
Abstract
Tooth extraction is the most common oral surgical procedure performed in human and veterinary dentistry. One possible complication during extraction is root fragment displacement into adjacent anatomical spaces. Root fragment displacement into adjacent anatomical spaces can lead to serious side effects including pain and infection; therefore, displaced fragments should be removed when possible. Root fragment removal techniques from the mandibular canal have not been studied in veterinary or human dentistry. A reported complication of dental implant placement in humans is displacement into the mandibular canal, and techniques have been developed to remove these displaced implants. This report compares 2 techniques to remove displaced root fragments from the mandibular canal in canine cadavers based on previously published methods to remove displaced dental implants from the mandibular canal in humans.
Introduction
Tooth extraction is the most common oral surgical procedure performed in human1-3 and veterinary dentistry. 4 In human dentistry removal of the maxillary and mandibular third molars, “wisdom teeth,” is the most common indication for extraction.2,5 These teeth are commonly removed to treat pericoronitis, caries and to prevent future problems such as inability of normal tooth eruption.6,7 In veterinary medicine, tooth extractions are most commonly performed to treat periodontal disease.4,8
The goal of tooth extraction is to completely remove the entire tooth while avoiding unnecessary damage to the surrounding hard and soft tissues. 4 Unfortunately, complications can occur during the extraction procedure and have been described in both the veterinary and human literature. Reported veterinary extraction complications include fractured roots, displacement of root fragments, hemorrhage, trauma to soft tissues, mandibular and maxillary fractures, oronasal fistula, ophthalmic complications, air embolism, and nerve damage.4,9 Noted human extraction complications are soft tissue injuries, abrasion or burn, root fracture, root fragment displacement, injury to adjacent teeth, mandibular fracture, nerve injury, oroantral communication, temporomandibular joint injury, and hemorrhage. 10 While an accurate prevalence of all extraction complications is not known, complications have been reported to be between 2.65% and 30.9% of human patients that were treated with third molar extraction 7 and in one published report the incidence of retained roots following extraction of the maxillary fourth premolars and mandibular first molar was 82% in dogs and 93% in cats. 11
Extraction complications in humans have been reported to be due to either patient or clinician related factors. 12 Patient-related factors include unfavorable anatomic features (e.g., tooth resorption, periapical pathology), and proximity of the root to anatomical areas such as the maxillary sinus or mandibular canal. Clinician related factors include limited oral surgical skills, insufficient visual and radiological analysis, improper use of instruments, and application of excessive force. Most cases of tooth extraction complications in humans are the result of clinician related factors. 12 Similarly, in veterinary medicine extraction complications are often attributed to clinician-related factors including lack of appropriate preoperative assessment, improper instrumentation, and not having the required knowledge or skills for the extraction.4,9
Placing dental implants has become a common procedure in human dentistry to replace missing teeth. 13 While dental implants have been shown to be beneficial in humans their use in veterinary patients is unjustified. 14 Similar to tooth extraction, complications can occur during implant placement including hemorrhage, nerve damage, mandibular fractures, damage to adjacent teeth and displacement of the implant into adjacent anatomical spaces.15,16
The displacement of tooth and implant structures into adjacent anatomical areas is considered a rare complication in human dentistry,3,15,17,18 and there are only a few isolated clinical cases of displaced tooth structures documented in the veterinary literature.19-21 Even though the existence of reported complications of displaced root fragments and dental implants is rare in humans it can have significant side effects including pneumonia, septic thrombosis, sinusitis, 22 sinus aspergillosis,23,24 pain,5,15,22-29 trismus,5,15,18,28 altered nerve sensation,2,10,17,30-32 infection,10,19 hemorrhage,16,33 and death. 7 Clinical signs noted in veterinary patients of displaced tooth structures include sneezing,19,21 nasal discharge,19,21 gingival recession, 20 tooth discoloration, 20 and tooth mobility. 20 Pain is the most common clinical sign in human patients with displaced tooth structure or dental implant.5,15,22-29 Since the physiologic process of pain is similar in animals and humans, when a condition is painful in humans, such as a displaced root, it can be speculated it will also be painful in animals. 34 Even though a displaced root fragment will likely be a source of pain in an animal, their behavioral response to that pain may not be noticeable due to an evolutionary survival mechanism where disguising pain can be the difference between life and death. 35 Because displaced root fragments in humans 22 and animals 4 and displaced implants in humans 27 can be associated with potentially serious side effects, removal is recommended unless the surgical procedure poses severe medical risk to the patient.
Displacement of mandibular root fragments during extraction has been briefly mentioned as an extraction complication in the veterinary literature and there is only discussion of displacement into the mandibular canal.4,9 It is the experience of the authors that when mandibular roots are displaced into adjacent anatomical spaces during extraction, displacement is typically into the mandibular canal. Removal techniques for displaced root fragments from the mandibular canal in animals have been only briefly described. 9 A technique has been published to remove the roots of mandibular third molar teeth in humans after crown amputation when the root apices involve the mandibular canal. The described technique does not mention its use in the retrieval of root fragments that have been displaced into the mandibular canal during extraction. 36 One case report has been described in the human literature for a displaced root fragment in the mandibular canal but the surgical technique used for retrieval was not described. 25 Displacement into and retrieval of dental implants from the mandibular canal in humans has been described by multiple sources13,15-18,26,30,31,33,37,38 and may serve as a model for removal of root fragments displaced in the mandibular canal of veterinary patients.
Techniques to remove displaced dental implants from the mandibular canal can be broadly classified into crestal and lateral surgical techniques. 30 When crestal techniques are utilized the implant is retrieved by surgical access through the alveolus from the alveolar margin in an apical direction. This is accomplished by enlarging the opening of the alveolus so the displaced implant can be visualized and then removed. When lateral techniques are utilized, surgical access to the displaced implant is created through the overlying buccal mandibular bone by making a “window” or hole through which the displaced implant can be removed. Technique selection depends on location of the displaced implant and surgeon's preference. 30
This report describes and compares the use of crestal, and lateral techniques adapted from previously reported techniques for removal of displaced dental implants in humans to remove displaced root fragments in the mandibular canal of canine cadavers.
Materials and Methods
Ten cadaver dog heads were acquired from a commercial osteological suppliera for this study. The sex, weight, age, and breed were not available. All specimens appeared to be from large breed dogs. Ethical approval was not required for this study as the specimens were obtained from a commercial source for purposes unrelated to this study.
Study Design
Inclusion in the study required the cadaver specimens to have both right and left mandibular third premolars, fourth premolars and first molars. To be included, these teeth could not have signs of alveolar bone loss, tooth resorption, ankylosis, periapical pathology, or structural abnormalities that would prevent the tooth from being extracted and a root fragment being displaced into the mandibular canal at the site of the distal root of the right and left mandibular fourth premolars.
Oral examination including dental probing, dental radiographsb and cone beam computed tomography (CBCT)c of right and left mandibular third premolars, fourth premolars and first molar teeth was performed to screen the specimens and ensure they met all the requirements for inclusion in the study. All dental radiographs obtained during the study were exposed using the parallel technique, 39 and images were viewed using a commercially available software programd. The CBCT scans were performed with the specimens resting on a carbon-fiber radio-clear extension platform manufactured for the scanner. The long axis of the mandibles was placed parallel to the platform. A standard scanning protocol was used resulting in a 0.3 mm voxel size, 24 Å∼ 14 cm field of view, 120 kVp, 57.6 mAs and 20 s of acquisition time. Viewing of the CBCT images was performed using the same acquisition softwaree.
The left and right mandibular fourth premolars were surgically extracted using well-established and accepted techniques 40 by author MTB. Vertical buccal alveolar bone removal was standardized (4 mm) during extraction to maintain consistent post extraction alveolar bone height between specimens. Post extraction dental radiographs were obtained to ensure complete removal of the teeth. The length of the distal root was measured from the cementoenamel junction to the apex with calipersf and recorded. The apical 4 mm of the distal root was measured with calipers, marked with a surgical marker and removed with a crosscut fissure carbide burg and the root fragment was saved for later experimental use.
The specimens and corresponding root fragments were frozen for preservation for the subsequent experimental phase of the study at which time the specimens were thawed for 24 h at room temperature (22 °C).
Root Displacement
A communication was created from the alveolus of each distal mandibular fourth premolar into the mandibular canal. The alveolus of the mandibular fourth premolars was arbitrarily selected for the study due to ease of root fragment displacement into the mandibular canal. Alveolus communication with the mandibular canal and root fragment displacement were performed by author SMM.
The goal in creation of the communication was to allow displacement of the root fragments with mild to moderate apical force. First an awlh was placed into the apical portion of the alveolus and moderate apical pressure placed by hand to create an initial communication to the mandibular canal. Then a series of pin punchesi−k (Figure 1) increasing in diameter from 1.5 mm to 3.2 mm and a nail setl were used similar to the awl to enlarge the opening to a consistent diameter of 3.2 mm. If the resistance of the apical alveolus was too great to push the pin punch into the mandibular canal by manual force, a mallet was used to gently tap the pin punch through the floor of the alveolus. A dental radiograph was obtained to ensure the final pin punch had entered the mandibular canal. The previously sectioned distal root fragment was placed into the corresponding alveolus and then displaced into the mandibular canal by applying apical pressure with a dental elevatorm until the root fragment was displaced into the canal. No effort was made to displace the root fragment into any specific location within the canal. An intraoral dental radiograph was obtained to ensure the root fragment was displaced in the mandibular canal and completely free from the alveolus. After confirmation that the root fragments were effectively displaced on the left and right sides of the specimen a CBCT scan was performed as previously described.

Image of pin punches used to create communication from alveolus to mandibular canal increasing in size from top to bottom: 1.5 mm (1/16 inch) diameter; 2.4 mm (3/32 inch) diameter; and 3.2 mm (1/8 inch) diameter.
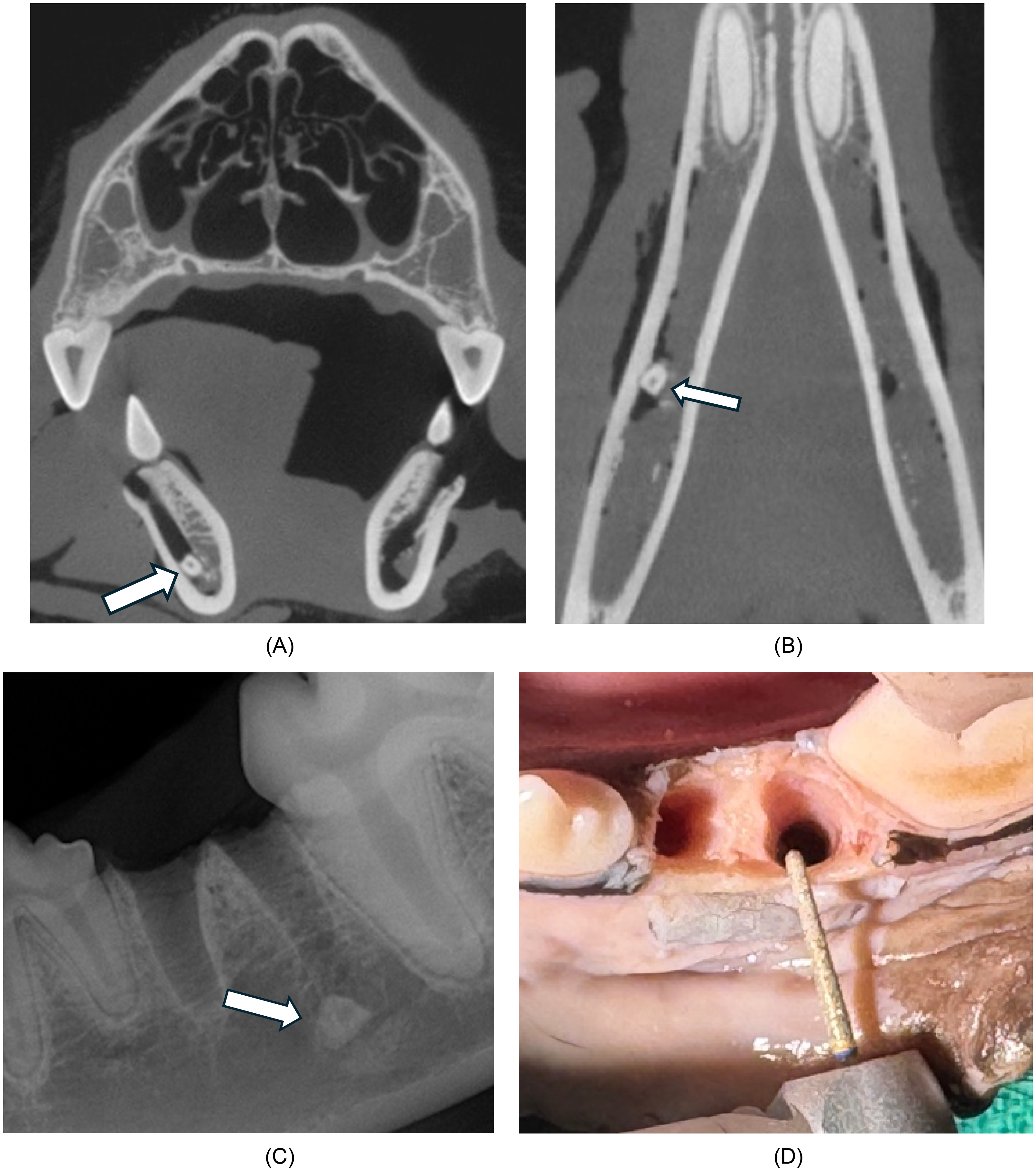
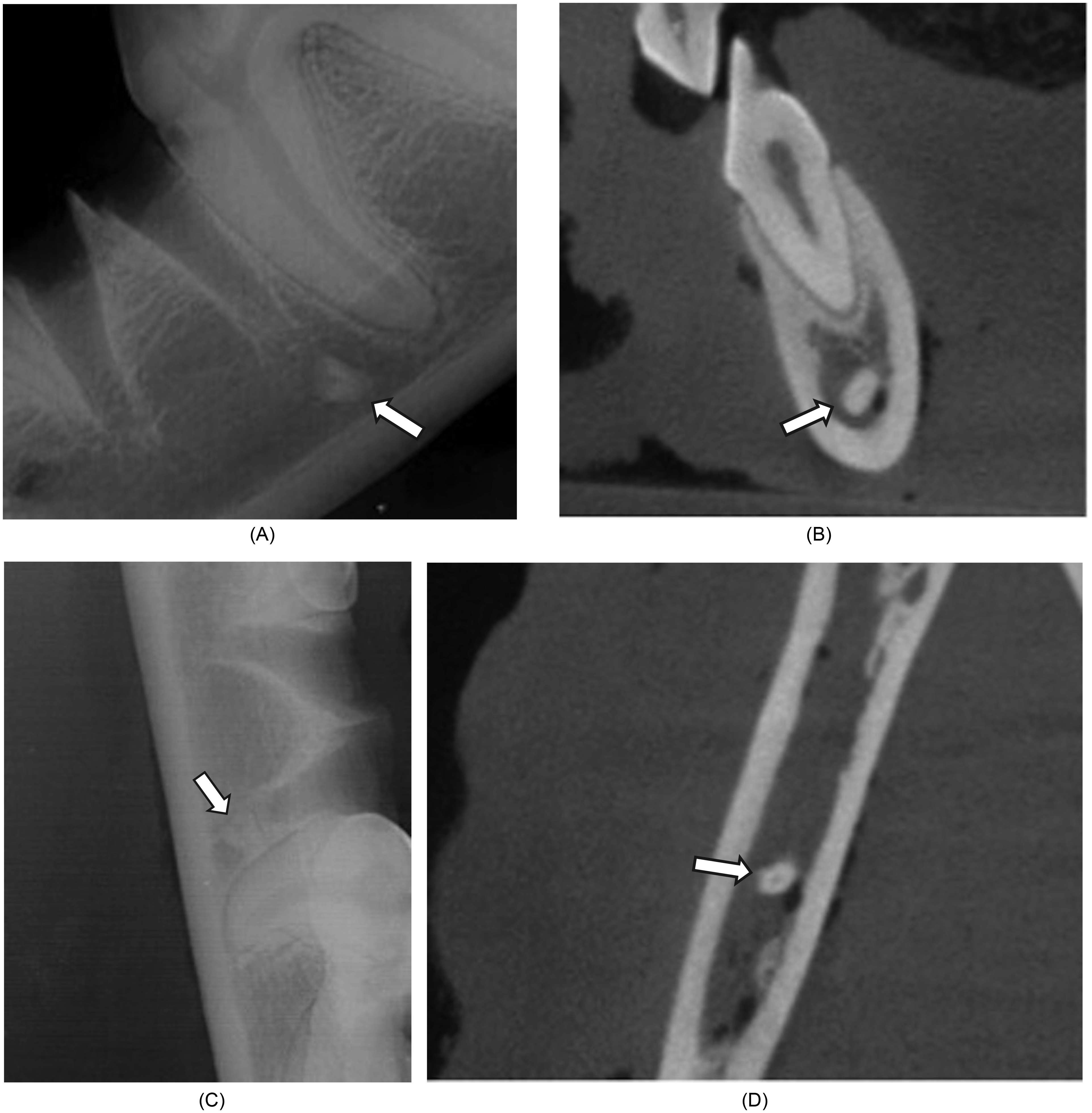
The position of the displaced root fragment in the mandibular canal was radiographically evaluated with intraoral radiographs and CBCT (Figure 2A-D). The CBCT transverse (mesial to distal) and dorsal (dorsal to ventral) planes were used to determine the location of the root fragment in the mandibular canal. In the transverse plane, the root fragment was determined to be displaced either dorsal or ventral in the mandibular canal. The root fragment was considered dorsally displaced when over half of the root fragment was determined to be in the dorsal half of the mandibular canal and ventrally displaced when over half the root fragment was in the ventral half of the mandibular canal. The dorsal plane was used to determine if the root fragment was buccally, lingually, or centrally displaced. The root fragment was considered buccally displaced if over half the root fragment was in the buccal third of the mandibular canal, lingually displaced if over half the root fragment was in the lingual third of the mandibular canal and centrally displaced if over half of the root fragment was in the central third of the mandibular canal. Intraoral radiographs were used to determine the location of each root fragment in relation to the created apical opening of the alveolus to the mandibular canal. If more than half of the root fragment was displaced mesial to the opening of the alveolus to the mandibular canal it was considered mesially displaced. If more than half of the root fragment was displaced distal to the opening of the alveolus to the mandibular canal it was considered distally displaced. If a majority of the displaced root fragment was directly below the opening of the alveolus to the mandibular canal it was considered centrally displaced. The location of the displaced root fragment was recorded in relation to the mandibular canal as a combination of either dorsal or ventral and lingual, buccal, or central. The location of the displaced root fragment in relation to the alveolus was recorded as mesial, central, or distal.

Dog #4. Cone beam computed tomography (CBCT) and intraoral dental radiograph images showing previously extracted left mandibular fourth premolar tooth with displaced root fragment ventral/lingual in mandibular canal and central to alveolus. (A) Transverse image CBCT (arrow shows ventrally displaced root fragment left mandible); (B) Dorsal image CBCT (arrow shows lingually displaced root fragment left mandible); (C) Sagittal image CBCT (arrow shows displaced root fragment left mandible, unable to determine location in relation to alveolus of distal left mandibular fourth premolar); (D) Intraoral radiograph (arrow shows displaced root fragment left mandible, centrally located in relation to distal alveolus).
The specimens were numbered 1 to 10, and R-4 1.0 statistical software 41 was used to randomly assign one of the 2 root retrieval techniques for distal root fragments of right and left mandibular fourth premolars in each specimen. This process ensured random assignment of 5 crestal and 5 lateral root fragment retrievals to left mandibles, and 5 crestal and 5 lateral root fragment retrievals to right mandibles.
Root Retrieval
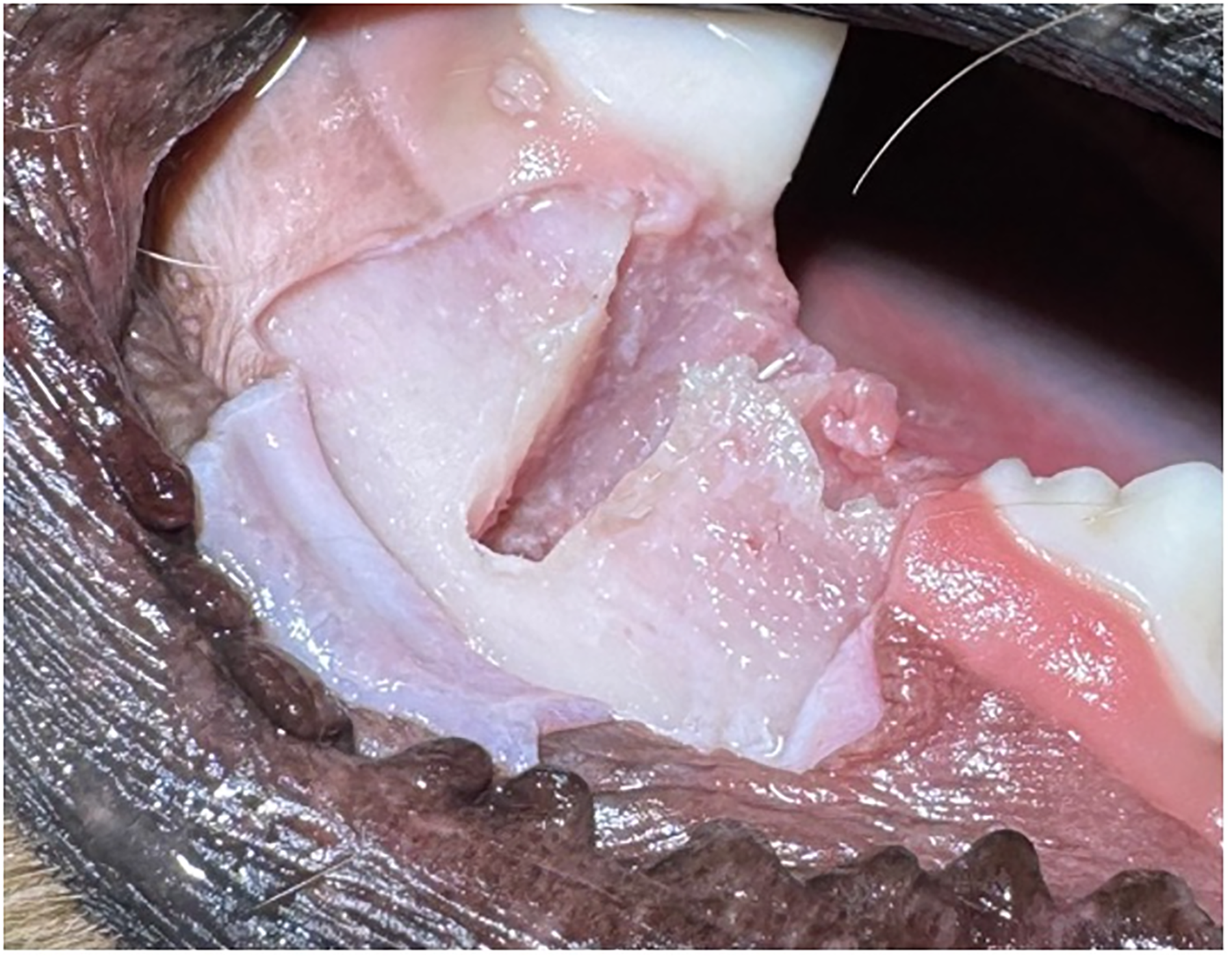
Prior to performing the retrieval techniques, the specimens were positioned and prepared uniformly. The specimens were placed in lateral recumbency with the surgical site facing up. The previously created mucoperiosteal flaps for tooth extraction of the right and left mandibular fourth premolars were extended to the level of the ventral aspect of the mandibular canal. A combination of previously obtained radiographs, CBCT scans and, when possible, direct visualization of the root fragment through the alveolus (Figure 3), was used for both techniques to determine the location of the displaced root fragment in the mandibular canal. Magnification loupes and a head lamp were used to aid in visualization during performance of each technique. A coarse grit round end taper dental diamond burn on a water-cooled high-speed handpiece was used for mandibular bone removal for each retrieval technique. Gentle suction, rather than forced air, was used to improve visualization by removing accumulated water build up from the high-speed handpiece but it was not used to directly aid in removal of the displaced roots during retrieval. In a clinical case use of forced air to clear a surgical dental field of accumulated fluid is not recommended due to the risk of creating an air embolism which could result in death. 9 A periodontal probe was used to gently manipulate and reorient the displaced root fragments as needed so they could be removed with fine tip forcepso. Care was taken in each procedure to limit mandibular bone removal to only what was necessary to identify and remove the displaced root fragment and to avoid neurovascular and adjacent dental structures as much as possible. The root fragment removals were performed by the author MTB.

Photograph of distal left mandibular fourth premolar root fragment dorsally displaced in the mandibular canal visible through alveolus prior to starting retrieval technique.
Crestal Technique
The crestal technique was defined as removal of the displaced root fragment through the original alveolar extraction site. After determining the location of the displaced root fragment (Figure 4A-C), all crestal procedures in this study started with vertical height reduction of the alveolar bone on the lateral aspect of the alveolus. The long axis of the dental bur was placed perpendicular to the alveolar margin (Figure 4D) and light pressure applied on the dorsal crest of the lateral alveolar bone in a mesial to distal motion approximately the width of the alveolus. The vertical bone was reduced until the dental bur had enlarged the previously created communication between the alveolus and mandibular canal (Figure 4E). To enlarge the communication, the dental bur was positioned parallel to the alveolus and advanced ventrally until the tip of the bur made contact inside the dorsal aspect of the communication from the alveolus to the mandibular canal (Figure 4F and G). Light pressure was applied to the bur on the bone to widen the diameter of the alveolus/canal communication while avoiding neurovascular and adjacent dental structures. Vertical bone removal and widening of the diameter of the opening to the mandibular canal was continued until the fine tip forceps could firmly grasp the root fragment and retrieve it (Figure 4H).
Canine cadaver demonstration of the crestal technique to remove a displaced left mandibular fourth premolar root fragment from the mandibular canal. (A) Transverse plane of the cone beam computed tomography (CBCT) shows dorsal displacement of root fragment (arrow) in mandibular canal; (B) Dorsal plane of the CBCT shows buccal displacement of root fragment (arrow) in mandibular canal; (C) Intraoral radiograph shows central displacement of root fragment (arrow) to alveolus; (D) Image of dental bur placement perpendicular to the alveolar margin for vertical bone reduction; (E) Image of lateral mandibular bone after vertical bone reduction; (F) Image showing alveolus and displaced root fragment (arrow) after vertical bone reduction (red circle outlines communication from alveolus to mandibular canal that will be enlarged; (G) Image showing dental bur position in alveolus to enlarge communication to mandibular canal; (H) Image of fine tooth forceps removing displaced root fragment through alveolus.
Lateral Technique
In the lateral technique, the root fragment was retrieved through an access created by removing mandibular bone buccal to the displaced root fragment. The access was created by using a dental bur to remove a circular window of buccal mandibular bone into the mandibular canal over the site of the displaced root fragment. After identifying the location of the displaced root fragment (Figure 5A-D) the tip of the dental bur was placed perpendicular to the buccal aspect of the mandibular bone at the level of the root fragment (Figure 5E). The bur was used to remove bone in a buccal to lingual direction to create an approximately 3 mm wide circular window of bone (Figure 5F). As buccal bone was removed, proximity to the mandibular canal could be determined by the appearance of a dark hue visible through the thinning buccal bone. Care was taken to minimize possible trauma to the neurovascular bundle as the bur came close to entering the mandibular canal. After the mandibular canal was entered and the root tip visualized (Figure 5G), additional bone removal was performed to enlarge the access only as needed to allow root fragment retrieval with fine tip forceps (Figure 5H).
Canine cadaver demonstration of the lateral technique to remove a displaced right mandibular fourth premolar root fragment from the mandibular canal. (A) Transverse plane of the cone beam computed tomography (CBCT) shows ventral displacement of root fragment (arrow) in mandibular canal; (B) Dorsal plane of the CBCT shows central displacement of root fragment (arrow) in mandibular canal; (C) Intraoral radiograph shows mesial displacement of root fragment (arrow) to alveolus; (D) Image of exposed right buccal mandibular bone with star marking location to make access for root retrieval based on imaging; (E) Image of dental bur placement perpendicular to the buccal mandibular bone for lateral technique access; (F) Image showing initial creation of bony window with dental bur; (G) Image showing bony window to mandibular canal with visible displaced root fragment (arrowhead) and neurovascular bundle (arrow); (H) Image of fine tooth forceps removing displaced root fragment through lateral bony window.
Observations and Measurements
The time period to complete each retrieval procedure was measured in seconds using a stopwatch beginning when initial bone removal was started and ending when the root fragment was successfully retrieved with the forceps from the mandibular canal. A grading scale from 1 to 3 was created by the authors to subjectively measure the difficulty of root fragment retrieval and the score recorded for each root: (1) root fragment easy to find and remove by performing the described technique; (2) moderate difficulty to find and remove root fragment due to interference by neurovascular bundle or adjacent dental structures; (3) procedure was difficult to perform and involved considerable additional effort to identify and remove the root fragment.
The dimensions of mandibular bone removed for each procedure were measured using calipers to allow the surface area to be calculated and recorded. The shape of bone removal for the crestal technique approximated a rectangle (Figure 6), so surface area was determined by multiplying height by width. The height (dorsal/ventral) was measured 4 mm from the alveolar crest (post extraction alveolar bone height) to the most ventral aspect of bone removal and width was measured at the widest (mesial/distal) aspect of bone removal. The shape of bone removal with the lateral technique most approximated a circle (Figure 7). The surface area of the bone removed in this technique was determined by measuring the diameter at the widest aspect and then multiplying the square of the radius by “π” (pi) using the formula A = πr², where “A” represents the area and “r” represents the radius of the circle and “π” (pi) is a mathematical constant approximately equal to 3.14159.
Dog #6. Lateral image of the right mandible following crestal technique.

Dog #6. Lateral image of the left mandible following the lateral technique.
Post root fragment removal radiographs and CBCT images were used to verify all root fragments were completely removed. A rectangular area of overlying buccal alveolar bone at the surgical sites was removed to visually evaluate the inferior alveolar neurovascular bundle for obvious damage. An approximately 2 cm wide by 1 cm high full-thickness osteotomy was created through the buccal mandibular bone centered over the root fragment retrieval sites using a crosscut fissure bur. A dental elevator was then used to remove the lateral mandibular bone section to allow visualization of the inferior alveolar neurovascular bundle. The neurovascular bundle was carefully assessed for any visual signs of trauma by authors MTB and SMM and graded on a scale created by the authors of 1-3: (1) no obvious sign of damage (Figure 8A); (2) damage in which the surface of the vessel or nerve appeared traumatized; and (3) trauma in which there was a laceration into the vessel or nerve (Figure 8B).
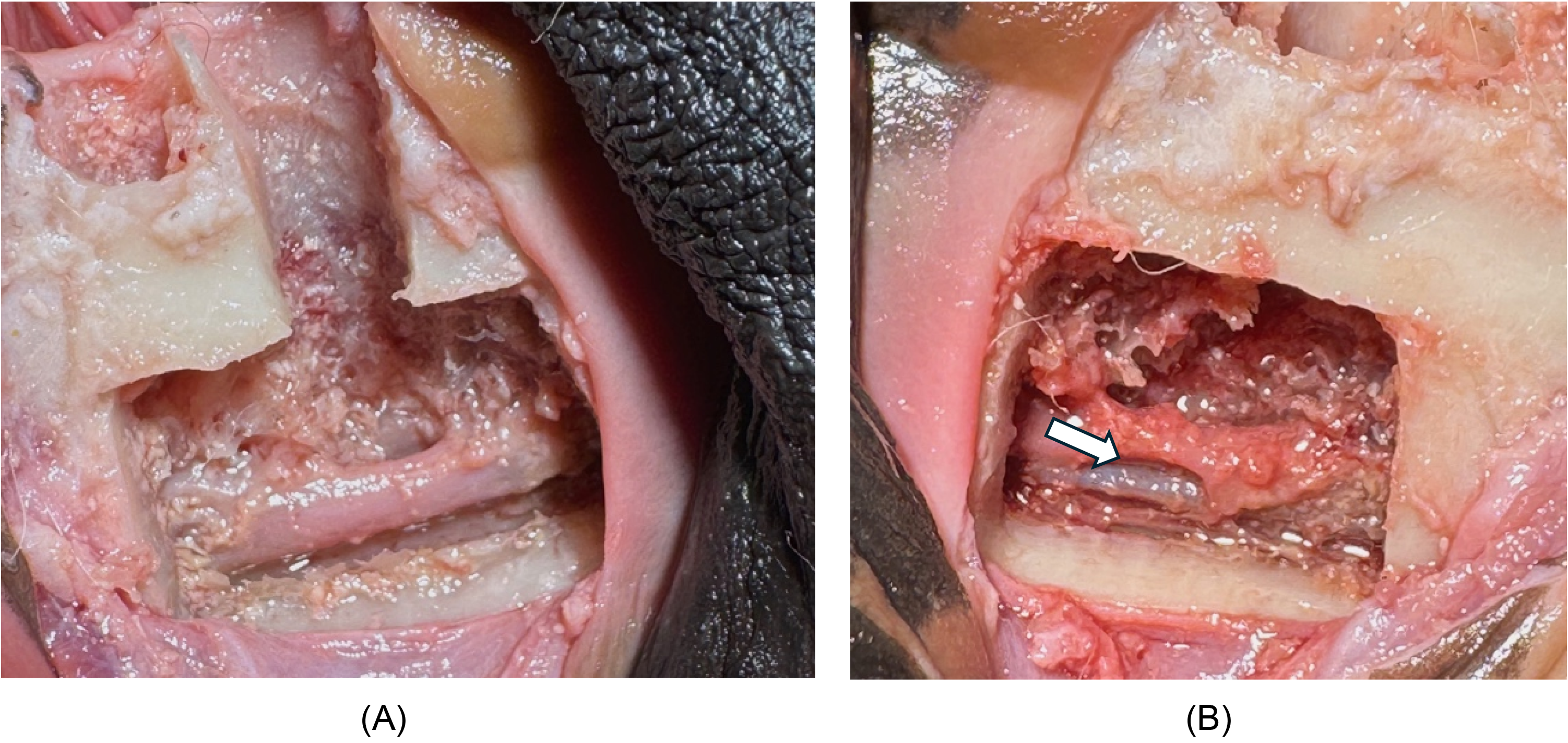
Dog #3. Lateral images of mandible showing neurovascular bundle after removal of buccal mandibular bone plate over root fragment retrieval sites. (A) Left mandible at site of fourth premolar root fragment retrieval site showing no obvious trauma to neurovascular bundle. (B) Right mandible at site of fourth mandibular premolar root fragment retrieval site showing laceration of neurovascular bundle (arrow).
Statistical Analysis
All statistical analyses were performed using R-4.1.0 statistical software. A Fisher exact test was used to identify potential differences in the frequency distribution between crestal and alveolar root fragment retrieval for the following parameters: root length (11, 12, 13, 14, or 15 mm); degree of procedure difficulty (grade 1, 2, or 3); degree of normal structure damage (grade 1, 2, or 3); location of the root fragment to be retrieved in relation to the neurovascular bundle (dorsal buccal, dorsal central, dorsal lingual, ventral buccal, or ventral lingual); and location of the root fragment to be retrieved in relation to the alveolus (central, distal or mesial). Continuous parameters were first assessed for normality using a Shapiro-Wilk test. A Mann-Whitney U test was used to identify potential differences in the time required in seconds to retrieve displaced root fragments using the crestal technique compared to the alveolar technique. A Student t test was used to identify potential differences in the area of bone removed in mm2 with the crestal technique compared to the alveolar technique. P-values of ≤.05 were considered significant in all cases.
Results
The data collected in this study in relation to each specimen are listed in Table 1. There was no statistically significant difference between the crestal and lateral techniques when comparing the measured difficulty to remove the root fragment from the mandibular canal (P = 1.000), time to retrieval (P = .545) and noted amount of damage to neurovascular structures (P = .179). There was a statistically significant difference in the amount of mandibular bone removal between the 2 techniques with the crestal technique having considerably more bone removed compared to the lateral (P < .001).
Data From Study.
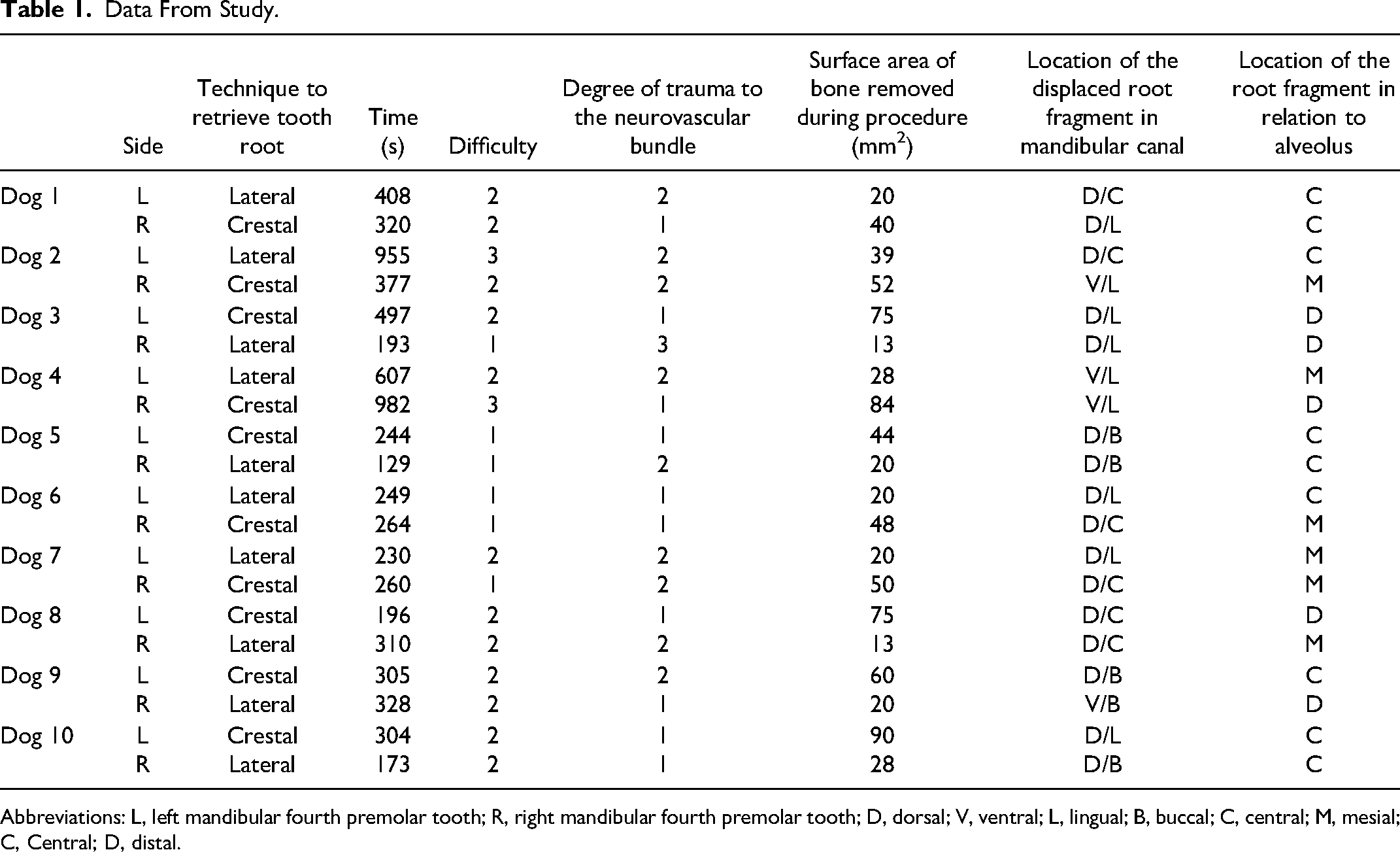
Abbreviations: L, left mandibular fourth premolar tooth; R, right mandibular fourth premolar tooth; D, dorsal; V, ventral; L, lingual; B, buccal; C, central; M, mesial; C, Central; D, distal.
The average difficulty rating for all 10 crestal techniques was 2 (moderate difficulty to find and remove root fragment due to interference with neurovascular bundle or adjacent dental structures). Only one crestal procedure (Dog #4 right mandibular fourth premolar) was rated at a difficulty of 3 (procedure was difficult to perform and involved considerable additional effort to identify and remove root fragment). The root was displaced ventral and lingual to the mandibular canal and distal to the alveolus. Six of the crestal techniques were rated a difficulty of 2. In 3 specimens, the root fragment was displaced dorsal and lingual in the mandibular canal, of these fragments 2 were central to the alveolus and one was distal to the alveolus. In the remaining 3 crestal techniques rated 2, the root fragment was displaced: (1) ventral and lingual in the mandibular canal and mesial to the alveolus; (2) dorsal and central in the mandibular canal and distal to the alveolus; and (3) dorsal and buccal in the mandibular canal and central to the alveolus. Three of the crestal techniques were rated as a difficulty of 1 (root fragment easy to find and remove by performing the described technique). Two of the specimens had root fragments displaced dorsal and central in the mandibular canal and mesial to the alveolus. The remaining specimen's fragment was displaced dorsal and buccal in the mandibular canal and central to the alveolus.
Similar to the crestal technique, the average difficulty rating for all 10 lateral techniques was 2. One specimen had a difficulty rating of 3 (Dog #2 left mandibular fourth premolar) where the root fragment was displaced dorsal and central in the mandibular canal and central to the alveolus. Six of the lateral techniques were rated as a difficulty of 2, of these 2 had root fragment displacement dorsal and central in the mandibular canal, one was mesial and one was central to the alveolus. In the remaining 4 lateral techniques rated as a difficulty of 2 the root fragment was displaced: (1) ventral and lingual in the mandibular canal and mesial to the alveolus; (2) ventral and buccal in the mandibular canal and distal to the alveolus; (3) dorsal and lingual in the mandibular canal and mesial to the alveolus; and (4) dorsal and buccal in the mandibular canal and central in the alveolus. Three of the lateral techniques were rated as a difficulty of 1, 2 of these specimens had root fragments displaced dorsal and lingual in the mandibular canal, one was central to the alveolus and the other distal. In the remaining lateral technique with a difficulty rating of 1 the root fragment was displaced dorsal and buccal to the mandibular canal and central to the alveolus.
The average time to retrieve the root fragment in all 10 of the crestal techniques was 375 s (6.25 min) (Table 2). The longest crestal technique, and overall longest retrieval time was 982 s (16.4 min) (Dog #4 left mandibular fourth premolar) where the root fragment was displaced ventral and lingual to the neurovascular bundle and distal to the alveolus. The shortest crestal technique time (Dog #8 left mandibular fourth premolar) was 196 s (3.3 min) where the root fragment was displaced dorsal and central in the mandibular canal and distal to the alveolus.
Time to Remove Displaced Root Fragments Comparing the Crestal and Lateral Techniques.a
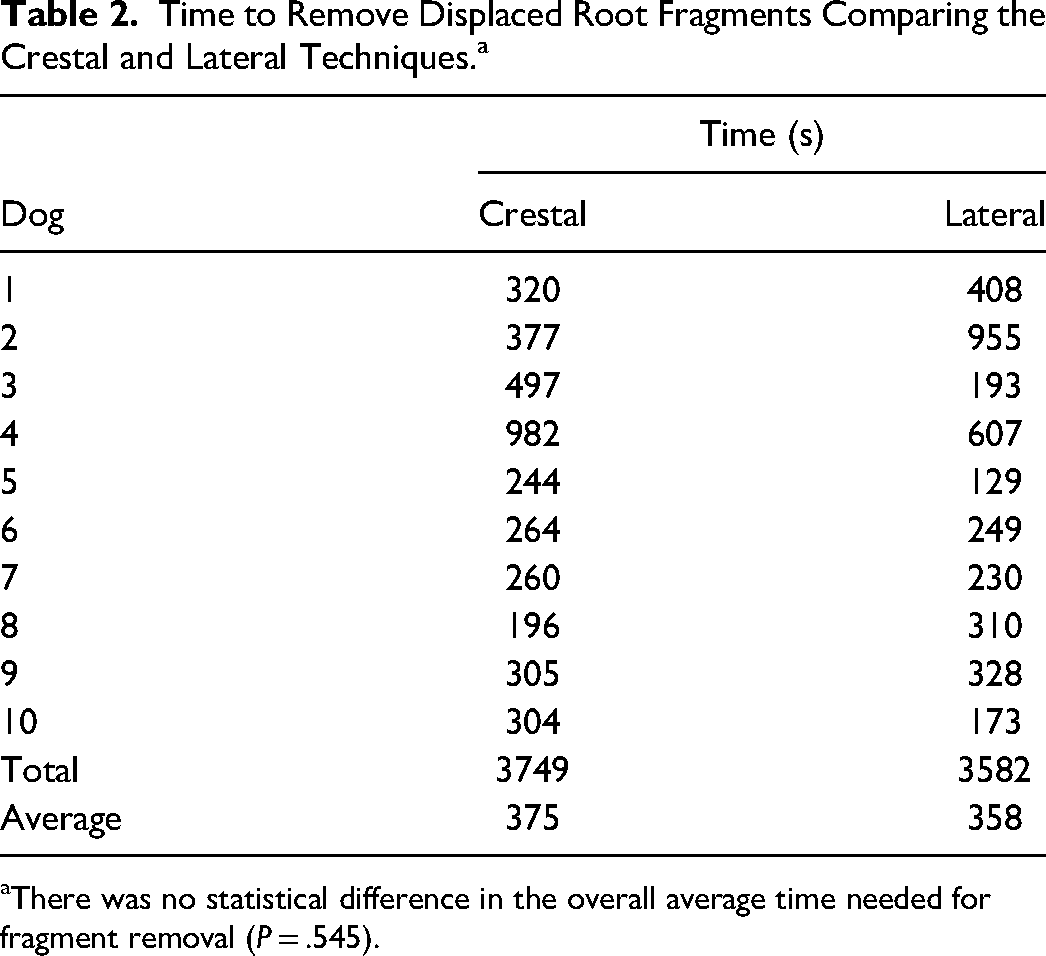
There was no statistical difference in the overall average time needed for fragment removal (P = .545).
The average time to retrieve the root fragment for all 10 lateral techniques was 358 s (6 min) (Table 2). The longest lateral technique time was 955 s (16 min) (Dog #2 left mandibular fourth premolar) where the root was displaced dorsal and central in the mandibular canal and central to the alveolus. The shortest lateral technique time, and overall time, was 129 s (2.15 min) (Dog #5 right mandibular fourth premolar) where the root was displaced dorsal and buccal in the mandibular canal and central to the alveolus.
While not statistically significant, the amount of damage to the inferior alveolar neurovascular bundle was greater with the lateral technique compared to the crestal. Three out of the 10 crestal techniques showed obvious signs of damage to the neurovascular bundle compared to 7 out of the 10 lateral techniques. Only one procedure was rated as having trauma rated as severity 3 (trauma in which there was a laceration into the vessel or nerve) (Dog #4 right mandibular fourth premolar) (Figure 8B). This trauma occurred with a lateral technique when the root fragment was displaced ventral and lingual in the mandibular canal and distal to the alveolus.
The surface area of bone removal required for root fragment retrieval was statistically different between the 2 techniques. The lateral technique had significantly less bone removed with an average of 22 mm2 compared to the crestal technique with an average of 62 mm2 bone removed (P < .001).
Statistical analysis confirmed that the positioning of the displaced root fragments in this cadaver model was random between the 2 different procedures, that is, there was no difference in the placement of the roots in the mandibular canal (P = .856), and there also was no difference in the placement of the root fragments in relation to the alveolus (P = 1.000). Four out of the 20 displaced roots were ventral in the mandibular canal. Out of these 4, 2 were removed with the crestal technique and 2 were removed with the lateral technique.
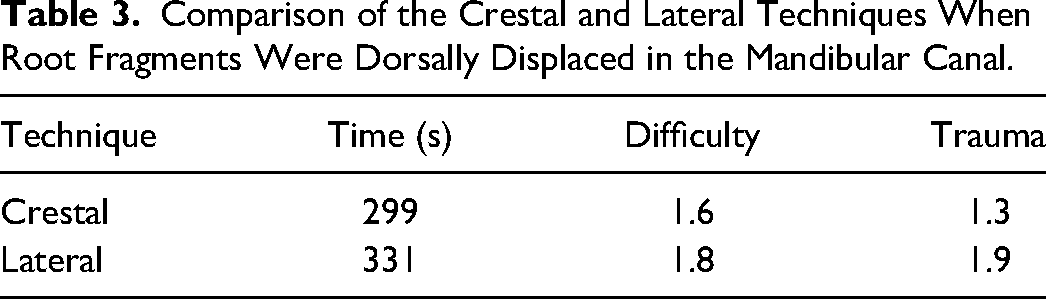
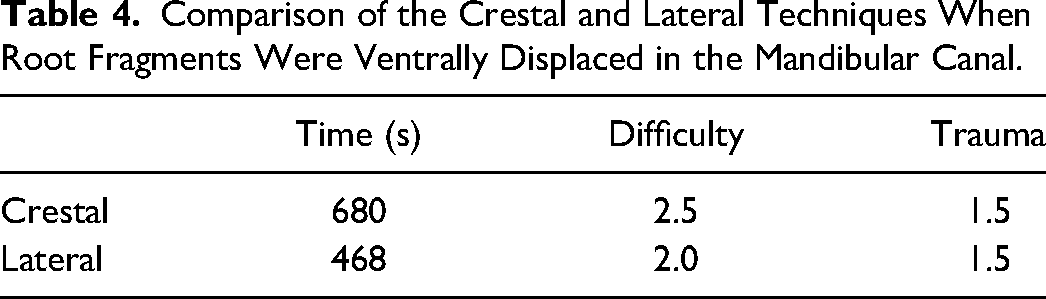
There was no statistical difference between the use of the crestal or lateral techniques when roots fragments were displaced either more dorsal or more ventral in the mandibular canal but several observations are worth noting. When the root fragments were displaced dorsal to the mandibular canal the average time to retrieve was 299 s (5 min) for the crestal, 331 s (5.5 min) for the lateral; difficulty was 1.6 for the crestal, 1.8 for the lateral; and trauma was 1.3 for crestal and 1.9 for lateral (Table 3). When the root fragments were displaced ventrally in the mandibular canal the average time to retrieval was 680 s (11.3 min) for crestal and 468 s (7.8 min) for lateral; difficulty was 2.5 for crestal and 2.0 for lateral; and trauma was 1.5 for both (Table 4).
Comparison of the Crestal and Lateral Techniques When Root Fragments Were Dorsally Displaced in the Mandibular Canal.
Comparison of the Crestal and Lateral Techniques When Root Fragments Were Ventrally Displaced in the Mandibular Canal.
Discussion
This study describes and compares 2 techniques to retrieve displaced root fragments from the mandibular canal in canine cadavers adapted from methods used to remove displaced dental implants in humans. To the authors’ knowledge, no previous studies have been performed to evaluate techniques to retrieve displaced root fragments in veterinary patients.
Dental implant removal techniques in humans from the mandibular canal are broadly categorized as crestal or lateral. The crestal technique used in this study is similar to the crestal technique to remove dental implants in humans where the root fragment was removed through the alveolus. In humans, the displaced implant is removed through the alveolus by enlarging it with a dental bur30,38 or piezoelectric surgical unit. 37 Similarly, a dental bur was used in this study for the approach as previously described. Unlike what is described in the human literature, the vertical height of the buccal alveolar bone first needed to be reduced in this study. As part of the extraction procedure for this study the vertical height of the buccal alveolar bone was reduced only 4 mm in all cases to maintain consistency between the specimens to help limit other variables that could affect outcomes. The height and width confines of the alveolus, even after performing the extraction, prevented the dental bur from reaching the opening to the mandibular canal through the alveolus for the crestal technique. This required further vertical buccal alveolar bone reduction to effectively contact and enlarge the alveolar opening to the mandibular canal, even in cases when the displaced root fragment could be visualized through the alveolus. It is possible if a longer length bur had been used in this study to enlarge the communication from the alveolus to the mandibular canal the amount of vertical bone removed could have been reduced. In a clinical veterinary patient when a root fragment is displaced into the mandibular canal, the displacement would commonly occur after fracture of the root during attempted extraction. 9 In commonly used fractured root extraction techniques, the height of the buccal alveolar bone would have likely been reduced further than this study prior to displacement to aid in extraction and retrieval of the root. 42 The need to significantly reduce the buccal alveolar bone height during the crestal technique in this study likely increased the retrieval time compared to a clinical case in which the alveolar bone height would have had greater reduction prior to root fragment displacement. The amount of vertical bone removal needed for the crestal technique could also be dependent on the size of the patient, with smaller animals requiring less bone height reduction to access the communication between the alveolus and the mandibular canal.
The lateral technique is performed by removing the displaced dental implant through a “window” or bone access created on the buccal aspect of the mandibular bone. Prior to creating the window of bone access, creation of a mucoperiosteal flap is needed for the lateral technique to access the buccal mandibular bone.17,33 After the mandibular bone is exposed, 2 methods to create the window of bone have been described: (1) osteotomies are performed to allow removal of a buccal section of cortical bone over the displaced implant, also called a bone “plate”13,16-18,31,37 or (2) buccal bone is burred away to create a cortical window30,33 to access the displaced implant. Osteotomies to remove the overlying cortical bone sections in humans are created with an oscillating saw, 16 piezoelectric surgical unit,13,18,31,37 and some have not been described. 17 Cortical bone sections are created in either rectangular or trapezoidal shapes. Sections in a rectangular shape were either replaced after the procedure and secured with microplates and screws16,31,37 or not replaced and simply had the mucoperiosteal flap closed over the window. 17 Sections that were created in the trapezoidal shape were replaced after the procedure and did not require plates or screws as their shape prevented shifting after refitting.13,18 Mucoperiosteal flaps are closed over the buccal aspect of the mandible after completion of the lateral technique.17,33 A procedure similar to the lateral technique has been briefly described in the veterinary literature to remove displaced root fragments from the mandibular canal. In the described procedure, a bony window is created through the buccal mandibular bone over the site of the displaced root fragment with a piezoelectric surgical unit to allow root fragment retrieval. 9 In this study, the lateral window over the displaced root fragment was created by removing a circular area of mandibular bone using a diamond bur. Removing a rectangular or trapezoidal section of overlying mandibular bone could be done in canine patients as described in humans, but may not be possible in smaller animals which have a negligible amount of mandibular bone.
The advantages of the crestal technique over the lateral in humans is that the technique is considered simpler and can be performed using solely local anesthesia. 30 Widening the already exposed alveolus is less complicated compared to the lateral technique, which is more extensive as it involves creating a window through the buccal mandibular bone. Because the crestal technique is limited to access through the alveolus it has been recommended for retrieval of implants dorsal to the inferior alveolar nerve in humans. 30 Although observed differences were not statistically significant, this study found that when the displaced root fragment was dorsally displaced in the mandibular canal, the crestal technique required less time on average, was less difficult and showed fewer signs of trauma to the neurovascular bundle compared to the lateral technique (Table 3). Because veterinary patients must be under general anesthesia to perform dental procedures, 43 removing displaced root fragments using solely local anesthesia is not applicable as it is in humans.
The advantages in humans of the lateral technique compared to the crestal are reported as being better visualization due to greater bone removal over the displaced dental implant and being less likely to result in nerve damage as the displaced implant does not need to be rotated to be removed. 30 In this study, the authors attempted to minimize the amount of bone removed with each technique, yet that also allowed the authors to visualize and remove the displaced root fragments. This resulted in the average size of the lateral access site being statistically significantly smaller when compared to the crestal technique. While the lateral technique in this study did not have a larger window of bone compared to the crestal technique as is shown in the human literature, access to the displaced root fragment was often closer for ventrally displaced root fragments compared to the crestal technique, making retrieval quicker and less difficult in those cases. The authors found that when the root fragment was displaced ventrally in the mandibular canal the average time to remove and difficulty rating were lower for the lateral technique compared to the crestal, although these differences did not reach statistical significance. The average amount of trauma was the same for both procedures (Table 4). Gentle manipulation of the orientation of the root fragments in the mandibular canal with a periodontal probe was necessary for most of the crestal and lateral techniques to allow the fragment to be positioned in a way the forceps could cleanly grasp and remove it through the created access. This manipulation could have resulted in damage to the neurovascular structures. A larger buccal mandibular window of bone with the lateral technique in this study may have minimized the need to manipulate the root fragment for removal and limited neurovascular damage which is described in the human literature. 30
The reported disadvantages of the crestal technique in humans include limited vision with a small operative field that can result in further displacement of the dental implant, and the possibility of excessive bone removal that may result in insufficient remaining alveolar bone for implant placement. 30 The access opening was small for both techniques in this study, limiting visualization. Even with the use of magnification and a head lamp, visualization of ventrally displaced root fragments was most difficult when using the crestal technique due to the increased distance of the root fragment from the access site. Further root displacement occurred once in the study (Dog #4 right mandibular fourth premolar) when retrieving a ventrally displaced root fragment using the crestal technique. The combination of the small access site, distance from the alveolar access to the ventrally displaced root fragment and the presence of the neurovascular bundle between the access and root fragment made it difficult to visualize and manipulate the root fragment to a position that it could be grasped by the forceps, which resulted in the root inadvertently being further displaced in the mandibular canal before it could be retrieved. The need to retain alveolar bone to effectively place an implant is not applicable to veterinary patients, but general conservation of mandibular bone should be a goal, especially in smaller patients that may already have minimal mandibular bone. A disadvantage of the crestal technique in this study was the large amount of alveolar bone that needed to be removed. In a clinical case similar bone removal could weaken the mandible and predispose it to fracture. If the displaced root fragment requires significant vertical bone reduction to retrieve using the crestal technique then the lateral technique may be a better option.
While the reported primary disadvantage of the lateral technique in humans is it requires a more extensive surgery compared to the crestal technique, 30 the design of this study was intended to minimize variables between the 2 techniques. The primary difference between techniques in this study was the location in which the accesses were made to retrieve the displaced root fragments. Large mucoperiosteal flaps were created for both procedures to allow complete access to the lateral mandible throughout all parts of this study. In a clinical case a mucoperiosteal flap created for tooth extraction may need to be extended and enlarged to achieve the required access to the buccal mandibular bone for the lateral technique. If removal of a displaced root fragment using the lateral technique is performed at a time other than when the displacement occurred, a semilunar or curved flap could be created in the alveolar mucosa buccal to the displaced root as previously described for surgical endodontic therapy 44 rather than a pedicle flap for access to the buccal mandibular bone. In the human literature the size of the lateral window made by burring away buccal mandibular bone for the lateral technique, as done in this study, was not recorded.30,33 When bone sections were removed, sizes of the removed buccal cortical bone sections for the lateral technique in humans were 2 cm by 1 cm, 16 1 cm by 0.5 cm, 31 1 cm by 1.1 cm and 1 cm by 1.3 cm. 13 The calculated average area of the bone sections was 1.2 cm2. Compared to the size of the created bone sections in humans, the amount of bone removal using the lateral technique in this study was much smaller, with an average area of bone removal of 0.2 cm2. During this study one of the 2 procedures graded as a difficulty of 3 (Dog #2 left mandibular fourth premolar) occurred when using the lateral technique to remove a root fragment displaced dorsal and central in the mandibular canal and central to the alveolus. The initial approach was incorrectly created mesial to the location of the displaced root, and when the root fragment could not be visualized, an intraoperative radiograph was required to correctly realign the access to the displaced root. This experience illustrates why it is important with the lateral technique to place the access on the buccal mandibular bone as close as possible to the location of the displaced root to minimize difficulty in visualizing and retrieving the root fragment.
While there is not an established consensus in the human literature on when to use the crestal versus the lateral technique, it is generally recommended to use the crestal technique in situations when the implant is minimally displaced and dorsal to the neurovascular bundle.30,37 The findings in this study agree with these recommendations. The crestal technique should be primarily used in situations when the root fragment is displaced dorsally in the mandibular canal. When the displaced root fragment was dorsal in the mandibular canal, locating and visualizing the root fragment was typically less difficult with the crestal technique compared to the lateral. Often a portion of a dorsally displaced root fragment could be visualized through the alveolus in the mandibular canal prior to starting retrieval. This visualization allowed constant monitoring of the root fragment's location, so the surgical access was more accurately directed and there was better avoidance of the neurovascular bundle and therefore a lower incidence of trauma when using the crestal technique. In a clinical patient, hemorrhage could significantly inhibit visualization of the root fragment complicating the procedure. In this study when the displaced root fragment was more ventrally displaced in the mandibular canal, locating, visualizing and retrieving the root fragment was often more difficult using the crestal technique compared to the lateral as previously discussed.
While not statistically significant, the lateral technique resulted in more visible signs of trauma to the neurovascular structures compared to the crestal technique. This noted increase in damage may have resulted from the dental bur inadvertently contacting the neurovascular bundle as it initially entered the lateral mandibular canal before the bundle could be identified and manually deflected. The crestal technique may have resulted in fewer visible signs of neurovascular damage because the neurovascular bundle could often be visualized through the alveolus during most of the procedure and efforts could be made to avoid and deflect the bundle when using the dental bur. Trauma to the neurovascular bundle may be decreased in both procedures if a piezoelectric surgical unit were used as described in the human13,18,31,33,37 and veterinary literature. 9 Piezosurgical instruments create ultrasonic microvibrations that cut through bone, but do not harm adjacent soft tissues such as neurovascular structures. 45 The traumatic method of root fragment displacement creation and root manipulation during retrieval could also be possible causes of damage to the neurovascular bundle for each technique. Because the method used to displace the root fragments was the same for both approach techniques and root manipulation was used in most procedures, the increased trauma reported with the lateral technique is more likely associated with the root fragment retrieval procedure. Due to the techniques being evaluated on cadaver specimens, trauma may have occurred to the neurovascular bundle that could have resulted in pain or hemorrhage in a clinical patient but was not grossly apparent on the post procedure evaluation during this study.
When a tooth root fragment is displaced into an adjacent anatomical space the decision whether to remove or monitor should be carefully considered. In humans when root fragment displacement occurs into the maxillary sinus, treatment protocols have been advised. 10 The practitioner should identify the size of the root fragment and determine if there was any infection of the tooth or periapical tissues. If the root fragment is small (2-3 mm) and there is no sign of preexisting infection, a brief attempt should be made to remove the root fragment and if unsuccessful, the procedure should be stopped, location of the root fragment documented, and patient informed. If the patient develops clinical signs associated with the displaced root, then referral to an oral-maxillofacial surgeon for removal should be recommended. If the root fragment is large or infected and simple removal cannot be achieved, then referral to an oral-maxillofacial surgeon is recommended. 10 Similarly, recommendations in the veterinary literature advise if a displaced root fragment into an adjacent anatomical space cannot be removed immediately after the complication occurs using minimal exploration, the location of the root fragment should be radiographically documented and the client informed. 9 If the patient exhibits signs of discomfort such as pawing or rubbing at the face then referral to a veterinary dental specialist should be recommended. 9
In reviewing the literature for this study, no previous reports regarding the long-term effects of leaving displaced roots in the mandibular canal were found in veterinary or human dental literature. In human dentistry, patients who had a dental implant displaced into the mandibular canal that was not immediately retrieved experienced pain, 26 hypoesthesia,17,30 paresthesia, 31 or had no noted issues. 33 The standard length of dental implants is ≥10 mm, 46 which is much larger than the length of the displaced root fragments in this study. At this size, a displaced dental implant may occupy more of the mandibular canal and potentially put more pressure on the neurovascular bundle, therefore being likely to cause more neurologic issues compared to a root fragment of smaller size. It is also possible that displaced root fragments in the mandibular canal may not lead to significant discomfort if there is not associated infection and if they are relatively small in size. Due to the large variation in size of dogs, applying a specific measurement of displaced root fragment that should be recommended for removal is not suggested by the authors. If there are signs of infection associated with the tooth root or the periapical tissue that becomes displaced, then the root fragment should be removed no matter the size.9,10,47 The decision to intentionally retain a displaced root fragment in the mandibular canal should only be made after considering the skills of the practitioner, determining the size and location of the root fragment, and evaluating if there are any signs of infection associated with the root or associated periapical area. Reported risks associated with attempts to remove displaced root fragments and dental implants can be serious and include further displacement of the root fragment or dental implant,12,26,27,48 severe hemorrhage,5,12 prolonged procedure time, 12 and damage to adjacent neurovascular structures.5,46,49
When considering the previously discussed recommendations from the human 10 and veterinary 9 literature on displaced root fragments and observations from this study, the authors have developed treatment guidelines for when root displacement into the mandibular canal occurs. If the practitioner does not possess the necessary experience, equipment or clinical skills to remove the displaced root fragment then retrieval should not be attempted. The location of any displaced or retained root fragment should be determined radiographically, ideally with 3-dimensional (3D) imaging, recorded in the medical record and the client informed. Referral to a veterinary dental specialist should be discussed for any retained displaced root fragment as there is the potential for discomfort that the patient may not clinically demonstrate. If the decision is made to not remove the displaced root and to not refer to a veterinary dental specialist, then the client should be instructed to carefully monitor the patient for any signs of discomfort such as pawing or rubbing at the face and annual radiographic monitoring of the root should be performed. If clinical signs are noted, then referral to a veterinary dental specialist should be strongly recommended for removal of the displaced root fragment.
The best way to manage a displaced root fragment is to prevent it from occurring in the first place. Prior to performing any extraction, the practitioner should be completely prepared with appropriate preoperative imaging, proper instrumentation and experience necessary to execute the procedure successfully. If the practitioner is not comfortable performing the extraction, then the patient should be referred to a veterinary dental specialist. 4
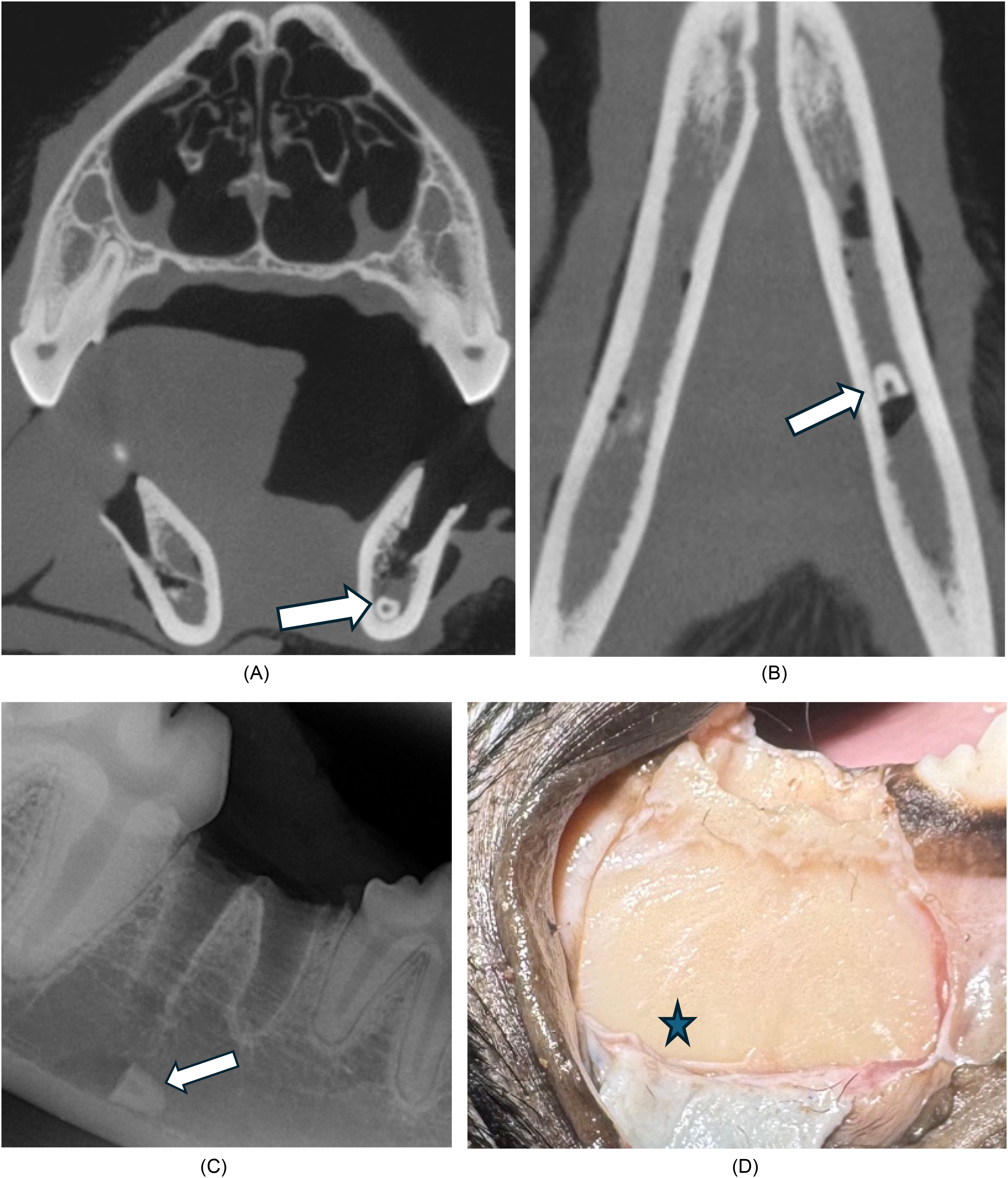
Cone beam computed tomography and intraoral dental radiographs were both used in this study to locate the displaced root fragments in the mandibular canal. Intraoral dental radiography is the most widely available dental imaging modality in veterinary medicine but computed tomography (CT) and CBCT are considered the “gold standard” to evaluate the bony structures of the head and temporal mandibular joint of veterinary patients. 50 Intraoral radiographs merge anatomical structures in a 3D area into a 2 dimensional (2D) image and are mostly obtained in a facial-oral axis. 51 Superimposition (overlap of structures in the x-ray path), summation effect (superimposed structures add or subtract radiopacity) tangential effect (2D structures are diminished when perpendicular and enhanced when parallel to the x-ray beam) and the inability to localize a structure's distance from the dental film or plate can be limitations of intraoral radiographs. 51 While detailed comparison and analysis of the imaging modalities was not included in this study, images were acquired for each specimen and procedure with each modality and used by the authors. Both dental radiographs and CBCT provided useful information for displaced root fragment localization. The authors found the tangential effect of intraoral radiography beneficial in being able to clearly visualize the radio-opaque (white) lines of the alveolus that allowed identification of the root fragment's location (mesial, central, or distal) to the alveolus (Figure 2D). A single dental radiograph utilizing the parallel technique did show the displaced root fragment in the mandibular canal but could not localize its precise location due to the 2D limitation. The authors obtained 2 radiographic views of a displaced root fragment in the mandibular canal in a cadaver as has been previously described to locate a displaced dental implant 26 to determine if 2 dental radiographs almost perpendicular to each other could accurately localize the root fragment in the mandibular canal. One view was obtained using the parallel technique, 39 and the other was obtained using an occlusal view 52 at a near 90-degree angle to the parallel view. In this particular example, the occlusal view could not be exactly 90-degree to the parallel otherwise the crown of the first mandibular molar was superimposed on the displaced root fragment preventing visualization of the fragment. The CBCT imaging was also performed to analyze the ability to localize the displaced root fragment using the 2 view dental radiographs. The parallel dental radiograph showed the displaced root fragment appeared more ventrally located in the canal (Figure 9A) which was consistent with the transverse plane on the CBCT (Figure 9B). It was more difficult to interpret the location of the root fragment in the mandibular canal using the near occlusal radiograph due to overlap of adjacent structures (Figure 9C) but did show the root more lingually displaced, consistent with the dorsal plane of the CBCT (Figure 9D). The study concluded CBCT was able to provide a clearer image of the location of the displaced root fragment in the mandibular canal compared to the dental radiographs but if 3D imaging is not available to locate a displaced root fragment in the mandibular canal, then utilizing the parallel and occlusal dental radiograph views could be considered.
Intraoral radiographs and cone beam computed tomography (CBCT) images of displaced root fragment (arrow) in left mandibular canal of a canine cadaver. (A) Intraoral radiograph using parallel technique shows displaced root fragment more ventrally located in mandibular canal; (B) Transverse CBCT shows displaced root fragment more ventrally located in mandibular canal; (C) Intraoral radiograph using near occlusal view shows displaced root fragment more lingually located in mandibular canal; (D) Dorsal CBCT shows displaced root fragment more lingually displaced in mandibular canal.
Cone beam computed tomography uses x-rays to create high-resolution tomographic images of mineralized tissues. 50 Cone-beam computed tomography allows for multiplanar reconstruction (MPR) which permits viewing of the displaced root tip in 3 different planes (dorsal, transverse and sagittal) eliminating overlap of adjacent anatomical structures giving a precise location of the displaced root tip in the mandibular canal. The transverse and dorsal planes on the CBCT were used to document the location of the root fragment in relation to the mandibular canal as previously discussed. Due to the small size of the mandibular canal, classifying the location of the root fragment in the study as far as dorsal or ventral and buccal, central or lingual was sometimes difficult depending on the angulation of the displaced root fragment. The use of this location classification was intended to help determine how the 2 removal techniques compared when removing the root fragment from different areas in the mandibular canal. This classification system may not be as significant for a clinical case, but being able to precisely localize the root fragment radiographically is necessary to allow the practitioner to determine the appropriate treatment. Intraoral radiographs were commonly used by the investigators in this study to determine the root fragment's location in relation to the alveolus, as the sagittal view of the CBCT did not allow the complete alveolus to be viewed in one frame due to the curvature of the mandible (Figure 2C and D).
Imaging used to identify and localize displaced root fragments and dental implants in the human literature includes dental radiographs (periapical, occlusal, panoramic),3,5,16,17,26,27,37 CT,3,37,48,53 CBCT,3,13,17,18,24,29,31-33 and various combinations of these imaging modalities. The human literature recommends 3D radiological examination to confirm localization of a displaced root. 22 The use of CT, either conventional or cone beam, is considered the most accurate way to determine the exact size and location of a root fragment. 5 Cone beam computed tomography is considered the ideal diagnostic tool for imaging of displaced roots in human dentistry as it has the advantage of lower radiation exposure, decreased cost and better image quality of teeth and surrounding bone structures when compared to conventional CT.5,29,54 In a veterinary study that evaluated retained tooth roots in dogs, dental radiographs were used but CT or CBCT is mentioned as a more accurate method of identification and measurement 47 and based on the authors observations in this study, CBCT imaging is recommended in addition to dental radiographs to accurately localize displaced root fragments in the mandibular canal.
There are several limitations associated with this study. The relatively small study population of a total of twenty procedures (ten for each technique) limited the power of the statistical analyses performed. Because cadavers were used in this study, hemorrhage, as would typically be encountered in a clinical case, was not a factor in root fragment removal which may have reduced or affected the time and difficulty scores for each study procedure when compared to a clinical setting. The size of the root fragments created in this study were based on human 10 and veterinary 8 sources that recommends root fragments greater than 4 mm in size should be removed. Since the size of a displaced root fragment in an actual clinical case will vary, the validity and usefulness of observations on the techniques used for this study may vary also based on size of the root fragment. Since the specimens used were all large breed dogs the optimal techniques for successful root retrieval in small dogs and cats may be different than those evaluated in this study. No attempt was made in this study to displace the root fragments to a particular location in the mandibular canal (i.e., dorsal or ventral to the neurovascular bundle) but rather just to randomly displace the root as it may occur in a clinical case. Further studies in smaller breed dogs and cats with intentional displacement of the root fragment into particular aspects of the mandibular canal could provide more information on the use of the techniques studied. Because of the limited number of published reports regarding this topic, single clinical case reports of root fragment retrieval from the mandibular canal would also be beneficial to better understand the application of these procedures in a clinical setting.
This study aims to provide a foundation that can be used when making decisions on root fragment retrieval from the mandibular canal in the dog. The methods analyzed were based on dental implant removal techniques in humans and provide viable options to remove displaced root fragments in dogs. The results of this study indicate the crestal approach should be limited to cases when a displaced root fragment is more dorsal in the mandibular canal and the lateral approach may be better for root fragments displaced more ventrally. Ultimately the best technique will depend on individual patient considerations, and the practitioner's experience and personal preference. Review of existing literature supports that displaced root fragments should be removed if possible unless the risk to the patient is greater than the anticipated side effects of leaving the root fragment in place. Based on the authors’ observations CBCT imaging is recommended in addition to dental radiographs to accurately localize displaced root fragments in the mandibular canal. Removing displaced root fragments in the mandibular canal is a potentially difficult procedure with serious potential complications. Unless the practitioner possesses the appropriate skills and knowledge to remove the displaced root fragment, referral to a veterinary dental specialist is recommended.
Materials
Skulls Unlimited, Oklahoma City, OK, USA
CR7 Vet, iM3, Vancouver, WA, USA
VetCATTM, Xoran Technologies, Ann Arbor, MI, USA
Vet Exam, iM3, Vancouver, WA, USA
VetCATTM, Xoran Technologies, Ann Arbor, MI, USA
EKG Caliper, Frienda Technologies Co. LTD, Beijing, China
FG 701L, Henry Schein, Melville, NY, USA
Scratch Awl, Craftsman, Towson, MD, USA
Pin Punch 1/16″ (1.5 mm), Irwin, Towson, MD, USA
Pin Punch 3/32″ (2.4 mm), Dasco Pro, Towson, MD, USA
Pin Punch 1/8″ (3.2 mm), Dasco Pro, Towson, MD, USA
Nail Set 0.8 mm, DeWalt, Towson, MD, USA
EXW2XS, Cislak Manufacturing Inc., Niles, IL, USA
850L-016-12-ML, Diatech, Mt. Pleasant, SC, USA
Straight Fine 4.5″ Stainless Steel Dissecting Forceps, Scientific Labwares, Gainesville, VA, USA
Footnotes
Acknowledgments
The authors would like to thank Dr Chel Hee Lee for his insight and contributions to the study design and statistical analysis as well as Drs Curt Coffman, Alexander Adrian, and Lisa Fink for their contributions to final manuscript review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning this article's research, authorship, and/or publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.