
Abstract
Background
Drug-Induced Multisystem Syndromes (DIMS) represent a clinically significant yet under-recognized group of delayed immune-mediated adverse drug reactions characterized by heterogeneous clinical presentations, diagnostic uncertainty, and substantial morbidity. Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) and Drug-Induced Hypersensitivity Syndrome (DIHS) are prototypical conditions within this spectrum.
Methods
This narrative review synthesizes current evidence on the immunopathogenesis, pharmacogenomic susceptibility, clinical manifestations, diagnostic challenges, and pharmacovigilance strategies associated with delayed multisystem drug hypersensitivity reactions. The DIMS framework is proposed as a mechanistic, hypothesis-driven construct intended to enhance pharmacovigilance signal recognition rather than replace existing diagnostic classifications.
Results
DIMS typically develop weeks after drug exposure and involve multisystem inflammatory injury affecting organs such as the liver, kidney, lungs, and heart. T-cell-mediated immune activation, cytokine amplification, and viral reactivation are central pathogenic mechanisms. Mortality varies by syndrome subtype, ranging from approximately 5–10% in DRESS/DIHS to 25–35% in Toxic Epidermal Necrolysis (TEN). Pharmacogenomic factors, including HLA alleles and cytochrome P450 polymorphisms, contribute to susceptibility.
Conclusion
The DIMS framework may support improved early recognition, pharmacovigilance signal detection, and prevention strategies. Integration of pharmacogenomics and artificial intelligence-based analytics may facilitate risk stratification and safer, personalized therapeutic decision-making.
Keywords
Introduction
Drug-Induced Multisystem Syndromes (DIMS) are here conceptualized as a cluster of delayed, immune-mediated drug hypersensitivity reactions characterized by T-cell activation, systemic inflammatory amplification, and involvement of multiple organ systems (e.g., HHV-6, EBV, CMV). 1 DIMS, such as Drug-Induced Hypersensitivity Syndrome (DIHS) and Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), are examples of severe adverse drug reactions that typically occur 2 to 8 weeks after the introduction of a drug, 2 disproportionate involvement of internal organs (e.g., hepatitis, nephritis, myocarditis, or pneumonitis), skin in cancerous areas, fever, and lymphadenopathy. 3 These reactions may be complicated by reactivation of the virus, especially human herpesvirus six and cytomegalovirus, and are often associated with hematologic abnormalities (eosinophilia, atypical lymphocytosis), further augmenting the risk of morbidity and mortality. Mortality varies according to syndrome subtype. DRESS/DIHS is associated with mortality rates of approximately 5–10%. These syndromes are clinically significant due to a High risk of multi-organ failure and mortality (up to 10%), where as SJS/TEN, particularly TEN, within the DIMS spectrum mortality up to 10% carries substantially higher mortality ranging from 25% to over 30%, and even higher in cases complicated by extensive epidermal detachment or multiorgan dysfunction, 4 association with thyroiditis, along with other autoimmune sequelae, even after elimination. 5 Diagnosis is often delayed due to its resemblance to infections or malignancies, leading to inappropriate treatment and potential re-exposure to the offending drug. Management requires lifelong avoidance of the causative and structurally related medications, which may complicate future therapeutic choices. 6 Recent advances in understanding genetic and immunologic predispositions, such as HLA associations, have improved risk stratification and preventive methods. 7 The importance of these syndromes is found in their potential for high morbidity and mortality, their ability to prevent life-saving medications for afflicted patients, and their delayed and difficult diagnosis because of their varied, stepwise, multiorgan symptom presentation. Due to their widespread systemic involvement and long-lasting health consequences, DRESS/DIHS are considered among the most severe forms of drug hypersensitivity, despite being relatively rare. 8 The burden of morbidity and mortality associated with ADRs is still significant worldwide. The age-standardized mortality rate due to adverse effects of medical treatment (AEMT), of which DIMS are a severe subset, has decreased by 36.3% to 3.71 per 100,000 in low-SDI (Socio-Demographic Index) countries, but it is still nearly four times higher than in high-SDI regions, according to recent analyses of Global Burden of Disease data (1990-2021). Although AEMT caused a nearly 40% drop in disability-adjusted life years (DALYs), the absolute figures show enduring disparities, particularly in environments with fewer resources. According to the WHO, serious adverse drug events (SADEs) cause a considerable percentage of deaths, life-threatening circumstances, extended hospital stays, or severe impairment globally. 9 The impact is compounded by late diagnoses, the magnitude and scope of the clinical sequelae, the current diagnostic ambiguity, and under-reporting that increases the need to have strong, internationally coordinated pharmacovigilance. It is only by early clinical detection and systematic reporting and generalizing findings that the healthcare system stands any chance of reducing the severity of such syndromes. 10 This review outlines the variety of clinical presentations and delayed onset of DIMS, such as DIHS and DRESS, highlighting their potential for multi-organ involvement and serious morbidity and death and objective of the introduction of the DIMS concept is not to substitute any of the previous classifications like SCARs, but to highlight a clinically important category of delayed immune-mediated drug hypersensitivity, multisystem adverse drug reactions, which have common pharmacogenomic risk factors such as genetic predispositions (HLA associations) and shared mechanistic pathways such as (T-cell-mediated immune activation) or and medication metabolism variations (CYP Polymorphisms). This conceptual categorization is intended to improve pharmacovigilance signal identification, better risk classification, preventive measures, and inform clinicians, researchers, and policy makers about strategies for better identification, management, and prevention of these rare but severe syndromes. The DIMS construct is proposed as a hypothesis-driven, mechanistic grouping intended to enhance pharmacovigilance signal recognition rather than replace existing diagnostic classifications.
Methodology
A structured narrative literature search was conducted using PubMed, Scopus, and Web of Science. Keywords included “Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS),” “Drug-Induced Hypersensitivity Syndrome,” “severe cutaneous adverse reactions,” “pharmacogenomics,” “HLA allele,” “cytochrome P450 polymorphisms,” “pharmacovigilance,” and “artificial intelligence in adverse drug reaction detection.” Boolean operators were used to combine related terms. Studies were included if they addressed drug-induced hypersensitivity reactions, multisystem adverse drug reactions, pharmacogenomic risk factors, or pharmacovigilance strategies. Peer-reviewed articles published in English were prioritized, particularly those from the last decade, although seminal earlier studies were included where relevant. Articles focusing on non-drug-induced inflammatory syndromes, non-immune toxic reactions, editorials, and poorly indexed sources were excluded. Titles and abstracts were screened for relevance, and full texts of selected studies were reviewed to synthesize current evidence related to DIMS.
Mechanism-based classification of delayed immune-mediated drug-induced multisystem syndromes (DIMS)
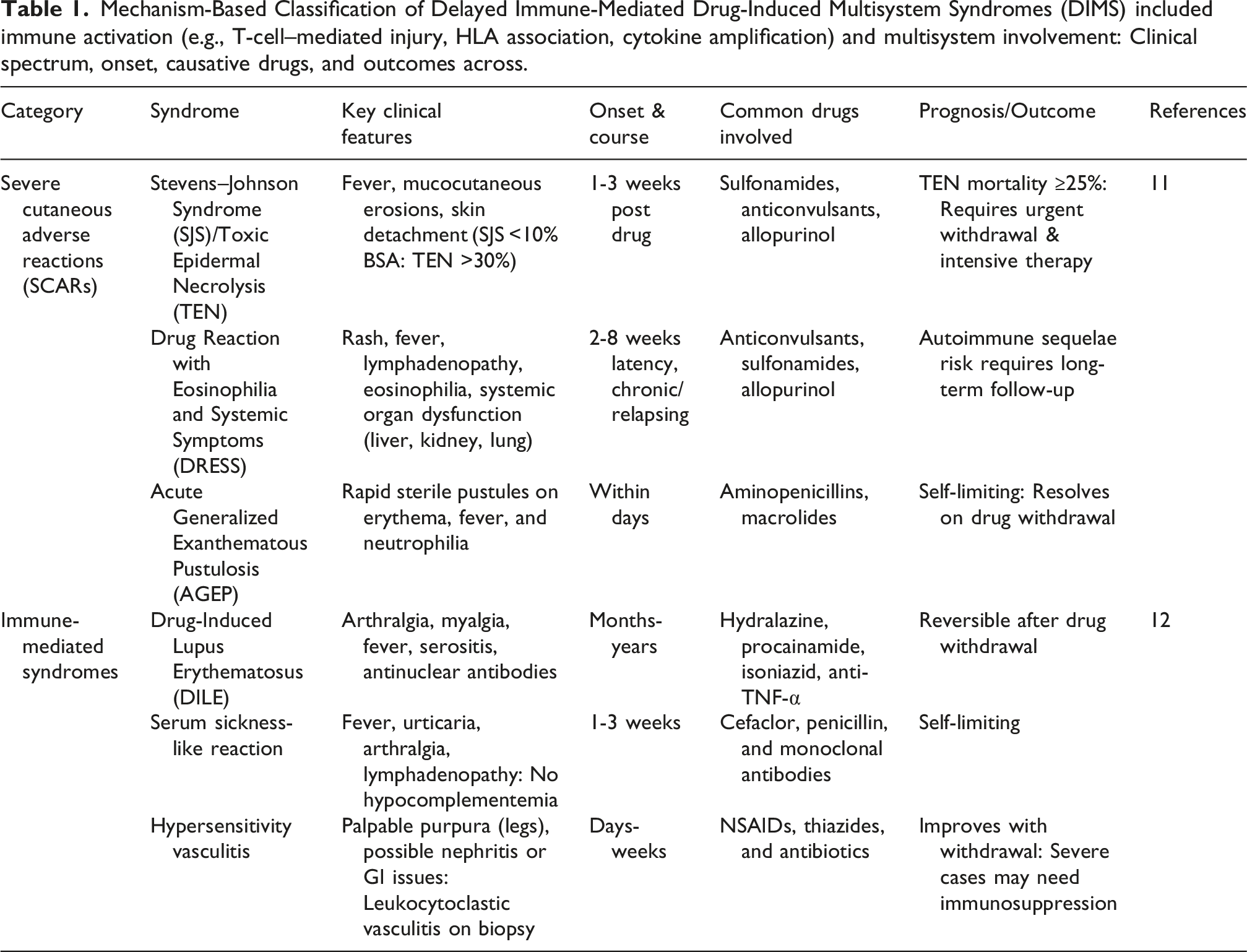
Mechanism-Based Classification of Delayed Immune-Mediated Drug-Induced Multisystem Syndromes (DIMS) included immune activation (e.g., T-cell–mediated injury, HLA association, cytokine amplification) and multisystem involvement: Clinical spectrum, onset, causative drugs, and outcomes across.
Mechanistic insights into immune, genetic, and metabolic pathways
Mechanisms of DIMS focus on immune-mediated injury, pharmacogenomic associations, and drug metabolism polymorphisms.
Immune-mediated injury (T-cells, cytokine storm)
Immune-mediated tissue injury triggered by T-cell activation, Dendritic cells (DCs) uptake drugs/metabolites, express them through drug-modified peptide-HLA, which primes naive T-cells and enhance immune-mediated tissue damage. DAMPs (damage-associated molecular patterns) that are emitted during early hepatic injury stimulate DCs, which connect innate and adaptive immunity. Macrophages and monocyte-derived DCs contribute to the priming of T-cells and the production of cytokines (e.g., TNF-α, IL-6, IL-1) in drug-induced liver injury (DILI), and together with an overwhelming inflammatory response, so-called cytokine storm, is a frequent mechanism underlying DIMS.13,14 T-cell-targeted immunotherapies and several antibody-targeted therapies can lead to excessive cytokine release, including interleukins and interferons, thereby interfering with normal immune regulation and induction of the systemic inflammatory response and multiorgan damage. This cytokine storm is characterized by positive feedback loops between cytokine production and inflammatory cell death that serve to amplify tissue injury and organ dysfunction. The pathogenesis is mediated by the JAK-STAT pathway, Toll-like receptors, inflammasomes including NLRP3, and neutrophil extracellular traps. Therapeutic targeting of inflammatory mediators such as cytokines, chemokines, and related pathways is being studied to ameliorate life-threatening inflammatory responses (Figure 1).15,16 Immunopathogenesis of Drug-Induced Multisystem Syndromes (Illustration of the immune cascade underlying DIMS, including drug or metabolite presentation by antigen-presenting cells, T-cell activation, cytokine amplification, and resulting multisystem tissue injury).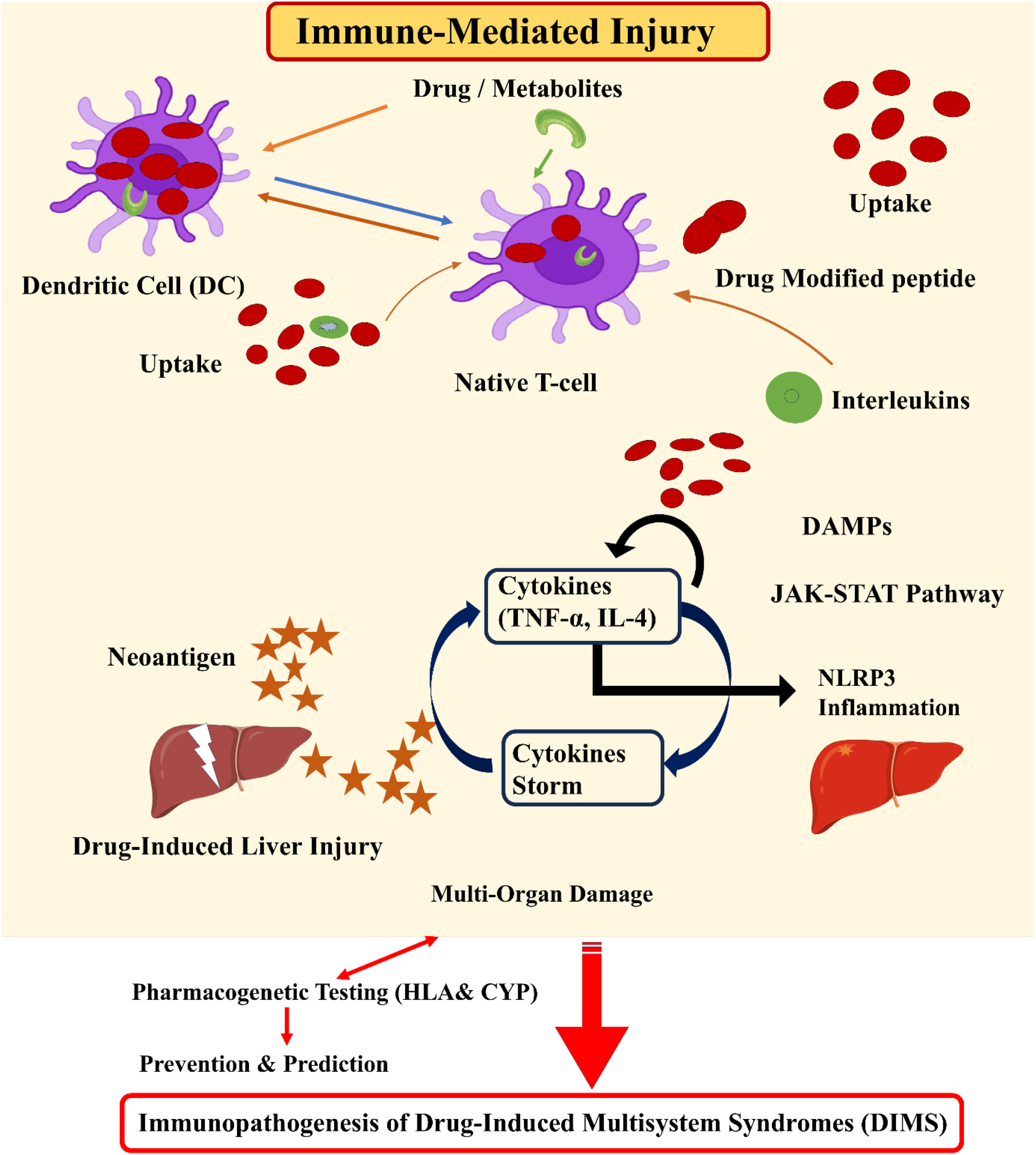
Pharmacogenomic associations (HLA alleles)
Variants of human leukocyte antigen (HLA) genes are closely associated with susceptibility to drug-induced hypersensitivity reactions and to multisystem adverse reactions. Certain HLA alleles, including HLA-B13:01, HLA-B15:02, HLA-B57:01, HLA-B58:01, and others, have been linked to severe cutaneous adverse reactions, drug-induced liver injury, and agranulocytosis (abnormal decrease or absence of a certain type of white blood cell) with drugs such as carbamazepine, abacavir, allopurinol, and flucloxacillin or cephalosporins. These alleles sensitize those individuals to abnormal immune responses resulting from drug molecules or their metabolites. HLA alleles differ among groups, and genetic variability in HLA alleles contributes to risk profiles, making pharmacogenetic testing an important tool for preventing and predicting severe adverse drug responses (Figure 2).17–19 Genetic and Metabolic Susceptibility Factors in DIMS (Overview of pharmacogenomic contributors, including HLA risk alleles and cytochrome P450 polymorphisms that modulate immune response intensity and influence individual susceptibility to multisystem drug reactions).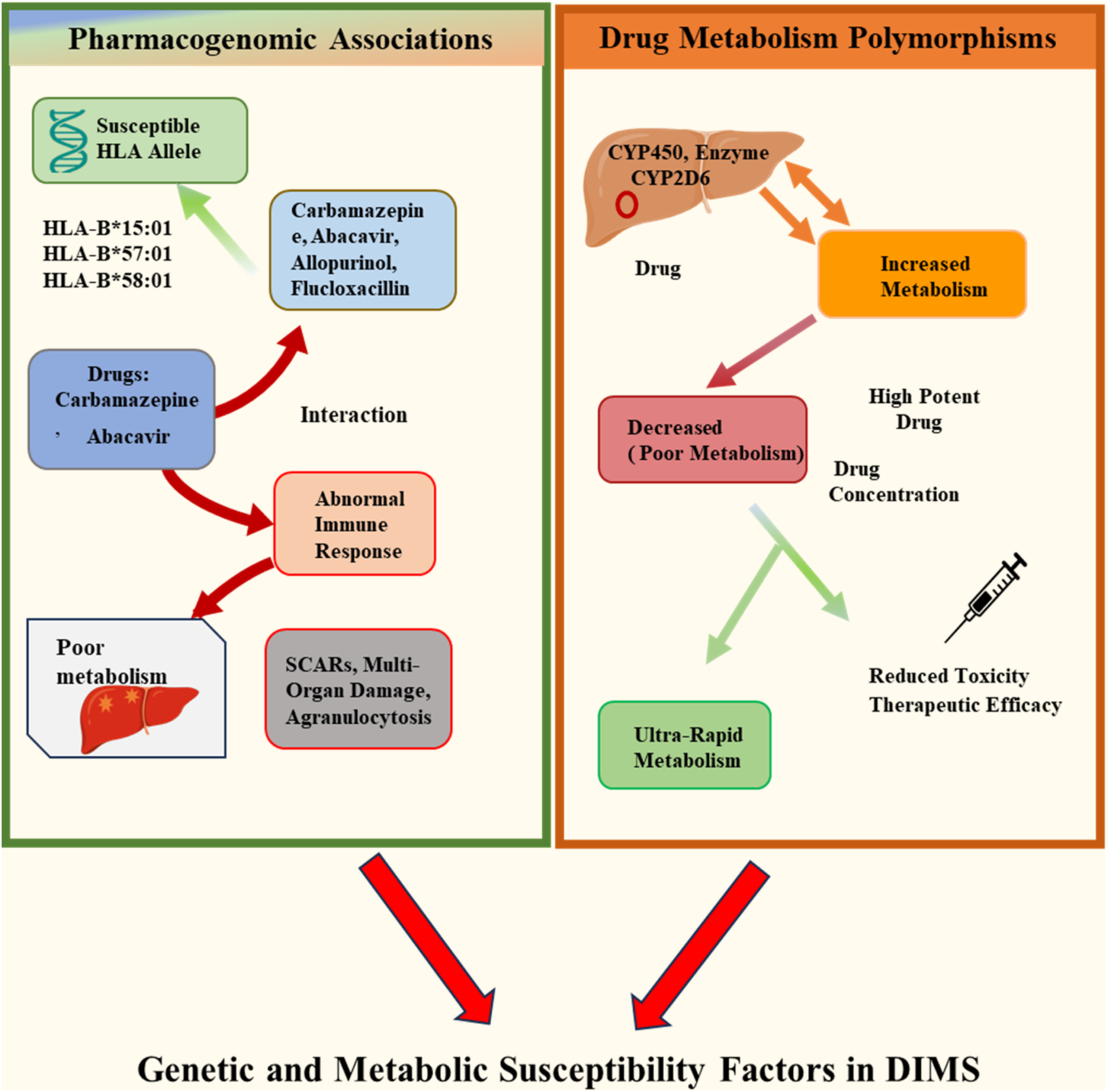
Drug metabolism polymorphisms (CYP polymorphisms)
Polymorphisms in drug-metabolizing enzymes, particularly cytochrome P450 isoforms like CYP2D6, play an important role in multisystem drug responses. Variants in CYP3A4/5 and CYP2D6 may result in five-fold differences in drug metabolism, including metabolic, efficacy, and toxicity risk
Clinical spectrum
Recent clinical reviews note the improvements in the knowledge and diagnosis of DRESS and DIHS syndromes. The contemporary methods involve the use of new biomarkers, the enhanced knowledge of immune mediators like cytokine storm, and the validation of diagnostic certainty scoring systems. Moreover, screening of pharmacogenetic CYP450 polymorphisms and HLA risk alleles is becoming the norm within high-risk populations, which is improving patient safety and drug effectiveness. 22
Syndromic pattern recognition
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) is characterized by a rash (typically maculopapular), persistent high fever, blood eosinophilia (≥1.5 × 109/L or ≥1.5 × 103 cells/µL), lymphadenopathy, and internal organ involvement such as hepatitis (liver transaminases > 2x upper normal), nephritis, and pneumonia. 3 The common presentation is the rash, fever, and eosinophilia, also facial edema, atypical lymphocytosis, and transaminitis. A patient showing these features with a history of drug exposure must raise a high level of clinical suspicion, particularly in agents that are known to cause DRESS. 23
Overlap with infections and autoimmune diseases
DRESS and other DIMS have clinical phenotypes that overlap with infections (e.g., sepsis, viral hepatitis) and autoimmune diseases (e.g., systemic lupus erythematosus (SLE), vasculitis, and inflammatory myopathies). Similar patterns include fever, rash, organ involvement, increased inflammatory markers, and autoantibody formation. Differentiating between drug-induced disease and true infections or autoimmune etiology may involve a complex history of pill usage and exclusion of infectious and autoantibody-driven etiology. There is also diagnostic confusion, as some patients might be harboring latent autoimmune diseases that the drug does not reveal, and the characteristics, such as lymphadenopathy, cytopenia, and complement activation, are shared between the two groups. 24
Diagnostic scoring systems (RegiSCAR for DRESS)
The RegiSCAR (Registry of Severe Cutaneous Adverse Reactions) scoring system is the most widely used and validated tool for diagnosing DRESS syndrome in both children and adults. It is a scoring system based on the acute rash, high fever (>38.5°C)→(+1), lymphadenopathy in two locations, internal organ involvement, lymphocytosis or lymphocytopenia→(+1 per organ, max +2), eosinophilia (>10% or >700cells/µL)→(+1), and thrombocytopenia (<120 × 109/L)→(+1).25,26 In clinical and research settings, patients are categorized as having definite (score >5), Probable/likely (4–5), Possible (2–3), or no case (<2) DRESS, which improves diagnostic accuracy and consistency Bocquet’s and Japanese J-SCAR systems are additional criteria, but RegiSCAR is known for its precision and age-neutral usage. 27
Epidemiology & pharmacovigilance trends
Beyond individual clinical presentations, DIMS also carry significant population-level implications for global pharmacovigilance, with considerable consequences for patient safety and healthcare systems worldwide.
Global burden of ADR syndromes
DRESS/DIHS are estimated to occur in approximately 1 per 1000–10,000 drug exposures and represent a substantial proportion of severe cutaneous adverse reactions globally. 22 Adverse drug reactions cause 0.6 to 7% of hospital admissions worldwide, and severe ADRs cause 3% of overall deaths in the general population. 28 Severe cutaneous adverse reactions, including syndromes of DRESS, SJS/TEN, and AGEP, exhibit variable mortality depending on subtype and severity. DRESS is associated with mortality of approximately 5–10%, depending upon the syndrome and location, 6 whereas SJS demonstrates mortality rates of 5–15%, and TEN carries significantly higher mortality, ranging from 25 to 35%, with rates exceeding 40% in cases complicated by sepsis or multiorgan failure 28 These differences underscore the importance of distinguishing syndrome-specific risk profiles when discussing DIMS-related mortality in epidemiologic and pharmacovigilance analyses. These severe syndromes are more common in populations of East Asia and in areas with increased use of antibiotics 4 According to recent practical research based on pharmacovigilance databases in Asia, Europe, and North America, the incidence and mortality of severe cutaneous adverse drug reactions are higher in regions with more frequent antibiotic and antiepileptic use. Such studies show that population-specific risk factors, such as genetic variations and comorbidities, are present and justify the use of region-specific pharmacovigilance interventions and regular genetic screening where necessary.29,30
WHO-VigiBase & EudraVigilance data
WHO-VigiBase is maintained and developed on behalf of WHO by the Uppsala Monitoring Center (UMC), situated in Uppsala, Sweden. 31 The WHO-VigiBase is the largest global database on medicine safety and, as of February 2025, it has more than 40 million reports of suspected adverse events, such as adverse drug reactions, adverse events following immunization, medication errors, and drug-drug interactions that have been reported by more than 180 countries. 32 EudraVigilance, managed by the European Medicines Agency, serves as the central database for monitoring suspected adverse drug reactions in the European Economic Area. 27 The EudraVigilance database collects data on suspected adverse drug reactions in the EU and publishes it to VigiBase to support global safety surveillance efforts. 27 These databases feature standardized terminologies (MedDRA, WHO Drug Global) and improve signal identification, thus contributing to research and regulatory intervention in rare, severe multisystem disorders. 33
Under-reporting & signal detection challenges
Under-reporting remains a major concern, as spontaneous reporting methods frequently overlook mild or moderate cases and rely primarily on clinician awareness and suspicion, especially for complicated multisystem syndromes. 34 Multiple signal detection techniques are used, but their sensitivity and specificity vary. Rare multisystem syndromes are not always caught efficiently, resulting in missed signals and delayed safety communications. 35 Signal detection can be limited by confounding variables (comorbidity, polypharmacy), masking effects, and data quality so therefore, multimodal approaches that combine spontaneous reports, electronic health records, and cohort monitoring are becoming more and more crucial for reliable tracking. To improve worldwide pharmacovigilance of these syndromes due to under-detection, continual modification of reporting criteria, better awareness, and the use of electronic health records (EHRs) are required. 34
Management and prevention strategies
These syndromes have been associated with significant clinical risk, but enhanced awareness and better understanding of them will bring about optimistic effects, including safer choice of drugs, genotype-based prescribing, and a decrease in preventable severe ADRs by using a targeted approach to pharmacovigilance. Effective management and prevention of DIMS require a multifaceted strategy that integrates early detection, timely intervention, and long-term preventive measures. The immediate withdrawal of the suspected drug remains the fundamental step in management, as prompt discontinuation is consistently associated with improved outcomes and reduced risk of irreversible organ damage (Figure 3), particularly in severe conditions such as DRESS, SJS, TEN, and AGEP. Preventing progression depends heavily on early recognition of characteristic clinical features such as rash, fever, and eosinophilia.
32
Improved recognition of these syndromes also enables safer prescribing and prevention strategies, representing a tangible benefit of enhanced pharmacovigilance. The image illustrates a multifaceted strategy for managing drug-induced multisystem disorders, emphasizing early detection, timely drug withdrawal, supportive therapy (corticosteroids/IVIG), preventive pharmacogenomic screening, and AI-based predictive tools. Together, these approaches aim to improve recognition of severe adverse drug reactions and reduce their incidence through safer, personalized prescribing.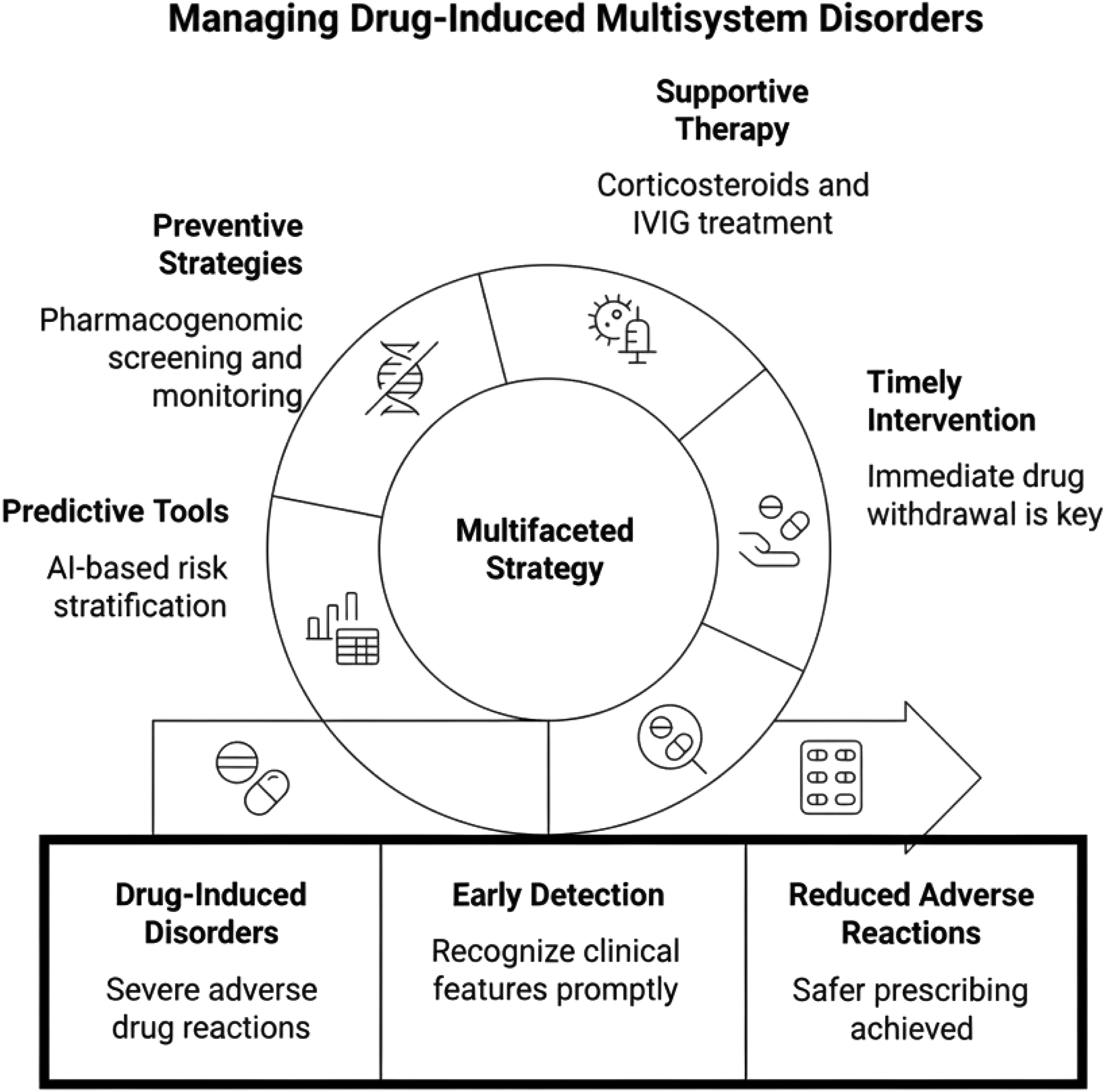
Supportive management plays a vital role once the offending drug is discontinued. The systemic corticosteroids are usually taken as the first agent, particularly when the involvement of internal organs is present. IVIG can be used in cases where patients fail to respond or show life-threatening manifestations. Clinical research indicates that corticosteroids and IVIG will be more effective when used jointly in fast-progressive cases. In case of refractory disease or in case of contraindications to corticosteroids, other immunomodulators like cyclosporine or mycophenolate mofetil can be used to manage the disease, and the choice of one of these agents should be based on the severity of the disease and the presence of comorbid conditions33,36 However, recent systematic reviews indicate the combination of IVIG, steroid-sparing immunomodulators (Figure 3), and customized therapy using the genotype-specific drug discontinuation in the management regimens of acute and refractory cases of DIMS. Risk stratification through genetic testing and AI-based monitoring can improve treatment response and patient outcomes (Figure 3). 23
In addition to acute management, preventive strategies are critical to minimizing the risk of recurrence and safeguarding vulnerable populations. A major advancement has been the pharmacogenomic screening, in which some HLA alleles are known to cause SJS/TEN in response to carbamazepine (HLA-B15:02) and in allopurinol hypersensitivity (HLA-B58:01). Regions where the prevalence of these alleles is high should have regular pre-prescription genetic tests to avoid potentially fatal reactions. 37 In addition to genetic approaches, clinical surveillance by organizing follow-ups, such as regular liver, renal, and hematological tests, and attention to early warning signs, assists clinical intercessors in responding in a timely manner. This is especially useful in patients who have several comorbidities or are on high-risk drugs, since the cases of severe adverse drug reactions decrease considerably. 33
Recent advances are exploring machine learning-driven predictive models to enhance preventive measures. These models combine the pharmacogenetic data, electronic health records, and the history of adverse events to determine high-risk patients, predict drug-drug interactions, and facilitate safer prescribing. Allowing the stratification of risks and prescribing alternative treatment methods, AI-based solutions shine in personalized prevention and can potentially decrease the occurrence and severity of the DIMS.38,39
Future perspective
The future of pharmacovigilance will be based on the application of large-scale genomics, AI, ML, DL, and big data analytics techniques to predict and anticipate multisystem drug reactions. By making personalized choices regarding medication, optimizing dosages, and reducing the global burden of DIMS, clinicians and regulatory agencies can integrate these strategies into routine practice. Recent studies indicate that this kind of integration is most effective in detecting and interfering with early development compared to traditional pharmacovigilance tools.40,41 Emerging strategies for managing DIMS focus on the integration of pharmacogenomics, advanced data analytics, and precision medicine to enhance prevention and therapeutic safety.42,43 One promising direction is the integration of pharmacogenomics with pharmacovigilance, which offers a transformative approach to predicting, preventing, and managing ADRs. By incorporating genetic variants such as HLA-B57:01 and CYP2C9 into safety surveillance, clinicians and regulatory bodies can better identify individuals at heightened risk for severe multisystem syndromes and optimize therapy accordingly.42,44 This approach enables a transition from conventional, generalized prescribing to individualized medication strategies, where pharmacogenetic data are merged with real-time pharmacovigilance signals, thus improving both drug safety monitoring and patient-specific risk assessment across diverse populations. 45
Pharmacovigilance uses artificial intelligence (AI) not only for general signal detection but also machine learning (ML), deep learning (DL), natural language processing (NLP), and network-based modeling. 45 Structured datasets, based on EHRs, pharmacogenomic repositories, and spontaneous reporting systems, have been used to predict ADRs using supervised machine learning algorithms, including random forests, gradient boosting machines, and support vector machines.44,46 Neural networks and transformer-based models are also deep learning architectures that are increasingly used to find latent patterns in large pharmacovigilance databases and genomic datasets.47,48 The AI models used in the framework of DIMS can be based on multidimensional data sources, such as: (1) pharmacogenomic profiles (e.g., HLA alleles, CYP polymorphisms), (2) clinical laboratory parameters (eosinophilia, liver enzymes), (3) history of past medication exposure, and (4) spontaneous safety adverse events reported in databases, such as WHO-VigiBase and EudraVigilance.34,36 Natural language processing methods have been used on unstructured clinical histories and case safety reports to enhance early identification of severe cutaneous adverse reactions. 45 Recent studies indicate that AI-based signal detection algorithms are more sensitive and have an earlier signal detection than conventional disproportionality algorithms in large adverse event databases. 49 Recent pharmacovigilance studies using machine-learning analysis of spontaneous reporting systems have successfully identified signals related to severe hypersensitivity reactions earlier than traditional disproportionality methods. 42 Moreover, predictive modeling methods that involve pharmacogenomic risk alleles as well as demographic and clinical covariates have been promising with regard to the stratification of individuals at high risk of severe hypersensitivity reactions. 47 In practice, in DIMS, the realistic future uses are the development of risk prediction tools, auto-early-warning systems, high-risk drug combinations development, and AI-assisted pharmacogenomic screening platforms to support genotype-guided prescribing. Nevertheless, there are still some challenges, such as heterogeneity of the data, the ability to interpret the model, the presence of algorithmic bias, and the necessity to prospectively validate the model in different populations. 44
The progression toward personalized medicine and safer drug development further strengthens this shift. Advances in genomics, proteomics, and biomarker discovery, complemented by AI-driven analytics, allow for more precise drug selection, personalized dosing regimens, and improved therapeutic efficacy while minimizing adverse outcomes.47,50,51 Incorporating genetic and molecular profiling into clinical trial design also accelerates the development of safer drugs by focusing on genetically defined patient populations. The transition toward precision-based therapeutics is intended to advance patient-centered care, enhance the prediction of adverse drug reactions, and strengthen global drug safety initiatives. Collaborative efforts in data integration, advanced analytical techniques, and genomically informed clinical practice are expected to significantly enhance patient outcomes and reduce the burden of DIMS in the future.52,53
Limitations of the DIMS framework
The DIMS construct is also purposely limited to delayed immune-mediated multisystem drug hypersensitivity reactions, which involve T-cell activation, systemic inflammatory amplification, and, in a few cases, viral reactivation.1,2,5 This differentiation was taken to maintain mechanistic coherence and match the framework to known immunopathogenic models of SCARs and drug-induced hypersensitivity syndromes.4,18 The framework, by design, neglects acute toxic, pharmacodynamic, metabolic, and dose-dependent adverse drug reactions that are not associated with adaptive activation of immune responses. Although such a limitation enhances scientific clarity, it might not be able to identify some kinds of multisystem drug toxicities that do not lie within classical immune mechanisms. Moreover, DIMS is also a hypothesis-based rather than an officially recognized nosological construct, a type of construct of mechanistic clustering. Future validation research that includes biomarker profiling, pharmacogenomic stratification, and standardized diagnostic criteria is needed to identify its clinical reproducibility and predictive power.
Conclusion
From a risk and safety perspective, Drug-Induced Multisystem Syndromes (DIMS) represent a critical target for prevention, early detection, and improved pharmacovigilance strategies. The term “DIMS” is proposed here as a conceptual framework to group delayed immune-mediated multisystem drug hypersensitivity reactions rather than as a replacement for established diagnostic entities. Enhanced recognition of these syndromes not only mitigates morbidity and mortality but also enables safer prescribing practices, genotype-guided therapy, and proactive risk stratification. By framing these conditions within a unified risk-management perspective, the DIMS construct may support more consistent signal detection, reporting practices, and preventive strategies across diverse healthcare systems
Footnotes
Ethical considerations
Not applicable (this article is a review and does not involve human or animal studies).
Authors contributions
All authors contributed to the study conception and design. Formal analysis were performed by [Mohd Haneef], [Ratima Sood], and [Sourabh Kosey]. The first draft of the manuscript was written and data collection by [Uttam Udesh Rai], and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.