
Abstract
Medical and dental records of Veterinary Dental Specialties and Oral Surgery were searched to identify dogs that received full metal prosthodontic crowns on canine teeth, using a feather or knife edge preparation between 2005 and 2017. A total of 160 teeth in 84 dogs were included in the study. Current follow-up by telephone, electronic mail, or electronic messaging was conducted, in addition to thorough record review for in-person recheck examinations. Treatment was considered successful if the prosthodontic crown was in place and no further or additional injury to the tooth had occurred at the time of reexamination, owner contact, or patient death. Tooth fracture apical to the prosthodontic crown occurred in 2 (1.25%) cases, bond failure between the tooth and the cement or the cement and the crown occurred in a single case (0.625%), and one metal crown required replacement after 3 years due to wear (0.625%), for an overall failure rate of 2.5%. These results suggest that feather preparation of the margin is at least as, if not more, successful as the more commonly accepted and performed chamfer margin, and thus is a successful, practical and durable option for prosthodontic crown treatment in dog canine teeth.
Introduction
The indications for performing successful prosthodontic crown therapy in small animal patients, in particular dogs, have been fully reported and explained in recent years.1–8 Crown therapy has become a widely accepted treatment option for teeth in canine patients. Indications for prosthodontic crown therapy include teeth that have been worn through attrition or abrasion, or fractured, as well as the teeth of working dogs, or dogs with behavioral predispositions to excessive or potentially damaging use of their teeth (eg, habitual cage chewers, or highly reactive or anxious individuals).3–7,9 Working dogs, particularly those used in bite work, are also frequent candidates for prosthodontic crown therapy. Affected teeth may or may not have been previously treated by root canal therapy.
Historically, recommendations for crown preparation in veterinary patients were extrapolated from human prosthodontics. However, in the past several years, more evidence-based research has become available in veterinary prosthodontics. While there is much work still to be done, the addition of such research to the body of knowledge is of great value. Recent contributions include data regarding tooth surface area, convergence angle, and height:diameter ratio of a tooth.10–12 These properties are related to and affect retention and resistance forms, which has resulted in recommendations for the practitioner based on research, rather than on assumption or extrapolation. 13
Although published studies continue to be scarce, several authors have reported excellent success rates of crowns in dogs. One study assessed 68 crowns in 41 pet and working dogs over a 12-year period and found an 83.5% success rate. 1 Although not a clinical study, examination of the preparation surface area and effects on outcome in 32 crowns found an 84.375% success rate. 10 An earlier clinical study of crowns in working dogs demonstrated an 87.8% success rate over a 2- to 52-month period.3,4
In the past decade, several evidence-based studies have been performed to improve the quality of the information available to veterinary dentists. In addition, there are now studies being published to evaluate prosthodontic techniques, including tooth preparation. 13 We hope to add useful information and data to this growing body with the present study.
There are 3 types of margins commonly used in veterinary crown preparation: bevel, chamfer, and 90° (shoulder). 2 In this study, we aim to demonstrate the success of a specific technique of crown preparation, using a feather or knife-edge margin technique rather than the more commonly employed and widely accepted “chamfer” margin. Personal preference (eg, bur choice) plays a significant role in crown preparation, but in general, a chamfer margin is created by first using a round diamond bur around the circumference of the tooth just above the gingival margin, cutting into the enamel to a depth of 0.5 to 1.0 mm. 5 The primary characteristic of the chamfer margin is the rounded internal line angle created with the round diamond bur as described above. 2 Shoulder margins, or 90° margins, are recommended for porcelain fused to metal (PFM) restorations, and may be created with a flat-end cylinder diamond bur.2,5 The axial portions of the tooth are then removed to the depth of the margin and shaped to create a smooth preparation, with no unsupported enamel or undercuts.
Any margin angle other than 90° is considered a bevel. The feather margin is a bevel margin of greater than 70°. 2 Anecdotally, feather preparations are faster and easier to perform, take impressions of, and finish, and because less tooth structure is removed in this preparation the remaining tooth is stronger and more resistant to fracture. 5 Crown preparation should remove as little enamel and/or dentin as is necessary, allowing space for a prosthodontic crown to fit without contacting other teeth, and eliminating enamel undercuts. 14 Enamel thickness in dogs is inconsistent, varying from 0.1 to 0.6 mm across a tooth, and the cervical bulge is an area of tooth thickening, not thicker enamel. 15
When performing feather margin crown preparations, it is not uncommon for the entire preparation to remain within the enamel layer, retaining even greater amounts of tooth structure than preparations extending into the dentin layer. In canine teeth, it is most vital to remove sufficient tooth structure for the prosthetic crown in occlusal areas (the mesial aspects of the maxillary canine teeth, and the mesial and distal aspects of the mandibular canines) to avoid contact between the metal crown and opposing canines and incisors. In non-occlusal areas of the canines, there is generally enough space to allow for minimal enamel removal, even though it may result in a metal crown slightly thicker or larger in these areas than the original, anatomic tooth. Without question, each patient must be thoroughly evaluated for bite, tooth spacing, and any preexisting malocclusion, and canine teeth prepared for prosthetic crowns that will comfortably accommodate an individual animal's anatomy. Our results show that feather preparation is at least as successful as the chamfer margin preparation most commonly taught and performed in veterinary prosthodontics.
Materials and Methods
A search of digital patient records at Veterinary Dental Specialties and Oral Surgery (VDSOS) was conducted to identify all patients that received full metal crown placement between 2005 and 2017. Records included patients receiving treatment by 1 of 4 veterinarians at any one of multiple practice locations. Three veterinarians were trained in feather preparation technique by the fourth veterinarian, a board-certified veterinary dentist.
Necessary criteria for study inclusion were: full metal crowns to one or more canine teeth, complete dental records for crown preparation and placement, follow up at least one year after crown placement by either in person examination, telephone, or electronic mail or messaging. Phone and/or email contact was attempted with each client between November 2018 and January 2019, and only those with whom contact was made, and/or which had reexamination performed by a VDSOS veterinarian, are included in the study data. Owners were asked whether the crown was currently in place, or still in place at the time of the pet's death (at least one-year post cementation), and whether they were pleased with the outcome of the procedure.
Medical and dental records were reviewed to determine which tooth was treated, the reason for treatment (fracture or wear), pet dog versus working dog (bite work, Schutzhund, police/military), whether endodontic treatment was performed, and length of time the prosthodontic crown remained in place from time of cementation. Data were summarized and compared where appropriate with 2-sided Fisher exact tests using GraphPad Prism 7.0. Statistical significance was considered as P < .05.
All teeth received full metal crowns. 73 of 160 teeth (45.63%) were treated endodontically (standard root canal treatment; no surgical root canal or vital pulp therapy cases are included) prior to prosthodontic crown placement. All teeth were prepared with a diamond-coated coarse grit flame point crown preparation bura on a high-speed, water-cooled drill, removing as little tooth structure as possible, while creating enough space for a prosthetic crown with a thickness of 1.0 to 1.5 mm, that would not interfere with occlusion. Horizontal margins were a feather (>70° bevel) margin. Margins were placed approximately at or no greater than 0.5 mm coronal to the gingival margin, using the flame point of the bur to create a smooth, consistent margin, 0.5 to 1.0 mm deep. Coronal tips of intact canines were blunted, removing approximately 1.0 mm of tooth, and careful attention applied to the occlusal aspects of the tooth to remove enough tooth structure to allow for the expected 0.5 to 1.5 mm thickness of the final prosthetic crown. Axial tooth structure was then gently and gradually reduced using smooth motions and the central portion of the bur, around the full circumference of the tooth, again, with particular attention paid to occlusal surfaces (Figure 1). It was generally not necessary to remove a full 1.0 mm of the entire tooth surface. No post and core procedures were performed, nor were any partial crowns. Detailed impressions were made using vinyl polysiloxane putty and wash materialb (Figure 2), partial or full mouth impressions with alginatec, and bite registration with polysiloxane putty. Dental stoned was used to create models. Alginate impressions and stone models were produced in the clinic by veterinarians and staff. All prosthodontic crowns were cast by the same labe, using a titanium metal alloyf, (72% nickel, 13% chromium, 5% molybdenum, 4.2% titanium, 2.0% aluminum) (Figures 3 and 4). All prosthodontic surfaces in contact with the tooth were sandblasted as part of the production and preparation process in the lab. Prosthodontic crowns were cemented by one of the same 4 veterinarians, using the same resin-based luting cementg. No temporary crowns were placed in any patient.
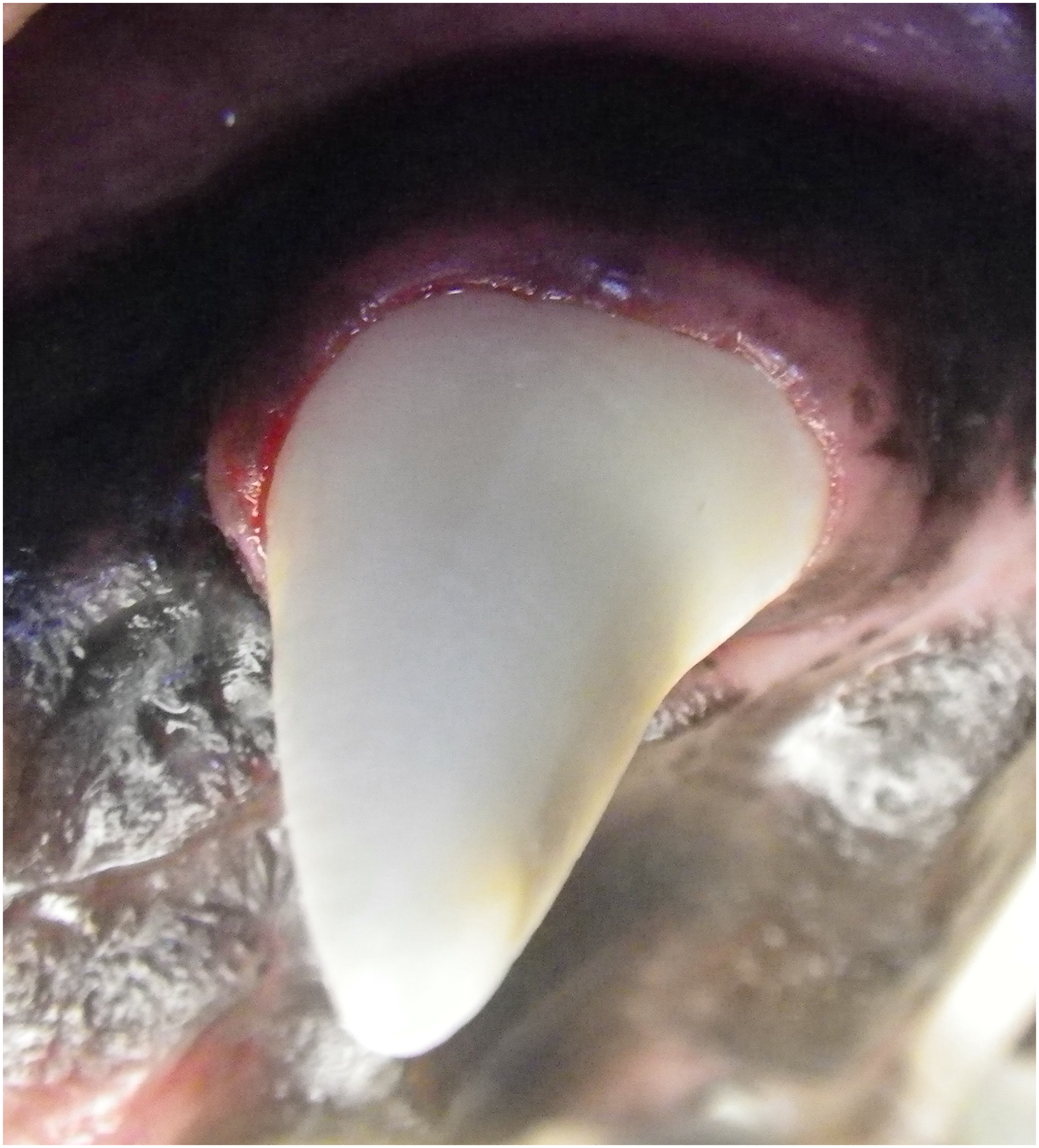
Example of feather edge crown prep, tooth 204 (photo courtesy R. Furman).
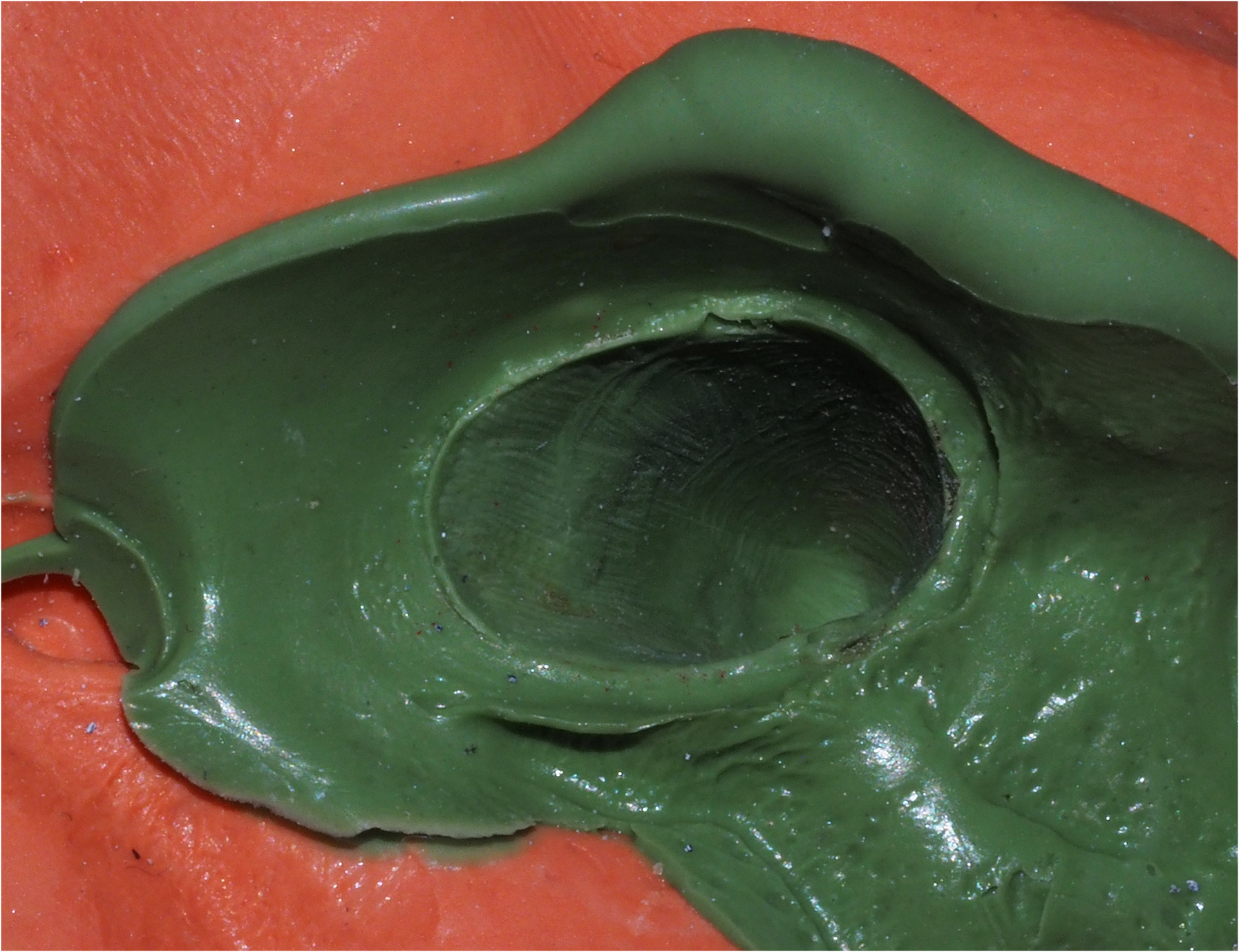
Example of prepared tooth impression (photo courtesy R. Furman).

Die fabricated from impression in Figure 2 (photo courtesy of precision ceramics).

Metal crown on die in Figure 3 (photo courtesy precision ceramics).
Materials
aMaxima diamond bur, flame, coarse grit, Henry Schein, Inc., Melville, NY.
bExpress, 3M ESPE Dental Products, St. Paul, MN.
cAlginate.
dSnap Stone, Whip Mix Corporation, Louisville, KY.
ePrecision Ceramics Dental Laboratory, Montclair, CA.
fTilite Premium, Talladium, Inc., Valencia, CA.
gPanavia 21, Kuraray Noritake Dental, Inc., Okayama, Japan.
Results
Our initial search revealed 339 cast metal full coverage prosthodontic crowns placed on the canine teeth of 202 dogs during the 13-year period of the study. Of these, a total of 84 dogs and 160 canine teeth had complete records to meet study criteria, including adequate follow-up. Where a crown was lost and replaced with a new crown, this was counted as 2 cases (n = 1). Only patients with follow-up at least 12 months after crown placement were included in the study. Crowns placed less than 12 months prior to owner contact (December 1, 2018, to January 15, 2019) were not included, nor were crowns that were only rechecked less than 12 months after initial cementation. No failures were noted prior to 12 months in the records review. Of the 49 crowns still in place when rechecked under anesthesia by a veterinarian, 67.3% were examined 12 to 36 months after cementation, and 89.8% were examined before 5 years post cementation. The remaining 5 (10.2%) teeth were rechecked between 7 and 10 years. The median duration of crown retention based on veterinarian rechecks was 29 months with a range of 12 to 114 months.
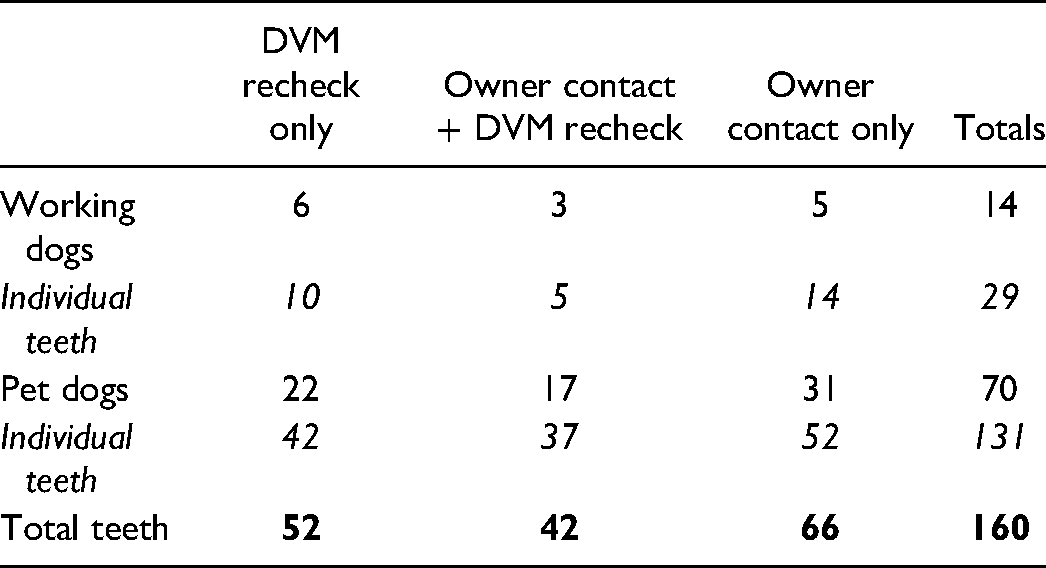
A total of 84 dogs and 160 canine teeth are included in the study. Most patients were classified as pets (70 dogs, 120 teeth). The remaining 14 patients, representing 29 teeth, were classified as working dogs (police/military, or other bitework/Schutzhund training). Twenty-two pet dogs (42 teeth) and 6 working dogs (10 teeth) were rechecked by a veterinarian in a practice location at least 12 months after initial cementation of the crowns. Email or phone contact was made with owners of 56 other dogs, representing 108 crowned teeth (8 working dogs, 19 teeth), none of which are represented in the 28 dogs included in the veterinarian recheck group. For 20 dogs (42 teeth), including 3 working dogs (5 teeth), owner contact was made in addition to veterinarian recheck records (Table 1).
Distribution of Included Teeth Between Working and Pet Dogs and Method of Confirming Presence or Absence of Crown (1 Year Minimum Follow-Up).
Two crowns were lost secondary to tooth fracture apical to the prosthodontic crown, one was lost to bond failure, and a fourth was removed and replaced with a new prosthodontic crown (new impressions were taken and a completely new crown manufactured) when the dog wore through the original metal crown.
Overall failure rate is 2.5% (4 of 160 teeth). Owner reported data (2 of 108 teeth) failure rate is 1.85%, and the veterinarian rechecks failure rate 3.85% (2 of 52 teeth). The 2 reporting methods were compared, using a 2-sided Fisher exact test, and no significant difference was found between owner-reported results and those checked by a veterinarian (P = .5963).
The 2 reporting methods were then combined and no statistically significant differences were found in maxillary versus mandibular canines (80 crowns each jaw, 2 failures each jaw) for a 2.5% failure for each, P = 1.0000). Neither was there any statistically significant difference between right or left sides (2.44% left, 2.56% right, P = 1.0000). Again, with Fisher exact test, no statistically significant difference was found (P = 1.0000) in failure rates between teeth treated endodontically prior to crown preparation and placement and those not treated endodontically.
In the veterinarian recheck group, the duration of crown retention ranged from 12 to 114 months (mean 34.23, median 29). Owner reported duration was from 20 to 161 months; owner-reported data for dogs that had also had at least one veterinarian recheck median 47 months with a range of 25 to 161. For owner reported data only, median 45 months with a range of 20 to 108. Deceased pets for which we could not be certain of the actual duration of crown retention were not included in mean nor median calculations for any group.
We compared our 97.5% success of crown preparations with feather margin, to the 92.16% success (47 of 51 teeth) of crown preparations with chamfer margins in an earlier paper, only making a comparison to canine teeth with full metal crowns (excluding PM4 s [n = 5] and partial crowns [n = 12]) from total numbers and from failure data, and the difference is not statistically significant (P = .0985). 1 When we exclude the worn crown and compare again (159 teeth, 3 failures), there is a strong trend towards greater success (P = .0609), though still not statistically significant, than for the chamfer prepared teeth. The data clearly show that the feather preparation is at least if not more successful than the more commonly accepted and performed chamfer margin.
Discussion
Neither described type of failure (fracture apical to the crown, bond failure) is unique to our preparation design or execution. Rather, these are typical failures for prosthodontic crown procedures in veterinary patients. We did not find other reports of a canine patient wearing through a metal crown, so this type of failure is either extremely rare, or unreported. In our patient, all 4 canine teeth were treated with full metal crowns for significant abrasion. One of the 4 original crowns showed signs of wear, with tooth visible through the worn metal, but was still in place after 39 months. The replacement crown lasted at least another 46 months, intact, before the patient was lost to further follow-up. Although we have included this case as a crown failure, the fact that crowns on the other 3 canine teeth in this same patient lasted 85 months or more, suggests that this could have been a failure of the crown material or manufacture itself.
Fractured teeth are frequently encountered in small animal practice. Little data are available on the prevalence of traumatic dentoalveolar injuries (TDI), which includes luxation as well as other dental injuries in dogs and cats. One study found that 26.2% of dogs and cats have at least one TDI, and that crown fractures constitute four-fifths of all TDI in dogs and cats. 16 In addition to tooth fracture, abrasive damage, behavioral characteristics, training, and/or work-related causes may also be indications for prosthodontic crown treatment. A prosthodontic crown is a cemented extracoronal restoration that covers the entire surface of the clinical crown. 17 Crown placement is indicated to protect and strengthen weakened teeth, and to restore function. 9
As veterinary dentistry matures and gains recognition in the pet-owning population, prosthodontic crown therapy will also continue to grow. Our ability to successfully apply proper planning and treatment must grow as well. Much work has been done in recent years to improve the quality and quantity of evidence-based research available on the subject. Although it was widely established that smaller convergence angles increase retention and resistance form, 13 it wasn't until 2011 that a study demonstrated that the clinically achievable convergence angle in canine teeth of dogs is actually much higher than previously recommended, and it provided evidence-based data for current and future recommendations. 11 Others investigated the effect of preparation surface area, and the use of axial grooves on dislodgment of metal prosthodontic crowns.10,18 The study showing the influence of crown height to diameter ratio on the force of fracture in dog canine teeth has also contributed to the growing body of literature upon which we may base future studies, and it has allowed improvement in clinical techniques. 12
The feather preparation is the most conservative of all margin preparation techniques, and may remain completely within enamel layers, without extending into dentin; it is therefore possible that significant surface area is retained. This was not, however, specifically investigated in the present study, and testing this is beyond our means and expertise. Although not statistically significant, one study did support a relationship between greater preparation surface area and improved crown retention. 10 Additionally, by not exposing dentinal layers, it may be presumed that the prepared tooth is less sensitive, leading to less patient discomfort while awaiting crown manufacture and cementation.19,20
The retrospective nature of the current study has several shortcomings. None of the aforementioned evidence-based research was available for the vast majority of the treatment planning, preparation, or implementation in patients in our dataset. Medical records are only as good as each individual completing them, and each veterinarian, technician, or receptionist may have different methods and habits of completion; though we aim for consistency and completeness as a practice group, medical records do occasionally fall short. Photographs and radiographs were not available for every case, nor at every recheck date, though what was available was consistent with the findings of overall success. Although great care was taken in selecting a comparison group, the current study would be strengthened by having a direct comparison of chamfer and feather margin preparation within the same practice group, rather than by comparison with a previous study from a separate institution.
Previous studies determined success or failure with similar follow-up methods to those used here, including telephone,1,3,4 electronic mail, 1 or in-person examination. 1 The study in which the methods most closely align with the current study did not specify whether in-person examinations were conducted in conscious or anesthetized patients. 1 As all veterinarian rechecks for this study were conducted in anesthetized patients, close examination of the crown fit and margin was achievable, as well as complete evaluation of the gingival margin for inflammation, or recession that could potentially arise from the metal prosthetic crown; no issues were noted in any of these patients.
The average thickness of the full metal prosthetic crowns used in this study is 1.0 to 1.5 mm. The minimum axial and occlusal thickness the lab will cast is 1.0 mm; thinner crowns risk creation of a defect if or when any adjustments to the fit may be necessary. The finish line of the marginal preparation is accurately identified at the lab as all dies are trimmed under high powered microscopes. All dies used in prosthetic crowns manufactured for this study were trimmed by highly skilled and experienced (>20 years) technicians. Under- or over-contoured restorations may lead to chewing issues, occlusal challenges, jaw problems, painful patients, and unhappy clients.
A concern regarding the near marginal preparation of these teeth is that it may result in gingival inflammation and eventual recession. However, these are not subgingival preparations and do not impinge on the biologic width. Subgingival crown preparations are not recommended, and if biologic width may be impinged upon, crown lengthening procedures are recommended. 5 Biologic width is “the combined width of the connective tissue and the epithelial attachment to the tooth above the crestal alveolar bone.”5,21 Interference with or impingement on biologic width (approximately 2.5 mm from the restoration margin to the crestal bone) leads to periodontal inflammation, and a physiologic response to reestablish biologic width.5,20 Subjectively, the feather preparation is relatively easy to perform, and the marginal or near-marginal placement is more cosmetic than the frequently recommended 1 to 2 mm supragingival margin (Figure 5). 2 In those teeth for which photographic and radiographic evidence was available, the examining veterinarian did not find any evidence of increased periodontal attachment or bone loss in these teeth at any time.

Example of metal crown after cementation in a study patient (author photo).
The current and similar future studies would benefit from a prospective approach, with regular, complete, anesthetized recheck exams, and clear measurements of biologic width, gingival inflammation, or recession. A large number of patient records reviewed for the current study were excluded for lack of follow-up, as all rechecks were entirely dependent on clients returning to our facilities for recommended annual prophylaxis and dental radiographs. It is possible there were additional failures of which we are unaware because of this reliance on client motivation and financial commitment.
Conclusion
The feather margin is at least as successful as the chamfer margin for preparation of canine teeth undergoing prosthodontic crown treatment in dogs, and therefore is an acceptable alternative to chamfer margin preparation.
Footnotes
Acknowledgments
Many thanks to Katherine Phillippi-Falkenstein, MPH for statistical analysis, Traci M. Timmons, RVT, and Carly E. Rando, RVT for data compilation assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.