
Abstract
Background:
Repetitive transcranial magnetic stimulation (rTMS) is increasingly used as a neuromodulatory intervention to facilitate motor recovery after stroke. However, the frequency-specific effects of rTMS on lower-limb motor control and their neurophysiological correlates remain insufficiently clarified.
Objective:
To compare the effects of low-frequency (1 Hz) rTMS applied over the contralesional (unaffected) lower-limb motor area of the primary motor cortex and high-frequency (10 Hz) rTMS applied over the ipsilesional (affected) lower-limb motor area on electroencephalographic (EEG) activity, affected-side lower-limb muscle activation, balance, and gait in individuals with chronic stroke.
Methods:
Thirty-nine participants with chronic stroke were randomly assigned to a low-frequency rTMS group (n = 13), a high-frequency rTMS group (n = 13), or a sham group (n = 13). rTMS was delivered for 10 sessions over 2 weeks. Resting-state EEG (relative beta-band power at Cz), surface EMG of the affected-side rectus femoris, biceps femoris, tibialis anterior, and gastrocnemius during sit-to-stand, Timed Up and Go (TUG), 10-meter walk test (10MWT), and limits of stability (LOS) were assessed before and after the intervention. A 3 × 2 mixed-design analysis of variance (ANOVA) (group × time) was conducted.
Results:
Significant group × time interactions were observed for rectus femoris activation (p < 0.001) and TUG performance (p = 0.037). Post hoc pairwise comparisons confirmed significantly greater improvements in TUG performance and rectus femoris activation in the low-frequency rTMS group than in the high-frequency and sham groups. Relative beta-band activity at Cz demonstrated a significant main effect of time (p < 0.001) without a significant interaction effect. Similarly, 10MWT and LOS showed significant time effects (p < 0.05) but no significant group × time interactions. No significant main effects of group were identified across outcomes.
Conclusion:
Short-term rTMS was associated with improvements in selected neuromuscular outcomes, while changes in resting cortical activity, gait speed, and postural stability appeared to reflect general time-related effects. Low-frequency rTMS demonstrated greater improvements in rectus femoris activation and TUG performance compared with high-frequency and sham stimulation. These findings suggest that frequency-specific rTMS may preferentially influence neuromuscular strategies underlying dynamic mobility rather than steady-state gait performance.
Keywords
Introduction
Stroke is one of the leading causes of long-term neurological disability worldwide and frequently results in persistent impairments in lower-limb motor function, balance, and gait (Feigin et al., 2025). Following stroke, deficits in postural control and locomotion are not only attributable to peripheral muscle weakness but are also associated with alterations in cortical and subcortical motor network activity. Previous studies have suggested that interhemispheric imbalance between the lesioned and contralesional hemispheres may contribute to motor impairment, although lower-limb and postural motor control also involves substantial bilateral and subcortical inputs (Edwards et al., 2023; Murase et al., 2004). In particular, reduced activation of the lesioned motor cortex and maladaptive dominance of the contralesional hemisphere have been suggested to interfere with efficient motor control during functional tasks such as standing and walking.
Repetitive transcranial magnetic stimulation (rTMS) has been increasingly applied as a noninvasive neuromodulatory intervention to promote neuroplastic changes in patients with stroke. The physiological effects of rTMS are known to depend on stimulation frequency. Low-frequency stimulation (≤1 Hz) has been associated with inhibitory effects on cortical activity, whereas high-frequency stimulation (≥10 Hz) is generally considered to facilitate cortical activation (Rossi et al., 2009; Rossini et al., 2015). Based on these principles, previous studies have applied frequency-specific rTMS protocols to modulate motor-related cortical regions in stroke rehabilitation. Clinical trials targeting the lower-limb motor cortex have typically employed stimulation frequencies ranging from 1 Hz to 10 Hz, delivered across 5–15 sessions over 1–3 weeks, with total pulse doses commonly between 600 and 1,500 pulses per session (Fisicaro et al., 2019; Hsu et al., 2012; Huang et al., 2025). While several studies have reported improvements in gait speed, balance performance, or functional mobility following rTMS, the magnitude and specificity of these effects have varied considerably depending on stimulation frequency, treatment duration, and concurrent rehabilitation programs. Consequently, the relative effects of low- and high-frequency rTMS on lower-limb function remain insufficiently clarified, particularly with respect to their underlying neurophysiological correlates.
In recent years, electroencephalography (EEG) has been utilized to examine neural activity changes associated with neuromodulatory interventions in stroke. Among EEG-derived measures, beta-band activity (approximately 13–25 Hz) has been widely recognized as a neural marker related to motor planning, sensorimotor integration, and movement execution (Gilbertson et al., 2005; Zrenner et al., 2018). Alterations in beta-band power have been reported during motor tasks and postural control in both healthy individuals and stroke populations, suggesting that beta activity reflects motor-related cortical processing rather than direct corticospinal excitability (Cassim et al., 2000; De Martino et al., 2024). Although changes in EEG beta activity following rTMS have been described, most previous investigations have focused predominantly on upper-limb function, with limited attention given to lower-limb motor control and balance-related outcomes. Moreover, relatively few studies have examined whether frequency-specific rTMS protocols differentially modulate resting-state motor-related oscillatory activity in stroke populations.
Surface electromyography (sEMG) provides complementary information regarding peripheral muscle activation patterns that are directly relevant to functional tasks such as sit-to-stand transitions, balance maintenance, and gait. Previous studies have demonstrated that abnormal lower-limb muscle activation patterns are closely associated with impaired balance and walking ability in individuals with stroke (Yang et al., 2015). Integrating EEG and sEMG measures may therefore allow for a more comprehensive examination of central and peripheral adaptations associated with rTMS interventions. However, few studies have simultaneously investigated frequency-dependent rTMS effects on EEG activity, lower-limb muscle activation, and functional balance and gait outcomes within a single experimental framework, particularly in individuals with chronic stroke.
High-frequency rTMS (≥10 Hz) is generally used to increase cortical excitability in the affected hemisphere, whereas low-frequency rTMS (≤1 Hz) may reduce excessive interhemispheric inhibition from the unaffected hemisphere (Murase et al., 2004; Rossi et al., 2009; Rossini et al., 2015). Based on these distinct neurophysiological mechanisms, both stimulation protocols were included to examine whether facilitation of the ipsilesional motor cortex or suppression of contralesional inhibition would differentially influence cortical activity, lower-limb muscle activation, balance, and gait outcomes in individuals with chronic stroke.
In addition to frequency-specific rTMS studies, recent evidence from other noninvasive neuromodulation approaches has further supported the therapeutic potential of cortical stimulation in chronic stroke rehabilitation. Specifically, anodal transcranial direct current stimulation applied during rehabilitation was shown to significantly enhance paretic rectus femoris muscle activation, improve functional mobility performance as assessed by the Timed Up and Go test, and reduce the electroencephalography-derived brain symmetry index, indicating improved interhemispheric cortical balance (Ruas et al., 2025). These findings suggest that cortical stimulation may positively influence corticospinal excitability, neuromuscular coordination, and motor performance after stroke. Compared with transcranial direct current stimulation, however, repetitive transcranial magnetic stimulation provides a more focal and targeted modulation of the motor cortex, which may allow more selective enhancement of lower-limb motor output. This provides an additional rationale for examining whether frequency-specific rTMS can differentially influence cortical activity, lower-limb muscle activation, balance, and gait outcomes in individuals with chronic stroke.
Therefore, the purpose of the present study was to compare the effects of low-frequency (1 Hz) rTMS applied over the contralesional (unaffected) lower-limb motor area of the primary motor cortex and high-frequency (10 Hz) rTMS applied over the ipsilesional (affected) lower-limb motor area on EEG beta-band activity, lower-limb muscle activation assessed by sEMG (rectus femoris, biceps femoris, tibialis anterior, and gastrocnemius), balance, and gait in patients with stroke. We hypothesized that both rTMS protocols would induce measurable motor-network changes, with frequency-dependent differences expected to emerge in dynamic functional and neuromuscular outcomes. Importantly, this study did not assume a strict interhemispheric competition model for lower-limb motor control, but instead explored frequency-specific rTMS effects within the broader context of lower-extremity motor network organization.
Methods
Study Design
This study employed a randomized, sham-controlled trial design to investigate the effects of frequency-specific repetitive transcranial magnetic stimulation (rTMS) on neural activity and functional outcomes in patients with stroke. Participants were randomly allocated to one of three groups: a low-frequency rTMS group (1 Hz), a high-frequency rTMS group (10 Hz), or a sham stimulation group. Outcome measures were assessed at baseline and immediately after the 2-week intervention period. Baseline assessments were conducted in the following order: EEG, surface EMG, Timed Up and Go (TUG), 10MWT, and limits of stability (LOS). Post-intervention assessments were performed using the same procedures and order within 48 h after completion of the intervention. The study design and reporting followed the principles of the CONSORT guidelines for randomized controlled trials (Schulz et al., 2010).
Participants
Participants were recruited from an inpatient rehabilitation hospital in Gwangju, Republic of Korea. Initially, 40 patients with stroke were enrolled; one participant withdrew during the study period, resulting in a final sample of 39 participants (low-frequency rTMS group, n = 13; high-frequency rTMS group, n = 13; sham group, n = 13).
Inclusion criteria were: (1) a diagnosis of unilateral stroke with hemiparesis, with a post-stroke duration between 6 and 24 months; (2) the ability to ambulate independently with or without an assistive device; and (3) a Mini-Mental State Examination–Korean version (MMSE-K) score ≥24. Exclusion criteria included a history of seizures, contraindications to rTMS such as metallic implants or stents, previous craniectomy, or severe visual or auditory impairments (Rossi et al., 2009).
This study was approved by the Institutional Review Board of Wise Rehabilitation Hospital (IRB No. 202410-WR-01), and all participants provided written informed consent prior to participation.
Randomization and Blinding
Participants were randomly assigned to one of the three groups using a computer-generated random allocation sequence, and group assignment was concealed until the intervention allocation. Outcome assessments were conducted by an experienced physical therapist who was not involved in the rTMS intervention. Participants were blinded to group allocation, while operator blinding was not feasible due to the nature of the rTMS intervention, which is consistent with previous rTMS clinical studies (Rossini et al., 2015).
Measurements and Procedures
Electroencephalography (EEG)
EEG data were recorded using a wireless dry-electrode EEG system (DSI-24, Wearable Sensing, USA), with electrodes positioned according to the international 10–20 system. Signals were collected from 21 channels (Fp1, Fp2, Fz, F3, F4, F7, F8, Cz, C3, C4, T3, T4, Pz, P3, P4, T5, T6, O1, O2, A1, and A2). Recordings were obtained in a quiet environment with participants seated comfortably and instructed to relax with their eyes closed to minimize motion artifacts (Van Putten & Tavy, 2004).
EEG signals were processed using manufacturer-provided software. The signals were sampled at 300 Hz and band-pass filtered between 1 and 50 Hz to remove noise and movement-related artifacts. Relative beta-band power (13–25 Hz) was calculated as the primary EEG-derived motor-related cortical activity variable associated with movement planning and postural control (Cassim et al., 2000; Zrenner et al., 2018). Resting-state EEG was therefore considered appropriate for examining baseline motor-related cortical activity without confounding task-related movement artifacts. Task-based EEG was not adopted to avoid movement artifacts and variability associated with functional tasks, particularly in individuals with post-stroke motor impairment, which may compromise signal reliability. For the primary analysis, the Cz electrode was selected as it anatomically corresponds to the lower-limb representation of the primary motor cortex.
Surface Electromyography (sEMG)
Electrodes were placed according to the SENIAM recommendations over the rectus femoris, biceps femoris, tibialis anterior, and gastrocnemius muscles on the affected side (Hermens et al., 2000). Muscle activation levels were normalized using the reference voluntary contraction (%RVC) method based on a standardized submaximal semi-squat posture rather than a one-repetition maximum task. For the reference contraction, participants were instructed to stand with both feet shoulder-width apart and perform approximately 30° of knee flexion while maintaining the posture for 5 s under therapist supervision. The middle 3 s of the EMG signal were extracted, and the RMS value obtained during this interval was used as the reference voluntary contraction. After one familiarization trial, three reference trials were recorded, and the mean RMS value was used for normalization. This submaximal %RVC procedure was selected because it is safer and more clinically feasible than maximal loading tasks in individuals with chronic stroke who often present with weakness, asymmetrical weight bearing, and impaired postural stability (Vigotsky et al., 2017). Although normalization to maximal M-wave (Mmax) obtained by peripheral nerve stimulation has been recommended to distinguish peripheral from central influences on EMG amplitude, Mmax normalization was not performed in the present study because the primary purpose was to compare within-subject functional changes in muscle recruitment patterns during repeated rehabilitation sessions rather than to quantify absolute neuromuscular transmission capacity (Girard et al., 2018). In addition, repeated peripheral nerve stimulation may increase participant burden and discomfort in clinical stroke populations. Therefore, the %RVC method was considered an appropriate and clinically applicable normalization procedure for the present repeated-measures design. Muscle activation was analyzed during a sit-to-stand task because this movement requires coordinated activation of proximal and distal lower-limb muscles and reflects functional transitional control relevant to dynamic balance. EMG during overground walking or the TUG test was not adopted due to potential signal contamination from movement artifacts and stride variability, which may compromise measurement reliability in individuals with post-stroke motor impairment.
Balance, Gait Assessment
Dynamic balance was assessed using the TUG test, which has demonstrated high intra- and inter-rater reliability in stroke populations (Chan et al., 2017). Participants performed the test from a standard chair (seat height 45 cm) and were instructed to walk at a comfortable and safe speed. One practice trial was allowed prior to the recorded trial. LOS were evaluated using a force platform system (Biorescue, RM Ingenierie, France), with participants instructed to shift their center of pressure in multiple directions while maintaining balance (Sturnieks et al., 2008). Three trials were performed, and the average value was used for analysis. Adequate rest periods were provided between trials to prevent fatigue.
Gait performance was measured using the 10-meter walk test (10MWT), with only the middle 6 m timed to minimize acceleration and deceleration effects, while 2 m at each end were provided for these phases (Steffen et al., 2002).
Intervention (rTMS)
The intervention consisted of repetitive transcranial magnetic stimulation (rTMS) administered over a 2-week period (five sessions per week, totaling ten sessions). All stimulations were performed by an experienced physical therapist and a clinical neurophysiologist following the international guidelines for noninvasive brain stimulation (Rossini et al., 2015).
A MagPro R30 stimulator (Medtronic Inc., Denmark) equipped with a figure-of-eight coil was used to deliver stimulation over the leg motor area of the primary motor cortex (M1). The stimulation site was determined by identifying the hotspot that elicited the most consistent motor-evoked potential (MEP) of the tibialis anterior muscle near the Cz location according to the international 10–20 system. In the low-frequency rTMS group, stimulation was delivered over the contralesional (unaffected) lower-limb motor cortex to reduce excessive interhemispheric inhibition from the non-lesioned hemisphere, whereas in the high-frequency rTMS group, stimulation was delivered over the ipsilesional (affected) lower-limb motor cortex to facilitate cortical excitability in the lesioned hemisphere (Murase et al., 2004; Rossini et al., 2015). The sham stimulation was delivered over the same ipsilesional lower-limb motor cortex position using the high-frequency setup, but with the coil rotated 90° to prevent effective cortical stimulation. The resting motor threshold (RMT) was defined as the minimum stimulus intensity required to evoke MEPs of ≥50 µV in at least 5 out of 10 trials while the participant was completely relaxed.
Statistical Analysis
Statistical analyses were performed using SPSS software (version 22.0; IBM Corp., Armonk, NY, USA). As the study was conducted by a small research team, data collection and statistical analyses were performed by the same investigator. However, group allocation was coded prior to statistical analysis to minimize potential bias. Descriptive statistics are presented as mean ± standard deviation. The normality of data distribution was assessed using the Shapiro–Wilk test.
To evaluate the effects of the intervention, a two-way mixed-design analysis of variance (ANOVA) was conducted for each outcome variable, with time (pre-intervention vs. post-intervention) as the within-subject factor and group (low-frequency rTMS, high-frequency rTMS, sham) as the between-subject factor. The main effects of time and group, as well as the group × time interaction effect, were examined.
When a significant interaction effect was observed, post hoc analyses with Bonferroni correction were performed to determine pairwise differences. For within-subject effects involving more than one degree of freedom, Mauchly's test of sphericity was applied, and Greenhouse–Geisser corrections were used when the assumption of sphericity was violated.
Effect sizes were calculated using partial eta squared (η2p) for ANOVA results. Statistical significance was set at p < 0.05.
Results
General Characteristics of Participants
A total of 39 participants completed the study and were included in the final analysis (low-frequency rTMS, n = 13; high-frequency rTMS, n = 13; sham, n = 13). The demographic and baseline clinical characteristics of the participants are presented in Table 1. There were no significant between-group differences in these variables (p > 0.05). Baseline RMT values also did not differ significantly among groups (p > 0.05).
General Characteristics of Participants (Mean ± SD).
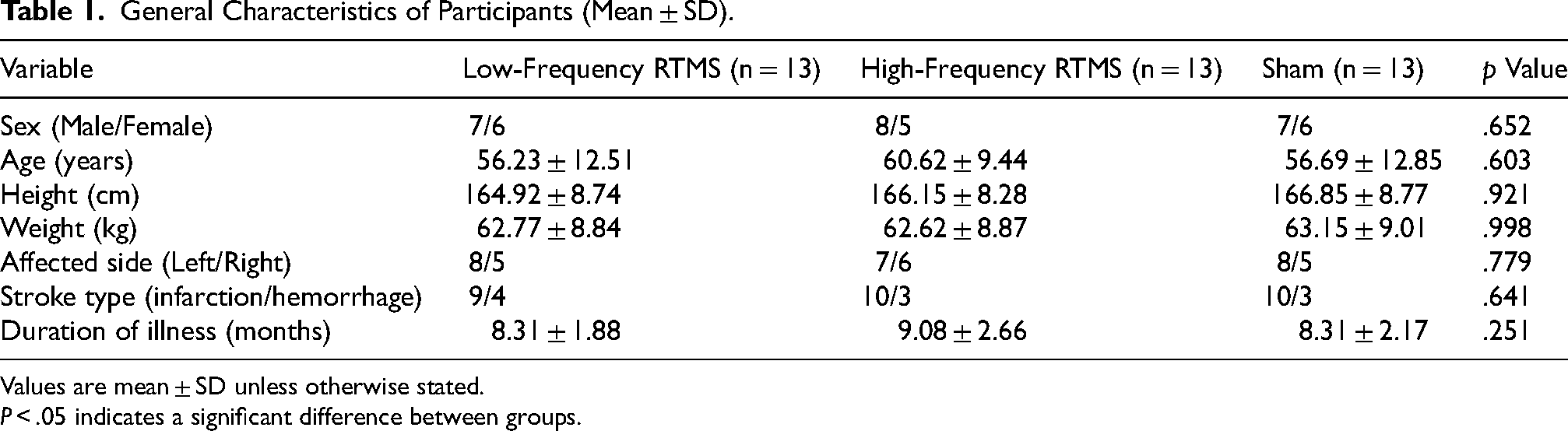
Values are mean ± SD unless otherwise stated.
P < .05 indicates a significant difference between groups.
Clinical Outcomes
Timed Up and Go (TUG)
TUG demonstrated a significant group × time interaction together with a significant main effect of time (Table 2). Post hoc pairwise comparisons confirmed significantly greater post-intervention improvement in the low-frequency rTMS group than in the high-frequency and sham groups. The differential post-intervention response across groups, including statistically significant post hoc between-group differences, is illustrated in Figure 1.
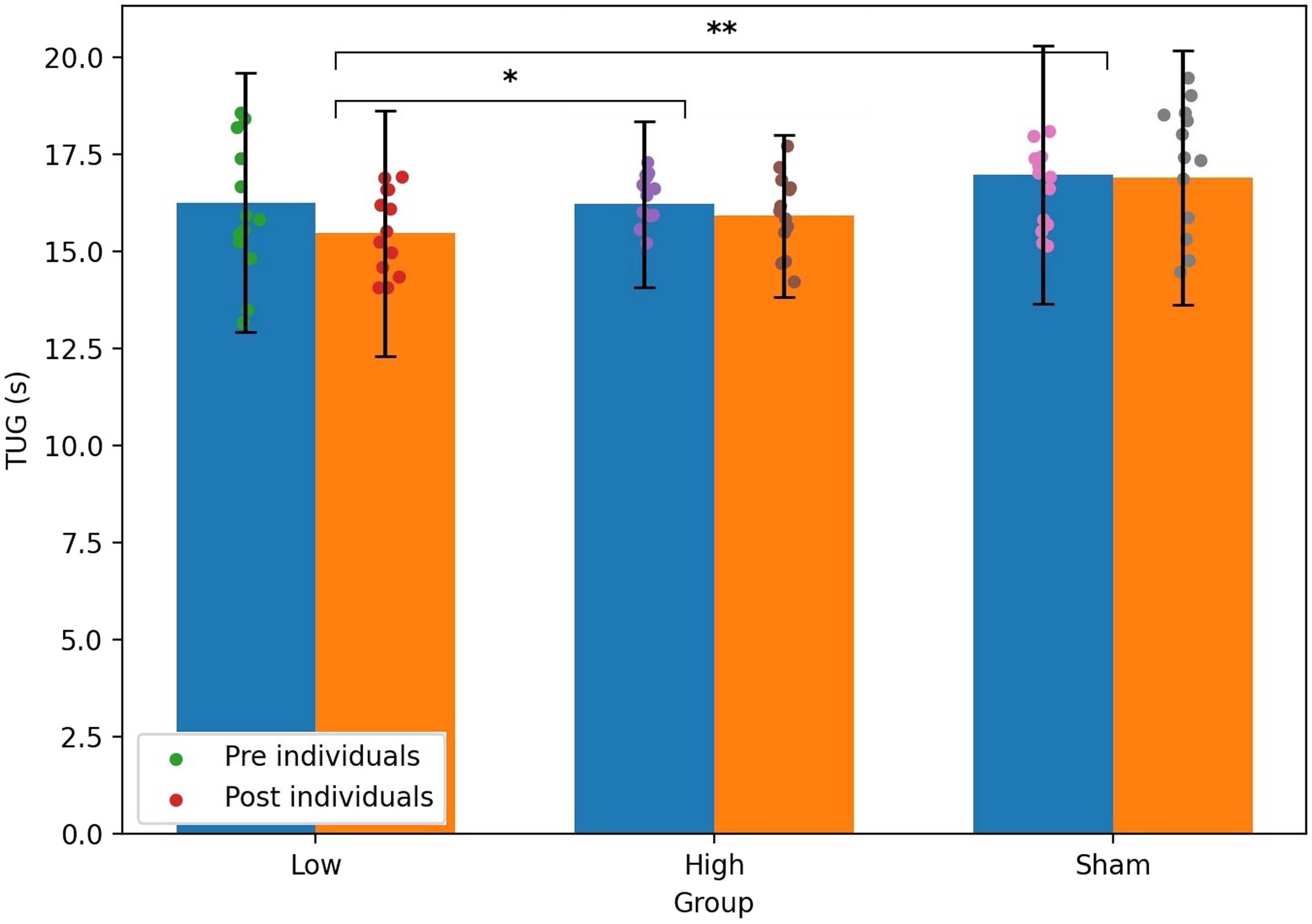
Pre- and post-intervention changes in Timed Up and Go performance across the low-frequency rTMS, high-frequency rTMS, and sham groups. Bars indicate mean values, error bars represent standard deviations, and dots represent individual participants. Asterisks indicate statistically significant post hoc between-group differences at post-intervention (*p < 0.05, **p < 0.01).
Pre- and Post-Intervention Outcomes and Mixed-Design ANOVA Results.
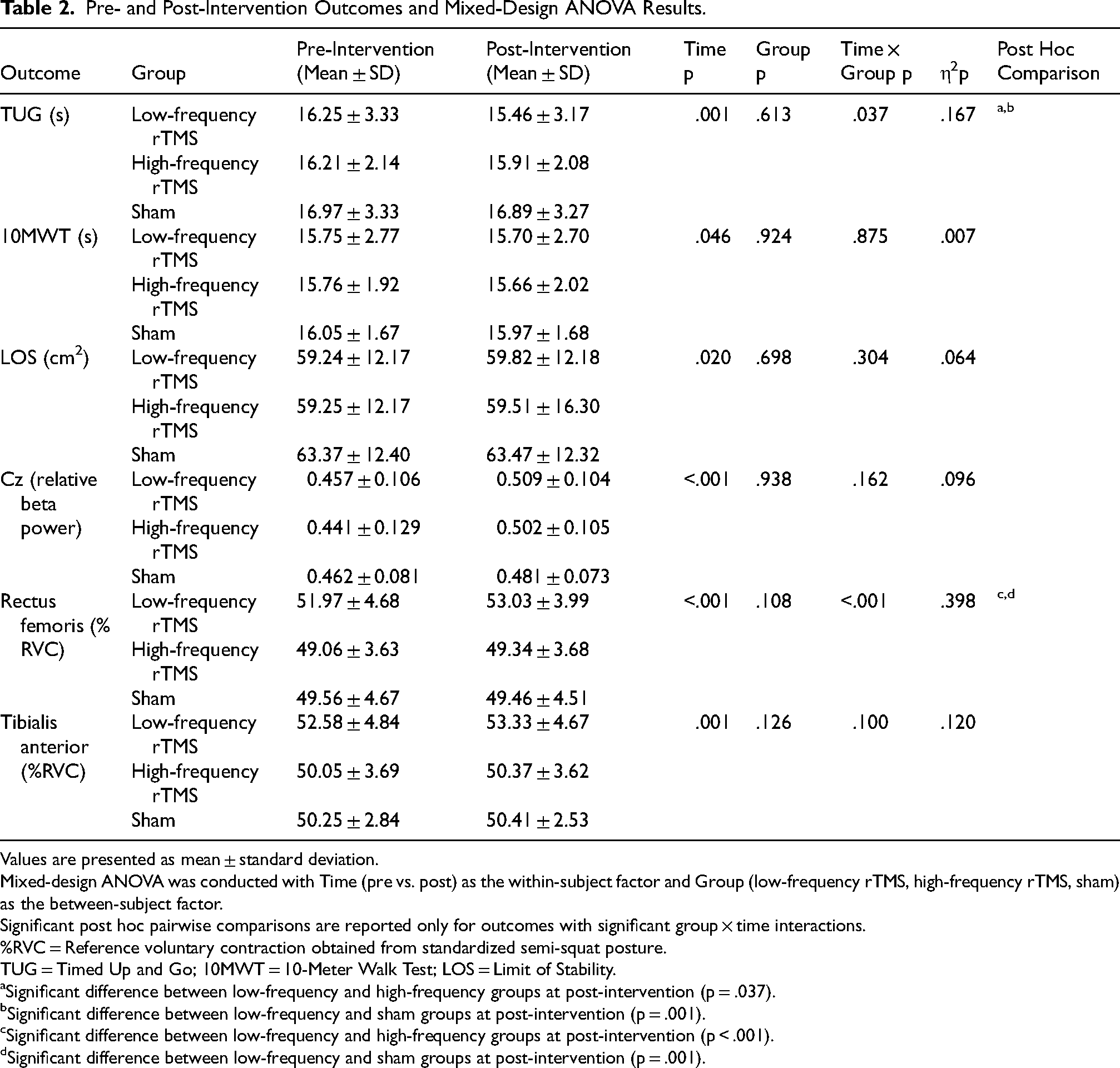
Values are presented as mean ± standard deviation.
Mixed-design ANOVA was conducted with Time (pre vs. post) as the within-subject factor and Group (low-frequency rTMS, high-frequency rTMS, sham) as the between-subject factor.
Significant post hoc pairwise comparisons are reported only for outcomes with significant group × time interactions.
%RVC = Reference voluntary contraction obtained from standardized semi-squat posture.
TUG = Timed Up and Go; 10MWT = 10-Meter Walk Test; LOS = Limit of Stability.
aSignificant difference between low-frequency and high-frequency groups at post-intervention (p = .037).
bSignificant difference between low-frequency and sham groups at post-intervention (p = .001).
cSignificant difference between low-frequency and high-frequency groups at post-intervention (p < .001).
dSignificant difference between low-frequency and sham groups at post-intervention (p = .001).
10-Meter Walk Test (10MWT)
For 10MWT, only a significant main effect of time was observed, whereas neither the interaction effect nor the group effect reached significance (Table 2). This indicates that gait speed improved similarly across all groups over time.
Limits of Stability (LOS)
LOS also demonstrated a significant main effect of time without significant group or interaction effects (Table 2), suggesting general improvement across groups rather than a frequency-specific intervention effect.
Electroencephalography (EEG) Outcomes
Relative beta-band power at the Cz electrode site showed a significant main effect of time only (Table 2), indicating an overall increase across groups from pre- to post-intervention.
Surface Electromyography (sEMG) Outcomes
Rectus femoris activation demonstrated a significant group × time interaction as well as a significant main effect of time (Table 2). Post hoc pairwise comparisons confirmed significantly greater post-intervention increases in the low-frequency rTMS group than in the high-frequency and sham groups. Group-wise changes, individual variability, and statistically significant post hoc between-group differences are illustrated in Figure 2.
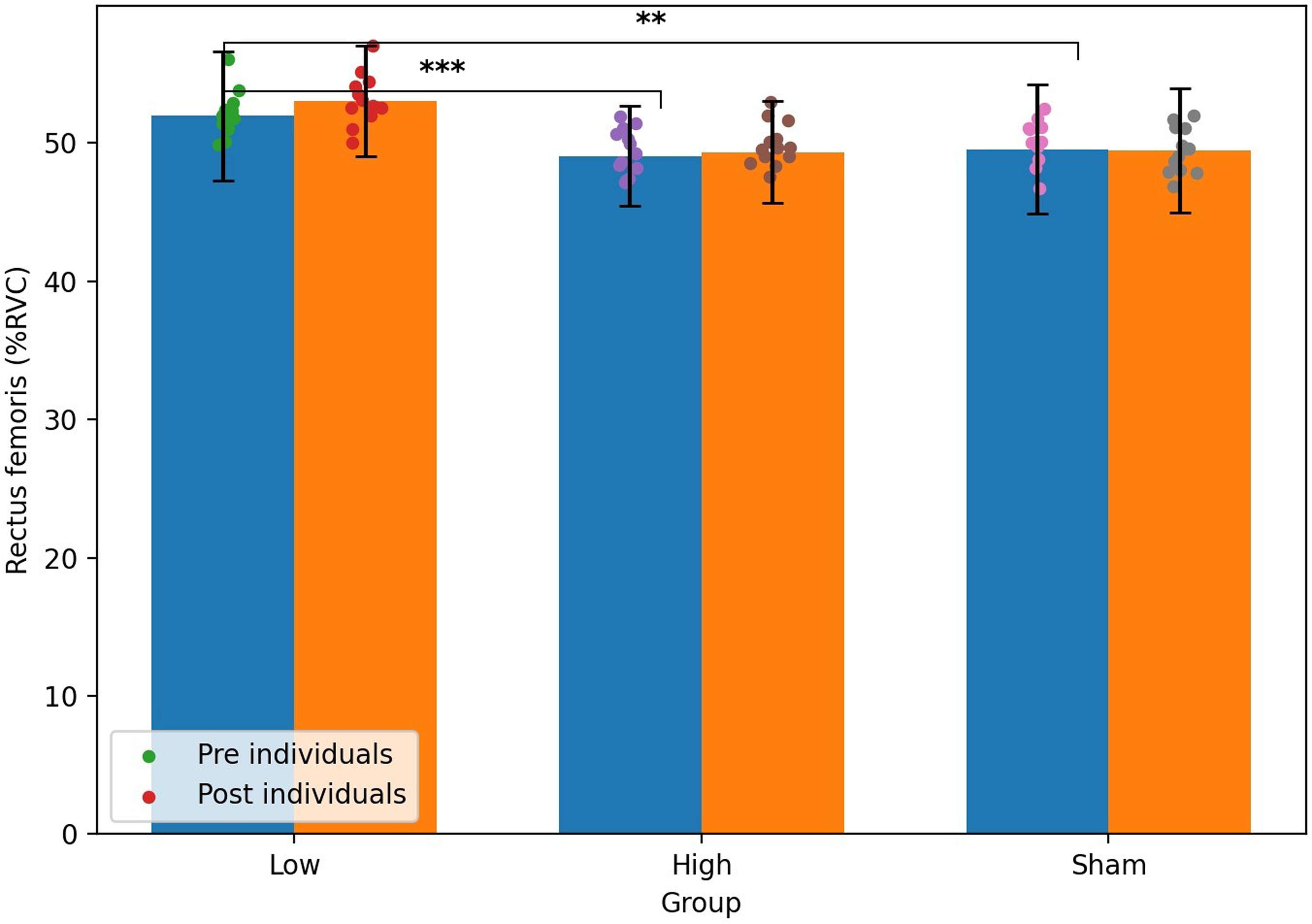
Pre- and post-intervention changes in rectus femoris muscle activation (%RVC) across the low-frequency rTMS, high-frequency rTMS, and sham groups. Bars indicate mean values, error bars represent standard deviations, and dots represent individual participants. Asterisks indicate statistically significant post hoc between-group differences at post-intervention (**p = 0.001, ***p < 0.001).
Tibialis anterior activation showed a significant main effect of time only, whereas no significant interaction or group effects were observed (Table 2), indicating a similar increase across all groups. No significant effects were found for biceps femoris or gastrocnemius activation.
Discussion
The present study examined the effects of contralesional low-frequency (1 Hz) and ipsilesional high-frequency (10 Hz) rTMS applied over the lower-limb motor cortex in individuals with chronic stroke. Significant group × time interactions were identified for rectus femoris activation and TUG performance, indicating differential changes in proximal muscle recruitment and dynamic functional mobility according to stimulation frequency. In contrast, relative beta-band activity at the Cz electrode site demonstrated a significant main effect of time without a significant interaction, suggesting an overall increase in motor-related cortical activity regardless of stimulation frequency. No differential effects were observed for gait speed (10MWT) or LOS, where only time effects were detected. Collectively, these findings indicate that short-term rTMS may be associated with improvements in transitional mobility and selected neuromuscular outcomes, whereas frequency-dependent effects were less evident in global gait and resting cortical measures.
Functional Mobility and Balance Outcomes
The most clinically relevant finding of the present study was the significant group × time interaction observed for TUG performance. This interaction suggests that the magnitude of improvement in dynamic functional mobility differed among groups following the intervention period. Post hoc pairwise comparisons confirmed that the low-frequency rTMS group demonstrated greater improvements in TUG performance compared with the high-frequency and sham groups, suggesting that low-frequency stimulation may be more effective for improving transitional mobility. Although both low- and high-frequency rTMS were associated with reductions in TUG completion time, the presence of an interaction effect indicates that stimulation frequency may differentially influence components of transitional mobility and dynamic balance control.
In contrast, gait speed (10MWT) and LOS demonstrated significant main effects of time without significant interaction effects. These findings suggest that general improvements over time occurred across groups, which may reflect nonspecific rehabilitation effects, repeated testing, or spontaneous adaptation rather than frequency-specific neuromodulatory effects. Similar patterns have been reported in stroke rehabilitation studies suggesting that dynamic functional measures may be more sensitive to short-term interventions, although such changes may also reflect general rehabilitation effects rather than neuromodulation alone (Jia et al., 2025).
The TUG test captures multiple components of functional mobility, including sit-to-stand transitions, turning, and dynamic postural control, which require coordinated proximal muscle activation and rapid sensorimotor integration (Chan et al., 2017). Such task complexity may render TUG more sensitive to short-term cortical modulation than isolated gait speed measures. Previous meta-analyses have suggested that rTMS-related improvements in gait parameters often emerge when stimulation is combined with task-oriented training or delivered over longer intervention periods (Fisicaro et al., 2019; Jia et al., 2025). Accordingly, the lack of frequency-specific effects for 10MWT and LOS in the present study may reflect the relatively short intervention duration and the moderately high baseline functional status of the participants.
EEG beta-Band Activity
In the present study, relative beta-band power at the Cz electrode site demonstrated a significant main effect of time without a significant group × time interaction. This pattern suggests that repeated rTMS was associated with an overall increase in motor-related cortical activity across groups rather than a clear frequency-specific cortical modulation.
Beta oscillations are widely regarded as markers of motor planning, sensorimotor integration, and postural control rather than direct indicators of corticospinal excitability (Cassim et al., 2000; Zrenner et al., 2018). Therefore, the observed increase in beta activity may reflect enhanced engagement or stabilization of motor network dynamics following repeated stimulation. Importantly, the absence of an interaction effect suggests that cortical activity changes occurred similarly across all groups, including the sham group, indicating that these changes may reflect general rehabilitation or repeated testing effects rather than frequency-specific rTMS effects.
Unlike upper-limb motor control, which is strongly dependent on lateralized corticospinal projections, lower-limb motor control involves substantial bilateral cortical contributions and subcortical pathways. Consequently, frequency-dependent modulation based on a strict interhemispheric competition framework may be less pronounced for lower-extremity networks (Edwards et al., 2023). The present findings are consistent with a model in which rTMS influences distributed motor-network activity rather than producing sharply differentiated oscillatory changes at rest.
It should also be noted that resting-state EEG was used as an index of baseline motor-related cortical dynamics, and direct measures of corticospinal excitability, such as motor-evoked potentials, were not obtained. Accordingly, the present findings cannot establish whether the observed oscillatory changes correspond to facilitatory or inhibitory shifts in corticospinal output.
Lower-Limb Muscle Activation
A significant group × time interaction was observed for rectus femoris activation, indicating that changes in proximal muscle recruitment differed among groups following the intervention. Post hoc pairwise comparisons further confirmed greater increases in rectus femoris activation in the low-frequency group compared with the high-frequency and sham groups, indicating a preferential effect of low-frequency stimulation on proximal muscle recruitment. This finding suggests a frequency-dependent modulation of neuromuscular activation patterns associated with rTMS applied over the lower-limb motor cortex. In contrast, tibialis anterior demonstrated a significant main effect of time without a significant interaction, and no meaningful changes were observed in biceps femoris or gastrocnemius activation.
The rectus femoris, as a biarticular muscle coordinating hip flexion and knee extension during gait transitions, may play a critical role in proximal motor control (Frigo et al., 2020). The presence of an interaction effect specifically in this muscle suggests that stimulation frequency may differentially influence proximal motor network recruitment rather than distal or steady-state muscle activation. Given that the TUG test also demonstrated a significant interaction effect, the observed modulation of rectus femoris activation may partially explain frequency-dependent differences in dynamic mobility performance. The relatively large effect size observed for this interaction further supports the clinical relevance of frequency-dependent modulation in proximal muscle activation. These findings suggest clinically meaningful improvements in proximal motor control related to functional mobility.
In contrast, the absence of interaction effects in tibialis anterior and distal musculature suggests that short-term rTMS may preferentially influence proximal motor strategies before producing measurable changes in distal or fine motor coordination. This proximal-dominant pattern aligns with previous observations that recovery of postural and transitional control may precede refined gait adjustments in stroke rehabilitation.
Nevertheless, substantial inter-individual variability was observed, and lesion characteristics were not stratified in the present analysis. Therefore, the frequency-dependent effects observed in rectus femoris activation should be interpreted cautiously and warrant further investigation in larger, stratified cohorts.
Limitations
Several limitations of this study should be considered. Although participants were blinded to group allocation, operator blinding was not feasible due to the nature of the rTMS intervention, and the sham condition was based on the high-frequency protocol to reproduce comparable sensory input rather than to implement frequency-matched sham controls. These factors may have influenced nonspecific treatment effects.
In addition, EEG beta-band activity was used as an indirect marker of motor-related cortical activity, and direct measures of corticospinal excitability such as motor-evoked potentials were not assessed. While EEG provides information regarding distributed motor network dynamics, the absence of MEP measurements limits conclusions regarding specific corticospinal mechanisms.
Furthermore, lesion characteristics were not stratified, the intervention duration was relatively short, and the sample size was modest, which may have limited the ability to detect small changes in gait outcomes and may restrict generalizability. Future studies incorporating longer intervention periods, multimodal neurophysiological assessments, and lesion-based stratification are warranted.
Conclusion
In conclusion, the present study demonstrated that short-term contralesional low-frequency and ipsilesional high-frequency repetitive transcranial magnetic stimulation (rTMS) applied over the lower-limb motor cortex was associated with selected neuromuscular and functional improvements in individuals with chronic stroke. Significant frequency-dependent effects were observed for rectus femoris activation and TUG performance, indicating that low-frequency rTMS may preferentially facilitate proximal muscle recruitment and dynamic transitional mobility.
In contrast, relative beta-band activity at the Cz site, gait speed, and limits of stability demonstrated overall time-related improvements without clear frequency-specific differentiation. These findings suggest that short-term rTMS may exert more distinct frequency-dependent influences on selected neuromuscular strategies than on global steady-state gait parameters.
Given the short intervention duration, modest sample size, and the absence of direct corticospinal excitability measures, the present findings should be interpreted cautiously. Future studies incorporating longer stimulation periods, multimodal neurophysiological assessments, and lesion-stratified analyses are warranted to further clarify the mechanistic specificity and clinical relevance of frequency-dependent rTMS in stroke rehabilitation.
Footnotes
Acknowledgements
The authors thank all participants and clinical staff of Wise Rehabilitation Hospital for their cooperation and contribution to this study.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of Wise Rehabilitation Hospital, Gwangju, Republic of Korea (IRB No. 202410-WR-01). All participants provided written informed consent prior to participation.
Consent for Publication
Not applicable.
Authors’ Contributions
M.S.N. designed the study, collected and analyzed the data, and drafted the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The data that support the findings of this study are not publicly available due to privacy and ethical restrictions involving patient information. However, de-identified data are available from the corresponding author upon reasonable request and with permission from the Institutional Review Board of Wise Rehabilitation Hospital (IRB No. 202410-WR-01).