
Abstract
Objectives
To examine the mediating role of activities of daily living (ADL) in the association between stroke and depressive symptoms, and to investigate whether moderate physical activity (MPA) moderates this mediation in older adults, using sex-stratified analyses.
Methods
Cross-sectional data from 31,137 participants (≥65 years) were analysed using wave eight of the Survey of Health, Ageing and Retirement in Europe. Depression, ADL limitations, stroke history and weekly frequency of MPA were assessed. Mediation and moderated mediation analyses were conducted.
Results
ADL partially mediated the association between stroke and depression in males (36.53%) and females (37.20%). In males, both medium and high weekly frequencies of MPA significantly moderated the direct and indirect associations between stroke, ADL and depression. In females, only a high frequency of MPA (> once per week) showed a significant moderating effect.
Conclusion
Limitations in ADLs represent an important pathway linking stroke and depression in older age.
Keywords
Highlights
• MPA proved to be a significant moderator in mediating ADL in the relationship between stroke and depression. • Among males, weekly frequency of MPA (once a week and more than once a week) was a significant moderator. • Among female, only the high weekly frequency of MPA (more than once a week) was a significant moderator.
Introduction
Worldwide, stroke is one of the leading causes of death and disability (Bill & Foundation, 2024). In the European Union (year 2017), there were 1.12 million strokes, 9.53 million survivors, and 0.46 million deaths. Estimates predicted that, due to the ageing population, by 2047, stroke cases in European countries will increase by up to 27% (Avan et al., 2019). The health consequences of a stroke can be serious. Following an event, cerebrovascular lesions affect cognitive processing, leading to physical and motor impairments, increasing the risk of disability in performing activities of daily living (ADLs) (Louie et al., 2022; Saa et al., 2019). In general, stroke survivors experience difficulties interacting socially due to impaired physical and motor skills, in addition to facing long periods of functional recovery (Lee et al., 2015). Thus, the combination of motor impairment and low autonomy is a strong risk factor for the development of post-stroke depression (PSD) (Guo et al., 2022).
The differences in stroke incidence between the sexes vary with age (Shao et al., 2024). Below the age of 45, the prevalence of stroke mortality is similar for both sexes. Between 45 and 74 years, the mortality rate is higher in males; above 74 years, the risk of stroke and death is greater in females (Ospel et al., 2023). The higher number of stroke deaths among females is associated with their greater representation in the population, as well as the mortality rate in this group, especially among older adults (Reeves et al., 2008). Furthermore, the higher risk of stroke in females may be related to factors such as post-menopausal hormonal changes, obesity, metabolic syndrome, atrial fibrillation, and migraine (Whitiana et al., 2017).
It is estimated that 5% of stroke patients develop PSD in the first week after the event. In comparison, up to 84% of them experience an increase in PSD symptoms in the following 3 months (Knapp et al., 2020). Although PSD occurs in both sexes (Medeiros et al., 2020), comparatively, it is more prevalent in females than in males (Zhao et al., 2020). Among the mechanisms that can potentiate PSD, especially in females, are disturbances in the hypothalamic-pituitary-adrenal axis, inflammatory disorders (cytokines), autonomic dysfunction, alterations in prefrontal-subcortical circuits, and post-menopausal oestrogen fluctuations (Thériault & Perreault, 2019). A study investigating sex differences in PSD among older adults in the United States found, over 1.5 years of follow-up, that females had a risk of 0.20, while males had a risk of 0.16 (Mayman et al., 2021). However, longitudinal studies are needed, as subsequent assessments at 3 to 12 months revealed the disappearance of depressive symptoms (Dong & Brisa, 2020; Wang et al., 2017).
Neurological damage caused by a stroke can lead to motor deficits, disabling the patient from performing important ADLs (Whitiana et al., 2017). Following a stroke, individuals often face a previously unknown state of dependency, limiting their ability to interact socially or work (Ytterberg et al., 2022). All of this leads to dependency and a consequent reduction in quality of life, contributing to a vicious cycle of worsening health (Sara et al., 2024). A non-invasive, complementary strategy to traditional PSD treatments is to increase physical activity (PA). After a stroke, PA can mitigate secondary health changes associated with decreased activity, such as loss of muscle and bone mass and decreased cardiorespiratory fitness.
A recent systematic review highlighted the importance of daily and weekly energy expenditure for the recovery of post-stroke patients (Pasztor et al., 2025). Among the reported benefits are reductions in cardiovascular risk factors, improvements in cognitive and functional abilities, and enhancing quality of life (Li et al., 2023). Furthermore, adequate weekly PA levels can help treat depression caused by disability in performing ADLs (Cunningham et al., 2020).
To our knowledge, no study has examined, differentiated by sex, the associations between stroke, ADL, PSD, and PA levels in the older European population. Therefore, understanding how PSD is affected by improvements or worsening in ADL performance can inform the development of healthcare strategies during ageing. In turn, adequate post-stroke PA levels reduce cardiovascular risk factors, which may moderate the risk of recurrent strokes. However, the ideal PA intensity for stroke survivors is still unknown and needs to be investigated (Kramer et al., 2019). Furthermore, adequate levels of weekly PA can contribute to better performance in ADLs, and benefit the treatment of PSD. In this context, the PROCESS macro for SPSS is a convenient statistical tool for testing mediation and moderated mediation hypotheses (Hayes & Rockwood, 2017).
Thus, this study aimed to compare the mediating role of ADL in the relationship between stroke and depression, as well as to determine the moderating role of moderate physical activity (MPA) during the mediation of ADL in the relationship between stroke and depression. Our hypotheses were as follows: H1 = Stroke has a direct effect on depression; H2 = ADL mediates the indirect effect between stroke and depression; H3 = The direct and indirect mediating effects differ significantly between genders; H4 = MPA moderates the direct effect of stroke on depression mediated by ADL: the higher the weekly frequency of MPA, the stronger the moderating effect; H5 = MPA moderates the indirect effect of ADL on the association between stroke and depression: the higher the weekly frequency of MPA, the stronger the moderating effect; and H6 = The moderating effects differ significantly between males and females.
Methods
Design and Data Source
Data were drawn from the Survey of Health, Ageing and Retirement in Europe (SHARE) (Börsch-Supan et al., 2013). SHARE is a transnational panel survey conducted biennially since 2004 to provide comparable information on the health and well-being, social and employment conditions of European and Israeli citizens aged 50 and older. We used data from wave eighth (2019–2020). Information was collected through face-to-face home interviews using computer-assisted methods. All participants gave informed consent before being interviewed. The procedures that ensured the confidentiality and data privacy of the SHARE protocol survey were reviewed and approved by the Ethics Committee of the University of Mannheim and the Ethics Committee of the Max-Planck Society for the Advancement of Science. All survey procedures were carried out in accordance with the ethical guidelines and regulations of the Declaration of Helsinki. Further details can be found on the project’s official website (https://share-eric.eu/), including methodological procedures for wave 8.
Study Population
This cross-sectional study utilised data from Wave 8 of the SHARE database, which comprised 46,270 participants aged 50 and above. Figure S1 illustrates the flowchart for selecting the study sample. Our analyses focused on individuals aged 65 and over, resulting in a sample of 32,643. We excluded participants with Alzheimer’s disease or dementia (n = 455) and those with missing data for any variables of interest (n = 1,051). This left us with a final sample of 31,137 participants (17,576 female) from the following 27 European countries. Figure 1 presents the flowchart of the study sample, while Table S1 (Supplemental Material) presents the detailed distribution of participants by country. Flowchart of the study sample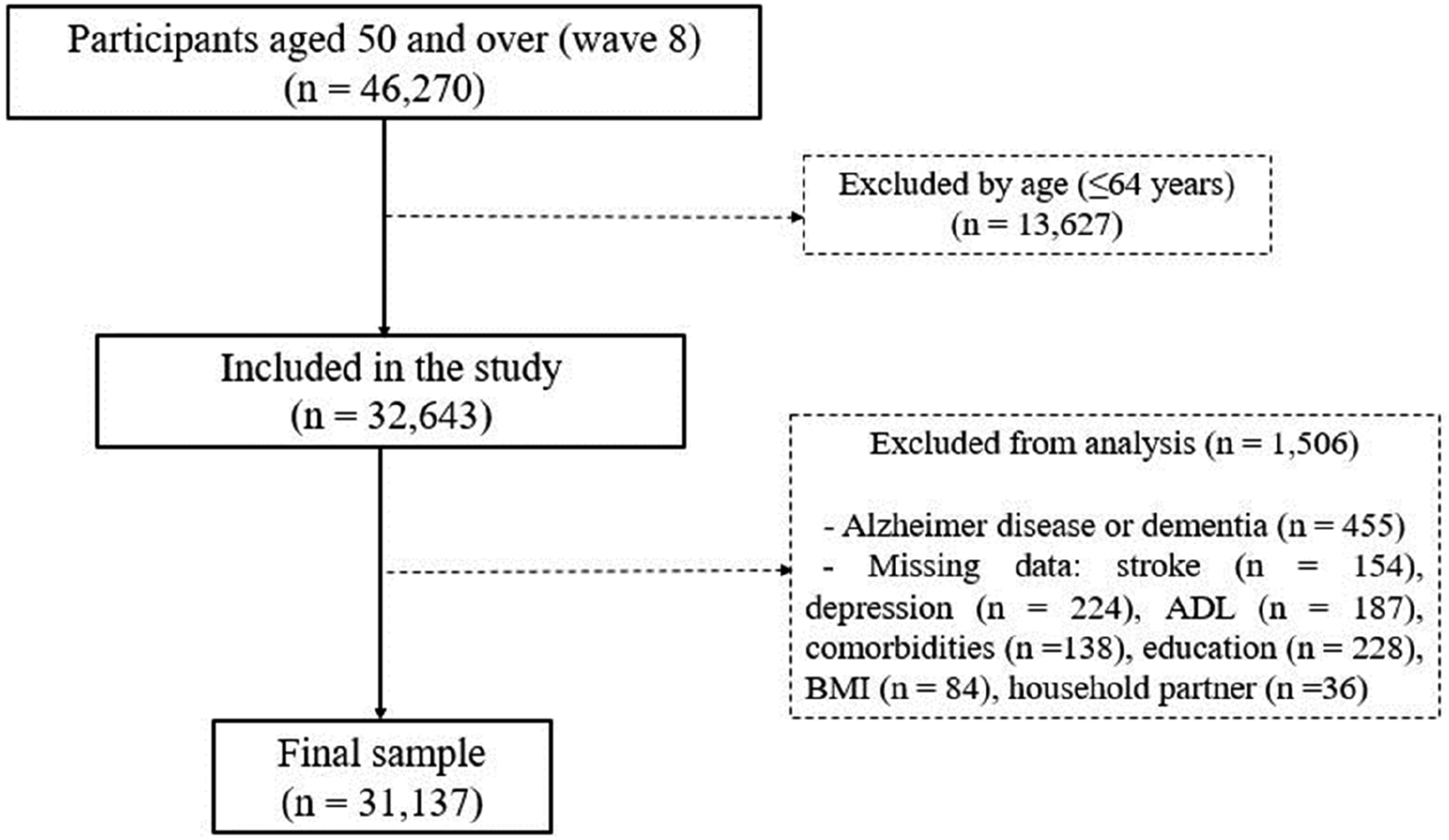
Measures
Depression
Depression was assessed using the 12-item EURO-D scale (Prince et al., 1999), which evaluates 12 aspects of depressive symptomatology over the past month. The scoring system varies from 0 to 12. The higher the score, the greater the indication of depressive symptom severity. The cutoff point ≥ 4 points is conventionally used to identify clinically significant depression (Gallagher et al., 2013).
Stroke
Information on stroke status and onset date was collected via self-report with the following questions: ‘Has a doctor ever told you that you had a stroke?’ (answers: ‘yes’ or ‘no’) and ‘About how old were you when you were first told by a doctor that you had a stroke?’.
Activities of Daily Living
The ADL index describes the degree of decrease in performing activities of daily living (Katz, 1963). The instrument uses a dichotomous scale (yes/no), with 1 point being assigned for each ADL in which the individual is dependent and 0 (zero) points for each ADL in which the respondent is independent. The score ranges from 0 to 6 (a high score means a need for assistance, while a low score indicates independence in performing ADLs).
Moderate Physical Activity
Moderate physical activity was analysed as a categorical variable reflecting weekly frequency, in line with the structure of the SHARE questionnaire and previous SHARE-based research, to ensure interpretability and model stability in sex-stratified moderated mediation analyses. Participants were asked about their physical activity levels, initially using the following question: ‘How often do you perform physical activities that require physical effort, such as sports, heavy household chores, or a job that requires physical labour?’. Subsequently, the weekly intensity of physical activity was questioned, as follows: ‘Do you perform moderate physical activity (MPA)?’. Finally, responses were reverse coded from lowest weekly/monthly frequency to highest weekly frequency: (1) MPA < once a week, (2) MPA once a week, and (3) MPA > once a week (Marques et al., 2019). Moderate physical activity and depression were assessed contemporaneously at the time of the interview and refer to recent or habitual behaviours, precluding the establishment of temporal precedence between these measures.
Covariates
A group of eight covariates related to stroke events, depression, reduction in ADLs, and physical activity were selected. All confounders were self-reported in face-to-face interviews: country, age, BMI, comorbidities (hypertension, diabetes, cholesterol, heart attack), lifestyle (alcohol, tobacco), previous heart attack, education, and household partner. BMI was calculated as weight/height2 (kg/m2) and categorised as underweight (<18.5), normal (18.5–24.9), overweight (25–29.9), and obese (≥30) (WHO, 2020). Comorbidities came from medical reports: hypertension was included because most acute ischaemic stroke patients present high blood pressure (Lee et al., 2019); diabetes is a recognised risk factor and frequent in stroke (Rouzbahani et al., 2021); cholesterol was considered due to its role in ischaemic heart disease, atherosclerosis, and risk of clots/embolism (Varbo & Nordestgaard, 2019). Alcohol and tobacco are stroke risk factors (Smith et al., 2024). Heart attack was included given its high post-stroke incidence and interrelation with stroke and depression (Kleindorfer et al., 2021). Education was controlled since, in advanced age, cognition sustains ADLs and autonomy; SHARE uses ISCED (Schneider, 2013), aggregated into four groups: (1) ISCED 0–1 (no/low), (2) ISCED 2–4 (intermediate), (3) ISCED 5–6 (tertiary), (4) university. Household partner (yes/no) was included as partner support may protect against post-stroke and age-related depressogenic stressors (Choi & Ha, 2011).
Statistical Analyses
Descriptive statistics were presented as frequencies (percentages) or means (standard deviations). Sex differences were tested with chi-square (categorical) and Student’s t-test (continuous). Relationships between main variables were verified with Pearson’s correlation, classified as 0.1 (small), 0.3 (medium), and ≥0.5 (large) (Cohen, 1988). Given the cross-sectional nature of the data, all analyses examined statistical associations rather than causal relationships. The PROCESS macro for SPSS, more specifically Model 4 (Figure 2(A)), was used to test ADLs as mediators between stroke and depression (Hayes, 2018). Analyses were controlled for covariates (i.e. countries, age, BMI, comorbidities, education, household partners). The model examined the direct effect of stroke on depression (‘c’ path) and the indirect effect through ADL (‘a1’ and ‘b1’ paths). Mediation was assumed when the 95% CI of the bootstrap-estimated indirect effect did not include zero (Hayes & Rockwood, 2017). Separate models were run for males and females: Model 1 without and Model 2 with covariates. The mediated proportion was calculated as the indirect effect divided by the total effect (Ditlevsen et al., 2005). Sex differences were assessed by comparing indirect effect CIs; overlap indicated no significant difference (Schenker & Gentleman, 2001). The analysis of moderated mediation was also processed in the PROCESS macro for SPSS (Model 59, Figure 2(B)) (Hayes, 2018). The procedures were controlled for covariates (i.e. countries, age, BMI, comorbidities, education, household partners). Stroke (dichotomous) and depression (continuous) were mediated via ADL (continuous), and moderated by three MPA paths (categorical: W0 = MPA <1/week, W1 = MPA = 1/week, W2 MPa >1/week). This procedure allowed us to examine the intensity and direction of each of the three MPA moderators on ADL during their mediation in the relationship between stroke and depression. In the analyses, W0 was assumed as the reference. The results were interpreted as M1 = W1 vs W0 and M2 = W2 vs W0. The analyses were stratified by sex. Moderation was assumed when indirect contextual effects differed (Hayes & Rockwood, 2017). Significance was assumed when the 95% bias-corrected bootstrap CI excluded zero (Hayes & Rockwood, 2017). Bootstrapping with bias correction and acceleration (BCa, 10,000 resamples) estimated CIs (95%). Post-hoc analyses tested moderated mediation at high (+SD), mean, and low (–SD) MPA (Preacher et al., 2007). Simple slope analysis verified MPA moderation of the stroke–depression relationship via ADL. All analyses used IBM SPSS 21.0. Significance was set at α < 0.05. Conceptual framework of the potential mediating effect of activities of daily living (ADL) on the association between stroke and depression, and model of potential moderating effects of moderate physical activity (MPA) levels on ADL mediation trajectories in the relationship between stroke and depression.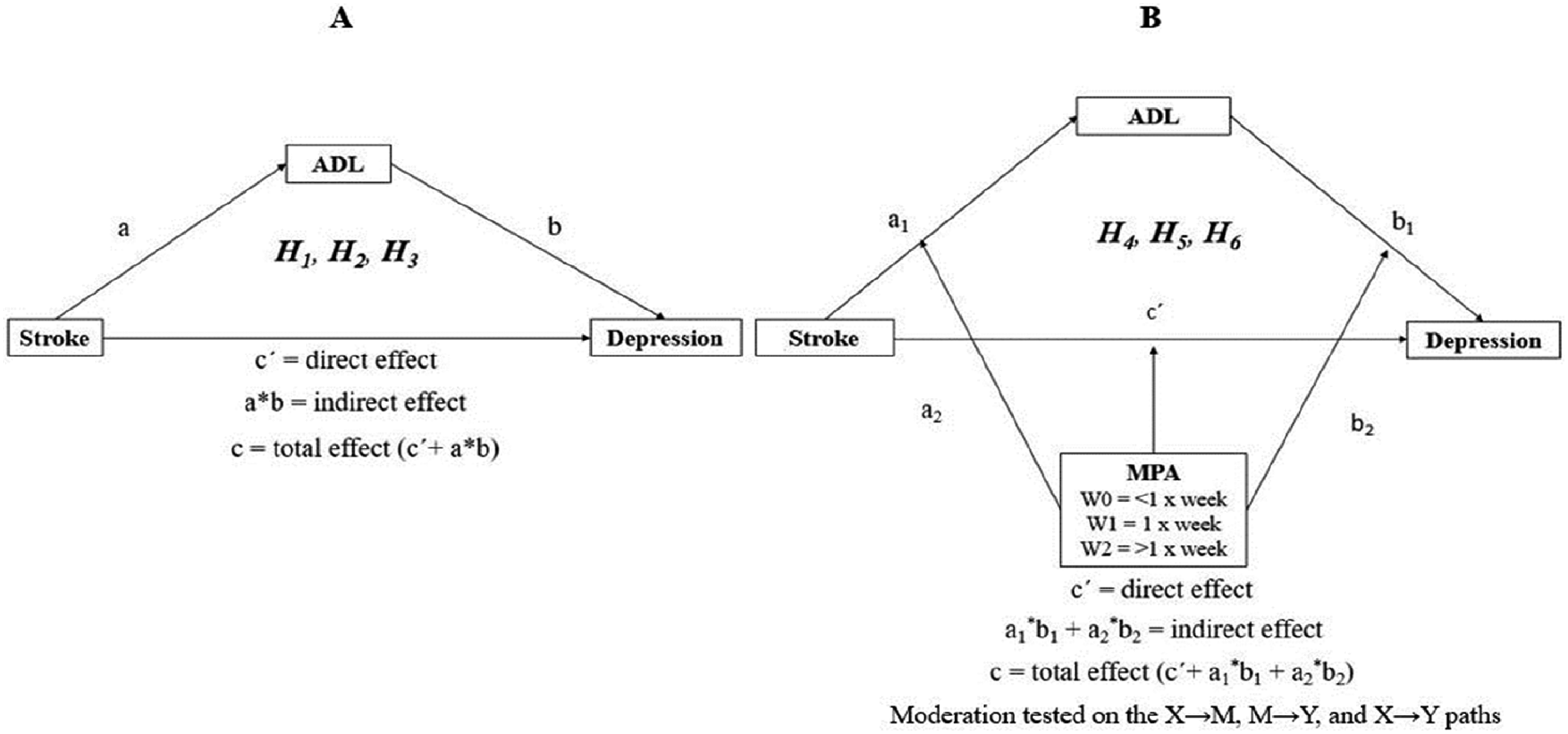
Results
Participant Characteristics
Main Characteristics of the Population Evaluated
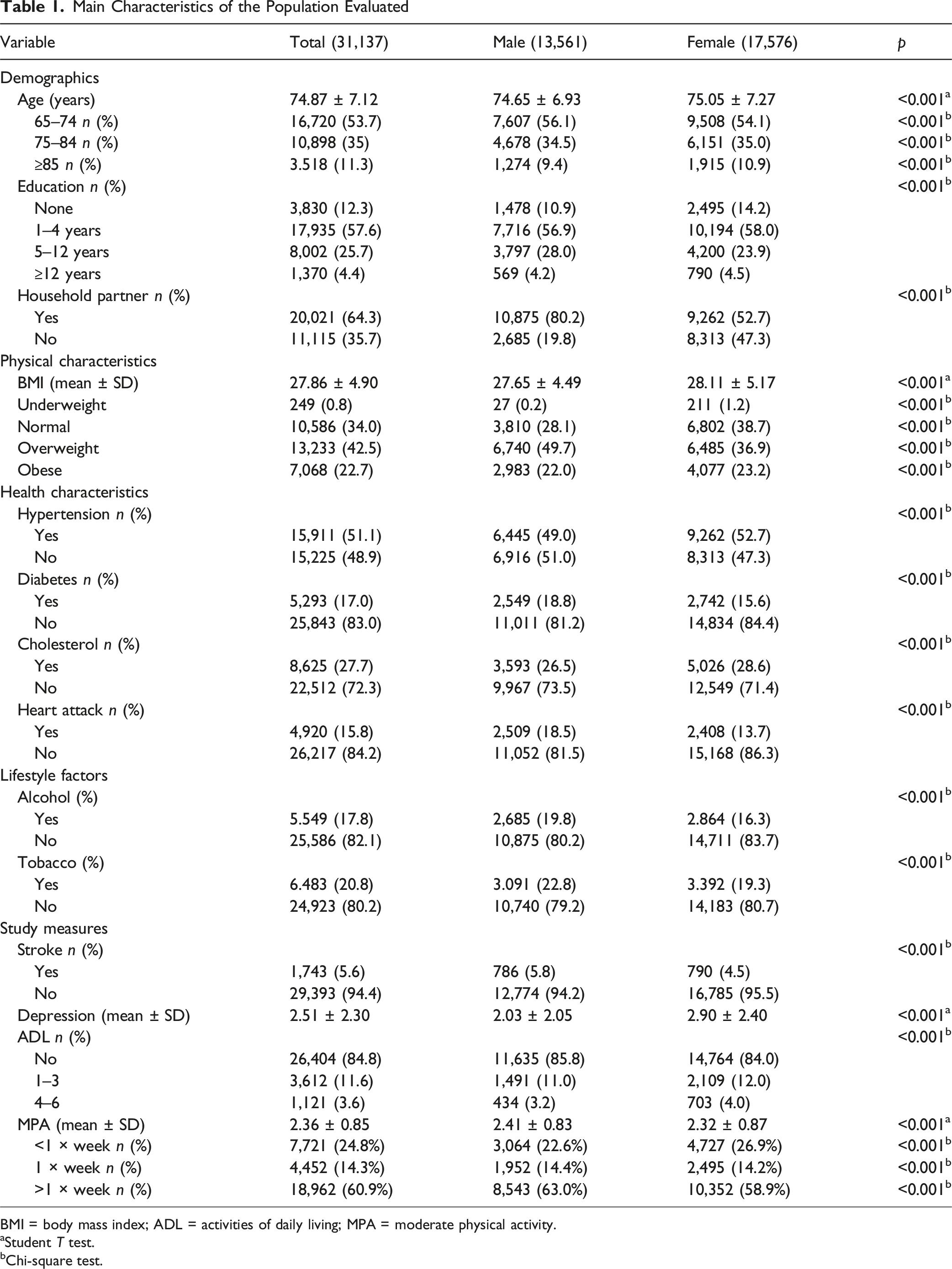
BMI = body mass index; ADL = activities of daily living; MPA = moderate physical activity.
aStudent T test.
bChi-square test.
Results of Intercorrelations Among Study Variables
Table S2 shows correlation analyses. Higher depression scores were associated with higher stroke incidence (r = 0.124, p < 0.001). A greater weekly MPA frequency was associated with lower stroke incidence (r = −0.105, p < 0.001). More ADL decreases were moderately associated with higher depression scores (r = 0.303, p < 0.001). Lower depression scores were associated with higher weekly MPA (r = −0.275, p < 0.001). Fewer ADL decreases were moderately associated with higher MPA frequency (r = −0.346, p < 0.001).
Testing for Mediation Effects
Associations for Males
Figure S1 presents the results of the mediation analysis for males. Stroke was significantly associated with a higher degree of ADL (β = 0.67, t = 21.494, p < 0.001). Similarly, a greater degree of ADLs impairments indicated a significant association with a higher depression score (β = 0.71, t = 36.018, p < 0.001). The overall impact of stroke on depression (total effect), without considering the mediating variable (ADL), was significant (β = 1.32, t = 17.40, p < 0.001). In turn, the direct effect estimated by the model (x → y) was also significant, indicating that stroke was associated with depressive symptoms among males (β = 0.84, t = 11.36, p < 0.001). This result supported the first hypothesis (stroke had a direct effect on depression). Furthermore, the indirect effect (transmitted by the mediator) was also significant (β = 0.48 (95% CI BCa = 0.4042–0.5677). The result suggested a partial association between the variables. Thus, our second hypothesis was also supported (ADL mediates the indirect effect between stroke and depression).
Associations for Females
Figure S2 presents the results of the mediation analysis for females. Stroke was significantly associated with a higher degree of ADL (β = 0.74, t = 21.34, p < 0.001). ADL was significantly associated with a higher level of depression (β = 0.69, t = 38.71, p < 0.001). The total effect, representing the full causal pathway between stroke and depression, was positive and significant (β = 1.40, t = 16.08, p < 0.001). The direct effect estimated by the model (x → y) indicated a positive and significant association, showing that stroke was linked to depressive events (β = 0.88, t = 10.39, p < 0.001). The result confirmed the first hypothesis among females (stroke had a direct effect on depression). The indirect effect, which ADL influenced, was significant (β = 0.52 (95% CI BCa = 0.4359–0.6147). Thus, our second hypothesis was also supported (ADL mediates the indirect effect between stroke and depression). Consequently, the results suggested a partial association between the variables.
Sex-Differentiated Comparison of Mediation Effects
To formally assess sex differences, indirect effects and mediated proportions were compared between males and females. The proportion of the total effect mediated by ADL was similar in males (36.53%) and females (37.19%), and the 95% bootstrap confidence intervals for the indirect effects overlapped, indicating no statistically significant sex difference in the overall mediation pathway (see Table S3). In contrast, sex-specific differences emerged in the moderated mediation models: among males, both medium and high weekly frequencies of moderate physical activity significantly attenuated the indirect effect of stroke on depression via ADL, whereas among females, only a high frequency of moderate physical activity (> once per week) produced a significant moderation effect. These findings support a sex-differentiated pattern in the conditional effects of physical activity, despite comparable baseline mediation structures.
Differential Patterns of Moderated Mediation for Males and Females
Males
Results of Moderation Analyses for Males and Females (W0 = MPA <1 × Week, Was Adopted as Reference)
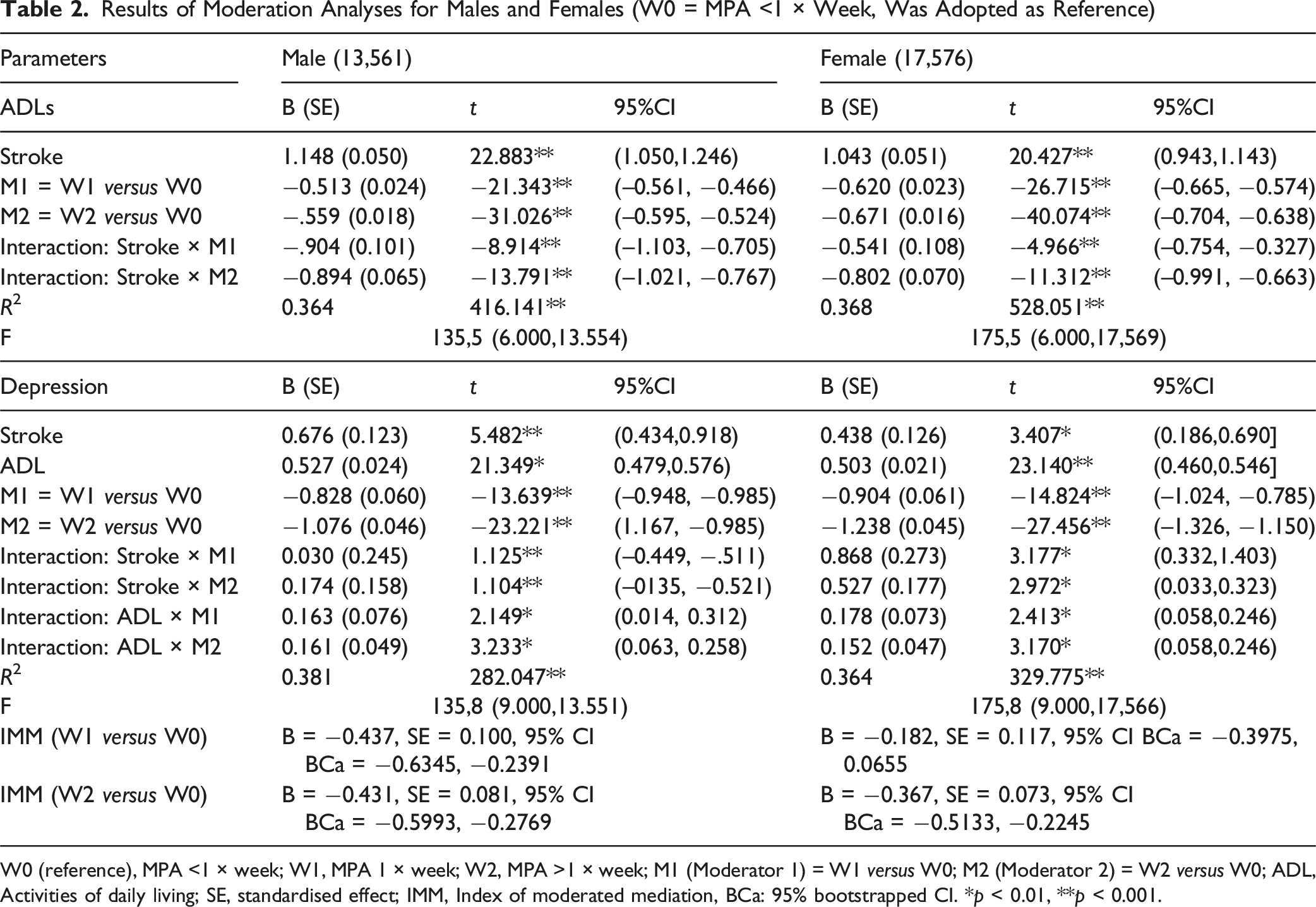
W0 (reference), MPA <1 × week; W1, MPA 1 × week; W2, MPA >1 × week; M1 (Moderator 1) = W1 versus W0; M2 (Moderator 2) = W2 versus W0; ADL, Activities of daily living; SE, standardised effect; IMM, Index of moderated mediation, BCa: 95% bootstrapped CI. *p < 0.01, **p < 0.001.
Females
Table 2 shows that stroke × MPA was negatively associated with ADL (p < 0.001): once/week (β = −0.541, p < 0.001), >1/week (β = −0.802, p < 0.001). Unlike males, only >1/week was strongly associated with lower ADL score. Stroke × MPA moderated stroke → depression (once/week: β = 0.868, p < 0.001; >1/week: β = 0.527, p < 0.001). ADL × MPA also moderated depression (once/week: β = 0.178, p < 0.001; >1/week: β = 0.152, p < 0.001). Thus, hypothesis 4 was supported. However, the moderation index showed that once/week was not significant (B = −0.1828, 95% CI [–0.3975, 0.0655]), whereas>1/week was significant (B = −0.3671, 95% CI [–0.5133, −0.2245]), supporting hypothesis 5 only for high MPA. Conditional indirect effects are in Table S4.
Results for Simple Slopes of the Categorical Moderator
Simple slope tests for males are shown in Figure 3(A). Comparatively, males who had a stroke reported higher depression scores. Furthermore, the lower the MPA weekly frequency in the sample, the greater the depression. The three moderators were significant and indicated an association between stroke and depression: −1 SD [MPA <1 × per week (B = 0.676, SE = 0.123, t = 5.48, p < 0.001)], medium [MPA 1 × per week (B = 0.707, SE = 0.084, t = 12.47, p < 0.001)], and +1 SD [MPA >1 × per week (B = 0.851, SE = 0.068, t = 18.04, p < 0.001)]. Thus, among males, the higher the MPA weekly frequency, the lower the depression score in post-stroke. In turn, the three moderators also indicated a significant association between stroke and ADL (Figure 3B): −1 SD [MPA <1 × per week (B = 1.148, SE = 0.050, t = 22.88, p < 0.001)], medium [MPA 1 × per week (B = 0.24, SE = 0.038, t = 2.76, p = 0.005)], and +1 SD [MPA >1 × per week (B = 0.23, SE = 0.029, t = 6.16, p < 0.001)]. The images suggested that medium and high weekly frequency of MPA had a similar association on reducing ADLs, being significant moderators for reducing depression in males with post-stroke. Slope analysis of the moderating role of MPA in the relationship between stroke and depression mediated by activities of daily living, according to sex.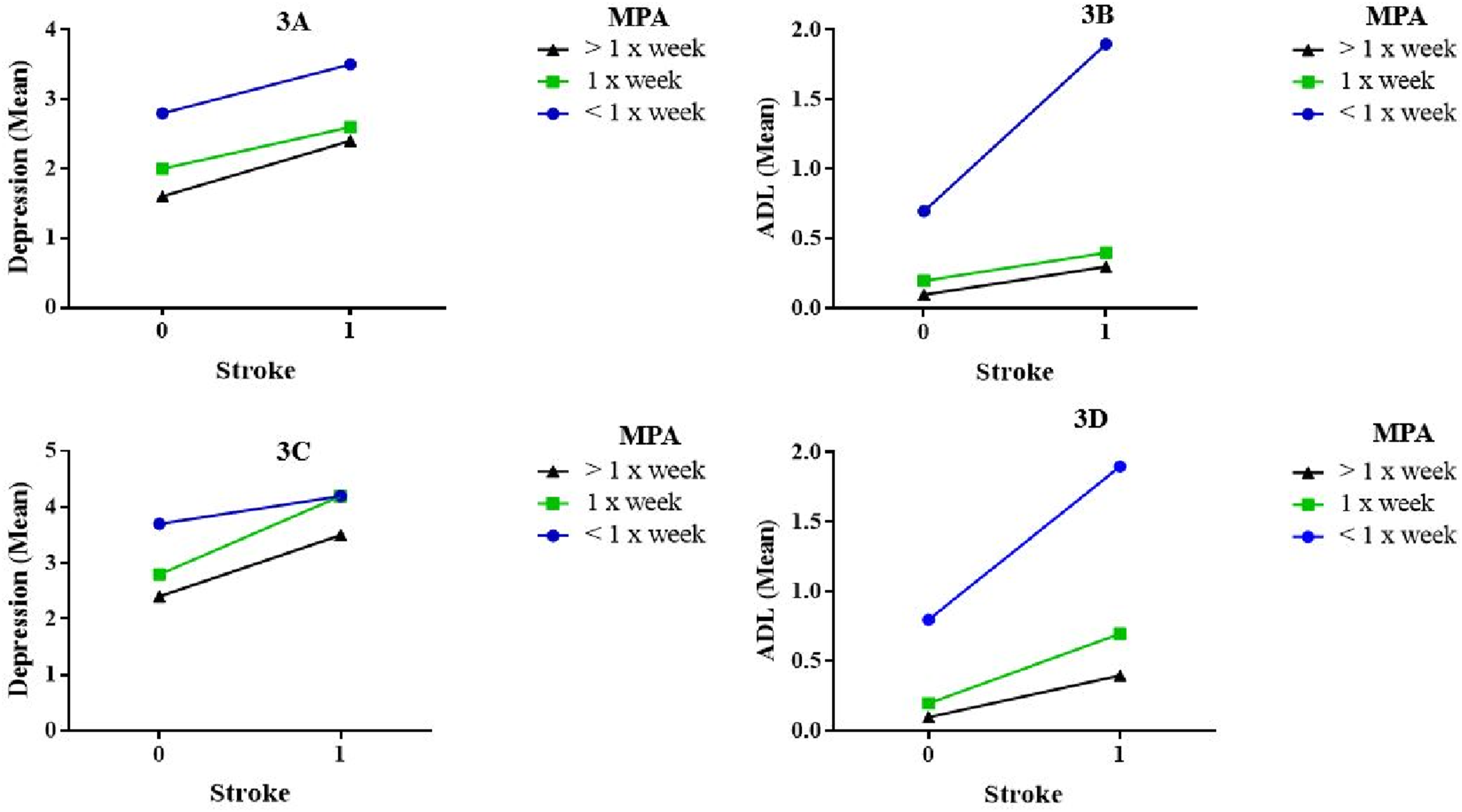
Among females, higher depression symptoms were reported by those with post-stroke and low MPA scores. All three moderators were significantly associated with depression and were differentiated by their effects: −1 SD [MPA <1 × per week (B = 0.438, SE = 0.126, t = 3.40, p < 0.001)], medium [MPA 1 × per week (B = 1.30, SE = 0.142, t = 5.41, p < 0.001)], and +1 SD [MPA >1 × per week (B = 0.96, SE = 0.058, t = 7.89, p < 0.001)]. Participants classified with MPA weekly frequency −1 SD and medium revealed similar depression scores (Figure 3(C)). The finding corroborated the analysis of the moderation index, which did not find M1 (MPA 1 × per week versus MPA <1 × per week) to be significant. This result also indicates that, in contrast to males, females with post-stroke conditions require MPA at a frequency of more than once per week to mitigate symptoms of depression. Furthermore, there was an inverse relationship between MPA frequency and ADL scores: higher weekly MPA frequencies were associated with lower ADL scores (Figure 3(D)). The moderators pointed out significant results: −1 SD [MPA <1 × per week (B = 1.04, SE = 0.094, t = 20.42, p < 0.001)], medium [MPA 1 × per week (B = 0.50, SE = 0.026, t = 5.21, p < 0.001)], and +1 SD [MPA >1 × per week (B = 0.24, SE = 0.012, t = 4.90, p < 0.001)].
Discussion
This cross-sectional study provided, differentiated by male and female, an understanding of the mediating role of ADL in the relationship between stroke and depression among older adults from 27 European countries, as well as the moderating effect of three weekly frequencies of MPA in this mediation.
The study hypotheses were grounded in established functional and biopsychosocial models of post-stroke depression, which posit that functional impairment and loss of autonomy in activities of daily living constitute key pathways linking stroke to depressive symptoms. From this perspective, ADL limitations were hypothesised to mediate the association between stroke and depression (H2), while physical activity was expected to act as a buffering factor by preserving functional capacity, psychological resilience and social participation. Furthermore, prior evidence of sex differences in stroke outcomes, physical functioning and physical activity patterns provided the theoretical basis for hypothesising sex-differentiated mediation and moderation effects (H3–H6).
The findings are consistent with previous research on the association between stroke and depression (Blake et al., 2024; Guo et al., 2022; Robinson & Jorge, 2016). In turn, the combination of stroke and depression exacerbates the inability of older adults to perform ADLs (Li et al., 2023; Sara et al., 2024). Although the overall mediation of the stroke–depression association by ADL did not differ significantly between males and females, the moderated mediation analyses revealed clear sex-specific patterns. In particular, males appeared to benefit from both moderate and high frequencies of physical activity. In contrast, females required higher levels of activity to achieve comparable protective effects. These findings justify the use of the term ‘sex-differentiated analysis’ and highlight the importance of considering sex when translating physical activity recommendations into post-stroke clinical practice.
Consistent with the theoretical assumptions underlying H1 and H2, our findings were in agreement with previous studies indicating that stroke and post-stroke depression are prevalent in females (Ospel et al., 2023; Zhao et al., 2020). However, regarding the mediating role of ADL in the relationship between stroke and PSD, females and males did not differ significantly. A possible explanation is that, in the examined population, factors underlying ADLs in each sex may have influenced PSD in a proportional manner. The present findings should be interpreted in light of the cross-sectional design. Although stroke history reflects a prior medical diagnosis, depressive symptoms, activities of daily living, and moderate physical activity were assessed contemporaneously. Therefore, the temporal ordering between these variables cannot be definitively established, and bidirectional relationships, particularly between physical activity and depressive symptoms, cannot be excluded.
Moderate mediation revealed that, for male, moderate physical activity (once a week) and high physical activity (more than once a week) were significant for the association between stroke and activities of daily living. Whereas for females, only a high frequency of MPA (> once a week) was identified as a better moderator. After the inclusion of ADLs, for both sexes, the direct effect of stroke on depression remained significant, indicating partial mediation. PSD arises from a combination of factors associated with decreased ADLs, such as restrictions on participation in social activities and changes in cognitive function (Robinson & Jorge, 2016; Ytterberg et al., 2022). Moreover, depending on the severity of the stroke, brain tissue can suffer severe damage. Thus, thrombotic, embolic or haemorrhagic events can affect cognitive performance, causing physical disabilities (De Meyer et al., 2016), such as difficulty walking and loss of fine motor skills (Bustamante et al., 2016). Furthermore, post-stroke symptoms include fatigue and social withdrawal (Thilarajah et al., 2018), which can contribute to feelings of loneliness (Blake et al., 2024), enhancing depressive symptoms such as anxiety, sadness, mood disorders, and apathy (Medeiros et al., 2020).
The total and indirect effects of the moderated mediation analyses indicated MPA as a significant moderator for both sexes. This finding is relevant because global guidelines for physical exercise in post-stroke patients lack detailed guidance on physical activity measures (Church et al., 2022). At the same time, although PA intensity is known to be beneficial for post-stroke rehabilitation, it remains an underutilised biomarker in this context (Addoh et al., 2025). An interesting finding among males was that a weekly frequency of physical activity of once a week or more was sufficient to reduce the degree of impairment in ADLs.
On the other hand, among females, a frequency of MPA greater than once a week was necessary to neutralise the negative impact of sedentary behaviour on ADLS. This may be because males reported lower ADL scores than females. The results were consistent with previous studies that highlighted the inability of post-stroke patients to perform ADLs due to sedentary behaviour and the severity of physical disabilities (Church et al., 2022; Gil-Salcedo et al., 2022).
These sex-specific patterns are theoretically consistent with evidence on sex differences in baseline functional reserve, physiological responses to physical activity, and social roles across the life course. This may reflect sex differences in baseline functional status, physiological reserve, hormonal and inflammatory profiles, and social roles in adulthood. Conversely, males may obtain functional and psychological benefits with lower activity thresholds. Although these differences were not tested using formal sex-moderated physical activity interaction terms in a pooled model, they were consistently observed in sex-stratified analyses and in comparisons of conditional effects, supporting a differentiated interpretation by sex.
Among the possible strategies to increase PA levels post-stroke are motivation to become more active, emphasis on lifestyle changes, and structured exercise programs (Pasztor et al., 2025). Those responsible for the rehabilitation of stroke survivors must focus on improving physical activity levels, especially in the dose-response relationship, to enhance cardiorespiratory fitness. Consequently, neuroplasticity will be benefited, particularly in the early post-stroke stages (Kramer et al., 2019). In this case, structured exercise programs may be more effective because they can tailor exercise intensity to the patient’s needs (Billinger, Arena, Bernhardt, Eng, Franklin, Johnson et al., 2014). Issues such as intensity, frequency, recovery, and ideal modality for post-stroke training still require further exploration (Addoh et al., 2025). Thus, the present study has shed light on important information for the field of stroke survivor rehabilitation.
Strengths, Limitations and Future Direction
To our knowledge, this is the first study that tested the moderating role of MPA in mediating ADL in the relationship between stroke and depression in individuals aged ≥65 years using data from the 2019 SHARE survey, bringing to light sex-differentiated information. Among the strengths of this study are the large number of participants from 27 European countries and information that can complement the understanding of the potential mechanism underlying PSD. This aspect is important for triggering clinical reasoning and outlining planning rehabilitation measures through MPA. Physical activity and exercise are simple, low-cost strategies that can simultaneously benefit different areas of health. Our findings can serve as a basis for the development of clinical studies with stroke survivors, as previous research has reported gaps in the assessment and treatment of strokes (Ospel et al., 2023). On the other hand, the study has limitations: First, the cross-sectional design does not allow establishing causal relationships; that is, life events other than stroke and ADL may have contributed to the establishment of depression symptoms. Furthermore, the results cannot be generalised to countries not included in the analyses. Secondly, the analyses were not controlled for covariates affecting stroke survivors, which are associated with a higher risk of depressive symptoms and disability in activities of daily living, such as sedentary habits, cognitive performance, social isolation, chronic pain, as well as the severity of the stroke itself. Therefore, this may introduce bias in the interpretation of the results. Thirdly, because of the use of complete case analysis, 1,051 participants with missing data were excluded from the analyses. Excluded individuals tended to be older and to present poorer health and functional profiles, suggesting that missingness was not completely at random. This may have introduced selection bias, generating conservative estimates of the observed associations. Future studies using longitudinal data and multiple imputation techniques are warranted to address this limitation. Fourth, self-reported information may have introduced bias into the results. Another point to consider is that respondents tend to overestimate the weekly frequency of physical activity compared to measurements collected by specific devices (Gorzelitz et al., 2018). Fifth, it was not possible to know the temporal relationship between depression and stroke. Thus, it is possible that the stroke occurred before the interview (2019), while the information on depression and ADL disability referred to the period of 2019. Sixth, although the EURO-D scale has been widely used in cross-national SHARE analyses (Prince et al., 1999), full measurement invariance across all participating countries has not been formally established. Therefore, some degree of measurement heterogeneity cannot be excluded, although adjustment for country and the use of EURO-D as a continuous outcome mitigate this concern. Seventh, factors such as polypharmacy, as well as the social, political, economic, and cultural diversity of the 27 countries analysed, could not be controlled. Eighth, our data were collected before the pandemic. The eighth wave of SHARE began in October 2019 and was interrupted in all participating countries due to the outbreak of the COVID-19 pandemic in March 2020. Thus, it is possible that after COVID-19, both the incidence of stroke and PSD, as well as patterns of physical activity and general health habits may have changed. In this perspective, future studies could compare our findings with current data from the ninth wave of the SHARE survey/post-pandemic. Nine, due to the cross-sectional nature of the data, it is not possible to infer causal relationships. Although the history of stroke precedes the assessment of depressive symptoms and limitations in activities of daily living, the temporal dynamics between these variables remain uncertain and bidirectional associations cannot be ruled out. Tenth, because depression, limitations in activities of daily living, and physical activity were assessed simultaneously, the observed associations may reflect reciprocal or bidirectional relationships, which cannot be separated in a cross-sectional study.
We suggest that future studies invest in combining devices (measuring energy expenditure) and questionnaires (Fini et al., 2023). Second, studies could stratify participants by age group, initial sedentary time, and stroke-specific factors (e.g. cardiovascular disease, years of education, genetics, residence, family support, income, health insurance, and lifestyle). Finally, it would be useful to focus on ideal levels of physical activity (i.e. weekly frequency, time per session, intensity, type of activity), and always consider monitoring by a specialist physician to avoid under- or over-dosing of physical effort (Billinger, Arena, Bernhardt, Eng, Franklin, Johnson, MacKay-Lyons et al., 2014).
Conclusion
In this large European sample of older adults, stroke history was associated with higher depressive symptomatology and greater limitations in activities of daily living. Higher frequencies of moderate physical activity were associated with weaker associations between stroke history, functional limitations, and depressive symptoms, with distinct patterns observed between males and females. Although causal inferences are not possible due to the cross-sectional design, these findings highlight the potential relevance of physical activity as a correlational marker of better functional and mental health profiles in post-stroke populations.
Supplemental Material
Supplemental Material - Post-Stroke Depression and Activities of Daily Living: Sex-Differentiated Analysis of the Moderating Role of Physical Activity in Older European Adults
Supplemental Material for Post-Stroke Depression and Activities of Daily Living: Sex-Differentiated Analysis of the Moderating Role of Physical Activity in Older European Adults by Marcelo de Maio Nascimento, Andreas Ihle, Miguel Peralta, Gerson Ferrari, Élvio R. Gouveia and Adilson Marques in Journal of Aging and Health
Footnotes
Acknowledgements
This paper uses data from SHARE (DOIs: 10.6103/SHARE.w7.700, 10.6103/SHARE.w8.100); see Börsch-Supan et al. (2013) for methodological details. The SHARE data collection has been primarily funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT2005-028857, SHARELIFE: CIT4-CT-2006-028812) and FP7 (SHARE-PREP: N°211909, SHARE-LEAP: N°227822, SHARE M4: N°261982). Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071 C) and from various national funding sources is gratefully acknowledged (see ![]() ).
).
Ethical Considerations
All participants gave informed consent before being interviewed. The procedures that ensured the confidentiality and data privacy of the SHARE protocol survey were reviewed and approved by the Ethics Committee of the University of Mannheim and by the Ethics Council of the Max-Planck-Society for the Advancement of Science. All survey procedures were carried out following the ethical guidelines and regulations of the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.