
Abstract
Objective
This study aimed to evaluate cyclophosphamide contamination in community pharmacies, investigate patient-mediated transfer and indirect risks to the public, and examine the association between the use of hospital closed system transfer devices (CSTDs) and this contamination.
Methods
Wipe samples from patient counselling counters at 24 community pharmacies near 10 hospitals were analysed for cyclophosphamide contamination using liquid chromatography-mass spectrometry. A questionnaire survey was conducted to assess CSTD use and cleaning practices.
Results
Contamination was detected in 5/24 pharmacies (20.8%; median level: 0.7 ng/625 cm2). The overall median across the 24 pharmacies was below the limit of quantification, which does not necessarily indicate absence of contamination. Moreover, four of the five pharmacies with contamination did not have cyclophosphamide in stock during the sampling period. Contamination was observed irrespective of hospital CSTD use or the pharmacy’s handling of cyclophosphamide.
Conclusions
Cyclophosphamide contamination detection on patient counselling counters in community pharmacies may be a result of patient-mediated transfer. However, alternative sources within pharmacies, such as inventory, packaging, and local handling, cannot be ruled out. Contamination was detected in settings with and without hospital CSTD use, indicating that CSTDs address handling-related contamination but do not mitigate patient-mediated pathways.
Introduction
In recent years, healthcare workers have faced various health risks from exposure to anticancer drugs used in chemotherapy, including skin damage, reproductive toxicity, and carcinogenicity, necessitating appropriate preventive measures.1–3 In 2022, the International Society of Oncology Pharmacy Practitioners (ISOPP) revised and published the ISOPP Standards for the Safe Handling of Cytotoxics, which outlines specific safety practices for healthcare professionals handling cytotoxic drugs and emphasises the need for organisation-wide commitment. 4 Many anticancer drugs used in chemotherapy are classified as hazardous. The term ‘hazardous drugs’ was introduced by the American Society of Health-System Pharmacists in 1983 to describe drugs, including anticancer agents, which may pose health risks to healthcare professionals.5,6 Since then, various guidelines have been developed for the safe handling of hazardous drugs, including a 2004 alert issued by the U.S. Centers for Disease Control and Prevention’s National Institute for Occupational Safety and Health.7,8 Additionally, the U.S. Pharmacopeia General Chapter <800> provides detailed standards for handling hazardous drugs to promote patient safety, worker safety, and environmental protection. 9
Occupational exposure to anticancer agents is a significant concern for healthcare workers inside and outside hospital settings. Cyclophosphamide, which is classified as carcinogenic to humans (group 1) by the International Agency for Research on Cancer, 10 has been experimentally proven to be volatile and mutagenic even at room temperature, and the risk of inhalation exposure to healthcare workers is of particular concern. 11 Therefore, closed system transfer devices (CSTDs) are widely adopted to mitigate this risk. However, recent studies have shown that dermal exposure from contact with contaminated surfaces is the predominant route of occupational exposure, which sometimes presents a higher risk than inhalation.12,13 This finding highlights the importance of considering inhalation and dermal pathways in evaluating the safety of healthcare workers.12–14 These devices are specifically designed to maintain a closed transfer pathway for hazardous drugs, preventing the release of aerosols, vapours, and droplets into the surrounding environment during drug preparation and administration. This also protects the drugs from external contamination. Beyond the well-documented occupational risks to healthcare workers, a concern has been raised about the potential for hazardous drug residues, such as cyclophosphamide, to spread to environments outside hospitals, including community pharmacies. Consequently, posing an indirect risk to patients, their families, and the general public. The management of these risks is crucial to maintaining patient safety and ensuring public health, which necessitates a shift in focus from solely protecting healthcare workers to ensuring a safe environment for all individuals who visit clinical settings.
Previous studies have detected cyclophosphamide in the home toilets and in the sweat and saliva of patients receiving cyclophosphamide-containing regimens,15–18 indicating the possibility of contamination in other locations frequented by these patients. Specifically, cyclophosphamide is primarily excreted through the urine, which requires particular attention due to its potential for environmental contamination. Furthermore, the volatility of cyclophosphamide increases the risk of airborne spread following toilet use. Beyond urinary excretion, sweat and saliva represent other critical pathways for cyclophosphamide contamination that warrant attention. Scientific literature has extensively reported on the excretion of unmetabolised cyclophosphamide through sweat from patients’ skin, which begins soon after treatment. Studies have detected cyclophosphamide in the sweat of patients receiving cyclophosphamide-containing anticancer agents,17,18 with another study confirming its excretion in saliva. 19 Patients who come into contact with pharmacy counters and waiting room furnishings, for example, while waiting to receive medication instructions, can transfer the cyclophosphamide in their sweat or saliva onto these surfaces. For instance, cyclophosphamide residue may be left behind when patients touch counters while collecting prescriptions or during medication counselling. Therefore, the cyclophosphamide detected on pharmacy counters could originate directly from patients’ skin via sweat excretion, rather than solely from environmental contamination within hospital wards. However, despite the established efficacy of CSTDs in reducing hospital environmental contamination, no reports have evaluated the likelihood that the use of CSTDs indirectly reduces cyclophosphamide transmission from patients to community pharmacies by decreasing environmental contamination within hospitals. Many patients with cancer receive anticancer infusions at hospitals and subsequently fill their prescriptions at community pharmacies. The guidelines classify cyclophosphamide-containing regimens as having moderate to high emetic risk,20–22 leading physicians to prescribe supportive care for nausea and vomiting. Patients receiving cyclophosphamide often visit community pharmacies between the hospital and home, so contamination in these settings may be widespread.
To the best of our knowledge, previous studies have not investigated cyclophosphamide contamination in community pharmacies located near hospitals that use CSTDs. Cyclophosphamide was selected as a sentinel compound for contamination monitoring due to its wide use as an alkylating agent and its well-documented role as a human carcinogen and mutagen. Additionally, its high frequency of usage and environmental detectability make it a representative marker in occupational exposure studies. Therefore, cyclophosphamide was chosen as the target analyte for this study to evaluate potential contamination in community pharmacy settings. This study provides valuable insights into community-level exposure pathways beyond hospital settings. This study aimed to evaluate the prevalence of cyclophosphamide contamination in community pharmacies and investigate the potential for patient-mediated drug dissemination beyond hospital settings. Furthermore, this study examined whether the use of CSTDs in hospitals influenced this contamination.
Methods
Selection of hospitals and community pharmacies
This study included 10 hospitals affiliated with the National Center for Advanced and Specialized Medical Care or the National Hospital Organization, where outpatients received intravenous cyclophosphamide. Community pharmacies participating in the contamination assessment were selected based on consent and proximity to the participating hospitals, prioritising those with higher outpatient prescription demand from the corresponding hospital. The study was conducted between December 2023 and March 2024. A total of 24 pharmacies, nominated by the 10 participating hospitals, were included in the contamination assessment and questionnaire survey.
Measurement of contamination status
Cyclophosphamide contamination on patient counselling counters of community pharmacies was assessed using the wipe sampling method. Accordingly, a 25 × 25 cm frame was placed on the counselling counter from which samples were collected by wiping the area within the frame three times lengthwise and crosswise using a single sterile wipe (approximately 3 × 1 cm) saturated with deionised water (Figure 1). Sampling was explicitly restricted to patient counselling counters to avoid ambiguity about sampling sites; thus, other surfaces were not sampled. Wiping procedures were planned referring to those established and reported for surface sampling of hazardous drug residues by Connor et al.
11
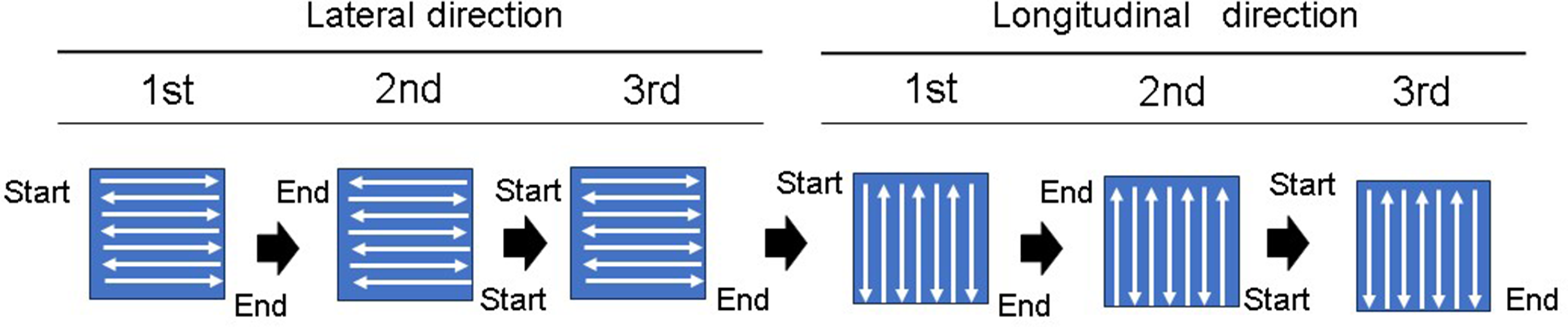
All pharmacists received standardised instructions on the wiping technique (Figure 2). However, specific details, such as the consistent use of protective gloves by all sampling staff and the exact timing of sampling relative to daily operations or cleaning schedules, were not uniformly controlled or recorded across all participating pharmacies. After sampling, the wipes were placed in designated centrifuge tubes and sent via courier to Toshiba Nanoanalysis Corporation for analysis. A research associate prepares the extraction by setting up a 25 × 25 cm frame and wiping the designated area. Wipe method: Standardised wiping procedure. Wipe three times horizontally (i) from the upper left to the lower right without gaps between strokes, (ii) back from the lower right to the upper left, and (iii) repeat as in step (i). Then, wipe three times vertically using the same method.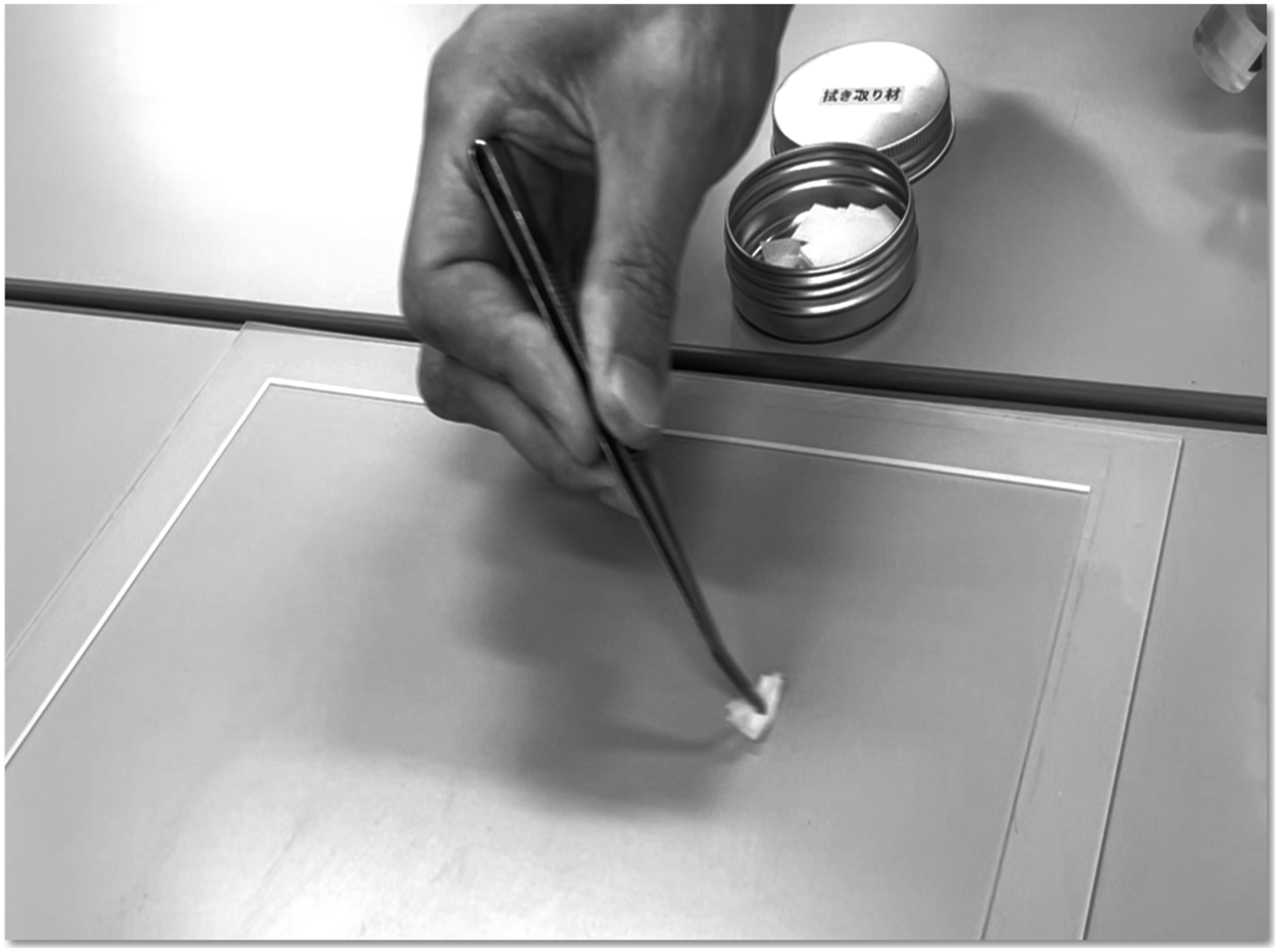
Cyclophosphamide assay method
All cyclophosphamide measurements were conducted by Toshiba Nanoanalysis Corporation (Kanagawa, Japan). The wiped material was placed in a centrifuge tube containing 2 mL of pure water, followed by sonication for 5 min and shaking for an additional 5 min to maximise cyclophosphamide extraction. The solution was subsequently filtered through a 0.2-μm membrane filter to prepare the test solution. Deionised water used for dilution was obtained from the Auto Still R pure water system (WG711, Yamato Scientific, Tokyo, Japan). Calibration solutions were prepared using cyclophosphamide powder (Fujifilm Wako, VA, USA) and test solutions were analysed via liquid chromatography-mass spectrometry (ACQUITY UPLC/TQ-XS, Waters Corporation, MA, USA). Cyclophosphamide-d4 (Toronto Research Chemicals, Toronto, Canada) was used as the internal standard. The limit of quantification of this method was 0.1 ng per 625 cm2 (equivalent to 0.00,016 ng/cm2).
Statistical analysis
Data were summarised using descriptive statistics, including detection frequency, median values, and ranges. Given that this study was exploratory and was not designed or powered to detect between-group differences, no inferential statistical tests were performed. Contamination levels were presented as ng/625 cm2 (sampling area) and normalised to ng/cm2 to facilitate comparison with previous studies.
Questionnaire survey
A questionnaire survey was conducted among the participating hospitals and their neighbouring community pharmacies. The survey was administered with the cooperation of the pharmacy directors of each participating hospital and the managers of community pharmacies. The survey assessed the use of CSTDs in hospitals and the acceptance of cyclophosphamide tablets in aseptic preparation areas in community pharmacies. It also assessed current cleaning practices within these areas, including cleaning frequency and methods. Specifically, questions regarding cleaning frequency inquired about regular cleaning procedures, such as cleaning at least once before opening and again after closing or at similar times. Questions concerning cleaning methods covered techniques such as ethanol wiping, water, and sodium hypochlorite solutions. Furthermore, the survey inquired about the inventory status of cyclophosphamide tablets in community pharmacies.
Results
The actual use of CSTDs in hospitals and the results of the questionnaire for each community pharmacy and the amount of CPA detected.
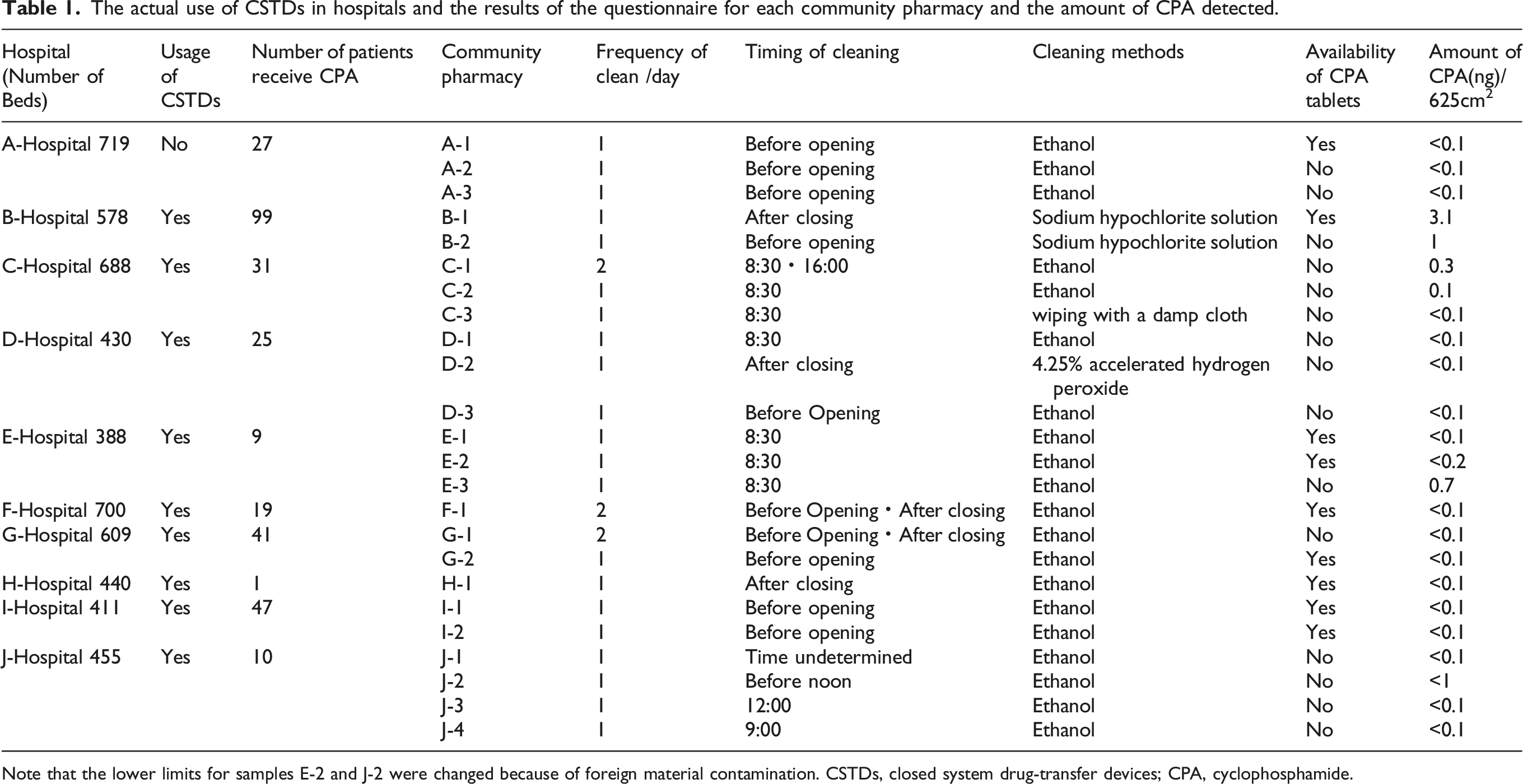
Note that the lower limits for samples E-2 and J-2 were changed because of foreign material contamination. CSTDs, closed system drug-transfer devices; CPA, cyclophosphamide.
Discussion
To the best of our knowledge, this study is the first to report cyclophosphamide detection in community pharmacies, particularly those near hospitals using CSTDs. The significance of this study lies in raising critical questions about patient and public safety in a community setting. This study showed that although the overall median contamination level across all pharmacies was below the LOQ (<0.1 ng/625 cm2; <0.00016 ng/cm2), this does not indicate the absence of contamination. Previous wipe sampling studies have reported trace or sub-quantifiable residues, which may contribute to cumulative occupational exposure.23–25 These findings provide internationally relevant baseline data on patient-mediated contamination pathways, underscoring the need for future interventions, including enhanced cleaning protocols and environmental surveillance in community settings.
Our findings regarding low residue levels are relevant when considered in the context of exposure pathways. Although inhalation exposure has historically received the most attention, recent evidence has demonstrated that dermal exposure from contact with contaminated surfaces is the predominant route of occupational exposure to cytotoxic drugs.12,13 The detection of trace contamination on patient counselling counters, even at sub-quantifiable levels, indicates a tangible risk of contact exposure for pharmacy staff. These findings underscore the importance of adhering to rigorous cleaning practices, consistently using protective equipment and performing environmental monitoring in accordance with international recommendations.26,27
Although CSTDs have been shown to significantly reduce handling-related contamination in hospitals,28–33 systematic reviews have demonstrated that the evidence for a consistent reduction in healthcare worker exposure, as assessed by biological monitoring, remains limited. 32 Additionally, their protective effect does not extend to patient-mediated pathways, such as excretion.
The presence of residues in community pharmacies highlights the limitations of the current safety measures and underscores the need to broaden protective strategies beyond hospital-based handling controls. Previous studies have shown that cyclophosphamide residues may be present in patient excretions, such as sweat and saliva, providing a plausible pathway for surface contamination in pharmacies.15–19 These findings underscore the importance of considering patient-mediated dissemination as a critical component of occupational safety strategies.
In this study, residues were detected on patient-facing surfaces, indicating that direct transmission from patients is a primary contributor. Touching pharmacy counters or furnishings after treatment could transfer drug residues. Given the volatility and potential airborne spread of cyclophosphamide following toilet use, 11 patient excretion should be recognised as a key limitation of existing hospital-based containment strategies. These findings underscore the importance of implementing consistent cleaning practices in accordance with established guidelines, such as the guidelines for safe handling of hazardous drugs 26 and the USP guidelines, 9 with the use of effective decontaminating agents. However, the study results showed contamination in pharmacies without direct handling of cyclophosphamide, indicating that additional pathways should be considered. Although cross-contamination from drug packaging has been documented in pharmacies, 34 this is less likely in our setting, as residues were observed in pharmacies that did not have cyclophosphamide in their inventory. This finding highlights the need for surveillance strategies that extend beyond drug handling to include patient-mediated and indirect contamination routes.15–19
This study showed a maximum cyclophosphamide detection level of 0.0050 ng/cm2 on pharmacy–patient counselling counters. This concentration is far below the doses associated with reproductive or developmental toxicity in experimental models. However, even low-level and sporadic exposure to hazardous drugs has been reported to be associated with adverse outcomes, including reproductive effects and increased cancer risk. 35 No occupational exposure limit has been established for cyclophosphamide, and the relationship between surface contamination levels and actual biological uptake remains unclear.23–25 These uncertainties highlight the need for continued precautionary measures, routine monitoring and research to further define safe exposure thresholds in community settings.
Limitations
This study has some limitations. First, the frequency of patient visits to community pharmacies could not be determined. Therefore, assessing the frequency of potential contamination events is challenging. Second, although the possibility of cyclophosphamide ingestion by pharmacy staff was considered, no staff members reported using cyclophosphamide, reducing the likelihood of this pathway. Third, variability in cleaning practices and timing across pharmacies might have influenced contamination levels, and wipe sampling was not standardised with respect to cleaning schedules. Fourth, the sampling consistency was limited. Training was conducted remotely, glove use was not uniformly enforced and the timing of sample collection (e.g. before or after cleaning) was not standardised, which may have introduced measurement bias. Finally, although this study investigated the relationship between hospital CSTD use and community contamination, differences in CSTD types and nursing practices were not fully considered, which may affect the generalisability of our findings. Further studies employing standardised sampling protocols, controlling for cleaning practices and incorporating detailed patient visitation data are needed to evaluate contamination pathways more reliably.
Conclusions
To the best of our knowledge, this exploratory survey is the first to detect cyclophosphamide residues in community pharmacies, including those without direct handling of cyclophosphamide. The findings indicate that patient-mediated and indirect contamination pathways may exist beyond the hospital setting. Although our findings do not establish causality or evaluate the effectiveness of CSTDs, they underscore the importance of routine monitoring and harmonised cleaning procedures to ensure a safe environment for pharmacy staff and the public. Further studies employing standardised sampling methods and incorporating patient visitation data are needed to identify contamination sources and inform evidence-based preventive strategies.
Footnotes
Acknowledgments
We thank each hospital’s pharmacy director and all community pharmacy managers for cooperating in this study. We also thank Toshiba Nanoanalysis Corporation for preparing the sampling equipment, providing educational support on sampling methods, and assisting with sampling measurements.
Ethical considerations
In consultation with the institution of the principal investigator before the ethics review, ethical approval was not sought for this study because no personal information was involved.
Author contributions
Masato Komuro and Hisanaga Nomura conducted data curation. Masato Komuro, Hisanaga Nomura, and Takahiro Nishimura formulated the research questions, designed the study, and analysed the data. Masato Komuro, Hisanaga Nomura, Daisuke Hisamatsu, Chiaki Ogawa, and Takuma Matsumoto wrote the article. Takahito Furuya, Akio Murakami, Yoshimasa Nagao, Chiaki Ogawa, Takuma Matsumoto, Syuji Horita, Shinya Takada, Ryoko Udagawa, Hisashi Tagashira, Kazuki Fukuda, Fumitaka Shinkai, Daisuke Hisamatsu, Yasuyuki Sakamoto, Seiichi Osaki, Yurina Yasuda, Yusuke Okura, and Tsuneo Maki conducted the study. All authors contributed to study conception, data acquisition and interpretation, drafted or critically revised the manuscript, and participated in the critical review and approval of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a research grant from the National Council of Heads of Pharmacy Departments of National Hospitals. The supporting source had no such involvement or restrictions regarding publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article will be shared on reasonable request to the corresponding author.