
Abstract
Introduction
Restoring normal gait function remains a major clinical challenge in post-stroke rehabilitation. Backward walking may increase neuromotor demands compared with forward walking and performing it on an incline may further augment task complexity. However, the feasibility, safety, and tolerability of backward incline walking in individuals with chronic stroke have not been systematically examined.
Objective
To evaluate the feasibility of a single-session treadmill-based backward incline walking protocol in individuals with chronic stroke, focusing on recruitment, adherence, safety, tolerability, and participant acceptability.
Methods
Design
Prospective, nonrandomized pilot feasibility study.
Setting
Clinical Human Dynamic Laboratory at a university-affiliated rehabilitation program.
Participants
Six individuals with chronic stroke (≥6 months post-event) were enrolled (median age 68 years, interquartile range [IQR] 56–73, median time since stroke of 19 months IQR [15–98]). Inclusion criteria included ambulatory ability with or without a single cane for ≥10-meter and absence of cognitive, orthopedic, or cardiopulmonary contraindications, and ability to tolerate 15 min of treadmill walking. All participants met these criteria and provided informed consent.
Intervention
Participants completed three treadmill walking conditions delivered in a fixed order (level, forward incline, and backward incline walking), each for up to 15 min at self-selected speeds. Rest breaks and manual support were provided as needed.
Main Outcomes
Feasibility metrics included recruitment rate, protocol adherence, safety (adverse events), tolerability (rating of perceived exertion), and participant acceptability.
Secondary Descriptive Measures
Overground walking speed and spatiotemporal gait parameters recorded using an instrumented walkway before and after the treadmill conditions. These data were summarized descriptively without inferential statistical testing.
Results
Recruitment was feasible, with 40% of eligible individuals enrolled. All participants completed the single-session protocol without adverse events. Perceived exertion increased in our sample with task complexity and was highest during backward incline walking (median RPE = 6). Participant acceptability was high, with all individuals expressing willingness to repeat the protocol.
Significance
A single-session treadmill-based backward incline walking was feasible, safe, and well-tolerated in this pilot sample of ambulatory individuals with chronic stroke. These findings progression to adequately-powered, randomized studies designed to evaluate efficacy and to address order effects and individualized gait responses.
Keywords
Introduction
Background
Stroke remains a leading cause of long-term disability (Feigin et al., 2025), with persistent gait dysfunction representing one of the most disabling sequelae (Patel et al., 2025). Individuals with chronic stroke frequently demonstrate impaired limb coordination (Patterson et al., 2008), reduced walking speed (Perry et al., 1955), postural instability, and decreased endurance, all of which restrict community mobility and participation in daily activities (Nadeau et al., 2013). Although task-specific walking interventions are central to post-stroke rehabilitation, motor recovery often plateaus, and improvements achieved in structured clinical environments may not consistently generalize to more demanding locomotor contexts (Baricich et al., 2024).
Backward walking has been investigated as a strategy to increase locomotor challenge and alter neuromuscular recruitment patterns compared to forward walking (Balasukumaran et al., 2019; Grasso et al., 1998; Kim et al., 2014; 2017; Yang et al., 2005). Compared to forward walking, backward walking is associated with increased quadriceps and plantar flexor activation and greater demands on postural and proprioceptive processing. Experimental studies in healthy adults have demonstrated that walking backward on an incline further amplifies joint excursion, and electromyographic activity of the rectus femoris, gastrocnemius, and tibialis anterior, suggesting heightened muscular and neuromotor demands during this combined task (Cipriani et al., 1995).
While backward walking has been explored in neurologic populations, including individuals in the acute phase after stroke (Takami & Wakayama, 2010), the feasibility and safety of backward incline walking in individuals with chronic stroke have not been systematically examined. Given potential balance impairments, endurance limitations, and fall risk in this population, careful evaluation of tolerability and safety is necessary before considering therapeutic implementation.
Feasibility studies are a critical preliminary step in rehabilitation research, particularly when introducing novel and progressively complex locomotor tasks (Keefe et al., 2013; Kistin & Silverstein, 2015; Kraemer et al., 2006; Leon et al., 2011; Orsmond & Cohn, 2015). Such investigations aim to evaluate recruitment capability, protocol adherence, safety, tolerability, and participant acceptability prior to conducting adequately powered efficacy trials. Accordingly, this pilot study was designed to evaluate the feasibility of a single-session treadmill-based backward incline walking protocol in ambulatory individuals with chronic stroke. Secondary descriptive biomechanical and physiological measures were collected to inform protocol refinement and future study design; however, the study was not powered to assess therapeutic efficacy.
Methods
Design and Setting
This prospective, nonrandomized cross over pilot feasibility study was conducted at the Human Dynamic Lab located within a quaternary healthcare facility. Institutional Review Board approval was obtained prior to recruitment, and all participants provided written informed consent.
Participants
Six individuals with chronic stroke (5 male, 1 female) were recruited from a university-affiliated rehabilitation clinic. Individuals were included if they (1) age 18–85 years old, (2) first-time cerebrovascular accident (CVA) ischemic or hemorrhagic, (3) have sustained the CVA more than the past 6 months, (4) able to walk with/ without a single cane for 10 meters (32–33 feet). Individuals were excluded if they had (1) excessive spasticity in lower limbs, (2) a history of other major cardiovascular or neurological diseases that could affect their ability to walk or exercise, and (3) attended concurrent physical therapy or research involving gait or balance training. (Table 1).
Demographic and Clinical Characteristics of Participants (n = 6).
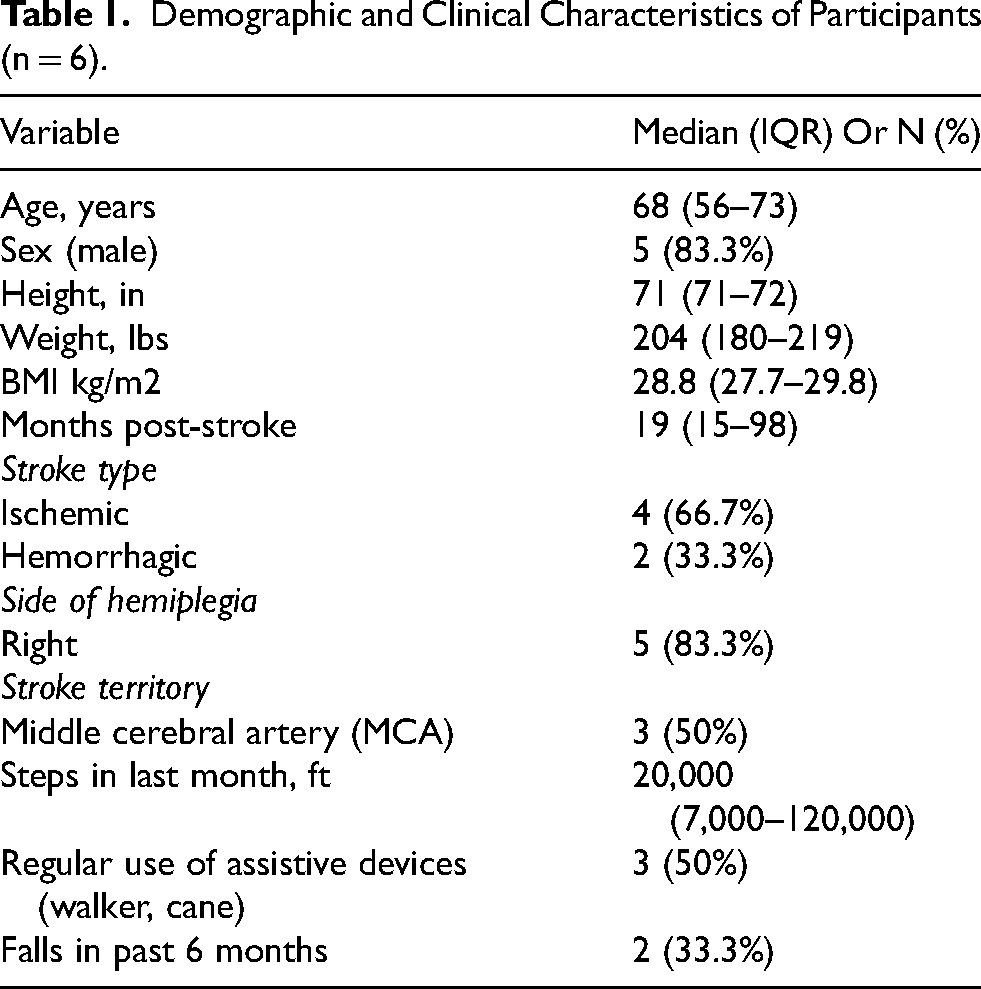
Stroke characteristics varied across cohorts. Per physician notes, four participants had ischemic strokes, two involving the left middle cerebral artery (MCA) and two subcortical in distribution and varying levels of aphasia. Two individuals had hemorrhagic strokes: one from left basal ganglia bleeding and another affecting the right hemisphere from the right MCA event. Lesion locations were primarily subcortical, and chronicity ranged from 18 months to over 8 years.
Participants also demonstrated a range of functional and mobility profiles as well as varying use of assistive devices. For instance, one individual ambulated with a narrow-based quad cane reported approximately 2.1 km of walking in the past week and over 61 km in the past month, primarily while using an ankle-foot orthosis (AFO). Another participant used a spiral AFO outdoors only, reporting no falls and high community mobility (approximately 9 km weekly, 37 km monthly). Two participants reported falls within the past 3 to 6 months, though none occurred in the preceding four weeks. One participant used a rolling walker indoors but was otherwise independent in community ambulation. Assistive devices included spiral AFO, single-point canes, and mobility scooters (the latter not used regularly by participants).
Participant Screening and Enrollment
The participant screening and recruitment process is illustrated in Figure 1.
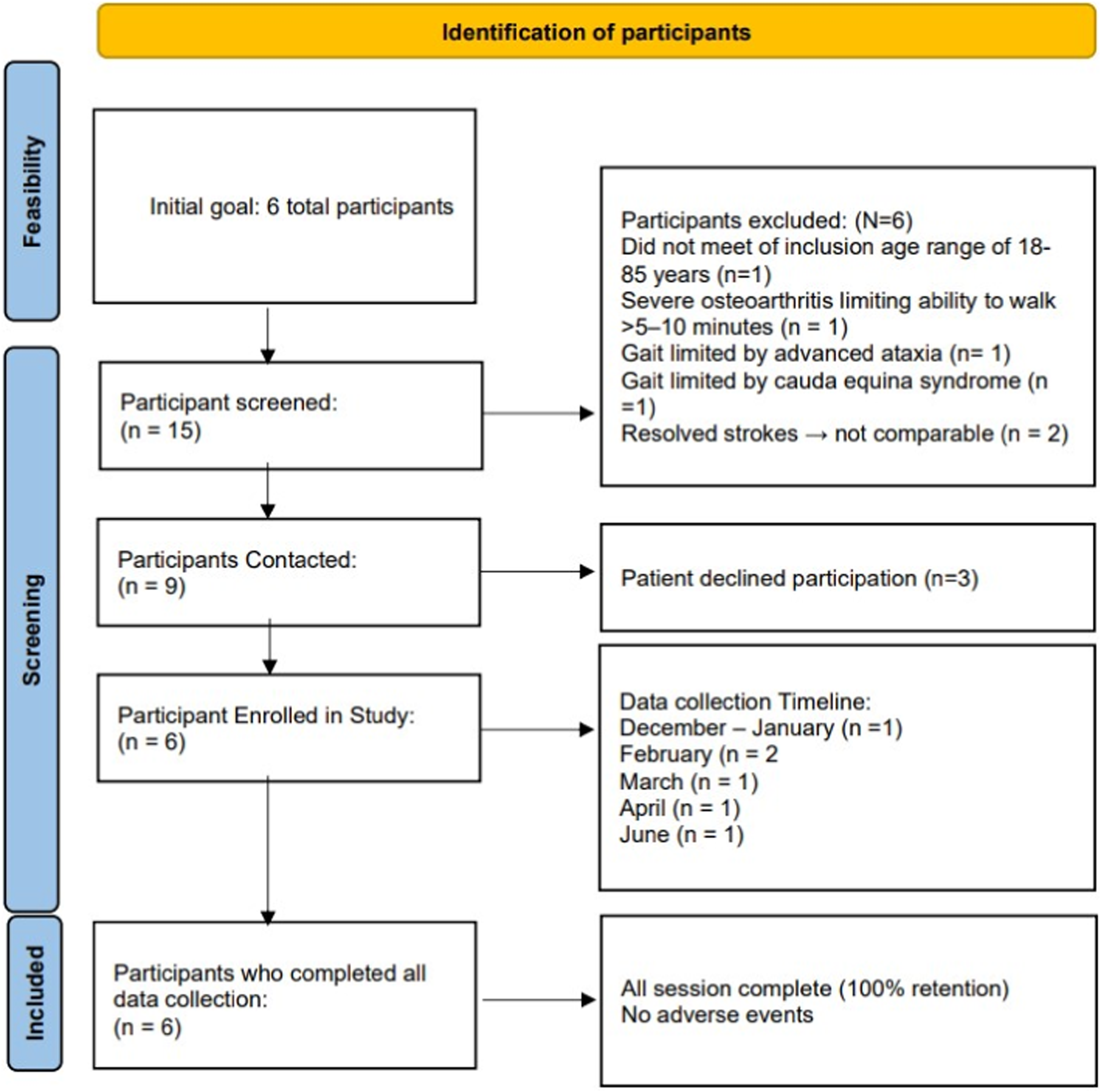
Study-flow diagram illustrating participant screening, enrollment and data collection procedures.
Intervention Protocol
Participants completed three treadmill walking conditions in a single session: (1) forward level (0% incline) walking, (2) forward incline (6%) walking, and (3) backward incline (6%) walking (Figure 2). Walking speed was standardized to each participant's self-selected comfortable pace, determined during a pretest session. Each condition lasted 15 min with seated rest permitted as needed. Transitions were supervised by trained spotters, and participants used side railings throughout. The treadmill condition order (level→ forward incline→ backward incline) was fixed according to the Institution Review Board (IRB)-approved protocol design. This sequence prioritized safety and accommodated the novelty of backward incline walking in this population, allowing participants to first acclimate to treadmill walking before performing the most technically demanding condition. No adverse events of near-miss events occurred. Rest breaks were provided between conditions to mitigate fatigue. Participant's perceived exertion was monitored throughout. The original design included three separate visits (∼30 min each) but was amended to a single-session to reduce participant burden while maintaining protocol fidelity.
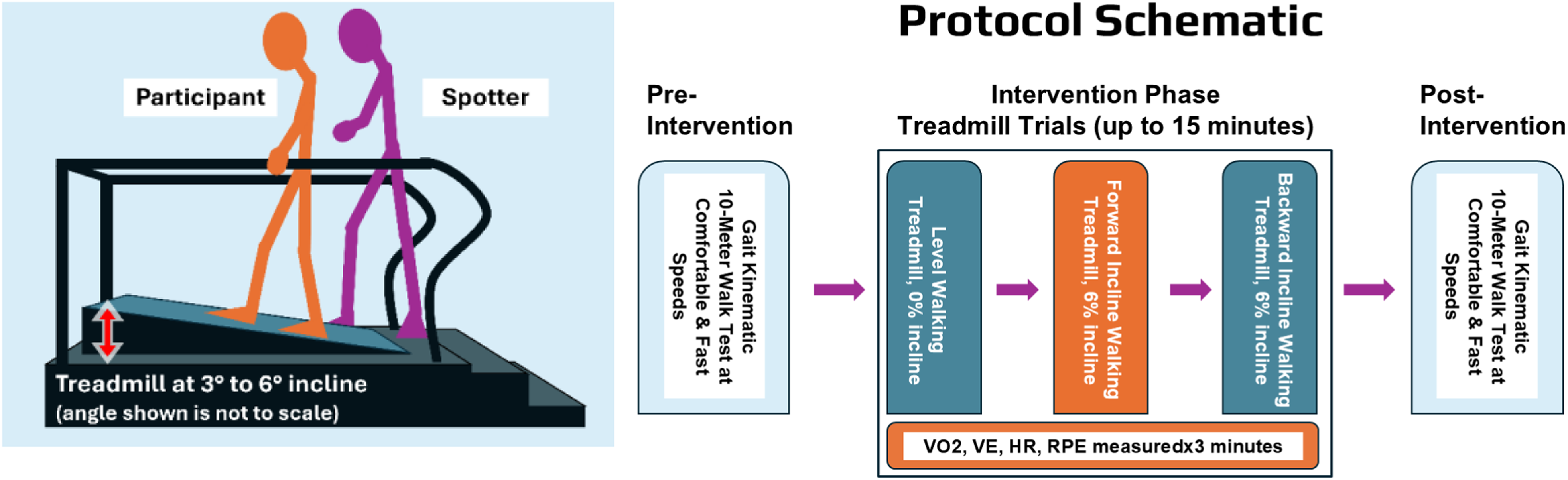
Experimental design and protocol schematic: Participants completed pre- and post-session overground walking assessments, including spatiotemporal gait analysis and the10-meter walk test (10MWT). Participants then completed sequential treadmill conditions consisting of level walking (0% incline), forward incline walking (6% incline), and backward incline walking (6% incline), each lasting up to 15 minutes. Cardiopulmonary responses, including heart rate [HR], ventilation [VE], and rating of perceived exertion [RPE] were monitored throughout each condition.
Physiological Evaluation (n = 3)
Cardiopulmonary testing was conducted using the COSMED kb5 portable metabolic analyzer system and the Polar hear rate monitor to assess participant's physiological responses across all treadmill conditions. Oxygen consumption (VO2), ventilation (VE), respiratory exchange ratio (RER), and heart rate (HR, beats/minute) were continuously monitored throughout. Participants wore a fitted mask connected to the metabolic unit, which collected and transmitted data in real time. Physiological variables were averaged across the final three minutes of each condition. The Rate of Perceived Exertion (RPE) was recorded verbally every 3 min using standard Borg Scale to capture subjective fatigue and exertion levels.
Overground Gait Assessment (TekScan, n = 5)
Overground walking was assessed using a TekScan Stride way system (TekScan, Inc. Boston, MA) to capture spatiotemporal gait parameters, including cadence, step length, walking speed, swing and stance times, and percentages of single and double limb support during the gait cycle. Participants completed trials at (1) self-selected comfortable speed and (2) fastest speed. The 10-Meter Walk Test (10MWT) was embedded within the walkway protocol, timing the central 6 m of a 10-m segment (Tyson & Connell, 2009). Two trials were performed per condition, and walking speed was averaged. High-speed video recordings (500 fps) were collected for treadmill walking from multiple views for cross-reference.
Feasibility Outcomes
The following feasibility outcomes were assessed according to the NIH-recommended domains, including: (Https://Www.Nccih.Nih.Gov/Grants/Pilot-Studies-Common-Uses-And-, n.d.)
(1) recruitment feasibility: number screened, eligible, and enrolled, (2) protocol adherence: number of participants completing all treadmill conditions, (3) safety and tolerability: occurrence of adverse events, need for assistance, and ratings of perceived exertion (RPE), (4) acceptability: participants’ willingness to repeat the protocol, and subjective feedback on task difficulty and comfort.
This pilot was not powered for hypothesis testing, but aimed to assess feasibility thresholds (i.e., ≥30% recruitment, ≥90% protocol adherence, and absence of adverse events) aligned with established methodological standards.
Exploratory Outcomes
Overground gait analysis parameters. cadence, walking speed, step length, swing and stance times, and single and double limb support percentage.
Cardiopulmonary responses (VE, HR, RPE) collected during treadmill walking, analyzed descriptively.
Data Analysis and Statistics
Overground gait data included (1) self-selected and fast-paced walking speeds and (2) full spatiotemporal gait parameters recorded at baseline and following each treadmill condition using the TekScan walkway system. All analyses were conducted using SAS version 9.4 (Cary, NC) for exploratory purposes only.
Results
Feasibility Outcomes
Recruitment feasibility: Of approximately 15 patients screened, 12 met eligibility criteria, 9 were contacted, and 6 enrolled (40%). Recruitment targets were achieved within the anticipated timeframe.
Session completion / adherence: All participants completed every treadmill condition (100% adherence), with over 90% of planned assessments successfully collected. Following IRB-approved protocol amendments, most participants completed all treadmill conditions within a single session, the first enrolled participant completed the protocol across three visits.
Safety and tolerability: No adverse events or near-miss incidents occurred during any walking conditions, including backward incline walking. No modifications to predefined safety procedures were required. Sessions were well tolerated with minimal manual assistance; Rate of perceived exertion (RPE) increased during the protocol in our sample and was highest during backward incline walking (median RPE = 6).
Acceptability: All participants provided positive experiences and expressed willingness to engage in backward incline walking in future sessions.
Walking Speed During Training
Walking speed varied across treadmill conditions in our sample, as expected. Median treadmill walking speeds were 0.45 m/s (IQR 0.4–0.45) during level walking, 0.35 m/s (IQR 0.34–0.35) during forward incline walking, and 0.21 m/s (IQR 0.04–0.23) during backward incline walking. These values seem to reflect task-dependent adjustments rather than performance changes over time.
Overground Walking Performance
Walking speeds (m/s) derived from the 10MWT for participants with fast speed available data are presented descriptively at the individual level. (Table 2) TekScan spatiotemporal measures summarized group level gait performance across conditions using median and interquartile ranges. Spatiotemporal parameters demonstrated variability across participants, reflecting differences in motor impairment. These descriptive data illustrate the variability in overground gait parameters observed following treadmill exposure and are provided to support transparency and inform future protocol development. Detailed spatiotemporal gait parameters of the paretic limb at comfortable and fast walking speeds are presented in Supplementary Tables 1 & 2. No inferential statistical analyses were performed for these exploratory measures.
Individual Fast-Paced Walking Speed (m/s) During Overground Testing (n = 6).
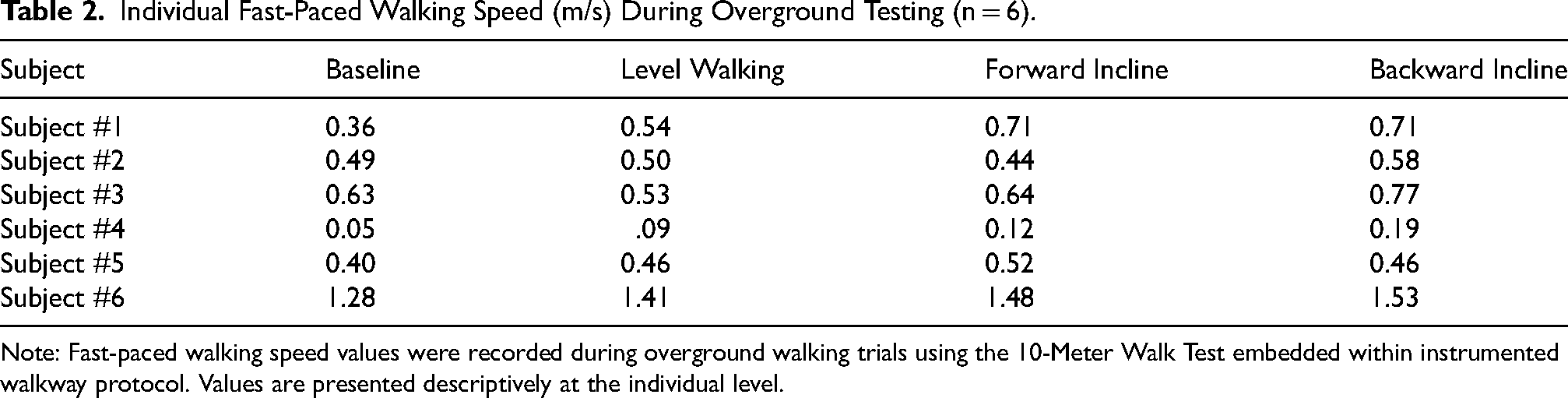
Note: Fast-paced walking speed values were recorded during overground walking trials using the 10-Meter Walk Test embedded within instrumented walkway protocol. Values are presented descriptively at the individual level.
Physiological Effort
Cardiopulmonary responses (HR, VE, RPE) were successfully collected in three participants and showed progressive increases with treadmill complexity. As only three participants underwent testing, these data are interpreted solely within a feasible framework – confirming the tolerability and technical viability of capturing these physiological signals during treadmill walking conditions, rather than physiological adaptation.
Physiological effort, as measured by Rating of Perceived Exertion (RPE), varied across walking conditions. Backward incline walking elicited the highest perceived exertion followed by level walking, forward incline and base line. Figure 3 illustrates these condition-specific differences in RPE.
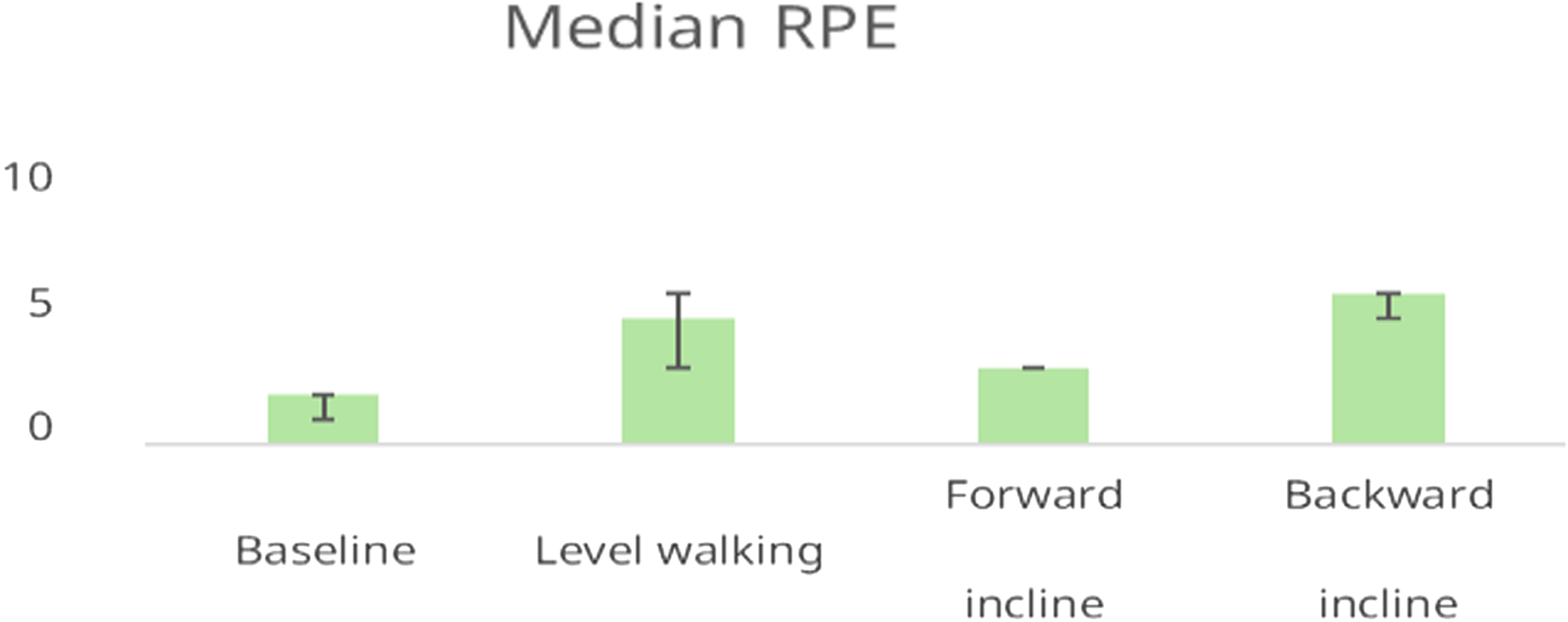
Median RPE across treadmill walking conditions.
Bars represent the median RPE for each condition. Error bars indicate the interquartile range (IQR). RPE was highest during backward incline walking, followed by level walking, forward incline and baseline.
Cardiopulmonary Response
During the initial seated rest and the treadmill walking, heart rate (HR) and ventilation (VE) were recorded under three conditions: level walking (C1), forward incline (C2), and backward incline (C3). Data was averaged during the first 5-min initial seated rest and final three minutes of each 15-min treadmill session.
HR ranged from 69–138 beats/minute, and VE ranged from 26–34 L/min across participants. Individual variability was observed, with some participants demonstrating elevated cardiopulmonary demand under incline conditions. For example, Patient 2 who was female and lighter in body weight (76 kg) demonstrated consistently elevated HR and VE values, peak of HR 138.6 and peak of VE 34.85 in backward incline condition suggesting higher physiological effort compared to the two male patients 81.65–99.34 kg.
Table 3 shows average treadmill speed (m/s), total exercise time (minutes), heart rate (HR, beats/minute), and minute ventilation (VE, L/min): the volume of air exhaled per minute (L/min); calculated as tidal volume×respiratory rate. It reflects the cardiopulmonary demand during activity. As only three participants completed cardiopulmonary testing, these data are interpreted solely within feasibility framework- confirming the tolerability and technical viability of capturing these physiological signals during walking conditions, rather than drawing conclusions about physiological adaptation.
Cardiopulmonary (Heart Rate and Ventilation) Responses During Final 3 min of Treadmill Walking Across Three Conditions: Level Walking (C1), Forward Incline (C2), and Backward Incline (C3). Each Value Reflects Individual Participant Data Captured During Steady State Walking. Despite Individual Variations, no Statically Significant Difference in HR or VE Were Observed Between the Three Walking Conditions Within Individual Subjects.
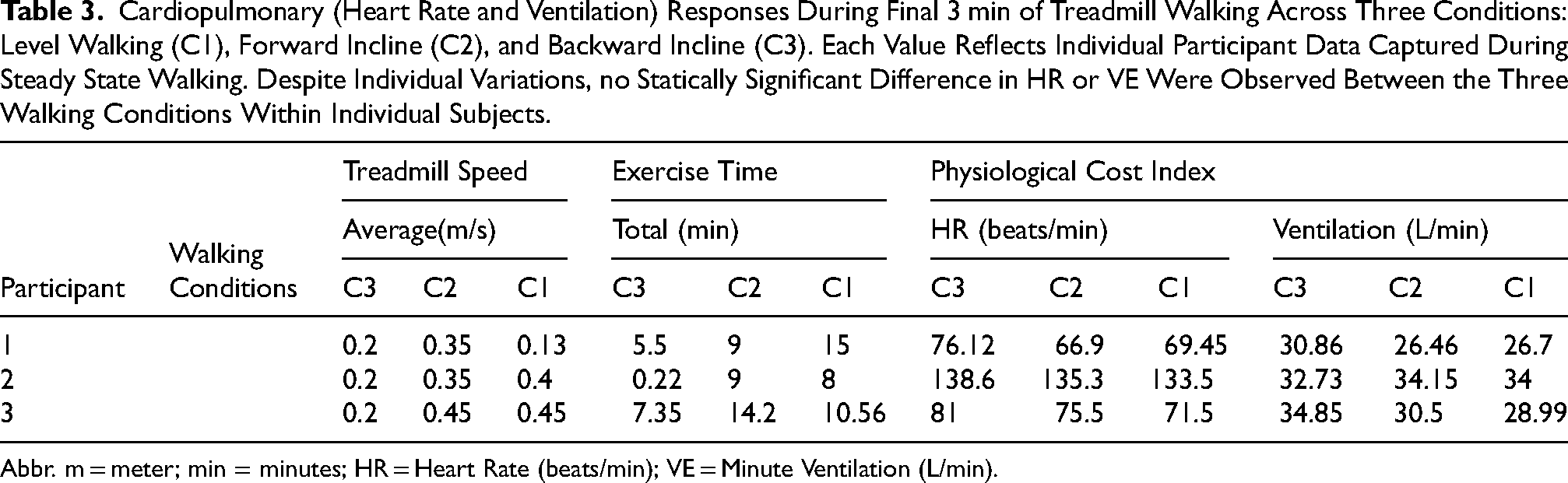
Abbr. m = meter; min = minutes; HR = Heart Rate (beats/min); VE = Minute Ventilation (L/min).
Discussion and Significance
This pilot study explored feasibility, safety, and immediate cardiopulmonary and gait related responses to a novel intervention - backward incline treadmill walking - in individuals with chronic stroke. While previous studies have shown benefits of backward walking on flat surfaces (Chang et al., 2021; Chen et al., 2020; Menezes et al., 2025; Wen & Wang, 2022), this is among the first to examine the added demands of incline within a single-session format. Our findings demonstrate this protocol is feasible and well-tolerated; all participants completed the session without adverse events, modifications to safety procedures, or the need for assistance during backward incline walking. Perceived exertion was higher in our sample during this condition, with median RPE of 6, consistent with greater postural and neuromuscular demands. Despite these demands, participants reported positive experiences and expressed willingness to repeat the task, highlighting strong acceptability. Importantly, these responses occurred without compromising safety, and the protocol was successfully completed even with individuals with varying chronicity, mobility levels, and assistive device use. This suggests broad potential applicability when appropriately supervised.
Physiological data, though limited to a subset, showed elevated heart rate and exertion during backward incline walking. However, due to the fixed order of treadmill conditions and small sample size, these findings should be interpreted with caution and not as evidence of relative task intensity. Cardiopulmonary responses were presented descriptively to inform future trial design.
This study provides a critical first-step in testing a task-specific, directional gait training approach that may eventually hold value for stroke rehabilitation. Future studies should build on this foundation by incorporating multi-session protocols, randomized designs, biomechanical instrumentation, and larger, more diverse samples (Rábago et al., 2015; Winstein et al., 2016).
Conclusion
Our data indicates that backward incline treadmill walking is a safe, feasible and well-tolerated task for individuals with chronic stroke. While exertion levels increased in our sample during this condition, participants completed the protocol without incident and found it acceptable. These findings provide preliminary support for further development and controlled testing of backward incline walking interventions.
Implication for Clinical Practice
Clinicians may consider supervised introduction of backward incline walking as a strategy to challenge gait and postural control, particularly for patients who have plateaued with tradition level walking protocols. With proper precautions, this modality may serve as engaging addition to individualized rehabilitation plans aimed at reducing compensatory strategies and enhancing directional stability.
Supplemental Material
sj-docx-1-rnn-10.1177_09226028261451969 - Supplemental material for Backward Incline Walking in Stroke Rehabilitation: A Pilot Feasibility Study
Supplemental material, sj-docx-1-rnn-10.1177_09226028261451969 for Backward Incline Walking in Stroke Rehabilitation: A Pilot Feasibility Study by Sharareh Sharififar, ChrisLamprecht, Anna Yozefovich Khanna, Parisa Rashidi, Paula Ackerman, Parisa Zarreii, Cynthia Garvan, Hassan Azari and Chandramouli Krishnan in Restorative Neurology and Neuroscience
Footnotes
Acknowledgments
The authors wish to sincerely thank Lydia Pezzullo BS., Ryan Nixon PhD, Mathew Martenson PhD, and APK interns: Charliegh Baab, David Zhang, Julian Pazmino, Nathalia Gonzalez, and all participants for supporting this pilot project.
Funding
University of Floria Department of PMR internal funds.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.