
Abstract
Objectives
We examined longitudinal associations between young adult heavy substance use and late midlife poor self-rated memory and whether problematic substance use in early midlife mediated the associations.
Methods
Data were from the Monitoring the Future Longitudinal Panel Study. Analyses included individuals ages 50–65 in 2018–2023 who provided longitudinal data starting at age 18 in 1976–1991.
Results
Young adult heavy use of all substances was directly associated with higher odds of late midlife poor self-rated memory. These associations were fully mediated by early midlife substance-use disorder symptoms for binge drinking and cannabis use, but not mediated for pack+/day cigarette smoking.
Discussion
Sustained heavy substance use in young adulthood appears to represent a cumulative risk factor for cognitive decline in late midlife. Examining risk factors, including substance use, across the life course may be crucial for earlier identification of risk for cognitive decline.
Introduction
Cognitive changes are frequently observed as part of the typical aging process (Brito et al., 2023; Murman, 2015). Some individuals develop dementia; estimates place the lifetime risk of dementia after age 55 at 42% (Fang et al., 2025), and increasing age is a strong risk factor for the severe cognitive impairment that results from Alzheimer’s disease and related dementias (ADRD). In 2025, more than seven million individuals, most of them ages 65 or older, were estimated to have ADRD in the United States, and the number is expected to increase in the future (Alzheimer’s Association, 2025). Early identification of dementia is crucial to manage and slow progression of the disease (Li et al., 2023; Rasmussen & Langerman, 2019). Memory problems have been found to be among the common early signs of dementia (Alzheimer’s Association, 2025; National Institute on Aging, 2023) in both U.S. and international research. For example, a multi-state study in the U.S. found individuals assessed as having low cognition scores (i.e., having scores in the lowest quartile on cognitive tests evaluating verbal learning and memory, processing, executive, and language functions) at ages 48–67 had a higher risk of developing mild cognitive impairment and dementia 20–25 years later, controlling for a range of other midlife health measures including hypertension, cholesterol level, diabetes, BMI, and total cigarette-years smoked at baseline (Knopman et al., 2018). A population-based study in a Swedish principality found self-reported memory at baseline (mean age in the 70s) predicted dementia or ADRD 10–12 years later independent of objective memory scores and depressive symptoms (Rönnlund et al., 2015). Further, in a case–control population-based study in France following adults ages 65+ for 14 years, those who developed Alzheimer’s disease reported increasing cognitive complaints over time, compared to no increases among those who did not develop the disease (Amieva et al., 2008). Understanding risk factors associated with poor memory during midlife may be crucial for preventing, identifying, and managing dementia.
Substance use may pose such risks. Smoking and alcohol use are known modifiable and preventable risk factors for cognitive impairment (Livingston et al., 2024). Alcohol, cannabis, and cigarette use have been shown to be strongly associated with decreased functioning in various cognitive domains, including memory (Broyd et al., 2016; Livingston et al., 2024; Mulhauser et al., 2023). The severity of such associations is dependent to various degrees on use frequency and duration, with higher use frequency and longer use duration shown to be strong risk factors for cognition and memory impairment, in particular. Use of alcohol at levels causing impairment has been found to impair memory processes (Van Skike et al., 2019), and sustained heavy or excessive consumption is associated with higher risk for cognitive dysfunction and dementia (Kim et al., 2012; Livingston et al., 2024; Oslin et al., 1998; Zhang et al., 2020). For cannabis, higher use frequency has been negatively associated with working or short-term memory (Maynard et al., 2023; Stypulkowski & Thayer, 2022); the strongest negative impacts of cannabis on memory have been found for chronic exposure, with some effects continuing to be observed after use cessation (Broyd et al., 2016). Dementia risks associated with cigarette use are stronger for those who start smoking in early versus later midlife (Livingston et al., 2024). Trajectories of rapid cognitive decline are highest for current smokers (Li et al., 2025). While cessation reduces risk, former smokers have higher odds of rapid cognitive decline than nonsmokers (Li et al., 2025). However, available research has not examined the extent to which sustained high-frequency alcohol, cannabis, or cigarette use during young adulthood may be associated with late midlife memory impairment. Specifically, it is unclear whether heavy substance use in young adulthood acts as an independent direct risk factor for both early midlife problematic use and late midlife poor memory, or if early midlife problematic substance use mediates the risks associated with young adult substance use. If the former, then young adult substance use may be critical in posing long-term risks for cognitive health across the lifespan and requires intervention in young adulthood. If the latter, young adult behavior may pose long-term risks for cognition only to the extent to which it is associated with continued heavy substance use into midlife, which suggests midlife interventions may have potential to mitigate the risks.
An extensive research literature has found higher risk of early aging and cognitive impairment among those with substance-use disorder (e.g., Bachi et al., 2017; Bruijnen et al., 2019; Cadet et al., 2014; Manning et al., 2016; Oscar-Berman & Marinković, 2007). Substance-use disorders, particularly at the severe end of the symptom spectrum, are known to affect brain circuits that regulate memory and other cognitive domains (Cadet et al., 2014). For example, both alcohol and cannabis-use disorders have been found to be associated with functional and structural changes in regions of the brain including the frontal lobes and hippocampus, which are both key areas for memory (Oscar-Berman & Marinković, 2007; Yücel et al., 2008). Findings related to cigarette use are more complex. Nicotine is associated with enhanced working and episodic memory (Valentine & Sofuoglu, 2018); research indicates that individuals with lower cognitive skills may be at higher risk for addiction due to nicotine’s cognitive-enhancing effects (Valentine & Sofuoglu, 2018). However, nicotine’s association with memory may be curvilinear, such that small doses lead to improved memory, while chronic heavy use leads to increased impairment as well as addiction. Data from the longitudinal population-based Dunedin Study in New Zealand have indicated that increasing waves with a cannabis dependence diagnosis across young adulthood and early midlife (ages 18, 21, 26, 32, 38, and 45) are associated with stronger within-person declines in IQ during early midlife (age 38 and 45) including memory-specific domains (Meier et al., 2012, 2022); associations are robust to adjustment for dependence on alcohol and tobacco (Meier et al., 2022). Dunedin Study data have also shown that negative impacts on various brain structures at age 45 exhibit dose–response associations with the number of young adult/early midlife waves (including age 45) with a dependence diagnosis for cannabis, tobacco, or alcohol (separately), but most of these structural differences are explained by polysubstance use (Knodt et al., 2022). The current study extends further into the life course to examine outcomes in late midlife (ages 50–65).
Young adult substance use may primarily act as a risk factor for early midlife problematic use (Patrick et al., 2020, 2021, 2023, 2024b; Jang et al., 2018; Schulenberg et al., 2016), which then may act as the primary risk factor for late midlife memory problems. That is, early midlife problematic use may fully mediate any observed associations between young adult use and late midlife memory. Alternatively, heavy and sustained substance use during young adulthood may act as an independent risk factor for both early midlife problematic use and late midlife poor memory, with only partial or no mediation through early midlife problematic use; for example, heavy, sustained substance use may affect ongoing brain development in young adulthood (Lebel & Beaulieu, 2011).
Research on substance use and cognitive impairment includes both clinical and subjective measures of cognitive function. Individuals who report subjective cognitive complaints of impairment, including with subjective memory (e.g., measured by respondent-reported difficulty to concentrate, remember, or make a decision due to physical, mental, or emotional conditions; Mulhauser et al., 2023), have increased risks of progressing to cognitive impairment and dementia than individuals with only objective complaints (Mendonça et al., 2016; Mitchell et al., 2014; Rönnlund et al., 2015). While some longitudinal research has not found strong connections between subjective and objective measures of cognitive decline (Gustavson et al., 2021; Topiwala et al., 2021), other studies find that subjective measures significantly predict later objective cognitive decline (Ferraro et al., 2023; Jessen et al., 2014; Jorm et al., 2001; Pai et al., 2023). Furthermore, as noted above, self-reported memory was associated with developing dementia of Alzheimer’s disease 10–12 years later, even after controlling for objective memory scores (Rönnlund et al., 2015). Use of subjective memory measures may be particularly informative when examining how sustained high-frequency alcohol, cannabis, or cigarette use during young adulthood may be associated with memory impairment among national samples of late midlife respondents.
The current study examined the following two research questions (RQs): (1) whether heavy substance use (alcohol, binge drinking, cannabis, and cigarettes) during young adulthood (at ages 18–30) was associated with poor self-rated memory in late midlife (ages 50–65) and (2) to what extent problematic substance use in early midlife (at age 35)—including alcohol-use disorder, cannabis-use disorder, and pack+/day cigarette smoking—mediated associations between young adult heavy substance use and late midlife poor self-rated memory.
Method
Data and Procedures
The current study used data from the Monitoring the Future (MTF) Longitudinal Panel Study. Every year since 1976, MTF has surveyed a new nationally representative sample of U.S. 12th grade students (at modal age 18; Miech et al., 2024). Approximately 2,450 individuals have been selected from each 12th grade cohort for the MTF Longitudinal Panel Study since 1976 (Patrick et al., 2024). In the MTF Longitudinal Panel Study, participants are randomly assigned to even or odd years for six biennial young adult surveys (ages 19/20, 21/22, 23/24, 25/26, 27/28, and 29/30); participants complete midlife surveys every 5 years starting at age 35 (Patrick et al., 2024). See Supplemental Table 1 for additional detail on years of data collection by 12th grade cohort.
The analytic sample for the current study included respondents sampled for the MTF Longitudinal Panel Study from the 1976–1991 12th grade cohorts (n = 38,918) who participated in the later midlife follow-up surveys (ages 50, 55, 60, or 65) in 2018–2023. Among these respondents, mean response rates among active participants averaged 79.6% across ages 50 to 65, leaving 16,620 respondents (42.7% of the possible 38,918) and providing 19,357 cases of data for the final analytic sample (respondents could have 1–2 waves of data collection depending on cohort; see Supplemental Table 1). Of these, 51.3% identified as female and 48.7% as male. For race/ethnicity, 4.6% identified as Hispanic, 78.0% non-Hispanic White, 11.8% non-Hispanic Black, 1.7% non-Hispanic Asian, and 3.9% another race/ethnicity.
Measures
Poor Self-Rated Memory in Late Midlife (at Ages 50–65)
Beginning in 2018, midlife surveys asked respondents, “Would you say your memory is…excellent, very good, good, fair, or poor?” (where 5 = excellent and 1 = poor). Responses were dichotomized to indicate poor self-rated memory, where 1 = poor/fair and 0 = excellent/very good/good.
Heavy Substance Use in Young Adulthood (at Ages 18–30)
At age 18 (12th grade) and each of the six young adult surveys (ages 19/20 to 29/30), respondents reported substance use via consistent measures over time; coded measures focused on identifying heavy use (defined as noted). Past 30-day alcohol use (number of occasions having any alcoholic beverage to drink—more than just a few sips) and cannabis use (number of occasions using marijuana or hashish) at each wave were dichotomized as 20+ occasions (indicating daily or near-daily use; Patrick, 2025; Patrick et al., 2024) versus fewer (0–19 occasions). Past 2-week binge drinking (number of times having five or more drinks in a row) was dichotomized as any past 2-week binge drinking versus none (National Institute on Alcohol Abuse and Alcoholism, 2025; Patrick et al., 2024). Past 30-day cigarette use (how frequently smoked cigarettes) was dichotomized as daily use (1+ cigarettes/day) versus less than daily (none or <1) (Inoue-Choi et al., 2019; Patrick et al., 2024). For each of alcohol, cannabis, binge drinking, and cigarettes, cases providing valid data on at least five of the seven possible waves were identified. If five or more waves of valid data were present, cumulative young adult substance use was coded based on the number of waves where respondents reported heavy use, with sums ranging from 0 to 5 (5+ waves).
Problematic Substance Use in Early Midlife (at Age 35)
Problematic substance use measures in early midlife (at age 35) included alcohol use disorder (AUD), cannabis use disorder (CUD), and a trichotomous 30-day cigarette use measure focused on pack+/day smoking. Respondents were asked whether they had used any alcohol or cannabis in the past 5 years. If yes, they were asked, “Think back over the last five years. Did your use of [alcohol, cannabis] cause you any of the following problems?” Respondents were then shown substance-specific symptom indicators addressing 8 1 of the 11 diagnostic criteria set by the American Psychiatric Association (APA) (2022) separately for AUD and CUD. The number of substance-specific criterion for which respondents reported symptoms were summed to create indicators of AUD and CUD following APA recommended cut-offs (American Psychiatric Association, 2022). The AUD and CUD measures were coded as 0 = no use of the specified substance in the past 5 years (hereafter referred to as “abstention”), 1 = non-disordered use (meeting 0–1 criteria), or 2 = disordered use symptoms (meeting 2+ criteria). These measures are not equivalent to a clinical diagnosis but are used to indicate possible use disorder (see Terry-McElrath & Patrick, 2025).
Since MTF surveys do not include items related to tobacco use disorder, the early midlife measure for tobacco focused on cigarette use. Respondents were asked how frequently they smoked cigarettes during the past 30 days (using the same wording and response options as the cigarette use item in young adulthood). For the early midlife problematic cigarette use measure, responses were recoded into three categories: no 30-day cigarette use (hereafter also referred to as “abstention”), smoking less than a pack/day, or smoking pack+/day.
Covariates
Covariates measured at age 18 included sex (male, female); race/ethnicity (coded for analysis as Hispanic, non-Hispanic Asian, non-Hispanic Black, non-Hispanic White, or other); and average high school grades (coded as C+ or lower vs. B- or higher). Highest degree was based on reports at age 35 (no college degree vs. bachelor’s degree or higher). In addition, age (coded as a linear term from 50 to 65) and year (2018–2023) when the outcome of self-reported memory was assessed were also included.
Analytical Approach
All analyses used MTF Longitudinal Panel analysis weights to account for sample selection and attrition (Patrick et al., 2022). SAS v.9.4 (SAS Institute Inc., Cary, NC) survey commands (PROC SURVEYFREQ and PROC SURVEYMEANS) were used to obtain descriptive statistics accounting for clustering (i.e., repeated measures) by respondents. Mediation analyses were conducted using Mplus v.8.8 (Muthén & Muthén, 1998-2022), using the MLR estimator with Monte Carlo integration, clustered at the respondent level (TYPE = COMPLEX). Missing data on all variables were addressed by using full information maximum likelihood (FIML; Arbuckle et al., 1996; Enders, 2001), specifically requesting that models estimate the variance for all variables with missing data. Indirect effects were computed using the product-of-coefficients method (Muthén, 2011; Terry-McElrath et al., 2015).
Analyses were conducted separately by young adult substance use predictor (alcohol, binge drinking, cannabis, cigarettes); all parameters of interest are depicted in Figure 1. In all models, X indicates heavy substance use in young adulthood, M indicates problematic substance use in early midlife, and Y indicates poor self-rated memory in late midlife. The referent categories for age 35 problematic substance use were non-disordered use (alcohol and cannabis) and smoking <pack/day (cigarettes). Hypothesized associations between young adult heavy substance use, early midlife problematic use, and late midlife poor self-rated memory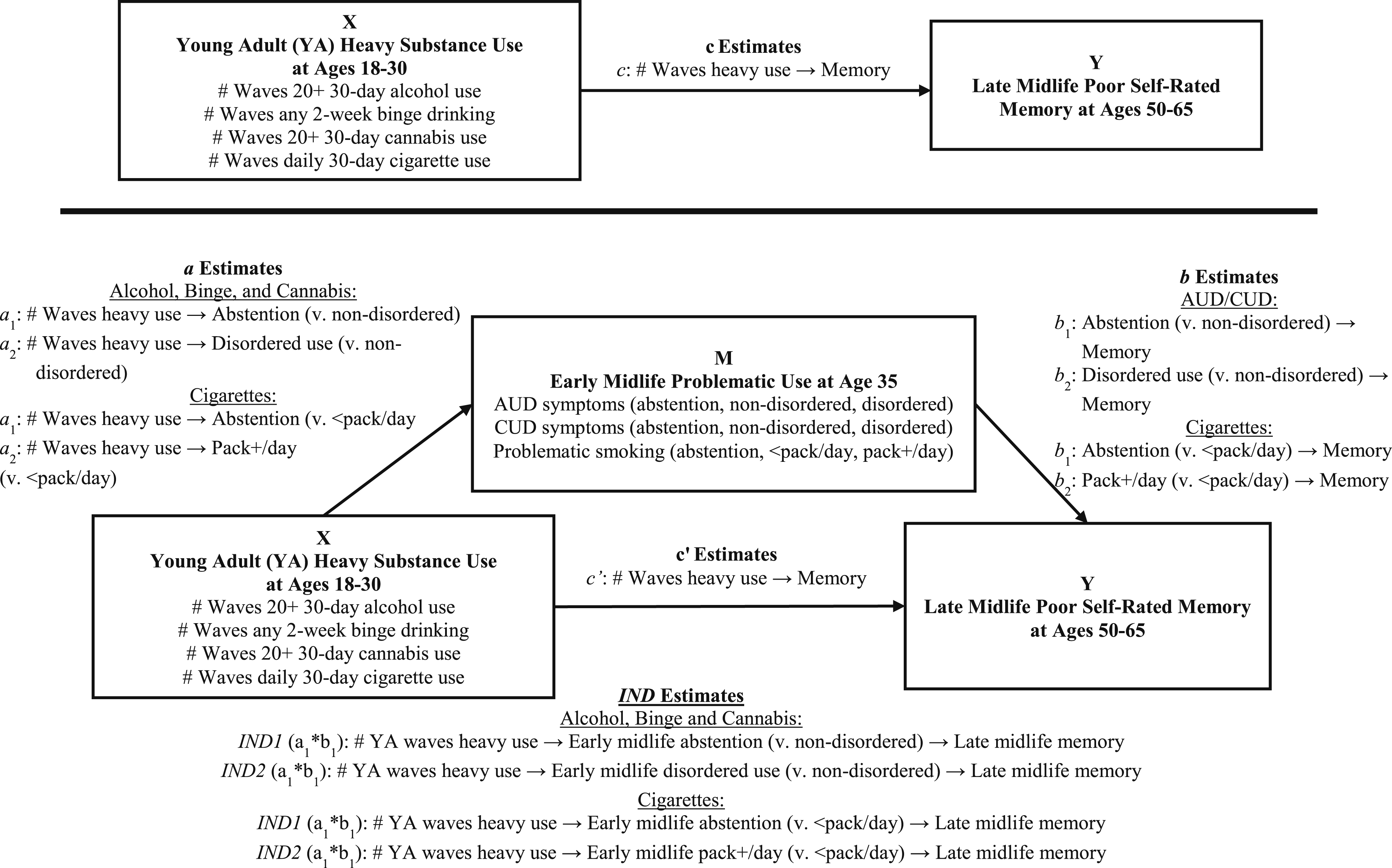
Analyses proceeded in two steps (see Figure 1). First, associations between young adult heavy substance use and poor self-rated memory in late midlife were estimated with: • parameter c estimates from bivariate and multivariable logistic regression of late midlife poor self-rated memory (X) on young adult heavy substance use (Y) (multivariable models controlling for sex, race/ethnicity, average high school grades, college degree, age, and year of outcome data collection).
Second, bivariate and multivariable mediation models were fit with: • parameter a estimates from multinomial logistic regression (using non-disordered use as the referent category) of early midlife problematic substance use (M) on young adult heavy substance use (X) (multivariable models controlling for sex, race/ethnicity, average high school grades, and college degree); • parameter b and c’ estimates from logistic regression of late midlife poor self-rated memory (Y) on early midlife problematic substance use (M) and young adult heavy substance use (X) (multivariable models controlling for sex, race/ethnicity, average high school grades, college degree, age, and year of midlife data collection); and ⁃ indirect (IND) parameter estimates (two per model): ⁃ IND1: young adult heavy substance use ⁃ IND2: young adult heavy substance use
Results
Sample Characteristics
Overall Analytic Sample Descriptives
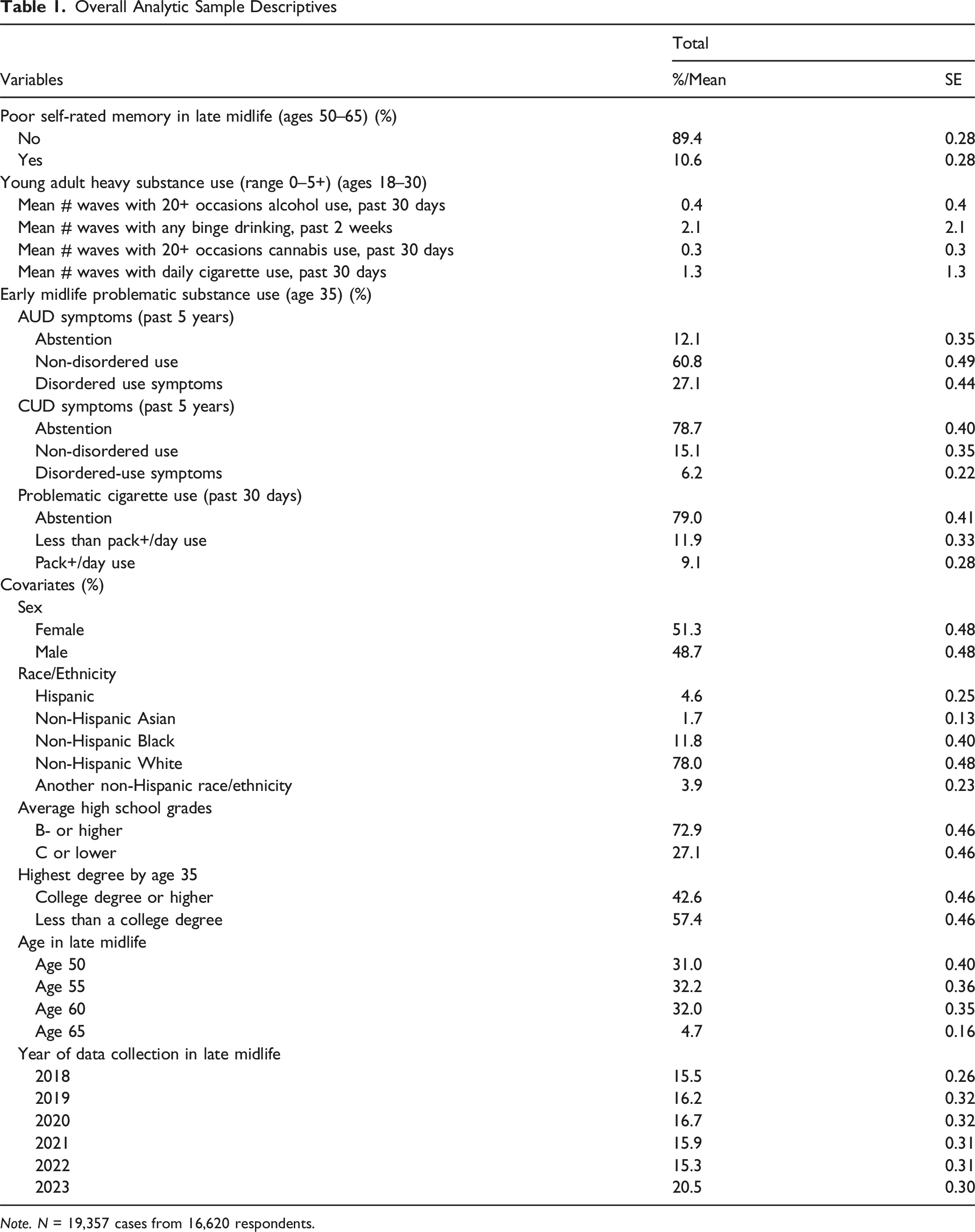
Note. N = 19,357 cases from 16,620 respondents.
Young adult heavy substance use and poor self-rated memory in late midlife (direct effects)
Multivariable Associations Between Young Adult (YA) Heavy Substance Use and Late Midlife Poor Self-Rated Memory: No Mediation
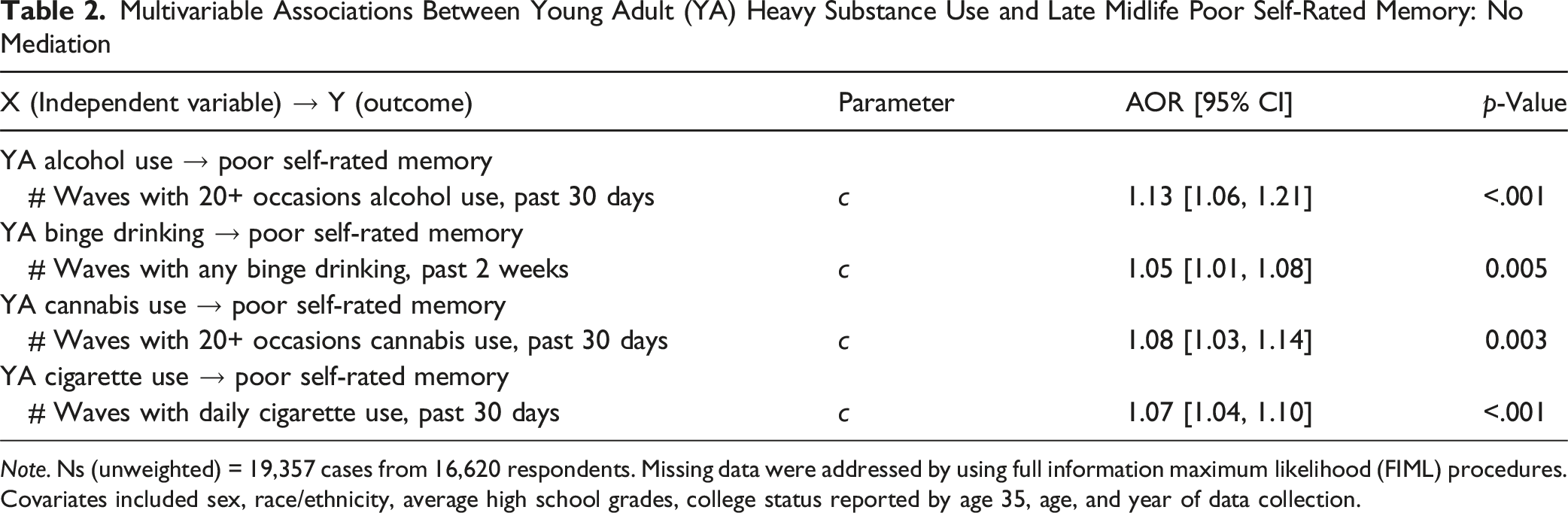
Note. Ns (unweighted) = 19,357 cases from 16,620 respondents. Missing data were addressed by using full information maximum likelihood (FIML) procedures. Covariates included sex, race/ethnicity, average high school grades, college status reported by age 35, age, and year of data collection.
Early midlife problematic substance use as a mediator of young adult heavy substance use associations with late midlife poor self-rated memory
Multivariable Associations Between Young Adult (YA) Heavy Substance Use (X) and Late Midlife Poor Self-Rated Memory (Y): Mediation via Early Midlife Problematic Substance Use (M)
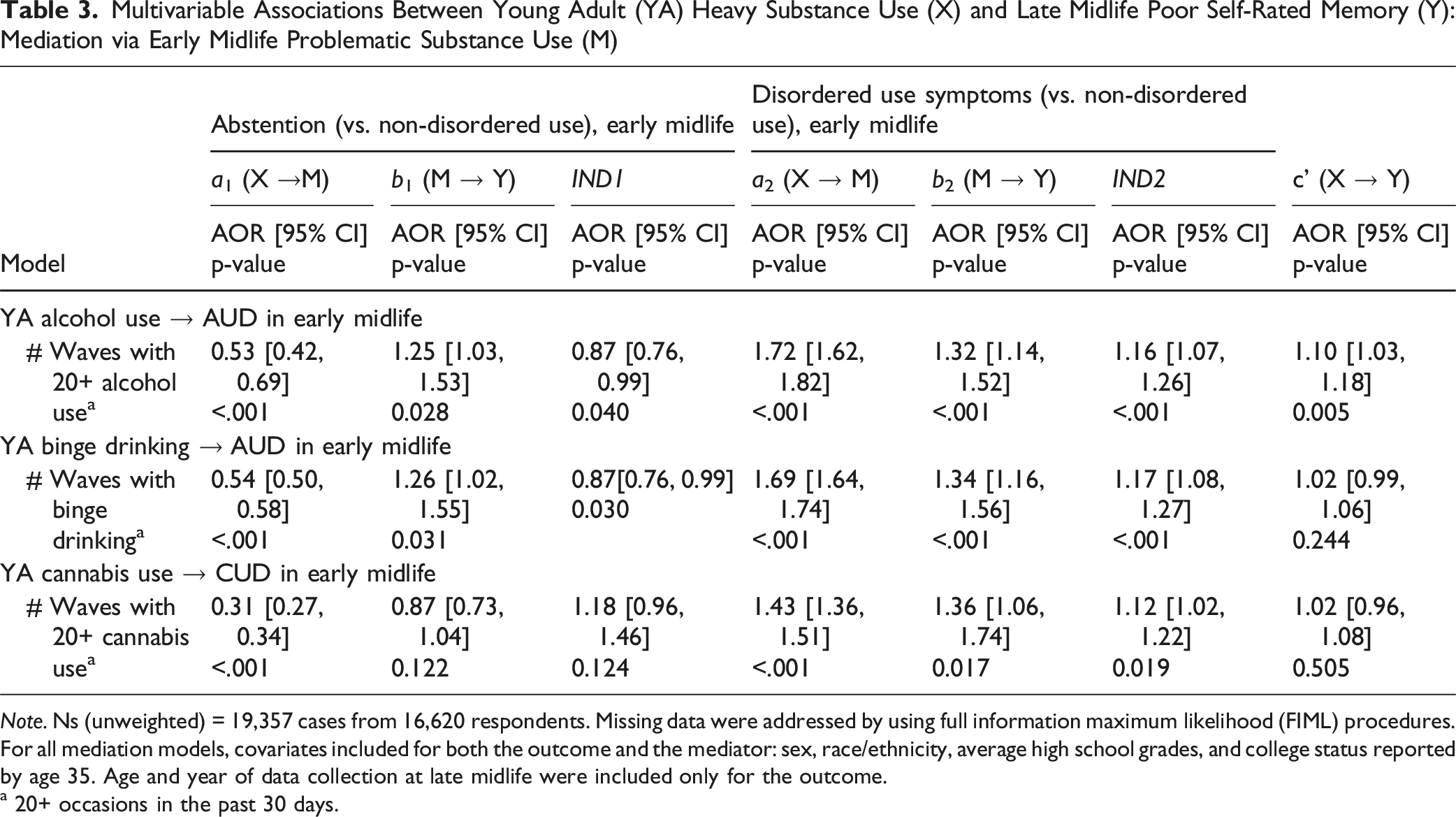
Note. Ns (unweighted) = 19,357 cases from 16,620 respondents. Missing data were addressed by using full information maximum likelihood (FIML) procedures. For all mediation models, covariates included for both the outcome and the mediator: sex, race/ethnicity, average high school grades, and college status reported by age 35. Age and year of data collection at late midlife were included only for the outcome.
a 20+ occasions in the past 30 days.
Multivariable Associations Between Young Adult (YA) Heavy Cigarette Use (X) and Late Midlife Poor Self-Rated Memory (Y): Mediation via Early Midlife Problematic Cigarette Use (M)
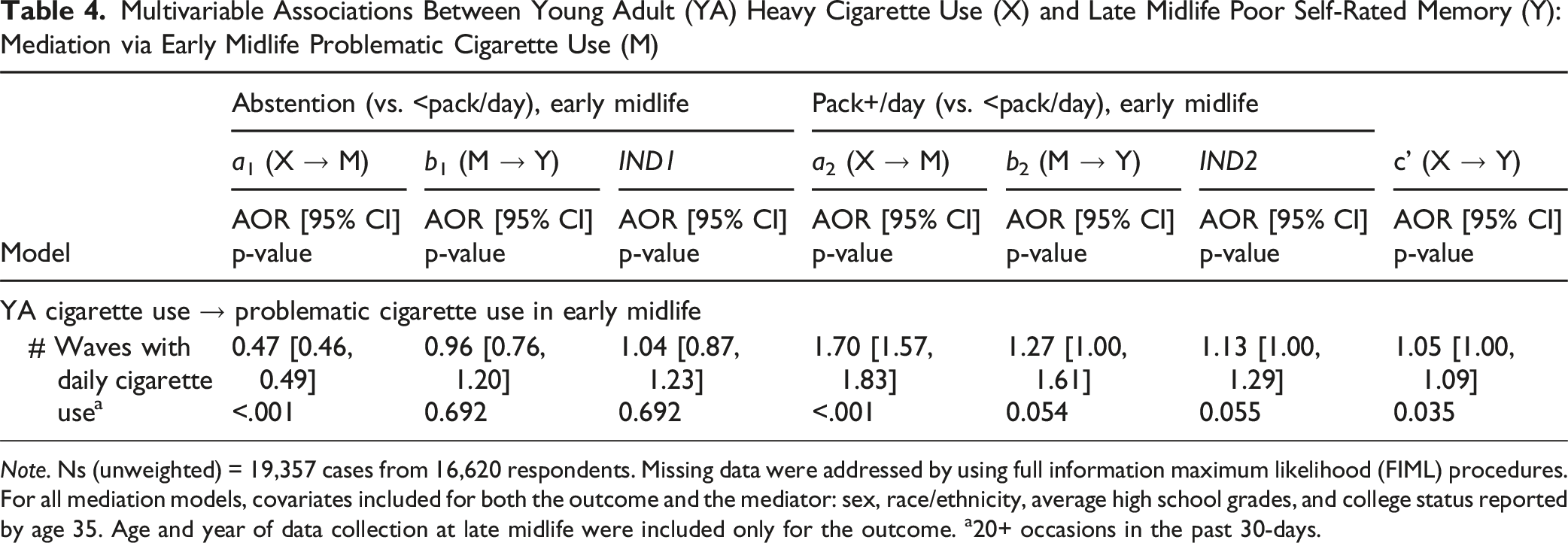
Note. Ns (unweighted) = 19,357 cases from 16,620 respondents. Missing data were addressed by using full information maximum likelihood (FIML) procedures. For all mediation models, covariates included for both the outcome and the mediator: sex, race/ethnicity, average high school grades, and college status reported by age 35. Age and year of data collection at late midlife were included only for the outcome. a20+ occasions in the past 30-days.
For heavy alcohol use, more young adult waves with 20+ occasions of alcohol use were associated with lower odds of abstention (vs. non-disordered alcohol use; a 1 AOR = 0.53, p < 0.001) and higher odds of disordered (vs. non-disordered) alcohol use (a 2 AOR = 1.72, p < 0.001) in early midlife. Both those reporting abstention and disordered use (vs. non-disordered) in early midlife were more likely to report late midlife poor self-rated memory (b 1 AOR = 1.25, p = 0.018; b 2 AOR 1.32, p < 0.001). Both significant direct (c’ AOR = 1.10, p = 0.005) and indirect (IND1 AOR = 0.87, p = 0.040; IND2 AOR = 1.16, p < 0.001) associations were observed, indicating that the association between young adult heavy alcohol use and late midlife poor memory was partially mediated by early midlife AUD symptoms.
For binge drinking, a greater number of young adult waves with binge drinking was associated with lower odds of abstention (a 1 AOR = 0.54, p < 0.001) and higher odds of disordered alcohol use (a 2 AOR = 1.69, p < 0.001), compared to non-disordered use in early midlife at age 35. Both those reporting abstention and disordered use (vs. non-disordered) in early midlife were more likely to report late midlife poor self-rated memory (b 1 AOR = 1.26, p = 0.031; b 2 AOR 1.34, p < 0.001). Significant indirect associations were observed for young adult binge drinking through early midlife AUD symptoms on the odds of late midlife poor memory (IND1 AOR = 0.87, p = 0.030; IND2 AOR = 1.17, p < 0.001). No significant direct association between young adult binge drinking and late midlife poor memory remained (c’ AOR = 1.02, p = 0.244), suggesting the positive association between the young adult binge drinking and increased odds of late midlife poor memory was fully mediated by early midlife AUD symptoms.
For cannabis use, a greater number of young adult waves with 20+ occasions of cannabis use was associated with lower odds of abstention (a 1 AOR = 0.31, p < 0.001) and higher odds of CUD (a 2 AOR = 1.43, p < 0.001), compared to non-disordered use in early midlife at age 35. The likelihood of reporting late midlife poor memory was not associated with abstention (vs. non-disordered use) (b 1 AOR = 0.87, p = 0.122), but those with CUD (vs. non-disordered cannabis use) in early midlife were more likely to report late midlife poor memory (b 2 AOR 1.36, p = 0.017). A significant indirect association was observed through early midlife CUD (vs. non-disordered cannabis use; IND2 AOR = 1.12, p = 0.019). No significant direct association between the number of young adult waves with 20+ occasions of cannabis use and late midlife poor memory remained (c’ AOR = 1.02, p = 0.505), indicating early midlife CUD fully mediated the positive association between the number of young adult waves with heavy cannabis use and late midlife poor self-rated memory.
For cigarette use, a greater number of young adult waves with daily cigarette use was associated with lower odds of abstention (vs. smoking <pack/day) (a 1 AOR = 0.47, p < 0.001) and higher odds of reporting smoking pack+/day (vs. <pack/day) (a 2 AOR = 1.70, p < 0.001) in early midlife at age 35. Early midlife cigarette use was not associated with the odds of late midlife poor self-rated memory (b 1 AOR = 0.96, p = 0.692; b 2 AOR = 1.27, p = 0.054), and no significant indirect associations were observed (IND1 AOR = 1.04, p = 0.692; IND2 AOR = 1.13, p = 0.055). After controlling for early midlife problematic cigarette use, the number of young adult waves with daily cigarette use continued to significantly increase the odds of reporting late midlife poor memory (c’ AOR = 1.05, p = 0.035). This pattern of results suggests a direct, rather than mediated, effect. That is, young adult heavy cigarette use was directly associated with late midlife poor self-rated memory.
Sensitivity Analyses
The above analyses strongly indicated that young adult heavy substance use was either directly or indirectly (via problematic use in early midlife at age 35) associated with late midlife poor self-rated memory, suggesting long-term consequences of substance use specifically during young adulthood. One alternative explanation could be that heavy substance use at one timepoint simply predicts continued heavy use at a following timepoint, and engaging in heavy use correlates with experiencing poor memory at any particular age. To examine this alternative hypothesis, we conducted a sensitivity analysis wherein the multivariable c path logistic regression models were repeated. For alcohol, binge drinking, and cannabis, the models added early midlife problematic use, and then added late midlife substance use (defined as 20+ occasions in the past 30 days for both alcohol and cannabis, any 30-day binge drinking). For cigarette use, early midlife problematic use was not included as the mediation analyses reported above showed no significant associations between early midlife problematic use and late midlife poor self-rated memory. Instead, the multivariable c path model for cigarette use was repeated, followed by adding late midlife substance use (defined as daily cigarette use in the past 30 days). Results are shown in Supplemental Table 10.
For alcohol, binge drinking, and cannabis, the inclusion of late midlife substance use did not substantively affect young adult heavy use or early midlife problematic use associations with late midlife poor memory. For cigarette use, the number of young adult waves of daily cigarette use remained positively and significantly associated with late midlife poor memory (AOR 1.05, p = 0.005), as was late midlife cigarette use (AOR 1.25, p = 0.036).
Discussion
Early detection of dementia is crucial for disease management. Subjective assessment of impaired memory in midlife is an indicator of future cognitive decline and dementia risks (Mitchell et al., 2014). The current study employed a subjective measure of poor memory in late midlife to examine direct associations between young adult heavy substance use (alcohol, binge drinking, cannabis, and cigarettes) and late midlife poor memory, with possible mediation through problematic substance use in early midlife. Our findings—which extend further across the lifespan than prior research (e.g., Meier et al., 2012, 2022)—show that reporting heavy substance use at a greater number of young adult timepoints was consistently associated with poor self-rated memory in late midlife, highlighting the long-term connections between substance use and cognition across the life course. While the magnitude of the observed associations was relatively small, the associations were significant and notable given that they span across decades. The associations observed between young adult heavy use of alcohol, cannabis, and cigarettes with late midlife poor memory are hypothesized to be overlapping versus additive, given comorbidity of use across these substances in these cohorts of young adults. We do not attempt to estimate causal associations or isolate the effects of any single substance because of their natural co-occurrence. Our findings build on previous research showing the effect of longer-duration substance use, such as cannabis, on cognitive functioning (Stypulkowski & Thayer, 2022). Evaluation of any symptoms of disordered cannabis use in the past may provide a crucial signal to late midlife poor memory, which may in turn play a significant role in early detection of dementia. These findings provide strong evidence that heavy and sustained substance use in young adulthood represents a risk factor for cognitive impairment decades later. However, the relationship of memory to dementia is complex and additional research is needed to increase specificity regarding the effects of substance use on various types of dementia.
Furthermore, the risk associated with young adult substance use may operate through continued use and disorder. In fact, young adult substance use was associated with problematic substance use in early midlife, at age 35. In turn, problematic use of alcohol and cannabis (but not cigarettes) in early midlife was significantly associated with greater likelihood of poor self-rated memory in late midlife, at ages 50–65. The degree to which early midlife problematic use mediated associations between young adult heavy substance use and late midlife poor self-rated memory varied by substance. For both binge drinking and frequent cannabis use, there was full mediation, indicating that the association between use during young adulthood and later poor self-rated memory was explained by symptoms of AUD or CUD in early midlife. That is, the stability of substance use over time, which has been previously documented (Patrick et al., 2021; Schulenberg et al., 2016), likely explains the long-term impacts on poor memory. For frequent alcohol use during young adulthood, the effects were partially mediated by AUD. In other words, there remained a direct effect of young adult alcohol use on poor self-rated memory, even after accounting for AUD in early midlife. This may indicate that the effects of earlier substance use affect the brain directly in addition to its effects through continued exposure to the substance. Finally, there was no mediation of young adult frequent smoking through pack a day or more in early midlife (and, in sensitivity analyses, no association between late midlife smoking and late midlife self-rated cognition once young adult heavy smoking was added to the model). Again, this shows that heavy nicotine exposure in early life may have lasting impacts on poor memory, regardless of whether a person quits or continues to smoke. A longer cumulative duration of frequent cigarette use in young adulthood was associated with poor self-rated memory in late midlife, and this association was not mediated by heavy smoking in early midlife. These findings are consistent with the evidence that nicotine use may change brain structures (e.g., Goriounova & Mansvelder, 2012).
In addition to the associations with substance-use disorder, results also show that those who were abstaining from alcohol in early midlife were more likely to report poor self-rated memory than those who were engaging in non-disordered drinking. This is consistent with the U-shaped association between drinking and cognitive function (Stampfer et al., 2005; Zhang et al., 2020) and that alcohol abstainers show the greatest decline in cognitive function (Zanjani et al., 2013). Adults who engage in light or moderate alcohol use tend to have higher cognitive scores than abstainers, likely due to increased socialization and social drinking (Cheng et al., 2023; Gutwinski et al., 2018), while those who are ill or unable to engage in moderate drinking due to mental or physical health are also likely to have poorer cognitive ability (Chikritzhs et al., 2015; Naimi et al., 2005).
Limitations of the study include using self-rated memory as an indicator of cognitive function, which may be influenced by other factors. Future research could be improved by incorporating comprehensive measures of cognitive function via objective assessments. Second, we do not have measures of memory in adolescence, although adolescent cognition may already differ by substance use (Abdulaal et al., 2023). Third, the MTF Longitudinal Panel data were from school-based samples starting at age 18, meaning that those who dropped out of high school were not enrolled. Educational attainment is associated with cognitive function and substance use, so this omission likely attenuated our results. Fourth, attrition during adulthood may have been related to substance use and cognitive decline; weights were used to approximate the national sample of high school students and, therefore, mitigate the influence of attrition. Finally, unobserved confounders such as overall health and lifestyle behaviors across the lifespan may impact observed associations between substance use and poor self-rated memory.
Despite the limitations, the current study is among the first to examine long-term associations between cumulative young adult substance use and late midlife self-rated cognition using prospective longitudinal data across the life course. This extends existing research using retrospective substance-use histories among older adults (Maynard et al., 2023; Rao et al., 2022; Woods et al., 2016) and replicates the association between prolonged substance-use exposure with later life cognition. Our results show potential long-term detrimental impacts of young adult heavy substance use on cognitive health decades later, which is partly explained by substance-use disorder in early midlife. Understanding these risk factors and how they unfold over time will point to potential interventions to support cognitive health.
Supplemental Material
Supplemental Material - Young Adult Substance Use as a Predictor of Poor Self-Rated Memory Decades Later in Midlife
Supplemental Material for Young Adult Substance Use as a Predictor of Poor Self-Rated Memory Decades Later in Midlife by Megan E. Patrick, Yuk C. Pang, Yvonne M. Terry-McElrath, and Joy Bohyun Jang in Journal of Aging and Health
Footnotes
Acknowledgments
The National Institute on Drug Abuse had no further role in the study design; in the collection, management, analysis, and interpretation of the data; in the writing of the manuscript; or in the decision to submit the paper for publication. The views expressed in this article are those of the authors and do not necessarily reflect the views of the funders.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute on Drug Abuse (R01DA001411 and R01DA016575).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.