
Abstract
Objectives
This study examined the influence of hearing status and loneliness on verbal fluency trajectories in adults aged 60 years and older, assessing their contributions to baseline performance and longitudinal change over time.
Methods
Data were drawn from 4,929 participants in the Health and Retirement Study (HRS) with objective hearing assessment in 2018 and three waves of semantic verbal fluency and loneliness measured in 2018, 2020, and 2022. Latent growth curve models were estimated to examine longitudinal change.
Results
Verbal fluency showed a small but statistically significant increase over time, whereas loneliness showed a slight decrease over time. Worse hearing status predicted lower baseline verbal fluency and higher baseline loneliness. The association between hearing status and longitudinal change in verbal fluency was observed in partially adjusted models but was attenuated and did not reach statistical significance after full covariate adjustment.
Discussion
These findings support an association between hearing status and baseline levels of verbal fluency and loneliness, while evidence for longitudinal change in verbal fluency was limited to partially adjusted models.
Background
Aging involves sensory, social, and cognitive changes that significantly affect older adults’ quality of life (World Health Organization, 2015). One of the most prevalent age-related changes is hearing loss, which affects approximately one in three adults aged 65 and older (WHO, 2025). The prevalence of moderate or severe hearing loss, defined by the World Health Organization as hearing loss greater than 35 decibels (dB) in the better-hearing ear, increases steadily with age, rising from 12.7% at age 60 to more than 58.6% at age 90, with half of all global cases concentrated among adults aged 60 and above (WHO, 2025). Beyond sensory decline, worse hearing status has been linked to increased risk of depression, accelerated cognitive decline, difficulties in verbal communication, and greater loneliness (Pronk et al., 2014; Shukla et al., 2020).
Loneliness is defined as a subjective, distressing feeling arising from perceived deficits in the quality of social relationships (Gu & Dupre, 2021). While this experience is fundamentally psychological in nature and can occur independently of objective social isolation (McKenna-Plumley et al., 2023), about one in six individuals worldwide are affected by loneliness, with older adults representing a particularly vulnerable group (WHO, 2025). Loneliness is associated with elevated risk of cardiovascular disease, stroke, depression, anxiety, dementia, and premature mortality (Valtorta et al., 2016; Wang et al., 2023).
Evidence indicates that untreated hearing loss is significantly associated with higher levels of loneliness, even after accounting for demographic, mental health, and medical factors. For example, Fu et al. (2022) found that greater audiometrically assessed hearing loss was associated with higher levels of loneliness among older Chinese adults. Similarly, Jiang et al. (2022) reported that hearing loss was associated with greater social isolation and depressive symptoms, with both loneliness and isolation acting as mediators of this relationship. Conversely, hearing aid use has been associated with reductions in perceived loneliness and may attenuate some of the broader adverse consequences of hearing loss over time (Reed et al., 2025; Weinstein et al., 2016). Recent studies suggest that both worse hearing status and higher loneliness may negatively impact verbal fluency, potentially through reduced environmental stimulation, less frequent language use, and diminished emotional well-being (Cachón-Alonso et al., 2023; Cardona & Andrés, 2023).
Within this context, verbal fluency is one of the cognitive abilities most strongly affected by aging (Lezak, 2012). Neuropsychologically, it reflects the capacity to generate words under phonological or semantic constraints and serves as a sensitive marker of linguistic and executive functioning (Sutin et al., 2019). Semantic fluency shows a steeper decline with age than phonological fluency and may signal early cognitive vulnerability (Clark et al., 2009; Gonzalez-Burgos et al., 2019). A recent systematic review further highlights that language difficulties including impairments in discourse production, naming, and comprehension are part of the early profile of mild cognitive impairment, reinforcing the clinical value of verbal fluency tasks in aging research (De La Hoz et al., 2021).
However, findings across the literature are mixed. Fields et al. (2020) reported no accelerated decline in verbal fluency associated with self-reported hearing loss, whereas Loughrey et al. (2020), using objective audiometric assessments, found differences in lexical access and retrieval efficiency between individuals with and without age-related hearing loss. Regarding loneliness, longitudinal evidence shows that higher baseline loneliness predicts poorer initial verbal fluency and greater decline over time, with bidirectional associations between loneliness and cognitive function (Simpson et al., 2019; Yin et al., 2019).
The common cause hypothesis of sensory-cognitive aging (Baltes & Lindenberger, 1997) provides a theoretical framework to integrate these findings. It posits that sensory and cognitive declines share underlying neurobiological mechanisms, a perspective that has been further refined by contemporary theoretical accounts highlighting multiple interacting pathways linking hearing loss and cognitive decline (Wayne & Johnsrude, 2015). Sensory and cognitive changes may also indirectly affect one another by reducing opportunities for social interaction, increasing loneliness, and creating a negative feedback loop between hearing status, social experience, and cognition (Dawes et al., 2015; Shukla et al., 2020). Longitudinal evidence further suggests that social isolation may function as a pathway linking sensory difficulties to cognitive decline in older adults (Yorgason et al., 2022), underscoring the importance of examining these constructs across time.
Despite extensive evidence linking age-related hearing loss and loneliness to cognitive vulnerability in later life, their combined longitudinal influence on language production remains underexamined. Existing studies have largely examined these factors independently, relying predominantly on cross-sectional designs and self-reported measures, which restrict causal inference and limit insight into mechanisms of change (Shukla et al., 2020). From a theoretical perspective, this gap can be considered in light of frameworks such as the common cause hypothesis, sensory deprivation accounts, and social cascade models, all of which posit that sensory decline and reduced social engagement may jointly exacerbate language and cognitive vulnerability in later life (Baltes & Lindenberger, 1997; Pichora-Fuller et al., 2016). However, longitudinal models integrating objective hearing assessments and perceived loneliness as simultaneous predictors of verbal fluency trajectories across multiple waves remain scarce, limiting understanding of language change as a dynamic process in cognitive aging.
Therefore, the objective of this study was to examine the influence of hearing status and loneliness on verbal fluency trajectories in adults aged 60 years and older, assessing their contributions to baseline performance and longitudinal change over time.
Methods
Participants and Design
Data were drawn from the Health and Retirement Study (HRS; Sonnega et al., 2014), a longitudinal survey of older adults in the United States based on an originally nationally representative sampling design and administered by the University of Michigan. Participants were selected based on the following sequential criteria: (a) being a self-respondent in the 2018 wave (n = 17,146); (b) being 60 years of age or older (n = 12,010); and (c) providing at least one valid objective hearing measure during the 2018 core interview (n = 4,929). These 4,929 individuals constituted the eligible baseline sample for the current study.
Variables and Measures
Hearing Status
Hearing was objectively assessed in 2018 using a pure-tone hearing detection test administered by trained interviewers during the in-person assessment. Participants were asked to remove any hearing aids prior to the test, following the standardized protocol of the Health and Retirement Study physical measures assessment.
Four measurements were obtained: two in the left ear (1000 Hz and 3000 Hz) and two in the right ear (1000 Hz and 3000 Hz). For each frequency, six tones were presented, and respondents were instructed to raise their finger whenever they detected a sound. The number of correctly detected tones (ranging from 0 to 6) was recorded for each measurement.
A global hearing detection score was calculated by averaging responses across the four measurements. Values were then reverse-coded so that higher scores indicated worse hearing status, reflecting reduced tone detection ability. Hearing assessments were available only in 2018 because in-person data collection was suspended during the COVID-19 pandemic.
Loneliness
Loneliness was measured with a single HRS item: “During the last week, did you feel lonely much of the time?” The original item is dichotomous (1 = yes; 5 = no). For analyses, responses were recoded into a dummy variable (1 = lonely, 0 = not lonely). Nonresponse codes (e.g., 8 = “Do not know” and 9 = “Refused,” blank values) were treated as missing data. Overall, 2 cases (0.06% of the total sample) were classified as missing for this item. This measure reflects momentary subjective loneliness rather than chronic or structural loneliness. Although single-item measures are less comprehensive than multi-item scales, recent validation studies have demonstrated acceptable convergent and construct validity in large population-based samples, showing moderate correlations with established multi-item loneliness scales (e.g., ρ ≈ .57) (Reinwarth et al., 2023). Such measures are commonly used in epidemiological research when brief assessment is required (Kotwal et al., 2022).
Verbal Fluency
Semantic verbal fluency was assessed across three waves (2018, 2020, and 2022). Participants were asked to name as many animals as possible within 60 seconds. This task is widely used in aging research as an indicator of language production and executive-linguistic functioning and has demonstrated sensitivity to cognitive change in older adults (Cachón-Alonso et al., 2023; Sutin et al., 2019).
Covariates
Covariates included age (continuous, measured in years), years of education (continuous, measured as years of formal education), gender (0 = male, 1 = female), marital status (0 = not married or partnered, 1 = married or partnered), self-rated physical health (1 = excellent to 5 = poor), and self-reported hearing aid use (0 = no, 1 = yes). All covariates were measured at the 2018 baseline wave. These variables were included given prior evidence linking sociodemographic and health-related factors to hearing status, loneliness, and cognitive performance in later life.
Procedure
Interviews were conducted under protocols approved by the University of Michigan Health Sciences/Behavioral Sciences Institutional Review Board. Prior to each interview, participants received a written informed consent information document and provided consent in accordance with IRB-approved procedures. Respondents were also read a confidentiality statement at the beginning of each interview. The HRS maintains formal documentation of all consent and confidentiality procedures. The present study used publicly available de-identified secondary data from the 2018, 2020, and 2022 waves; therefore, no additional institutional approval was required for these analyses.
Data Analysis
Prior to estimating the models, statistical assumptions and the handling of missing data were examined. The missing data mechanism was evaluated using Little’s test implemented through the TestMCARNormality function from the MissMech package in RStudio (Jamshidian & Jalal, 2010). Results indicated significant differences in both the Hawkins test (p < .001) and the nonparametric test (p < .001), suggesting that the data did not follow a completely random missingness pattern (MCAR).
Descriptive Statistics
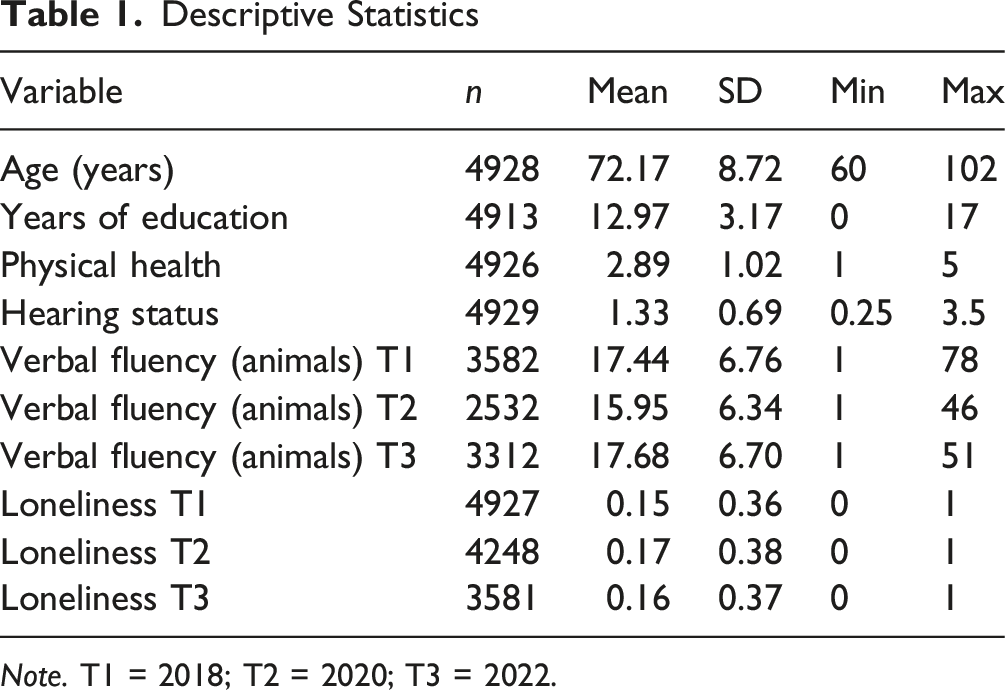
Note. T1 = 2018; T2 = 2020; T3 = 2022.
Outliers were inspected using the 1.5 IQR criterion for continuous variables. The proportion of cases outside the expected range was low (all <1%); therefore, given their minimal influence, no additional transformations were applied. Multivariate normality was evaluated using Mardia’s test, revealing significant deviations in both multivariate skewness and kurtosis (p < .001).
Latent Growth Curve Models (LGCMs) were fitted to examine longitudinal changes in verbal fluency and perceived loneliness across three waves, estimating both intercepts (initial levels) and slopes (rates of change). Because hearing was assessed only in 2018, it was included as a time-invariant predictor of both the intercept and slope of each trajectory. Age, gender, years of education, marital status, self-rated physical health, and self-reported hearing aid use were included as covariates in the fully adjusted models to control for potential confounding effects.
Models were estimated using robust maximum likelihood (MLR). Model parameters were estimated using full-information maximum likelihood (FIML) under the MAR assumption. All observed variables, including exogenous covariates, were incorporated into the model estimation so that cases with partially missing data could contribute to parameter estimation under the FIML framework.
Model fit was evaluated following Kline (2023) recommendations, reporting the scaled chi-square statistic (Yuan–Bentler correction), the robust Comparative Fit Index (CFI; acceptable values ≥.95), the robust Tucker–Lewis Index (TLI; acceptable values ≥.90), the robust Root Mean Square Error of Approximation (RMSEA; ≤.06 with its 90% confidence interval), and the Standardized Root Mean Square Residual (SRMR; ≤.08). Parameter interpretation was based on standardized estimates, with statistical significance defined as p < .05 for regression, variance, and covariance parameters.
All analyses were conducted in RStudio (R Core Team, 2025) using the lavaan package (Rosseel, 2012).
Results
Descriptive statistics are presented in Table 1. Participants had a mean age of 72.17 years (SD = 8.72), and 41.35% were men and 58.65% were women. A total of 53.29% were married or partnered and 46.71% were not. At baseline, 2.98% of participants reported using hearing aids. The longitudinal models were estimated using data from 4,929 participants.
The model fit indices indicated excellent fit to the data (χ2_YB(21) = 91.26, p < .001; robust CFI = .987; robust TLI = .965; robust RMSEA = .039 [.032, .046]; SRMR = .012).
For verbal fluency, the latent intercept was statistically significant and different from zero (b = 25.06, SE = 1.09, p < .001), whereas the latent slope was statistically significant and positive (b = 1.27, SE = 0.63, p = .043), indicating a slight model-estimated increase in verbal performance over time. Significant variance was observed around the intercept of verbal fluency (σ2_i = 22.30, p < .001), whereas the variance around the slope did not reach statistical significance (σ2_s = 1.10, p = .066), suggesting limited evidence of individual differences in rates of change.
For perceived loneliness, the latent intercept was positive and statistically significant (b = 0.13, SE = 0.05, p = .014). The latent slope was negative and statistically significant (b = −0.10, SE = 0.04, p = .007), indicating a slight decrease in loneliness over time. Significant variance was observed around both the intercept and slope of loneliness (σ2_i = 0.059, p < .001; σ2_s = 0.006, p = .027), suggesting meaningful heterogeneity in both initial levels and trajectories of perceived loneliness across participants.
Worse hearing status significantly predicted the initial level of verbal fluency (β = −.077, p < .001). Regarding the rate of change, hearing status was significantly associated with verbal fluency in partially adjusted models; however, this association was attenuated in the fully adjusted model and was not statistically significant (β = −.100, p = .067; see Supplemental Table 1). Accordingly, hearing status was not associated with the rate of change in verbal fluency in the fully adjusted model. Hearing status also predicted higher baseline loneliness (β = .109, p < .001), but it was not associated with longitudinal change in loneliness (β = −.033, p = .490).
Age was negatively associated with the initial level of verbal fluency (β = −.269, p < .001) and with baseline loneliness (β = −.072, p = .001) and positively associated with change in loneliness (β = .171, p < .001). Years of education predicted higher baseline verbal fluency (β = .355, p < .001) but was unrelated to baseline loneliness or its trajectory. Gender was not significantly associated with verbal fluency intercept or slope, nor with the loneliness slope, but was positively associated with baseline loneliness (β = .076, p < .001) indicating that women reported higher baseline loneliness than men. Marital status predicted higher baseline verbal fluency (β = .075, p < .001) and lower baseline loneliness (β = −.237, p < .001) indicating that married or partnered individuals reported lower loneliness than those not partnered, as well as a greater rate of increase in loneliness over time (β = .126, p = .003). Poorer self-rated physical health was associated with lower baseline verbal fluency (β = −.134, p < .001) and higher baseline loneliness (β = .258, p < .001), but was unrelated to change in either outcome over time. Self-reported hearing aid use was not significantly associated with the intercept or slope of verbal fluency or loneliness.
Finally, two significant covariances emerged between latent factors. The negative covariance between the intercepts of verbal fluency and loneliness (β = −.086, p = .002) indicated that higher baseline loneliness was associated with lower baseline verbal fluency. Similarly, the negative covariance between the intercept and slope of loneliness (β = −.405, p = .018) indicated that individuals with higher initial levels of loneliness experienced a steeper rate of decline over time. The covariance between the intercept and slope of verbal fluency was negative but not statistically significant (β = −.233, p = .126) (Figure 1). Latent growth curve model of verbal fluency and loneliness with hearing status as a time-invariant predictor. Note. Standardized coefficients are presented. Solid arrows represent significant paths (p < .05), and dashed arrows represent non-significant paths. Hearing status was measured in 2018, with higher scores indicating worse hearing status. Covariate paths (age, years of education, gender, marital status, self-rated physical health, and hearing aid use) are omitted from the figure for clarity but were included in all model estimations. T1 = 2018; T2 = 2020; T3 = 2022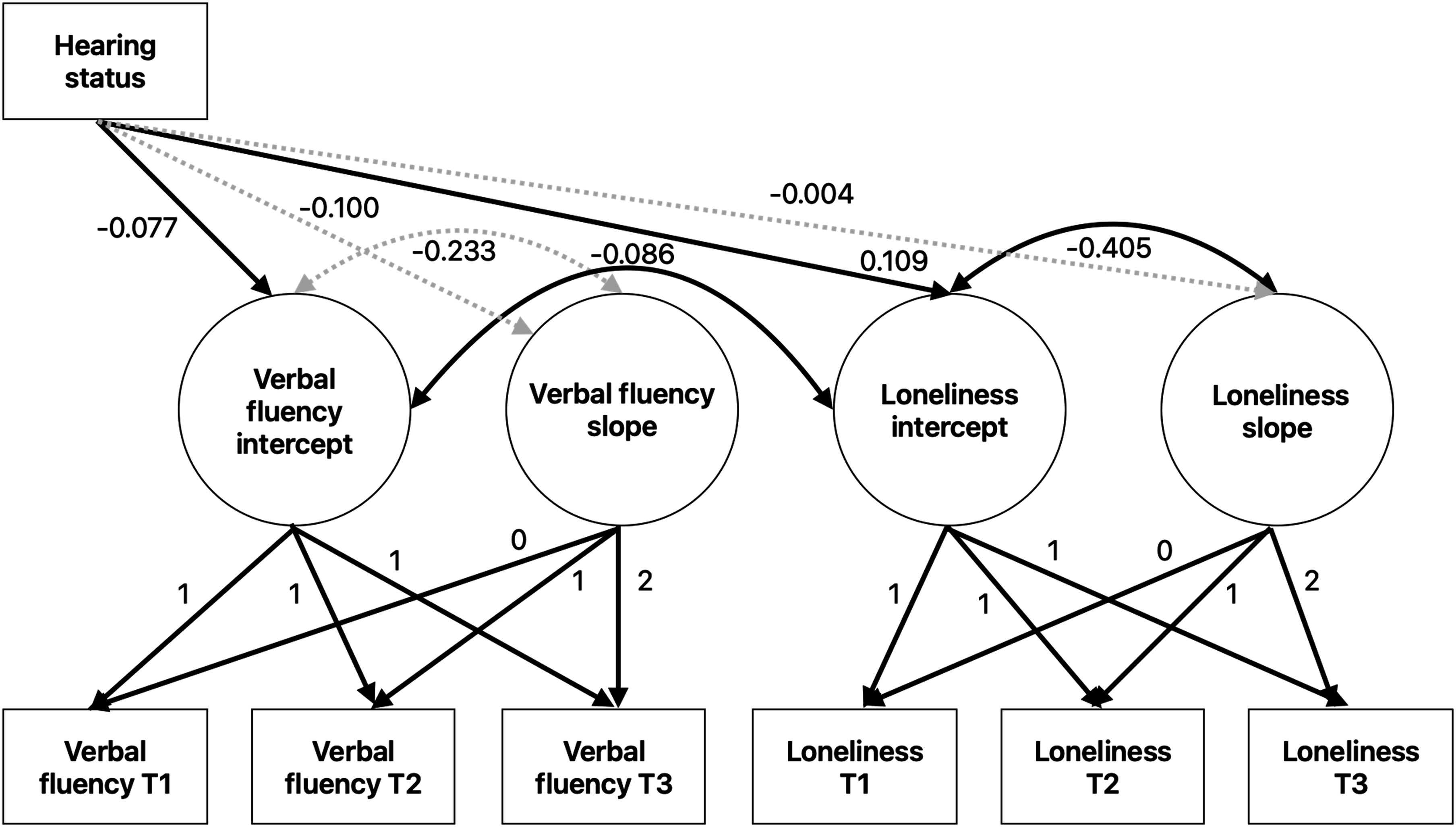
Discussion
The aim of this study was to examine the influence of hearing status and loneliness on verbal fluency trajectories in adults aged 60 years and older, assessing their contributions to baseline performance and longitudinal change over time. The findings contribute to a more nuanced understanding of how sensory and socioemotional factors relate to verbal fluency performance over time. Although the present measure reflects objective hearing detection ability rather than a full audiometric diagnosis, it provides a standardized indicator of hearing status in later life. Accordingly, the present findings should be interpreted in terms of variability in hearing status rather than clinical diagnoses of hearing loss.
The present findings support an association between hearing status and baseline verbal fluency, but not with longitudinal change after covariate adjustment. Worse hearing status was robustly associated with lower initial levels of verbal fluency, consistent with prior research (Lin & Albert, 2014; Shukla et al., 2020). The effect size showed a monotonic attenuation across increasingly adjusted specifications (β = −.269 in the unadjusted model; β = −.077 in the fully adjusted model; see Supplemental Table 1), but remained statistically significant throughout, suggesting that the baseline association is robust to covariate adjustment. For the rate of change, the attenuation was steeper (β = −.163 in the unadjusted model; β = −.100 in the fully adjusted model) and the association was no longer statistically significant after full adjustment, suggesting that the slope association may be partly accounted for by covariates such as age, education, and physical health.
The association between hearing status and baseline verbal fluency is compatible with the common cause hypothesis (Baltes & Lindenberger, 1997), particularly as observed across model specifications. This hypothesis posits that age-related changes in sensory and cognitive functioning may share underlying mechanisms. Reduced auditory input quality has been proposed to increase perceptual effort, thereby diverting cognitive resources from higher-order linguistic processing (Peelle, 2018; Pichora-Fuller et al., 2016; Tun et al., 2009). In this context, individuals experiencing greater hearing difficulty may show lower efficiency during tasks requiring rapid lexical access, such as semantic fluency, contributing to lower baseline performance.
Verbal fluency showed a small but statistically significant increase over time. This pattern should be interpreted with caution, as positive slope estimates in longitudinal cognitive data are commonly attributed to practice effects and increased task familiarity across repeated assessments (Calamia et al., 2012), as well as to selective attrition, whereby individuals with greater health burden are more likely to drop out over time, leaving a progressively healthier analytic sample (Salthouse, 2014). In addition, cohort effects may contribute to upward shifts in verbal fluency performance, as later-born individuals have been shown to exhibit higher baseline levels and less pronounced age-related decline (Massa et al., 2024). This trajectory should therefore not be interpreted as evidence of genuine cognitive improvement at the population level.
The covariance between the intercept and slope of verbal fluency was not statistically significant, indicating no reliable association between baseline performance and rates of change. Similarly, the variance of the slope did not reach statistical significance, suggesting limited evidence of interindividual variability in rates of change.
Perceived loneliness showed a slight model-estimated decrease over time, contrasting with some evidence suggesting gradual increases in loneliness in later life (Yin et al., 2019). This pattern is also consistent with longitudinal evidence from large U.S. samples showing that average loneliness remained stable or even slightly decreased during the early pandemic period, which may reflect compensatory social and family support (Docherty et al., 2021; Luchetti et al., 2020). Although broader contextual influences during the 2020–2022 window cannot be fully ruled out, the absence of a marked upward shift across waves and the stability of the hearing-status associations across baseline and slope models suggest that the observed patterns are unlikely to be solely attributable to pandemic-related effects.
Hearing status was associated with higher baseline loneliness, consistent with research showing that hearing difficulties may reduce opportunities for social and linguistic engagement (Cardona & Andrés, 2023; Pronk et al., 2014). However, hearing status did not predict changes in loneliness over time, and this null finding warrants cautious interpretation. Hearing difficulties have been more consistently linked to social isolation than to loneliness, which reflects a subjective appraisal of social connection. Prior work suggests that depressive symptoms, functional limitations, and environmental factors may mediate associations between hearing difficulties and loneliness (Bezerra et al., 2021). The absence of an objective measure of social isolation in the present study precludes a direct evaluation of these potential pathways.
Older adults with hearing difficulties may experience loneliness even when surrounded by others, given the additional cognitive effort required to decode speech (Pichora-Fuller et al., 2016). This increased cognitive load may affect both verbal processing efficiency and socioemotional well-being. Including separate measures of loneliness and social isolation in future work would help clarify how these constructs interact with hearing status across time. The significant negative covariance between the intercepts of loneliness and verbal fluency (β = −.086, p = .002) indicates that individuals reporting higher levels of loneliness also exhibited lower initial cognitive-linguistic performance, which is consistent with the notion of interconnected socioemotional and cognitive functioning in later life.
Regarding covariates, age, gender, education, marital status, and self-rated physical health showed significant associations. Age was negatively associated with the intercepts of verbal fluency and loneliness, and positively associated with change in loneliness, consistent with prior evidence on age-related differences in cognitive and socioemotional functioning (Jo et al., 2021). Education was associated with higher initial levels of verbal fluency, consistent with cognitive reserve models (Stern, 2009).
Marital status was associated with higher intercept of verbal fluency and lower intercept of loneliness, indicating that married or partnered individuals reported lower loneliness than those not partnered, which is consistent with the idea that partnership status may provide greater opportunities for conversational engagement and social support (Ng et al., 2022). Marital status was also associated with a greater rate of increase in loneliness over time, suggesting differential trajectories across partnership groups. Poorer self-rated physical health was associated with lower intercept of verbal fluency and higher intercept of loneliness, consistent with evidence indicating that physical vulnerability and functional limitations frequently co-occur with sensory and cognitive burden in aging populations (Chen et al., 2015). Gender was positively associated with the intercept of loneliness, indicating that women reported higher loneliness than men, consistent with prior evidence on sex differences in subjective social experiences in later life (Pinquart & Sörensen, 2001).
In contrast, hearing aid use was not significantly associated with the intercepts or slopes of verbal fluency or loneliness. The absence of an effect for hearing aid use may reflect the relatively low prevalence of use in the sample and the lack of detailed information regarding duration or consistency of use. Adjustment for covariates attenuated the magnitude of the associations between hearing status and the study outcomes, and the association with change in verbal fluency did not remain statistically significant in the fully adjusted model, suggesting that these associations may be partly accounted for by demographic and health-related factors.
This study has certain limitations that should be considered. Hearing status was assessed only in 2018, requiring its treatment as a time-invariant predictor. The hearing assessment tested only two frequencies (1,000 and 3,000 Hz) at a fixed screening intensity, which may not fully capture the broader audiometric profile of hearing impairment in later life, as it does not provide threshold-based audiometric classification. This testing protocol reflects the standardized hearing screening procedure implemented in the HRS physical measures module and was not modifiable by the researchers, as it was designed as a brief field-based assessment focusing on core speech-frequency ranges.
Although hearing aid use was included as a covariate, information regarding duration, consistency of use, or audiological adjustment was unavailable, which may limit interpretation of compensatory effects. The dichotomous measure of loneliness may have reduced sensitivity compared to multi-item scales. Additionally, the study could not distinguish late-life hearing difficulties from earlier-onset hearing impairment, which may influence language performance trajectories. The absence of an objective measure of social isolation also limits conclusions regarding potential mechanisms linking hearing status and socioemotional functioning.
Despite these limitations, the study has notable strengths. The use of latent growth curve modeling enabled the examination of dynamic trajectories rather than static associations. The large sample drawn from the Health and Retirement Study enhances the relevance of the findings. The inclusion of an objective hearing assessment improves methodological rigor relative to studies relying solely on self-report. Together, these strengths contribute to a more precise characterization of how hearing status relates to linguistic and socioemotional outcomes in later life.
Future studies should incorporate parallel assessments of social isolation and loneliness, examine potential mediators such as depressive symptoms or communication-related effort, and consider incorporating longitudinal assessments of hearing to better characterize changes in sensory functioning over time. Integrating cognitive effort indices or speech-in-noise measures would further clarify whether increased perceptual load partially accounts for changes in verbal fluency. Longitudinal designs with extended follow-up periods will also be essential for understanding how sensory, social, and cognitive domains interact across aging.
Overall, the findings highlight the importance of routine hearing assessment and timely intervention in later life. While the present findings document an association between hearing status and baseline verbal fluency and loneliness levels rather than causal evidence of intervention efficacy, they are consistent with frameworks emphasizing the value of auditory assessment within broader preventive strategies for healthy cognitive aging. Future intervention studies, including recent work such as the ACHIEVE trial (Reed et al., 2025), will be essential to determine whether audiological interventions translate into measurable benefits on cognitive and socioemotional trajectories in older adulthood.
Supplemental Material
Supplemental material - Hearing Status, Loneliness, and Verbal Fluency in Older Adults: A Latent Growth Curve Modeling Approach
Supplemental material for Hearing Status, Loneliness, and Verbal Fluency in Older Adults: A Latent Growth Curve Modeling Approach by Damián Medina-Valdebenito, Tomás Espinoza-Palavicino, Oscar Terán-Mendoza, Vicente Cancino, and Juan Barra-Barrera in Journal of Aging and Health
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Agencia Nacional de Investigación y Desarrollo (ANID): 21231906 and Programa de Becas, Doctorado Becas Chile: 21231269.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.