
Abstract
Objectives
This study examined how caregiving intensity, duration, and labor type are associated with physical and mental health among family caregivers (FCGs) across life-course stages.
Methods
Using cross-sectional data from 2,610 FCGs in the 2024 Behavioral Risk Factor Surveillance System, we applied multivariable logistic and linear regression models stratified by life-course stage.
Results
Women had 65% higher odds of depression than men (aOR = 1.65, 95% CI = 1.22–2.22), consistent across all age groups. Older FCGs who provided care for two or more years showed markedly worse physical health, a pattern consistent with wear-and-tear and cumulative disadvantage frameworks. Midlife FCGs presented a sandwich-generation profile of worse physical health with increased caregiving intensity.
Conclusion
Findings highlight the need for age-tailored caregiver support and structural reforms, including expanding the Family and Medical Leave Act, wage replacement programs, and a caregiving-linked Medicare benefit.
Keywords
Introduction
As the older adult population rapidly expands across the United States, family caregiving has become one of the most important, and least invested in issues affecting older adults and their families. By 2060, the number of Americans age 65 and older is expected to almost double, this growth will mark a substantial increase in the number of Americans who need ongoing support living with chronic illness, disability, and functional limitations (AARP & National Alliance for Caregiving, 2025). Today, one in five adults in the U.S. is caring, unpaid of charge, for a loved one with a chronic health condition or disability (Kilmer et al., 2024). Older adult caregivers—and specifically, older spousal caregivers, are uniquely positioned within this care work. They provide high-hours and high-intensity care while often experiencing their own age-related declines in health and often lack the workplace protections and structural supports that paid caregivers have. Broadly defined, a family caregiver (FCG) is an unpaid person, usually a spouse, adult child, sibling, or other family member who provides ongoing assistance to a relative with a chronic health condition, disability, or functional limitation (AARP & National Alliance for Caregiving, 2025). Unlike time-limited caregiving associated with acute illness or injury recovery, chronic caregiving is sustained over months or years, often without a foreseeable endpoint, and encompasses a wide range of responsibilities, including providing assistance with activities of daily living, household tasks, and in some situations complex medical and nursing care tasks (National Alliance for Caregiving & AARP, 2025).
Thinking of caregiving as informal unpaid work further highlights how the intensity, duration, and nature of caregiving is determined not just by clinical need but by how paid work and unpaid work is socially organized. Glucksmann’s (2016) framework of the Total Social Organisation of Labour (TSOL), defined as all forms of paid and unpaid, formal and informal work through which society is reproduced—provides a useful lens here to think about how caregiving subsidizes the formal economy while keeping it invisible, unprotected, and disproportionately falling on certain social groups. This framework rings especially true for older adult caregivers: the work performed by older spousal caregivers is vital to keeping households functioning and allowing care recipients to age in place, but it does not provide any of the legal protections, employer benefits, or safeguards we see in formal jobs.
As such, the demands of the caregiving role are multi-dimensional and can exact high physical and psychological costs for those who provide care. Caregiving demands have been characterized as ongoing stressors associated with declines in personal wellbeing over time, proliferating into secondary hardships including financial strain, role overload, and social isolation (Liang et al., 2024; Pearlin et al., 1990; Wagle et al., 2024). Physically, caregivers are at elevated risk for fatigue, sleep disturbance, pain, reduced physical functioning, and increased risk of cardiovascular disease compared to non-caregivers, with research indicating that higher caregiving intensity is associated with greater deterioration across multiple physical health dimensions (Cho et al., 2024; Keramat et al., 2025).
There are three main dimensions to the caregiving labor process that are tied to the demands on caregivers and associated outcomes. First, caregiving intensity (operationalized here as the average number of hours of care provided per week) can be conceptualized as the time demands of the job, ranging from low levels of sustained support to intensive, full-time care. Second, the duration of caregiving captures the time trajectory of the caregiver-care recipient relationship and ranges from temporary assistance (lasting a few weeks) to caregiving across several years or even decades. Duration may be particularly salient for older FCGs as lengthy caregiving careers are associated with chronic labor exposure in which physical and emotional demands accumulate over time (Schulz & Sherwood, 2008). Finally, type of caregiving labor can be differentiated between two main categories: direct personal care (i.e., helping with activities such as bathing or dressing), and household or instrumental caregiving tasks (e.g., preparing meals, providing transportation, managing finances, etc.). Similarly, whether a caregiver primarily performs hands-on personal care versus household and logistical tasks may shape the nature and magnitude of the burden experienced, as these labor types differ in physical demands, time requirements, and perceived role strain (Krämer & Bleidorn, 2024). While each type of caregiving places an unavoidable burden on FCGs both physically and mentally, each dimension of caregiving may differentially relate to caregiver quality of life (QOL) (Li et al., 2025). Yet these three dimensions are rarely examined simultaneously across the full population of FCGs in a large, nationally representative sample, leaving important gaps in our understanding of how each uniquely and jointly relates to caregiver wellbeing.
Using the Behavioral Risk Factor Surveillance System (BRFSS), a nationally representative, 50-state telephone survey, the present study sought to answer two questions: (1) whether caregiving intensity, duration, and type of labor are associated with five QOL indicators (physically unhealthy days, self-rated health, activity limitations, mentally unhealthy days, and depression status), and (2) whether these associations varied by life-course stage. The second question emerges from life-course theory’s central premise that the age or timing at which individuals take on care roles associated with the social and economic contexts in which care-related stressors occur and resources are accessed (Elder, 1994; Neller et al., 2024). Two directional hypotheses emerge from the literature above. First, we hypothesize that higher levels of caregiving intensity, duration, and involvement in direct personal care would each be related to poorer self-reported physical and mental health outcomes, controlling sociodemographic covariates. Second, we hypothesize that these relationships would differ by life-course stage such that physical health would be strongest among older caregivers in line with cumulative disadvantage and wear-and-tear models, and mental health would be strongest among young adult caregivers (in line with off-time role acquisition and disrupted transition frameworks). Collectively, these advance our knowledge of the ways in which intensity and duration of unpaid care work are each associated with health and wellbeing across the life course with implications for gerontological theory, policy and practice related to aging.
Methodology
Sample
Data for this study were drawn from the 2024 BRFSS dataset. The BRFSS is a continuous, state-based, random-digit dialed telephone health survey conducted by the Centers for Disease Control and Prevention (CDC) with participating state and territorial health departments. The data collection is conducted in all 50 states, District of Columbia, and three U.S. territories yearly through random-digit-dialed landline and cellular telephone interviews. It is currently the world’s largest continuously conducted health survey system (Centers for Disease Control and Prevention, 2024). BRFSS measures have been evaluated for reliability and validity in peer-reviewed methodological studies (Nelson et al., 2001; Pierannunzi et al., 2013). These prior studies suggest moderate to high reliability for most chronic disease, behavioral, and demographic items, though objectively defined indicators tend to perform better than subjective health appraisals (Nelson et al., 2001; Pierannunzi et al., 2013). The Caregiver Module is an optional module that states choose whether or not to include. Questions used in the current study on intensity, duration, and type of caregiving labor are standardized across states that administer the module. The final sample for this study is comprised of 2,610 respondents that completed the caregiving module and self-reported providing care to a family member; these respondents included participants that answered questions pertaining to the key variables used in our analyses including caregiving characteristics (i.e., caregiving intensity, caregiving duration, and type of labor), all QOL measures, and demographic covariates (education level, marital status, annual household income, employment status, number of children, and health insurance coverage).
Measures
Five QOL outcomes were measured by standard BRFSS items covering (1) poor physical health; (2) general health status; (3) poor physical or mental health activity limitation; (4) poor mental health; and (5) depression. Responses for outcomes 1, 3, and 4 were 0 to 30 days. Responses for outcome 2 were reverse coded to indicate improving general health status from poor to excellent. Outcome 5 responses were yes and no.
The first predictor, caregiving intensity, is measured as the average number of caregiving hours per week. This is a categorical variable with three responses: less than 20 hr per week; 20–39 hr per week; and 40 or more hours per week. The second predictor, caregiving duration, is measured as the length of time of provider care. This is a categorical variable with 4 responses: less than 30 days; 1 month to less than 2 years; 2 years to less than 5 years; and 5 years or more. The last predictor, type of caregiving labor, was measured by two questions; one question asked if the caregiver was managing personal care in the last 30 days, and the other asking if the caregiver managed household tasks in the last 30 days. Both questions had responses: yes/no.
Covariates were demographic characteristics including: race/ethnicity (non-Hispanic White, non-Hispanic Black, non-Hispanic Asian, non-Hispanic American Indian and Alaska Native, Native Hawaiian and Pacific Islander, Hispanic, or non-Hispanic other), sex (men [male], women [female]), education level (less than high school; high school graduate; attend college or technical school; and graduate college or technical school), marital status (married; divorced, widowed or separated; never married or unmarried couple), annual household income (less than $25,000; $25,000 to $49,999; $50,000 to $74,999; and $75,000 or more), employment status (currently employed, not currently employed), number of children (range 0 to 8) and health insurance coverage (yes, no). Age was used as covariate in the total sample and as a stratifying variable to see differences among the different age groups. Age was categorized as: young adult (18–34 years old), midlife (35–64 years old) and older (65 years or older).
Data Analysis
All analyses were performed using IBM® SPSS Statistics version 26.0. Given the complex sampling design and weighting methodology of the BRFSS, all analyses were done with the SPSS Complex Samples module to account for survey weights and design variables. Bivariate associations between age groups and categorical variables were evaluated using design-adjusted chi-square (χ2) tests; continuous variables were compared using Design-adjusted Wald F-tests. For continuous QOL outcomes, poor physical health days, poor mental health days, and health-related activity limitation days, multivariable linear regression models were used to assess associations with caregiving intensity, duration, and type of caregiving labor. Self-rated general health status was analyzed using multivariable ordinal logistic regression, given its ordered response categories. Depression status, a binary outcome, was analyzed using standard logistic regression.
Results
Sample Characteristics
The Characteristics of U.S. Family Caregivers by Age Groups, 2024 Behavioral Risk Factor Surveillance System (N = 2,610)
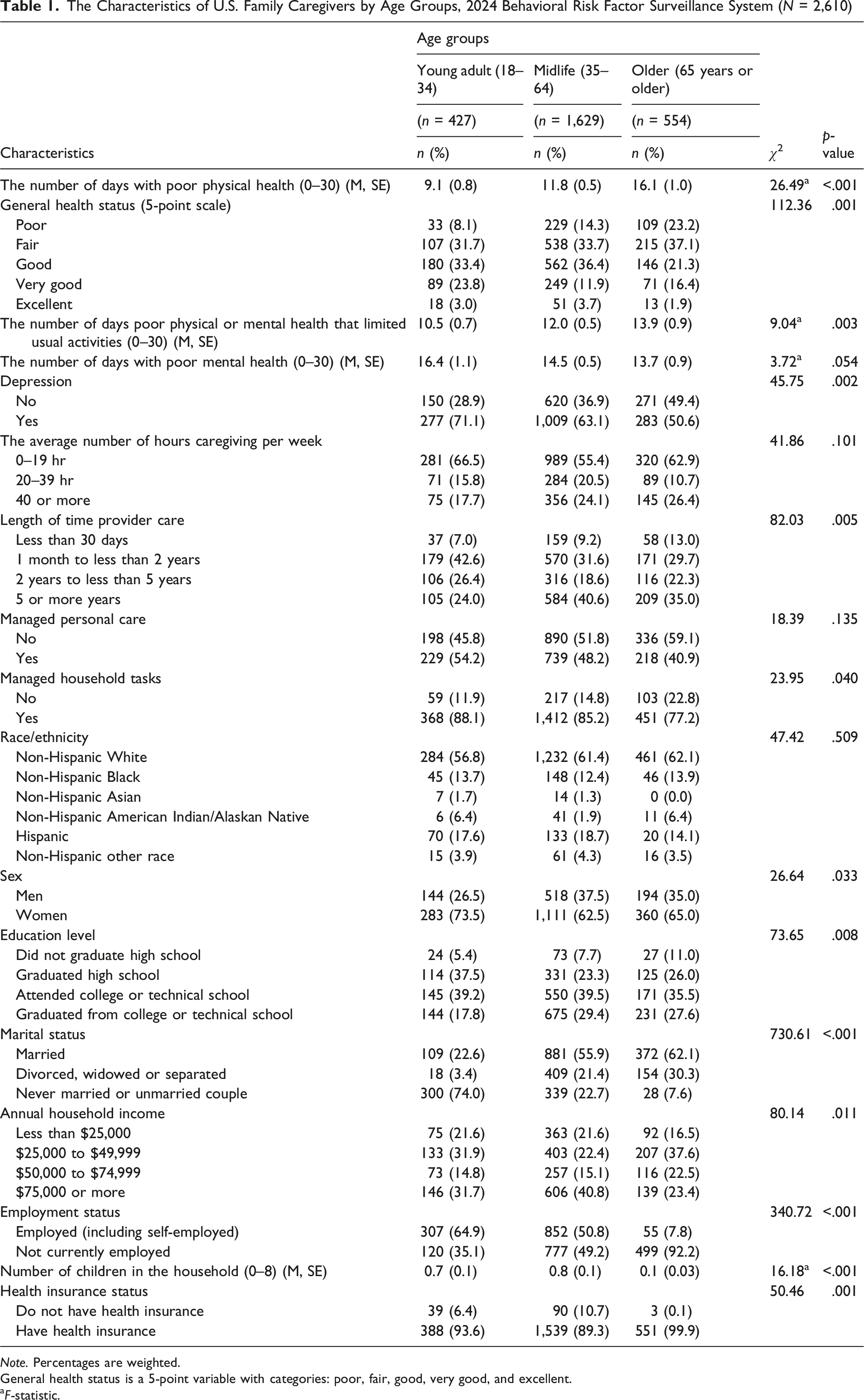
Note. Percentages are weighted.
General health status is a 5-point variable with categories: poor, fair, good, very good, and excellent.
aF-statistic.
Age groups differed significantly in duration of caregiving role (χ2 = 82.03, p = .005). These variables capture accrued caregiving responsibilities over the course of participants’ lives. Age groups differed significantly in the type of caregiving role relating to household task management (χ2 = 23.95, p = .040). Age group varied significantly by sex (χ2 = 26.64, p = .033). Women represented a majority of FCGs across life-course stages: 73.5% of young adult, 62.5% of midlife, and 65.0% of older caregivers sampled were women. As expected, given our U.S. population-based sample, sociodemographic characteristics differed across life-course groups. Midlife and older caregivers were more likely to be married compared with young adults; similarly, young and midlife caregivers had higher household incomes than older caregivers who were more likely to be retired. Education, employment status, presence of children in household, and insurance coverage also differed by age group (all p < .05; see Table 1). These age-graded differences in sociodemographics are consistent with previous population-based descriptions of U.S. adults and were thus included as covariates across multivariable models.
Poor Physical Health Days
The Association Between Caregiving Intensity, Duration, Type of Labor and the Number of Days With Poor Physical Health Among U.S. Family Caregivers, 2024 Behavioral Risk Factor Surveillance System
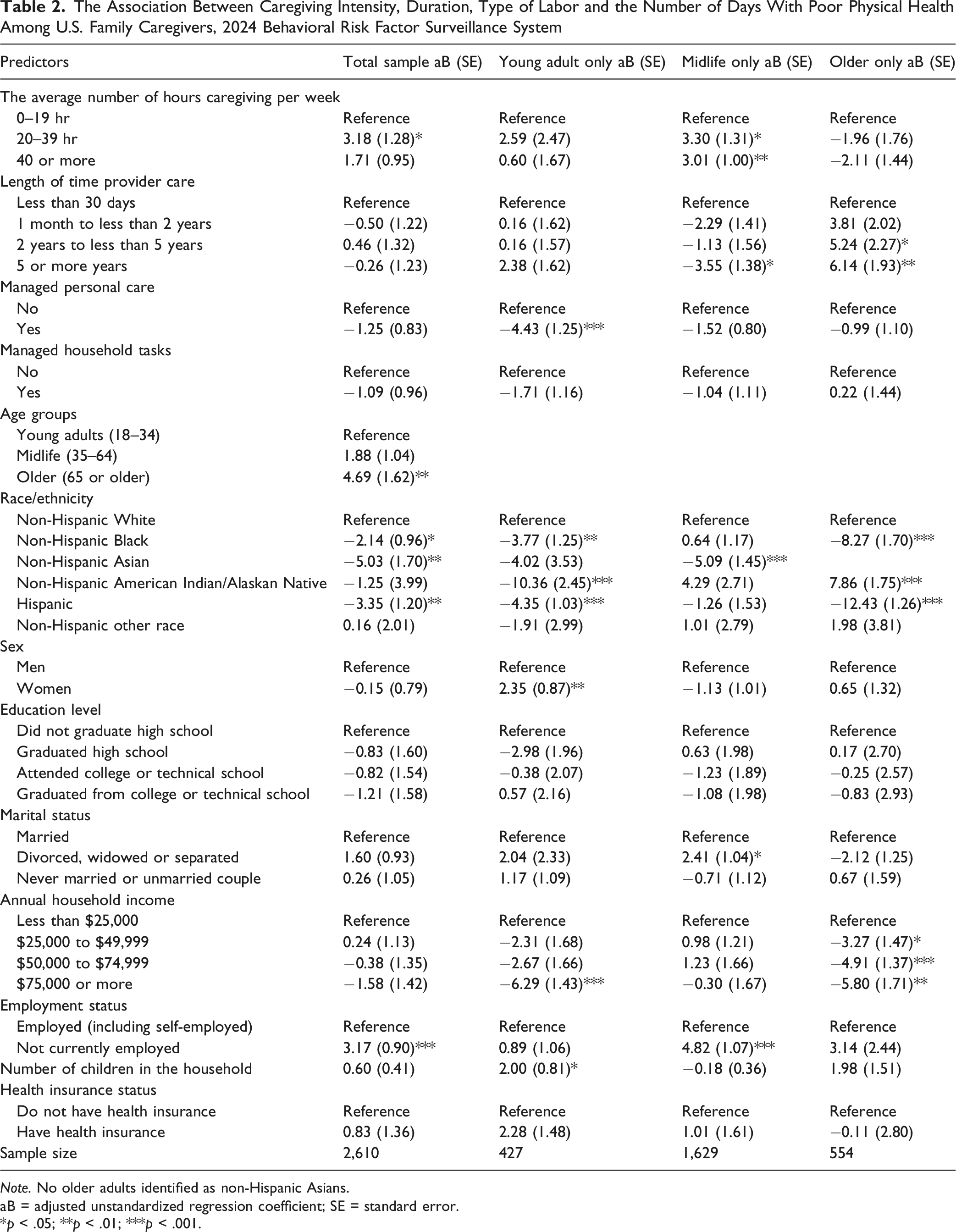
Note. No older adults identified as non-Hispanic Asians.
aB = adjusted unstandardized regression coefficient; SE = standard error.
*p < .05; **p < .01; ***p < .001.
Among stratified age models, several factors were associated with poor physical health days by life-course stage. In young adulthood, managing personal care of their family member was associated with fewer poor physical health days (aB = −4.43, SE = 1.25, p < .001). Having an income of $75,000 or more was associated with better physical health across household income categories compared with those caring for a parent with less than $25,000 income annually (aB = −6.29, SE = 1.43, p < .001). FCGs that had children in the household had a higher prevalence of poor physical health days than those who did not have children in the household (aB = 2.00, SE = 0.81, p < .05).
For midlife FCGs, giving 20–39 hr (aB = 3.30, SE = 1.31, p < .05) or 40 or more hours of care per week (aB = 3.01, SE = 1.00, p < .01) was associated with more poor physical health days. Caregiving for over 5 years had fewer poor physical health days than caregiving for less than 30 days (aB = −3.55, SE = 1.38, p < .05). Compared with non-Hispanic White midlife FCGs, non-Hispanic Asians (aB = −5.09, SE = 1.45, p < .001), reported fewer poor physical health days. Midlife FCGs who were divorced, widowed, or separated had more poor physical health days than married FCGs (aB = 2.41, SE = 1.04, p < .05). FCGs who were not employed versus employed had more poor physical health days (aB = 4.82, SE = 1.07, p < .001). Among older adult FCGs, providing care for 2–5 years (aB = 5.24, SE = 2.27, p < .05) or more than 5 years (aB = 6.14, SE = 1.93, p < .01) was associated with more days of poor physical health compared with caregivers who provided care for less than 30 days. Compared with non-Hispanic White older adults, non-Hispanic Blacks (aB = −8.27, SE = 1.70, p < .001) and Hispanics (aB = −12.43, SE = 1.26, p < .001) had fewer poor physical health days. Conversely, American Indian or Alaska Native had more poor physical health days than their White counterparts (aB = 7.86, SE = 1.75, p < .001). Income was positively associated with poor physical health days across all income categories when compared with less than $25,000 annually for older FCGs.
General Health Status
The Association Between Caregiving Intensity, Duration, Type of Labor and Ordered General Health Status Among U.S. Family Caregivers, 2024 Behavioral Risk Factor Surveillance System
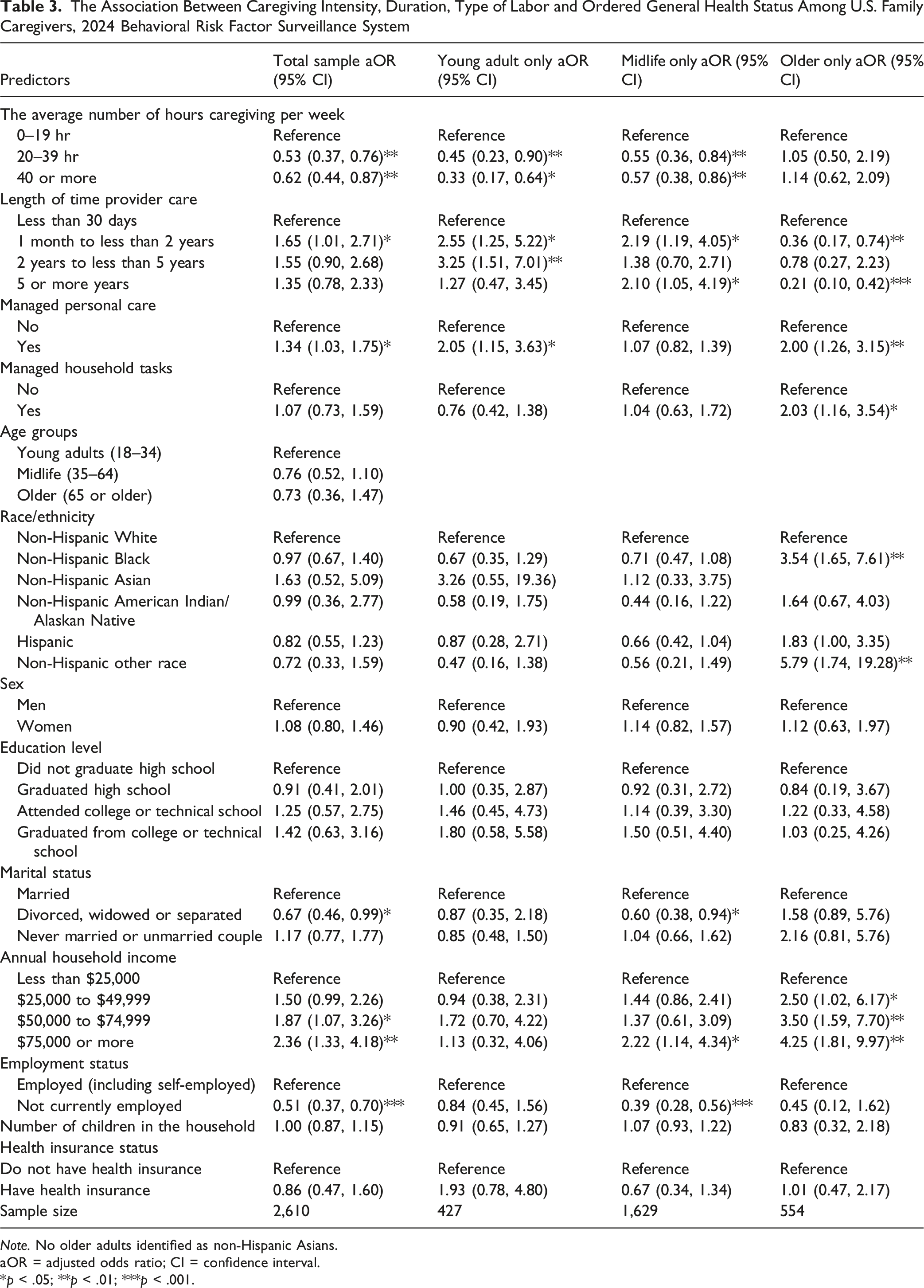
Note. No older adults identified as non-Hispanic Asians.
aOR = adjusted odds ratio; CI = confidence interval.
*p < .05; **p < .01; ***p < .001.
Among stratified age groups, caregiving for 20–39 hr per week or more was associated with poorer general health among young adult and midlife FCGs. Among young adult FCGs, those who provided care for 1 month to less than 2 years (aOR = 2.55, 95% CI = 1.25, 5.22) and 2–5 years (aOR = 3.25, 95% CI = 1.51, 7.01) had higher odds of reporting better general health status. Midlife FCGs who provided care for 5 years or more were more likely to report better general health than those who provided care for less than 30 days (aOR = 2.10, 95% CI = 1.05, 4.19). Among older FCGs, caregiving for 1 month or more was associated with poor general health, including those who provided care for 5 years or more (aOR = 0.21, 95% CI = 0.10, 0.42). Compared with managing their parent’s personal care, managing household tasks was associated with higher odds of better general health status among older FCGs (aOR = 2.03, 95% CI = 1.16, 3.54). Higher income was positively associated with reporting better general health status among midlife and older FCGs.
Activity-Limiting Poor Physical or Mental Health Days
The Association Between Caregiving Intensity, Duration, Type of Labor and the Number of Days Poor Physical or Mental Health That Limited Usual Activities Among U.S. Family Caregivers, 2024 Behavioral Risk Factor Surveillance System
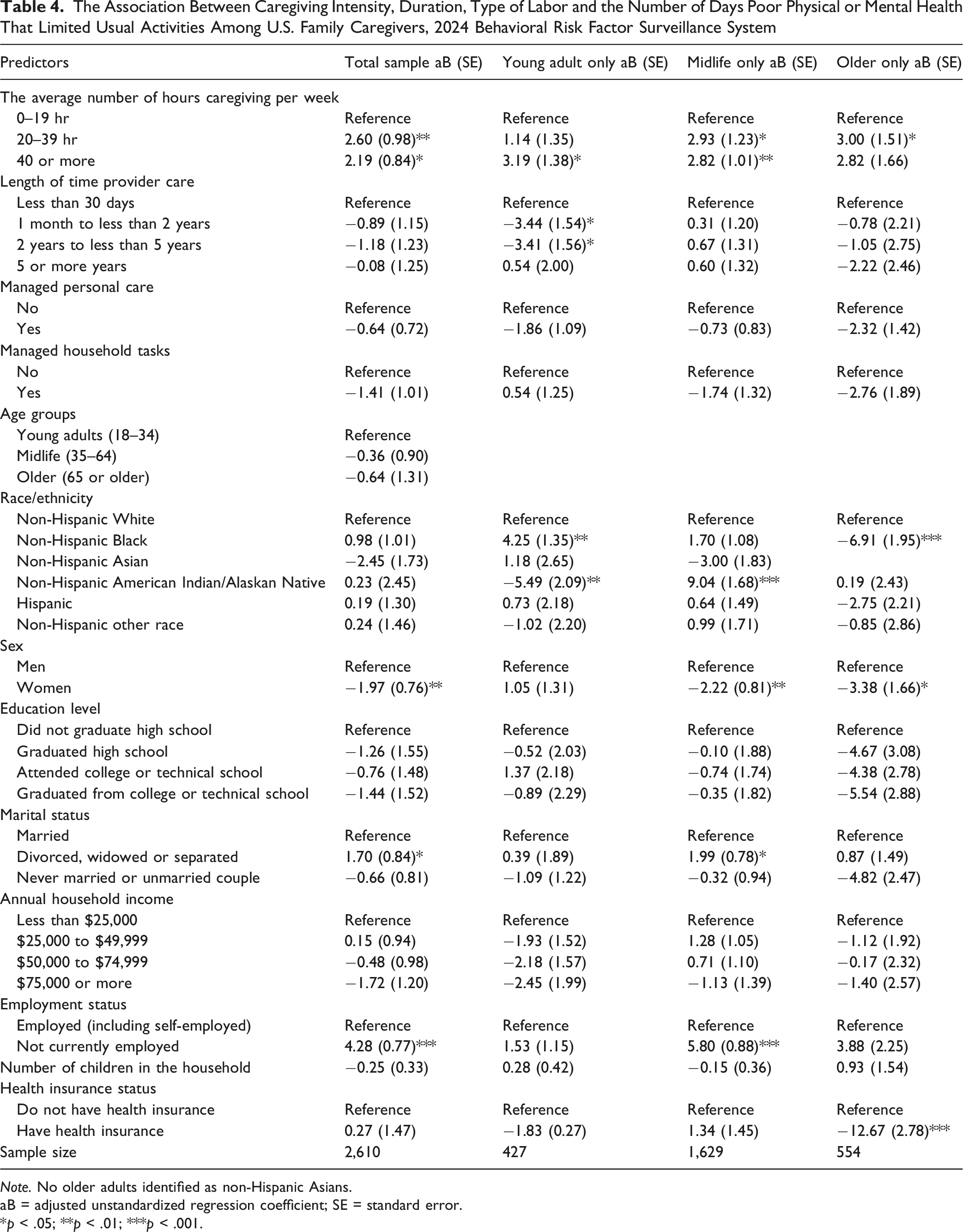
Note. No older adults identified as non-Hispanic Asians.
aB = adjusted unstandardized regression coefficient; SE = standard error.
*p < .05; **p < .01; ***p < .001.
Among age-stratified groups, providing care for 20–39 hr per week was associated with more days of activity being limited among midlife and older FCGs. Providing 40 hr or more of care was associated with more days of activity being limited among young adult and midlife FCGs. Among young adults, providing care for 1 month to less than 5 years was associated with fewer days of poor physical or mental health limiting activity compared with those who provided care for less than 30 days (1 month to less than 2 years: aB = −3.44, SE = 1.54, p < .05; 2 years to less than 5 years: aB = −3.41, SE = 1.56, p < .05).
Midlife female FCGs had fewer days of poor physical or mental health limiting usual activities when compared with midlife male FCGs (aB = −2.22, SE = 0.81, p < .01). Midlife FCGs that reported being divorced, widowed or separated reported more days of poor physical or mental health limiting usual activities than those who were married (aB = 1.99, SE = 0.78, p < .05). Midlife FCGs who were not employed versus employed had more days of activity limited by poor physical or mental health (aB = 5.80, SE = 0.88, p < .001). Compared with non-Hispanic White older FCGs, non-Hispanic Blacks reported fewer days of activity limited by health (aB = −6.91, SE = 1.95, p < .001). Among older FCGs, having health insurance coverage was associated with fewer days of activity limited by poor physical or mental health (aB = −12.67, SE = 2.78, p < .001).
Poor Mental Health Days
The Association Between Caregiving Intensity, Duration, Type of Labor and the Number of Days With Poor Mental Health Among U.S. Family Caregivers, 2024 Behavioral Risk Factor Surveillance System
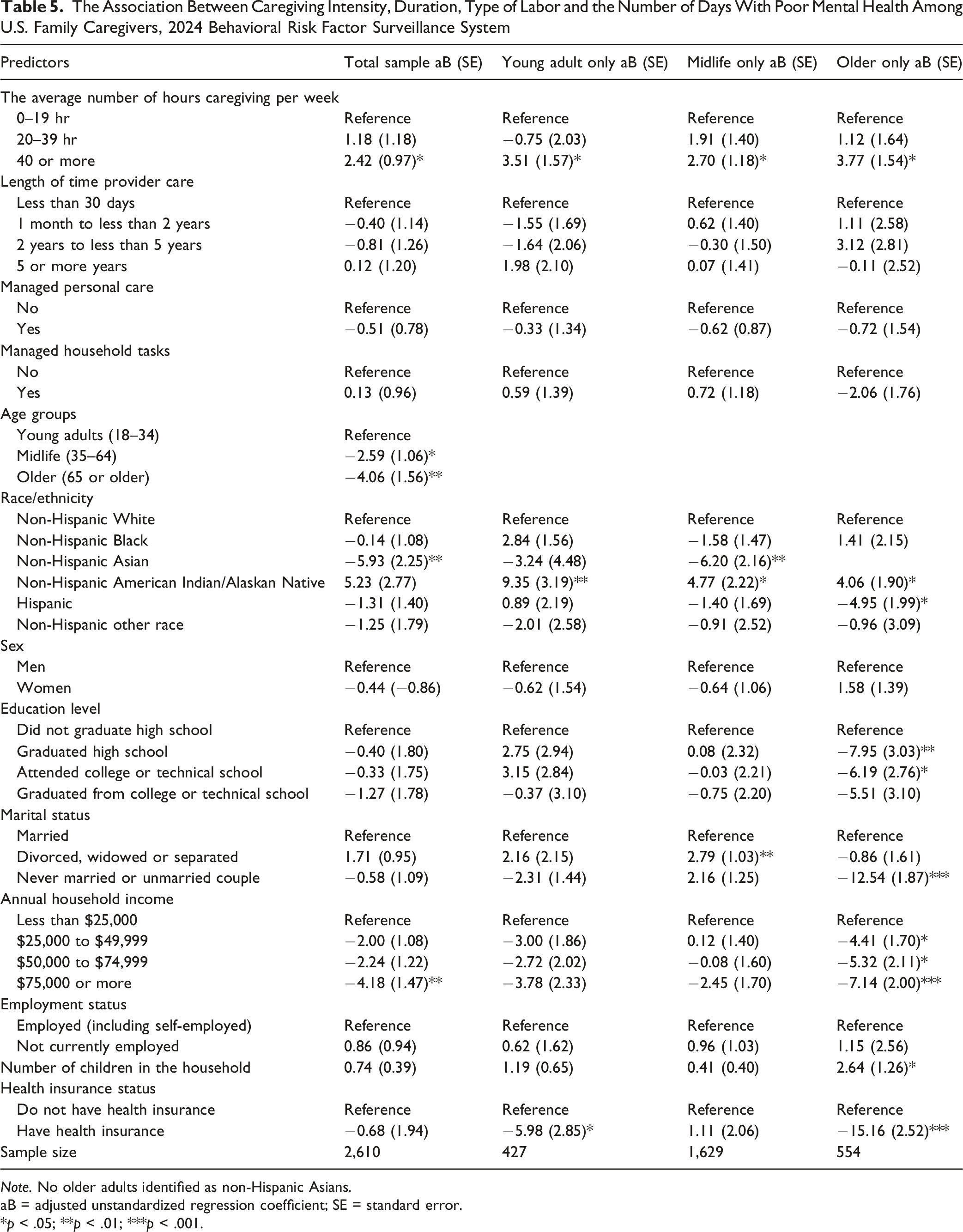
Note. No older adults identified as non-Hispanic Asians.
aB = adjusted unstandardized regression coefficient; SE = standard error.
*p < .05; **p < .01; ***p < .001.
In age-stratified regression models, providing 40 hr or more of care per week was associated with more poor mental health across all age groups. Among American Indian or Alaska Native adults, there were more poor mental health days for young adults, midlife and older ages. Among older FCGs, Hispanic race was associated with fewer poor mental health days compared to their White counterparts (aB = −4.95, SE = 1.99, p < .05). Lack of health insurance was associated with more poor mental health days among young adults and older FCGs. Among older FCGs, higher education level (graduated high school: aB = −7.95, SE = 3.03, p < .01; attended college or technical school: −6.19, SE = 2.76, p < .05) and never being married (aB = −12.54, SE = 1.87, p < .001) were associated with more poor mental health days. However, income was positively associated with poor mental health days across all categories when compared with those making less than $25,000 per year. Older FCGs who made more than $25,000 reported more days of mental health challenges in the last 30 days.
Depression
The Association Between Caregiving Intensity, Duration, Type of Labor and Depression Status Among U.S. Family Caregivers, 2024 Behavioral Risk Factor Surveillance System
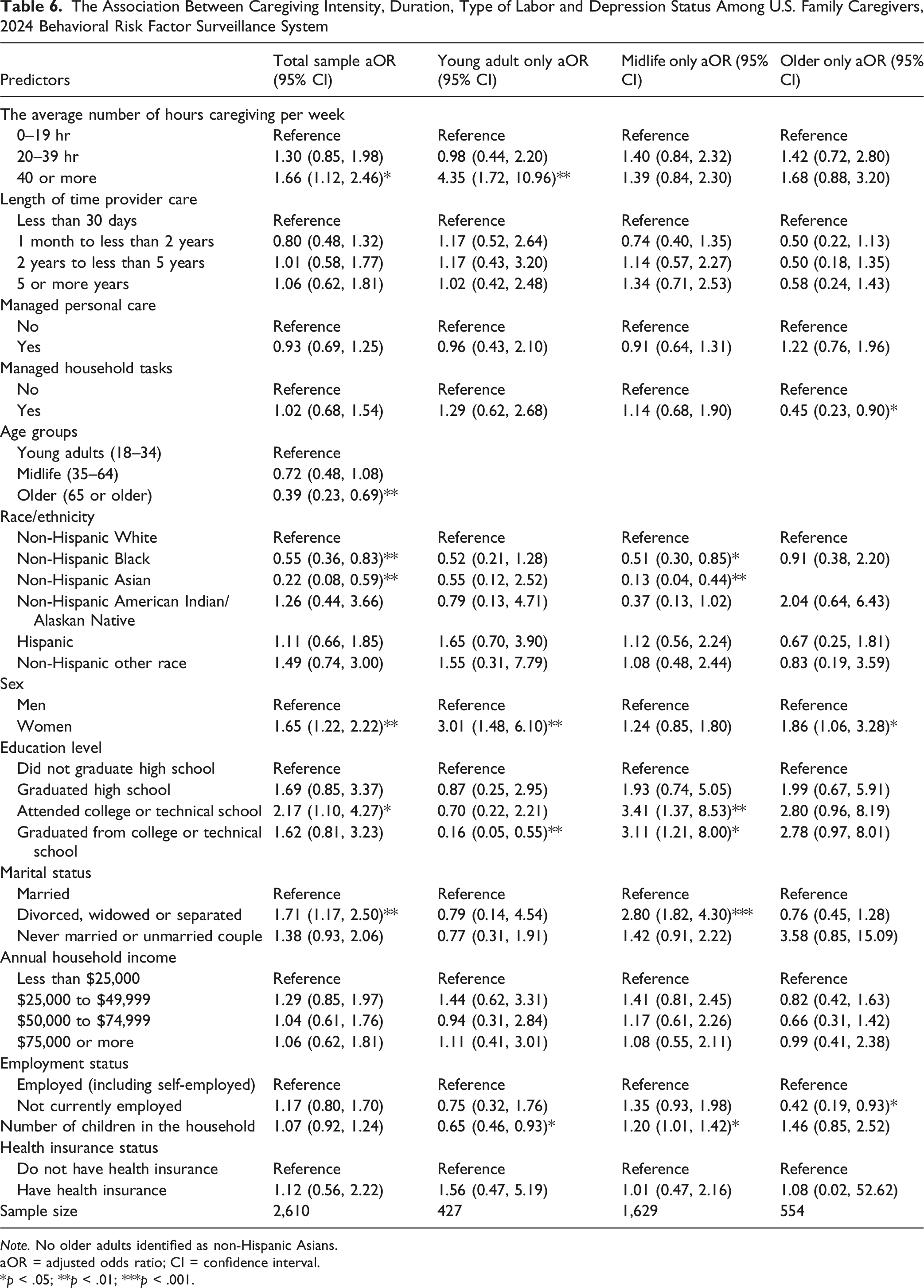
Note. No older adults identified as non-Hispanic Asians.
aOR = adjusted odds ratio; CI = confidence interval.
*p < .05; **p < .01; ***p < .001.
In age-stratified regression models, providing care for 40 hr or more per week was associated with higher odds of depression among young adult FCGs (aOR = 4.35, 95% CI = 1.72, 10.96). Among midlife FCGs, those who were divorced, widowed, or separated had higher odds of depression than those who were married (aOR = 2.80, 95% CI = 1.82, 4.30). Having a higher education level (attended college or technical school: aOR = 3.41, 95% CI = 1.37, 8.53; graduated from college or technical school: aOR = 3.11, 95% CI = 1.21, 8.00) was associated with higher odds of depression among midlife FCGs. Among older FCGs, managing household tasks of their family member (aOR = 0.45, 95% CI = 0.23, 0.90) and not being employed (aOR = 0.42, 95% CI = 0.19, 0.93) was associated with lower odds of depression.
Discussion
This study examined how caregiving intensity, duration, and type of caregiving labor are associated with multiple indicators of QOL among FCGs in the United States, including whether and how such relationships differed by respondents’ life-course stage. Among this nationally representative cross-sectional sample, older FCGs had the strongest relationship between long-duration caregiving and physically unhealthy days. Even though we can’t establish the temporal order with this dataset, the pattern offers both clinical and theoretical significance. Specifically, the finding that both two to less than 5-year caregiving and five-plus-year caregiving was associated with substantially more physically unhealthy days among older FCGs, but not among younger FCGs mirrors predictions from a wear-and-tear model of caregiver health. In this framework, chronic caregiving is hypothesized to accumulate biologic deficits that over time may lead to more rapid declines in health; the current cross-sectional findings fit that scenario, but cannot address it (Schulz & Sherwood, 2008). Notably, this pattern of results among older caregivers may also stem from the life-course principle of cumulative disadvantage. Given the confluence of caregiving with age-related chronic illness, diminished physical reserve, and decreasing social support throughout old age (Cho et al., 2024; Keramat et al., 2025), long-duration caregiving may represent less of an “additional responsibility” and more of a “stress multiplier” for older adults. Recent population-based estimates of the relationship between caregiving and health have converged on this conclusion, illustrating that it is the responsibility associated with high-intensity, long-duration caregiving, not caregiving per se, that is linked to higher rates of morbidity and mortality (Roth et al., 2015). These high-risk FCGs, in particular, older individuals who provide care for five or more years, are chronically exposed to the stressors of caregiving labor, such that the associated health profile may be difficult to reverse without intervention. Results from the present study underscore the need for clinical and policy initiatives that target this population.
Sex-stratified analyses revealed women experienced substantially higher odds of depression than men at each life-course stage, after adjustment for intensity, duration, employment, and income. Structural explanations are warranted over residual ones for this pattern. Unpaid care labor should be expected from gendered institutions of labor, norms, and welfare state arrangements that delegate primary caregiving responsibilities to women (Ervin et al., 2022; Glucksmann, 2016; Pinquart & Sörensen, 2003). Women perform care work more intensively than men, take it on for longer periods, and are more likely to cut back on paid work hours or leave the workforce entirely to provide it, enduring wage, pension, and health penalties along the way that their male counterparts in similar caregiving situations do not experience (Glucksmann, 2016; Krämer & Bleidorn, 2024). The structure of the U.S. care economy depends on the unwaged labor of women, particularly women of color and immigrant women and the health burden described here is the predictable result of that dependence. The competing activity-limiting result, where women reported fewer such days as men, is best interpreted in juxtaposition to the depression model: among caregivers in this sample, the gendered health burden of care is borne primarily as psychological distress rather than functional limitation that interrupts daily activities. Women may push through caregiving and household responsibilities during periods of health issues that men are more likely to report as activity limiting, though future research should measure this possibility directly.
Higher levels of caregiving intensity were consistently associated with increased odds of poor health across life-course stages. Providing between 20–39 hr of care or 40 or more hours of care per week was associated with more poor physical health days, poorer self-rated health, more activity limitations, more mentally unhealthy days, and increased odds of depression. These findings align with previous research which has found that FCGs providing full-time or near full-time care report markedly higher rates of chronic fatigue, stress, and depressive symptoms compared to caregivers providing fewer hours of care (Keramat et al., 2025; Oh et al., 2024; Pinquart & Sörensen, 2003). The observed dose-response relationship between caregiving intensity and negative health outcomes further highlights hours of care provided as a key metric for identifying caregivers at risk and intensity thresholds, especially the ≥20 and ≥40 hr/week cut-offs, may be useful for identifying FCGs at risk.
Compared to older FCGs, young adult FCGs had fewer self-reported days of physical health limitations, but experienced significantly more depressive symptoms and mentally unhealthy days. This difference may be due to young adult FCGs disproportionately experiencing mental health strains of caregiving while simultaneously navigating academia, beginning career paths, experiencing financial instability, and starting families (Neller et al., 2024; Ping et al., 2025). Consistent with hypotheses that caregiving relationships are differentially associated with functioning depending on when they occur across the life-course, young adulthood is a time when providing substantial amounts of informal care may disrupt typical role transitions. However, the increased odds of depression among young adult FCGs in this sample support that notion, though the cross-sectional nature of the data means we can’t confirm caregiving preceded the depression. Caregiving may also be more distressing for young FCGs who have less experience managing caregiving stressors and less access to caregiving resources. For young adult FCGs in particular, providing at least 40 or more hours of care per week was associated with over three times the odds of depression.
Midlife FCGs had higher caregiving intensity and relatively higher socioeconomic status, yet more poor physical health days were reported as caregiving hours increased among midlife FCGs. This may be explained by the “sandwich generation” theory where adults in their midlife are responsible for taking care of both aging parents and children while also working (Liang et al., 2024). These conflicting role expectations have been hypothesized to produce role strain and time pressures for self-care, and current correlations between midlife caregiving hours and increased poor physical health days are supportive of this explanation. Non-working midlife FCGs reported more days limited by activity and poor physical health days compared to working midlife FCGs, possibly reflecting time pressure from employment offset by financial security, social interaction, and health benefits.
FCGs who engaged in personal care tasks experienced higher levels of self-rated health, and engagement in household tasks was associated with better general health among older FCGs. This discrepancy may be due to different perceptions of care tasks and social context. Engaging in direct personal care may elicit greater feelings of fulfillment from caregiving or connection to care recipients, which has been found to buffer against caregiver strain under some conditions (Ping et al., 2025). Among older FCGs specifically, household tasks may be perceived as less physically burdensome than hands-on personal care and may allow caregivers to feel more self-efficacious and competent in their caregiving role. Point of care, these findings suggest that older spousal caregivers engaged in high-touch care duties (i.e., bathing, dressing, toileting) may be at particular risk for declines in caregiver health and could particularly benefit from tailored interventions focused on respite and skills-building.
Higher household income was significantly associated with better general health and fewer reported poor mental health days among all participants; however, it was positively correlated with more mentally unhealthy days among older FCGs. This finding may be due to higher-income older adults being more likely to continue working or have other obligations in conjunction with caregiving. Multiple demanding roles are associated with increased psychological strain. A study published this year found that caregivers who reported adjusting their work schedules or responsibilities experienced more stress and financial burden (Clem et al., 2024). Caregivers with more financial stability are not immune to the strains of employment and caregiving.
FCG racial and ethnic disparities in health outcomes suggest that caregivers who identified with minority racial and ethnic groups were less likely to report poor physical health days and depression in comparison to their non-Hispanic White counterparts. These trends were consistent with previous caregiving research (Cantu et al., 2024; Cohen et al., 2024; Pinquart & Sörensen, 2005). Structural factors, such as racialized disparities in labor force participation, caregiving options that are reimbursed by paid leave, and exclusionary policies preventing immigrant groups from historically accessing welfare may play a role in determining who is expected to become an informal caregiver and how care-related health burden among different races and ethnicities. Our findings should be acknowledged within this context and are subject to the following limitations: although there appears to be a health advantage for certain minority FCG groups, this may be partially attributed to the healthy worker effect, also known as the healthy caregiver effect, which hypothesizes that individuals with poorer health are filtered out of the caregiving workforce. This may also mask variations within racial and ethnic groups and differences in access to health resources that are driven by structural inequities. Solely attributing these findings to cultural differences risks essentializing groups and widening structural determinants of health that underlie these gaps.
These findings have implications for health care delivery, aging policy, and caregiver support programs. First, given the robust and graded relationship between caregiving intensity and adverse health outcomes observed across age groups, screening for caregiver burden should be implemented as a matter of routine during health care encounters. This is especially true in primary care, geriatric, and specialty care clinics that primarily care for older adults living with chronic illness. Clinicians with patients who have a high likelihood of dementia, heart failure, cancer, or another disease associated with high caregiving burden should have validated screening protocols in place to identify high-risk FCGs (e.g., those providing 20+ hr/week of care) and refer them to caregiver support resources. Second, the association between time spent caregiving and adverse health among older FCGs suggests a need for longitudinal support for caregivers that does not presuppose an endpoint to the caregiving experience. Caregiver training programs, respite care services, and other interventions should be designed to accommodate those in later stages of the caregiving career. Third, the heightened risk for depression among older adults providing care to a spouse and for women FCGs across the life course indicate an urgent need for mental health resources that are affordable and targeted to caregivers. The National Family Caregiver Support Program and Medicare-funded caregiver interventions should be expanded to better meet the mental health needs of these age-specific groups. Last, current limitations in Medicare and Medicaid coverage of caregiving support services, such as limited allotments of respite care and lack of reimbursement for caregiver training are examples of systemic policy barriers that can and should be addressed to lessen the health burden of informal caregiving among older Americans.
Several limitations should be noted when interpreting the present findings. First, because BRFSS data are cross-sectional in nature, causal relationships between caregiving characteristics and caregiver health cannot be determined. Specifically, given that all measures come from one time-point, no causal inference can be made between aspects of caregiving and health outcomes. Reverse causation, whereby previous poor health influences the type or level of caregiving one provides, cannot be discounted. Second, caregiving constructs and health outcomes were self-reported, resulting in the potential for recall or reporting bias. Third, the BRFSS caregiving module does not account for other caregiving complexities such as caregiving stress, caregiver coping mechanisms or care recipient health condition severity. While BRFSS’s caregiver module does assess caregivers’ relationship to the care recipient, this was outside the scope of the current study. Because caregiving for a spouse may be most common among older adult FCGs and could represent a unique health risk, it will be important for future studies to determine whether relationship to care recipient accounts for some of the association between longer caregiving duration on physical health among older adults. Moreover, longitudinal studies are needed to determine if the relationship between duration and health among older FCGs is better characterized by a threshold model, and if age-stratified interventions reduce health burden associated with intensive caregiving. To our knowledge, this is the first study to examine caregiving intensity, duration, and labor simultaneously using a large nationally representative sample of caregivers, and to report FCG health profiles across three life-course stages.
Conclusion
Given the rapid aging of the US population, the health correlates of family caregiving represent a serious public health concern. We show that how informal care work is distributed (intensity, duration, and type of labor) is associated with health inequities that differ by life-course stage. Older FCGs in the sample demonstrate the physical health profile most closely related to continued caregiving. This finding is in line with the life-course theory of cumulative disadvantage and the wear-and-tear model of caregiver health. Longitudinal data are required to confirm causal interpretation. In contrast, young adult FCGs show the strongest association between intensive caregiving and mental health symptoms and midlife FCGs face the dual challenges of the sandwich generation. Viewing caregiving as a form of unpaid labor, with health correlates akin to demanding employment yet lacking legal safeguards or institutional assistance, allows us to recognize its significance as a public health concern. Concretely, this refers to building upon the unpaid 12-week protections granted by the Family and Medical Leave Act of 1993 (FMLA), which currently leaves out about 44% of U. S. workers due to firm-size and tenure requirements and offers no wage replacement benefits (Brown et al., 2020). Policies abroad can help guide these improvements. Canada’s Compassionate Care Benefit allows workers to take up to 26 weeks of partially paid leave to care for a terminally ill family member through Employment Insurance, in conjunction with job-protections from being fired under both federal and provincial labor laws (Government of Canada, 2024). States such as California, New Jersey, New York, Washington, and Massachusetts have passed laws to provide paid family and medical leave for citizens that includes care for a seriously ill family member, and the 2018 RAISE Family Caregivers Act established the first federal caregiving strategy in the U.S. in 2022 (Administration for Community Living, 2022). The federal government should build on this groundwork by expanding FMLA protections to include small businesses, adding partial wage-replacements for caregivers taking leave from work, and establishing a Medicare benefit that can be used by FCGs for respite or skill-building that scales with hours of caregiving. Without policy change on this level, family caregivers will continue to shoulder the burden that policymakers have refused to share.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.