed of different combinations of social support and strain. Indeed, we found unique effects of relationship quality patterns between parents and adult children on ADL disability, emphasizing the importance of adverse, ambivalent, and indifferent relationships that are less often studied. First, we found that compared to older adults in high-quality relationships, older adults in adverse relationships had an earlier onset of ADL disability in later life. The negativity in these relationships may be a salient source of stress, which has deleterious effects on health (Pearlin, 1999; Rook, 2014). This finding supports other studies that reported a negative association between social strain and health broadly (Rook, 1984, 2014; Thomas et al., 2022). Adverse social relationships were considerably less prevalent than high-quality relationships, consistent with previous studies (e.g., Offer, 2021); however, the potency of intergenerational relationships patterned by low levels of support and high levels of strain is important to consider for understanding ADL disability in later life.
Second, consistent with prior studies on intergenerational ambivalence (Gilligan et al., 2015; Pillemer & Suitor, 2002), we found that ambivalent ties were common, with over 20% of respondents having above average levels of support and strain. Moreover, older adults who reported ambivalent relationships experienced the onset of ADL disability at earlier ages than those in high-quality relationships. This link between ambivalent ties and worse health has been reported in cross-sectional studies (e.g., Holt-Lunstad et al., 2007; Rook et al., 2012), yet the present study is distinct in that it examined and found long-reaching implications of ambivalent relationship patterns between parents and adult children.
When comparing ambivalent and adverse ties to each other as opposed to high-quality relationships, we found that adverse ties were more detrimental for ADL disability (i.e., an earlier onset) than ambivalent ties. Having a tie that is high in strain and low in support is more detrimental than one that is high in support and high in strain, indicating that ambivalent ties may be less damaging than adverse ties and that support in these ties may buffer some of the harmful effects of strain in these ties (e.g., Offer, 2020). Rook and colleagues (2012) found that ambivalent social ties were more strongly related to functional health limitations than exclusively problematic ties, but we found the opposite. We argue this difference could be due to several methodological decisions including (1) the type of relationship being examined, (2) the measure of functional health, and (3) a cross-sectional versus longitudinal analysis.
Third, unique to this study is the examination of indifferent relationship patterns. Indifferent relationships were the least common relationship pattern between parents and their adult children in this study. Respondents that reported indifferent relationships had an earlier onset of ADL disability than respondents in high-quality relationships after adjusting for factors known to influence the association. Moreover, respondents in indifferent relationships had a later onset of ADL disability than respondents in either ambivalent or adverse relationships. As such, intergenerational relationships composed of low levels of support and strain may indicate that the potency and intensity of the tie is lower and thus less influential for later-life ADL functioning.
Limitations and Future Directions
Although this study makes important contributions to the growing literature of relationships between parents and adult children and health, it is not without limitations. First, we used an indirect measure of ambivalence and indifference as opposed to a direct measure. The HRS did not ask respondents if they experienced ambivalence or indifference in their relationships, so we calculated patterns of relationships based on the mean reports of support and strain (Connidis, 2015), which could include some measurement error. Second, we were interested in the first onset of an ADL disability because even difficulty with one of these activities represents a significant threat to independent living. However, older adults may have acute episodes of disability for a variety of reasons. For example, the onset of disability may be caused by a specific ailment, such as a broken hip, but after orthopedic surgery and appropriate physical therapy the person may be able to gain back functional independence. As such, more work is needed to examine what factors are associated with transitions in and out of ADL disability, as well as what factors are associated with the development of more than one ADL disability. Relatedly, we specifically studied ADL disability in this study, but it would be beneficial for future research to study other forms of disability, such as difficulty with instrumental activities of daily living (e.g., preparing a meal and taking medication), hearing and vision loss, and cognitive impairment that also pose a significant threat to independent living in later life. Fourth, an important next step could be to assess how these relationship patterns compare to reports of social isolation and/or integration (e.g., is being lonely/isolated or having adverse relationships more detrimental for health?). Fifth, the HRS does not ask about each parent–adult child relationship separately. For example, overall parent–adult child relationship quality may be ambivalent—high in strain and high in support—but this could be due to different relationships: one person may experience an ambivalent relationship with one child, whereas another person may have high support from one child and high strain from another. Sixth, we assume these relationships to be parent–adult child; however, we do not account for the age of adult children, and it is possible that some of the “adult children” in our study may be under the age of 18. Finally, we examined relationships between parents and their adult children from the parents’ point of view, yet there are other relationships that adults are engaged in throughout their life. Future studies would benefit from exploring relationship quality among other relationship domains (e.g., friendship and spouse) and how those may influence ADL disability.
Conclusion
This study illustrates the importance of acknowledging relationships as multidimensional and complex. We found that adverse relationships between parents and their adult children had far-reaching implications on disability onset throughout the study period. In addition, older adults who experienced ambivalent relationships with their adult children, composed of both high levels of support and high levels of strain, also faced an earlier transition to ADL disability compared to older adults in high-quality relationships. Promoting positive social relationships that are free of strain through interventions, especially between parents and their adult children, may help delay the onset of ADL disability. Perhaps specific resources such as educational information, family therapy, and support groups that help mitigate strains in the relationship between parents and their adult children would provide benefit. Finally, respite services that lighten the demand felt by adult children, especially after becoming the primary caregiver, may improve interactions. In sum, examining the complexity and multidimensionality of relationships is important to develop a better understanding of how they are related to health; high levels of social support may not be as beneficial if it is intertwined with high levels of strain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided by a grant from the National Institute on Aging to K.F. Ferraro (AG043544) and a Bilsland Dissertation Fellowship from the Office of Interdisciplinary Graduate Programs at Purdue University.