
Abstract
Background
Arterial stiffness and endothelial dysfunction are early markers of cardiovascular disease (CVD) risk. While moderate-intensity aerobic exercise has demonstrated vascular benefits in untrained individuals, its acute effects on strength-trained athletes remain unclear.
Objective
This study investigates the impact of a single aerobic session on arterial stiffness and endothelial function in strength-trained throwers and untrained controls.
Methods
Eleven male university throwers and eleven healthy controls participated. Participants completed 30 min of moderate-intensity cycling at 50% of heart rate reserve. Brachial-ankle pulse wave velocity (baPWV) and reactive hyperemia-peripheral arterial tonometry index (RHI) were measured at baseline, immediately after exercise, and 40 min post-exercise.
Results
Arterial stiffness decreased significantly in the controls (p = 0.003) but showed no change in the throwers. Endothelial function, as measured by RHI, improved significantly in both groups post-exercise (p < 0.001). There was no significant difference in RHI improvement between groups.
Conclusions
In the throwers group, a single session of moderate-intensity aerobic exercise did not lead to a significant reduction in arterial stiffness but resulted in an improvement in endothelial function. These findings suggest that while endothelial function in strength-trained throwers can benefit acutely from aerobic exercise, their arterial stiffness may require more intensive or longer-duration aerobic interventions to achieve significant improvements.
Keywords
Introduction
Arterial stiffness and endothelial dysfunction are established early markers of cardiovascular disease (CVD) and are associated with an increased risk of adverse cardiovascular events.1,2 Notably, a 1 m/s rise in pulse wave velocity (PWV) correlates with a 12–13% elevation in cardiovascular events and cardiovascular mortality. 3 Likewise, diminished endothelial function, assessed by the reactive hyperemia-peripheral arterial tonometry index (RHI), has been linked to higher CVD risk. 4
Age-related declines in arterial stiffness and endothelial function underscore the necessity for timely interventions.5,6 Non-trained individuals have been shown to improve both arterial stiffness and endothelial function through regular aerobic exercise.7,8 Furthermore, even a single session of aerobic exercise can have significant acute benefits.9–13 Conversely, strength training, particularly high-intensity regimes, may either exacerbate arterial stiffness or show no effect.14,15 While strength training has demonstrated potential to improve endothelial function, its effects remain inconsistent among young adults. 16 On the other hand, throwing athletes, who habitually engage in high-load resistance training, have been shown to exhibit increased arterial stiffness and elevated endothelin-1 levels. 17 However, previous research reported no significant differences in arterial stiffness between throwers and untrained individuals. 18
In non-trained individuals, combining aerobic and resistance training may offer synergistic benefits for vascular health.19–21 However, the acute vascular effects of aerobic exercise in strength-trained populations like throwers remain poorly understood. We therefore hypothesize that, even in habitual strength–trained throwers, a single session of moderate–intensity aerobic exercise will acutely reduce arterial stiffness and enhance endothelial function. Therefore, this study investigates whether a single session of moderate-intensity aerobic exercise can acutely improve arterial stiffness and endothelial function in strength-trained throwers.
Methods
Study participants
Participants were recruited using a convenience sampling method in collaboration with the university's athletics and general student populations. Inclusion criteria for the Throwers group were as follows: (1) male university student; (2) at least three years of competitive experience in a throwing event (shot put, discus, hammer, or javelin); and (3) training regularly five days per week. Exclusion criteria comprised any history of smoking, regular alcohol consumption, or musculoskeletal or cardiovascular conditions that could limit participation. Eleven eligible Throwers (mean competitive career length: 6.2 ± 2.1 years; training frequency: 2.5–3 h/day, 5 days/week) were enrolled. For the control group, eleven healthy male university students, matched to the Throwers group by age only, were recruited. Exclusion criteria were identical, with the exception that participants must have no current regular exercise habits, no history of smoking or regular alcohol consumption, and no significant musculoskeletal or cardiovascular conditions. To avoid confounding effects of cyclical hormonal fluctuations on vascular measurements, only male participants were recruited. 22 The sample size of eleven participants per group was determined based on previous studies employing similar repeated-measures designs to evaluate acute vascular responses to aerobic exercise. 9 The participants were provided with written and verbal explanations about the purpose, methods, and safety of this study, and consent was obtained from each participant. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. This research was approved by the Kansai University Research Ethics Review Committee (approval number: 2018-04).
Experimental protocol
All testing took place in the Physical Education Laboratory at Kansai University's Central Gymnasium (Senriyama Campus, Suita, Japan). The laboratory—equipped with air conditioning, dimmable lighting, and sound-proofing—was maintained at 24 °C to ensure a quiet, temperature-controlled environment. Participants arrived at least three hours after breakfast and refrained from vigorous exercise for 12 h prior and from consuming caffeine after waking. Upon arrival, they changed into exercise attire in an adjacent changing room, then rested quietly in a waiting area for 15 min to stabilize cardiovascular parameters. Baseline (BL) measurements were obtained in the supine position using the HBP-8000 (Fukuda Colin, Tokyo, Japan) and Endo-PAT2000 (Itamar Medical, Caesarea, Israel) systems to assess pulse wave velocity (baPWV), pulse rate, blood pressure, and the reactive hyperemia index (RHI). Immediately following baseline, participants moved to the neighboring exercise room, where they underwent an aerobic exercise intervention. At exercise cessation (0 min), subjects returned to the measurement room and repeated the baPWV, pulse rate, blood pressure, and reactive hyperemia index (RHI) assessments exactly as at baseline. Subsequently, they remained seated in the same room for a 40-min recovery period, after which a final set of measurements (40 min) was performed. The choice of a 30-min bout of moderate-intensity cycling followed by a 40-min recovery period was directly informed by earlier investigations of vascular responses to acute exercise.9,12 All data were collected by the author, who underwent prior training on both the HBP-8000 and Endo-PAT2000 systems.
Aerobic exercise intervention
Using a bicycle ergometer (Aerobike 75XLII and 75XLIII; Combi Corporation, Tokyo, Japan), the participants were instructed to maintain 60 revolutions/min at 50% of the Heart Rate Reserve (HRR) and cycle for 30 min. In addition, the author asked participants to report any feelings of excessive fatigue, dizziness, or chest discomfort at 5-min intervals and observed for signs of labored breathing or pallor. The ergometer's workload was continuously adjusted: if a participant's heart rate exceeded the target 50% HRR, the resistance was automatically reduced to maintain the prescribed intensity. A 50% HRR has been reported to indicate moderate-intensity cardiorespiratory training. 23
Measurements
Age, competitive history, training frequency, and training duration were assessed via questionnaire. Height was measured to the nearest 0.1 cm using a stadiometer (Seca 213; Seca Japan, Chiba, Japan). Body weight, body mass index (BMI), and body fat percentage were determined using a multi-frequency bioelectrical impedance analyzer (InBody 270; InBody Japan, Tokyo, Japan).
Primary outcome
Measurement of arterial stiffness, pulse rate, and blood pressure
As an index of arterial stiffness, baPWV was measured using a blood pressure pulse wave device. In addition, pulse rate and brachial artery blood pressure were simultaneously measured using this device. BaPWV is a pulse wave velocity obtained by detecting pulse waves both in the upper arms and ankles using a blood pressure measurement cuff and based on the rise time difference and blood vessel length (distance from the aortic valve orifice minus the vessel length to the ankle and upper arm). BaPWV measures the PWV between the brachial and peroneal arteries, is easily measured and reproducible, and is highly correlated with aortic PWV measured by catheterisation. Therefore, it is clinically widely used in Japan as an index of arteriosclerosis. 24 The representative value used for the results was the mean value of the left and right baPWVs.
Measurement of vascular endothelial function
Vascular endothelial function was measured using the reactive hyperemia-peripheral arterial tonometry (RH-PAT) method. RH-PAT was measured using Endo-PAT2000. 25 This measurement method calculates the RHI from the expansion rate of the section corresponding to the test side with the opposite index finger as a control. Bilateral sympathetic nervous system effects are minimised by dividing the expansion rate of the test side by the expansion rate of the control side. Furthermore, this index is considered to reflect vascular endothelial function centred on nitric oxide (NO). 26
Statistical analysis
All data are reported as mean ± standard deviation. The normality of the data was assessed using the Shapiro–Wilk test, which is recommended for small to moderate sample sizes (n < 50). For all outcome variables, including baPWV and RHI, the assumption of normality was met at all time points (pre-exercise, post-exercise, and 30 min post-exercise), except for the RHI values at the pre-exercise time point (p < 0.05). Despite this minor deviation, the distribution was not markedly skewed, and no extreme outliers (defined as values > ± 3 SD from the mean) were observed. Given the robustness of mixed-design ANOVA to slight violations of normality, especially with balanced sample sizes over 10 per group and approximately equal variances, parametric analysis was deemed appropriate. A two-way mixed-design ANOVA (Group × Time) was used to examine the effects of group (Controls vs. Throwers) and time (baseline, post-exercise, and 30 min post-exercise) on each outcome variable. The assumption of sphericity was assessed using Mauchly's test, and Greenhouse-Geisser corrections were applied when sphericity was violated. When the ANOVA revealed a significant difference, post hoc testing was performed using the Bonferroni method. Effect sizes were reported as partial eta squared (η2p), with thresholds for small (0.01), medium (0.06), and large effects (0.14) based on Cohen's guidelines. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 27.0 (IBM Corp, NY, USA), and the statistical significance level was set at less than 5%.
Results
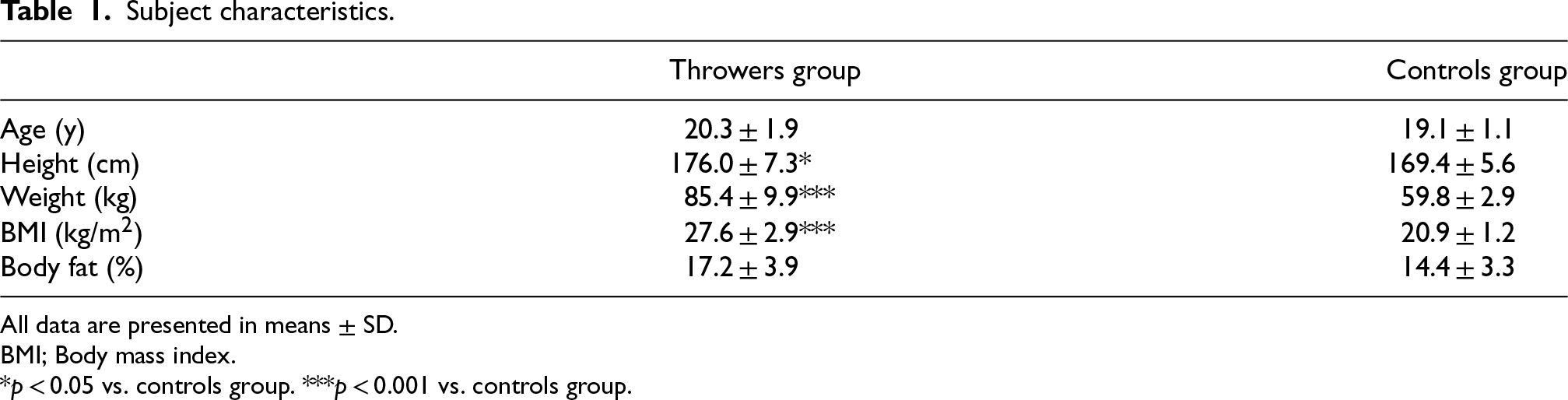
Table 1 presents the characteristics of the study participants. There were no significant differences between the groups in age or body fat percentage. However, height, weight, and body mass index (BMI) were significantly higher in the Throwers group compared to the Controls group (p = 0.028, p < 0.001, and p < 0.001, respectively).
Subject characteristics.
Subject characteristics.
All data are presented in means ± SD.
BMI; Body mass index.
*p < 0.05 vs. controls group. ***p < 0.001 vs. controls group.
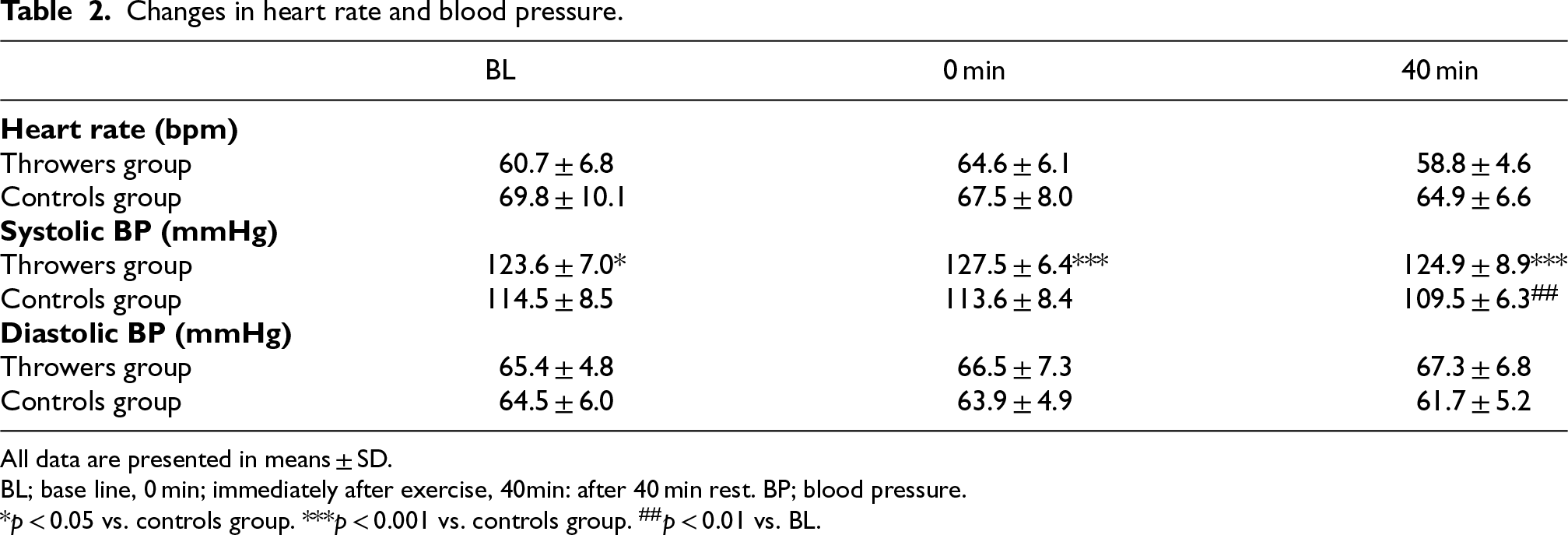
Table 2 presents the results for pulse rate and blood pressure measured at BL, 0 min and 40 min. Two-way ANOVA for pulse rate revealed no significant interaction between groups and time (p = 0.103, η2p = 0.108). However, significant main effects were observed for group (p = 0.033, η2p = 0.208) and time (p = 0.011, η2p = 0.202). Multiple comparisons indicated that pulse rate was significantly higher at 0 min compared to 40 min (p = 0.003). Two-way ANOVA for systolic blood pressure revealed a significant interaction between groups and time (p = 0.030, η2p = 0.160). Additionally, significant main effects were found for group (p < 0.001, η2p = 0.483) and time (p < 0.024, η2p = 0.170). Multiple comparisons showed no significant changes over time in the Throwers group (p = 0.069); however, a significant decrease over time was observed in the Controls group (p = 0.011). Systolic blood pressure in the Controls group was significantly lower at 40 min compared to BL (p = 0.007). Furthermore, systolic blood pressure was significantly lower in the Controls group than in the Throwers group at BL (p = 0.013), at 0 min (p < 0.001), and at 40 min (p < 0.001). Two-way ANOVA for diastolic blood pressure revealed no significant interaction between groups and time (p = 0.123, η2p = 0.100) and no significant main effects of time (p = 0.824, η2p = 0.010) or group (p = 0.177, η2p = 0.089).
Changes in heart rate and blood pressure.
Changes in heart rate and blood pressure.
All data are presented in means ± SD.
BL; base line, 0 min; immediately after exercise, 40min: after 40 min rest. BP; blood pressure.
*p < 0.05 vs. controls group. ***p < 0.001 vs. controls group. ##p < 0.01 vs. BL.
Figure 1 shows the baPWV results. Two-way ANOVA for baPWV revealed a significant interaction between groups and time (p = 0.023, η2p = 0.172); however, the main effects of time (p = 0.319, η2p = 0.056) and group (p = 0.237, η2p = 0.069) were not significant. Multiple comparisons showed no significant difference over time in the Throwers group (p = 0.491); however, there was a significant difference in the time of the Controls group (p = 0.016). BaPWV was significantly lower at 0 min compared to BL (p = 0.003).
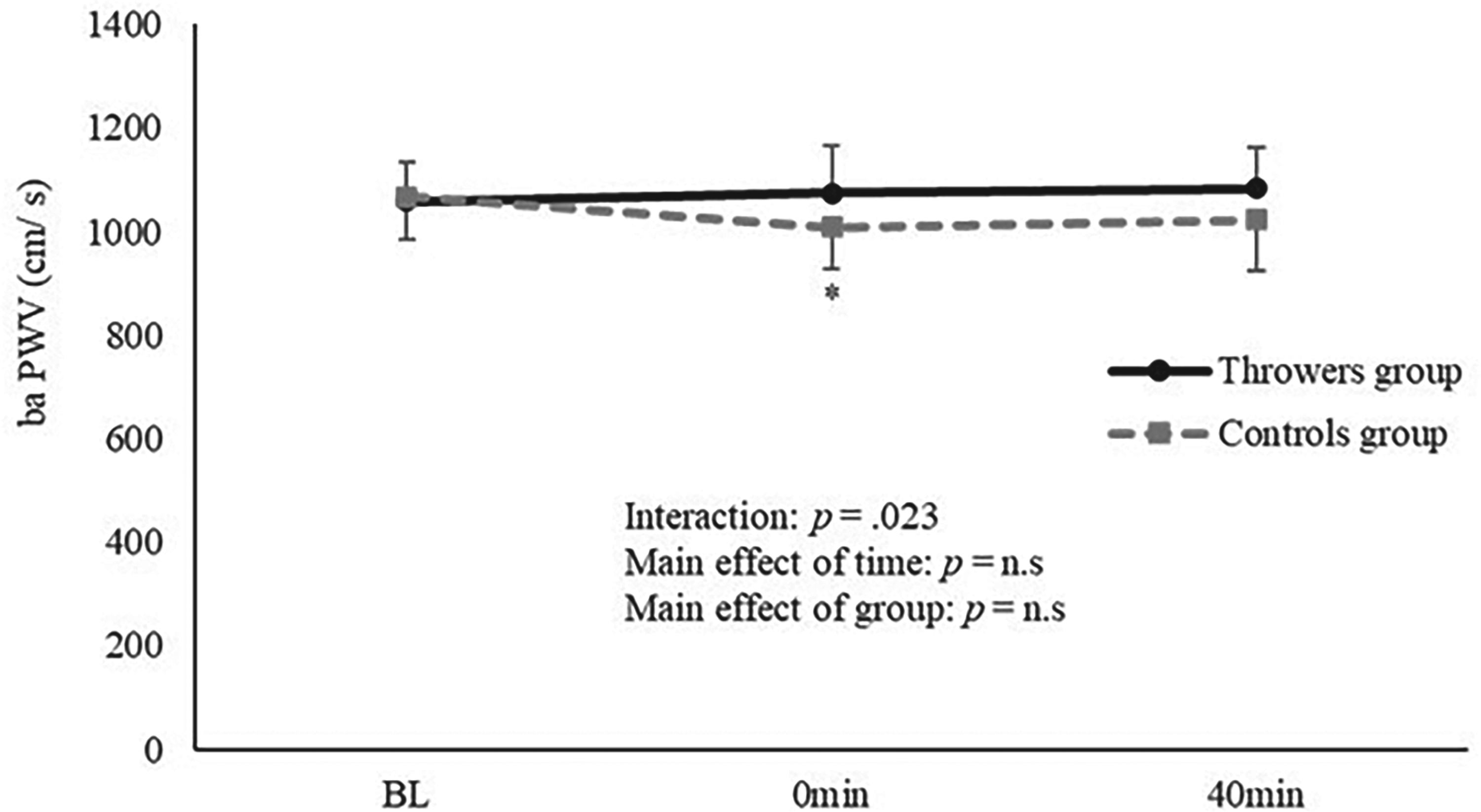
Changes in the baPWV before and after exercise. BaPWV brachial-ankle pulse wave velocity, BL base line, 0 min immediately after exercise, 40 min after 40 min rest, *p < 0.05 vs. BL (Controls group).
Figure 2 shows the RHI results. The two-way ANOVA revealed no significant interaction between time and group and no main group effect (p = 0.282, η2p = 0.061and p = 0.079, η2p = 0.146, respectively). However, a main effect of time was observed (p < 0.001, η2p = 0.302), and multiple comparison testing revealed a significant increase in RHI at 0 min and 40 min compared to BL (p = 0.045 and p = 0.006, respectively).
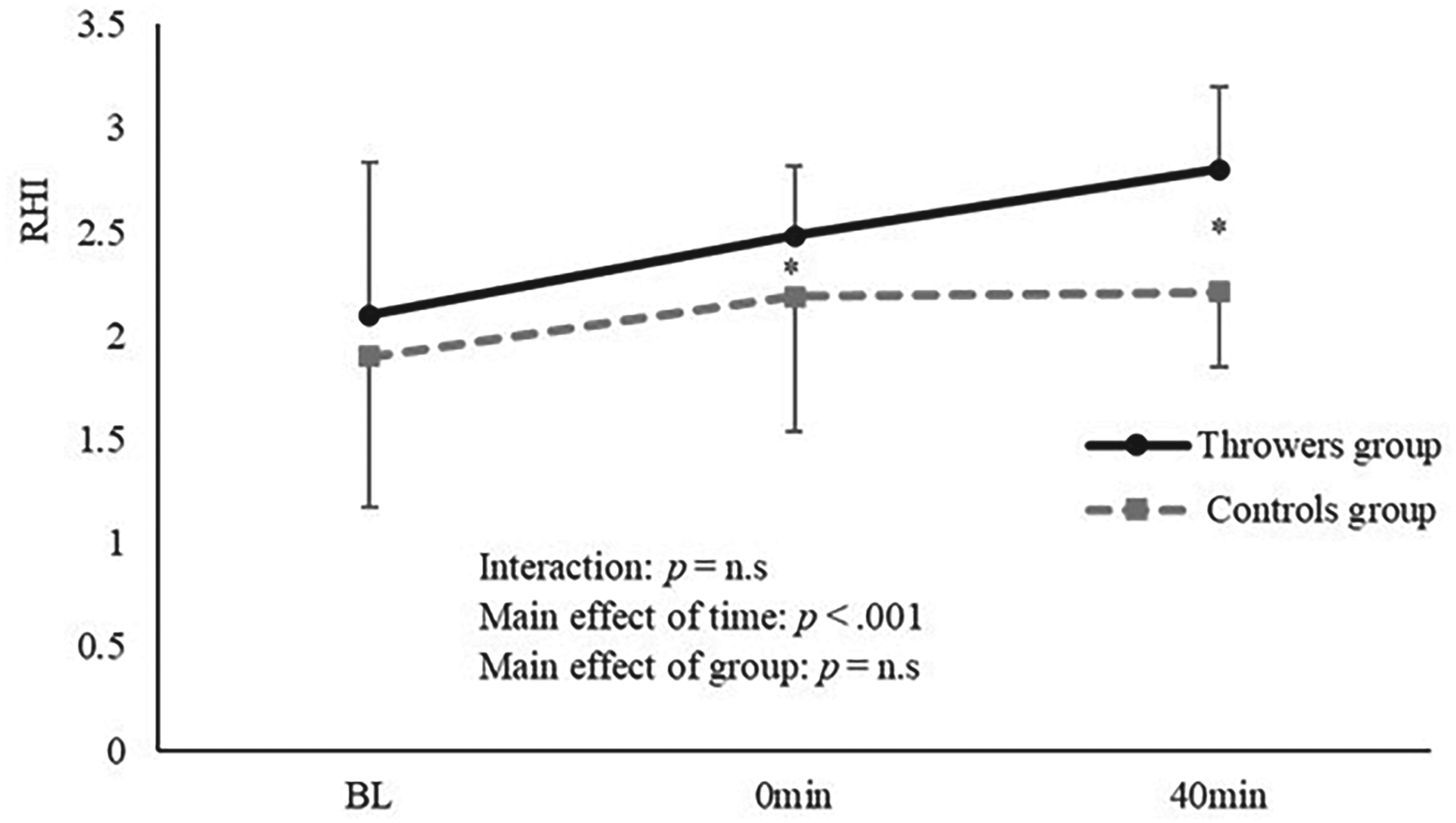
Changes in the RHI before and after exercise. RHI reactive hyperemia-peripheral arterial tonometry index, BL base line, 0 min immediately after exercise, 40 min after 40 min rest. *p < 0.05 vs. BL.
The primary objective of this study was to determine whether a single bout of moderate-intensity aerobic exercise could acutely alter arterial stiffness and endothelial function in strength-trained throwing athletes compared with untrained controls. Our results indicate that whereas throwers did not experience significant reductions in baPWV, both throwers and controls demonstrated significant increases in RHI post-exercise, suggesting a preserved endothelial responsiveness despite long-term resistance training.
A previous study has shown that strength-trained throwers exhibit higher arterial stiffness compared to untrained individuals. 19 However, no significant difference was observed in our study. Miyachi et al. (2003) reported 27 reduced arterial compliance in middle-aged but not young resistance-trained adults, suggesting that arterial stiffness may be less affected by strength training in young populations.
Strength-trained throwers exhibited no significant reduction in arterial stiffness following aerobic exercise, contrasting with findings in non-trained individuals where moderate-intensity aerobic exercise typically leads to improved arterial stiffness.11–13 Resistance exercises such as the leg press can elevate blood pressure significantly, with measurements reaching 480/390 mmHg during maximal effort, 28 whereas aerobic activities like jogging increase blood pressure to approximately 262/100 mmHg. 29 Given the habitual exposure of strength-trained throwers to high vascular loads, the 30-min moderate-intensity aerobic exercise used in this study may have been insufficient to reduce arterial stiffness. In contrast, Short-interval intermittent exercise may produce even larger and longer-lasting reductions in baPWV compared with continuous protocols. 12 Furthermore, high-intensity aerobic exercise may offer greater benefits.30–32 It has been reported that individuals with a habit of strength training have thicker vascular walls 27 and larger arterial diameters. 28 Therefore, differences in vascular structure may explain the varying arterial stiffness responses to aerobic exercise observed between throwers and non-trained individuals in this study. However, since this study did not employ imaging diagnostics or histological analyses, further investigation is needed to elucidate these mechanisms.
The RHI increased after aerobic exercise in both groups, consistent with previous research showing enhanced vascular endothelial function following exercise.9,29 The RHI primarily reflects nitric oxide (NO)-mediated endothelial function, which increases with exercise.33,34 The lack of group differences suggests that endothelial function may respond more acutely to aerobic exercise than arterial stiffness, even in strength-trained throwers.
This study has several limitations. The sample size limits the generalizability of the study's findings. The intervention was confined to a single 30-min session of moderate-intensity aerobic exercise, leaving the effects of long-term or high-intensity exercise unexplored. Additionally, only brachial-ankle pulse wave velocity (baPWV) and RHI were measured. Including other vascular markers and biochemical data could provide a more comprehensive analysis.
Conclusions
The findings indicate that while arterial stiffness did not improve in throwers after a single bout of moderate-intensity aerobic exercise, endothelial function showed significant improvement. This suggests that while aerobic exercise has short-term benefits for endothelial function, higher-intensity exercise may be necessary to reduce arterial stiffness in individuals who regularly engage in high-load training, such as throwers. These insights could help optimize aerobic exercise prescriptions and improve vascular health in individuals with specific training backgrounds.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to all the participants who contributed their time and effort to this study. Additionally, we acknowledge the Kansai University Research Ethics Review Committee for their ethical oversight and approval of this study (approval number: 2018-04).
Author contributions
Hiroya Koshiba and Etsuko Maeshima conceived and designed research. HK Hiroya Koshiba conducted experiments and analyzed data. HK Hiroya Koshiba wrote the manuscript with support from Etsuko Maeshima. All authors read and approved the manuscript.
Funding
This study was funded by the Grants-in-Aid for Young Scientists (18k17808) and the Ministry of Education, Culture, Sports, Science, and Technology.
Conflict of interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data availability
Data is provided within the supplementary information file. 10.6084/m9.figshare.28091849.