
Abstract
Abstract
Background
The rapid advancement of digital technologies has transformed healthcare delivery, yet significant gaps remain in patient-centred research on digital healthcare services (DHCS).
Objective
This study aims to map the global research landscape of patient-centred DHCS, identify key themes and collaboration patterns, and highlight gaps to guide future research.
Methods
Following a narrative review of DHCS evolution with China as a regional case study, a bibliometric analysis was conducted on 4163 publications retrieved from Scopus (2020–2025). VOSviewer and the Bibliometrix R package were used for visual mapping and trend analysis.
Results
Patient satisfaction with telemedicine has emerged as a key research focus, while on-site healthcare scenarios receive comparatively less attention. Additionally, the elderly population, as primary users of healthcare services, remains underrepresented in studies on the usability and experience of digital healthcare services. Research methodologies, including questionnaires, interviews, and randomised controlled trials, address diverse demographics and dimensions. International collaboration is dominated by the United States and European countries, reflecting their scientific influence.
Conclusion
Critical gaps identified include insufficient attention to on-site DHCS and elderly users, alongside disparities in global research influence. Future research should prioritise these areas and strengthen cross-continental collaboration to advance patient-centred digital healthcare delivery.
Keywords
Introduction
Reducing the burden on healthcare resources by providing services to a larger population at an affordable cost is one of the primary goals of healthcare services. 1 Globally, healthcare delivery methods have changed significantly due to the rapid development and extensive integration of digital technologies. 2 The efficiency and accessibility of healthcare services have been steadily improved through the widespread adoption of patient-facing digital tools, including wearable biosensors for chronic condition monitoring, teleconsultation platforms for remote physician consultations, mobile health applications for appointment and prescription management, and self-service kiosks for accessing test results and healthcare information.3–6 However, countries have different digital healthcare service models because of disparities in sociocultural origins, governmental orientations, and economic development levels. 7 When implementing Digital Healthcare Services (DHCS), it is impossible to overlook the patient as a key stakeholder in the industry. Healthcare, as a complex social and public service, involves multidisciplinary collaboration. Particularly in the dimension of patient-oriented interactions, research extends beyond medicine and public health into disciplines such as computer science, 8 engineering, 9 psychology, 10 design, 11 and ethics, 12 among many others. By gaining insights into DHCS through patient perspectives and feedback, we can provide essential knowledge and identify priority issues for future research, effectively improving user acceptance and experience of DHCS.
Despite the growing body of literature on DHCS, a systematic bibliometric analysis mapping the intellectual structure and thematic evolution of patient-centred DHCS has yet to be conducted. The motivation of this study is to address this gap through a bibliometric analysis of peer-reviewed literature published between 2020 and 2025. The scope is limited to patient-facing digital healthcare services that patients can access and operate independently—such as teleconsultation platforms, mobile health applications, and self-service kiosks—and excludes services where clinical professionals are the primary operators. The aim of this study is to map the global research landscape of patient-centred DHCS. To achieve this aim, the specific objectives are to identify high-impact publication venues, reveal thematic clusters and their temporal evolution, and ultimately identify research gaps to guide future investigation in this field.
Evolution and regional contexts of DHCS with patient perspective
Global trajectories and core components
As the Internet became more widespread in the late twentieth century, medical institutions recognised that digital technologies could enhance the patient experience while alleviating healthcare resource constraints. 13 Digital healthcare saw its initial stage of development with the arrival of the micro-computer, and the United States was the first to attempt to integrate the two into healthcare by constructing Electronic Medical Records (EMRs) to replace traditional paper-based printed and handwritten records. 14 During this time, the goal of digitisation was to improve information management in healthcare institutions, patient involvement was rarely used.
With the widespread use of the Internet in homes worldwide around the year 2000, digital healthcare began to expand beyond internal self-management, and the concept of telemedicine gained popularity along with it. This concept brought user engagement. Examples include video consultations based on online communication technologies 15 and delivering vital health information to people through websites. 16 Electronic Health Records (EHRs) are beginning to be widely used in clinical practice in developed countries, 17 to help healthcare departments assess population health. 18 Additionally, self-service kiosks, a prototype of digital healthcare service devices, are used as a link between external users and the internal systems of digital healthcare. 19 They offer users a basic reservation service to reduce waiting times and boost the effectiveness of triage data management in healthcare institutions.
Given smartphones’ broad use in the mHealth industry, digital healthcare reached a new level after 2010. 20 People can more easily manage their self-health data in the cloud with the help of wearable biosensing devices 21 and mobile health apps.18,22 This dramatically lowers the time and space costs associated with the on-site healthcare model. In particular, it plays an active role in controlling chronic diseases.23,24 Nevertheless, these also required patients to be more tech-savvy to participate. At this point, big data is being used to assist the development of concepts for personalised medicine and optimise service efficiency in the public healthcare system, in addition to the service dimension as experienced by the patient. 22 Furthermore, the capabilities offered by digital healthcare self-service kiosks in healthcare facilities are further enhanced, including access to test results, imaging data, medications, and more. Individual devices exchange data with one another to further maximise the effectiveness of the service. 25
The global pandemic COVID-19 after 2020 has accelerated the development of contactless healthcare26,27 on the one hand and the use of telecommunication technologies to reduce access to healthcare sites on the other. 28 On the other hand, healthcare institutions have further increased their investment in self-service kiosks to minimise physical contact between personnel. 29 The concept of “Wise Information Technology of 120 (WIT120)” was born with a greater emphasis on multidisciplinary collaboration in China, further integration of the Internet of Things, mobile payments, the Internet and big data, 30 and exploring the introduction of AI technology to assist with the quality of care. 31 For instance, China is rapidly growing the scope and services provided by its online hospitals, employing multimodal medical models to provide diagnosis guidance and spread medical expertise.32,33 By way of review, patient-centred DHCS can be categorised into two types: on-site and off-site models. Figure 1 illustrates the content of DHCS oriented towards patient interaction.
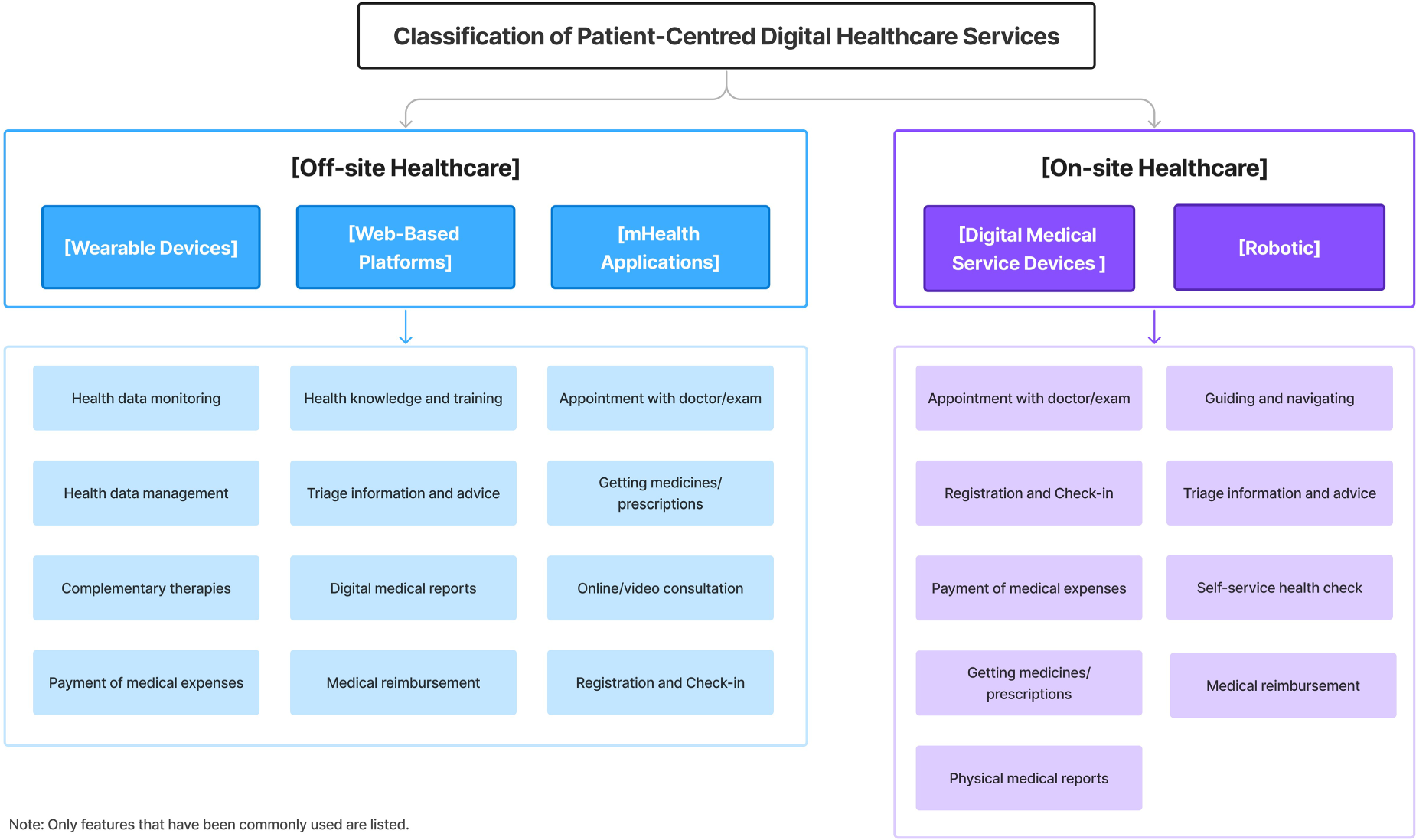
Content of patient-engaged digital health services.
According to the previous review, global DHCS are convergent regarding technology architecture and development trajectories. China is actively encouraging the use of digital technologies in healthcare scenarios; as the most populous country in the world, it faces the issues of an ageing population and unequal distribution of healthcare resources.34,35 This makes China a suitable window through which to observe the practice of digital healthcare delivery. Examining the practice in China will assist us in finding details that might have been overlooked, and when combined with the previously organised process of creating DHCS, it will offer direction for making the subsequent thorough review plan. Similar to the hierarchical diagnosis and treatment model adopted by most countries, China's DHCS refer to the hierarchical medical system (HMS) based on the number of beds as the core indicator, which divides healthcare institutions into three levels, including primary healthcare, secondary healthcare, and tertiary healthcare institutions in descending order. 36 The gradient distribution of digital healthcare service capability is reflected in this grading system in addition to the distinct features of resource allocation.
Tertiary Healthcare Institutions (THIs) are mainly located in densely populated urban areas, and their services radiate throughout the province and the country. These institutions have significant advantages in terms of digital healthcare service capacity: firstly, they have the complete departmental setup, which can provide a full range of diagnosis and treatment services; 37 secondly, they have the most advanced configuration of digital healthcare service devices, which include not only terminal devices for patients, but also include precise imaging devices, intelligent diagnostic systems, and a more comprehensive health information platform for the whole population; 33 thirdly, they have the complete telemedicine system, which can carry out cross-region video consultation, remote surgery guidance and other services. As of November 2023, more than 80 per cent of tertiary hospitals in 20 provinces had access to provincial-level universal health information platforms. 38
Most Secondary Healthcare Institutions (SHIs) are found in city sub-centres or county-level administrative districts. These institutions often have essential digital healthcare devices and can provide digital diagnosis and treatment services for common diseases. Their telemedicine systems mainly interconnect regional healthcare institutions and support two-way referrals and teleconsultations between upper and lower-level hospitals. 39 The regional universal health information platform has more than 8000 public hospitals above the second level connected as of November 2023. 38 SHIs across the country are required to universally carry out services such as Internet health consultation, booking of appointments, and testing of examination results in 2022. 40
Primary healthcare services in the community are primarily the responsibility of Primary Healthcare Institutions (PHIs), which are at the base of the healthcare delivery system. The development of digital service interfaces for patient engagement has not yet been achieved in rural and less economically developed areas. Better-off urban communities have simple digital services such as electronic health record management and basic self-service kiosks. 41 The Chinese government to promote national health during the 14th Five-Year Plan in 2022, proposed to enhance the digital service level of primary healthcare institutions by equipping them with intelligent terminals and wearable devices. 40
In promoting hierarchical medical care, China is now assisting citizens in choosing the best medical facility for their unique situation, primarily by differentiating medical insurance and allocating medical resources across geographical boundaries.36,42 The system has dramatically increased the convenience of healthcare services by granting patients the freedom to select their healthcare institutions. 41 However, it has also brought attention to the problem of excessive concentration of high-quality healthcare resources in large healthcare institutions, which impacts the primary healthcare institutions’ utilisation rate. 43 This is more evident in rural areas that are relatively economically backward. 36 As an innovative path to break the above dilemma, the role of digital healthcare in balancing healthcare resources has been proven in the practice of many countries.2,43,44 China is currently focusing on promoting the in-depth integration of innovative technologies and internet-based healthcare to facilitate the distribution of high-quality medical resources and establish a quality assurance system for hierarchical diagnosis and treatment. 40
As research in this field has grown rapidly, a quantitative approach is needed to map its intellectual structure and identify emerging trends. Recent studies have tended to focus on specific technological applications within digital health, such as machine learning models for disease detection, 45 AI-driven clinical monitoring systems, 46 and deep learning approaches in medical diagnostics, 47 rather than examining patient-facing DHCS as an integrated research domain. Bibliometric analysis offers a systematic means of addressing this gap, enabling macro-level mapping of knowledge structures and thematic evolution. While this approach has been applied to specific domains such as telemedicine 48 and mHealth, 49 a comprehensive bibliometric analysis of patient-centred DHCS remains absent, motivating the present study.
Insights into global DHCS with patient perspectives
Methods and tool
Given the complexity of healthcare systems, we decided to use bibliometrics to evaluate the content of international academic research on patient-centred DHCS methodically. This method enables the evaluation of the content from a macroscopic perspective and allows the quick exploration of interconnecting features from a large body of literature. Then, the open-source software VOSviewer (version 1.6.20) was used to transform the data into visual knowledge mapping to analyse the elemental information. 50 Moreover, the process also utilised the Bibliometrix R package (version 5.1.1), accessed via the biblioshiny interface in R 4.5.1, as supplementary analytical software to complement the findings from VOSviewer and provide additional analytical perspectives. 51 The process includes study design, data collection, cleaning, analysis, visualisation and discussion. The method focuses on three research directions: academic citation status, international cooperation network, and hot topic distribution.
Study design and data collection
The selection of the database was informed by a comparative assessment of the major bibliometric databases commonly used in health-related research. Web of Science (WoS), while widely adopted in bibliometric research, applies comparatively stringent journal inclusion criteria, which may result in the underrepresentation of newly established or emerging journals. 52 PubMed, as a database designed primarily for biomedical and life sciences literature, 53 predominantly indexes clinician-oriented content, which does not align with the patient-facing focus of this study. Google Scholar, despite its breadth, does not provide the structured metadata and exportable bibliometric indicators required for systematic quantitative analysis. 54 Therefore, Scopus was selected as the data source for this study. As a broad-coverage, peer-reviewed abstract and citation database, its interdisciplinary scope is more likely to capture the emerging and interdisciplinary nature of patient-centred digital healthcare research, thereby minimising the risk of relevant literature being overlooked. 55 However, reliance on a single database may nonetheless exclude studies indexed solely in other repositories, a limitation further discussed in Section 4.6.
Initial candidate keywords were drawn from three sources: existing bibliometric literature on digital health, the patient-centred research framework established in Section 2, and professional healthcare terminology. Given the study's focus on patient-centred DHCS, “patient interaction”, “patient engagement”, and “patient satisfaction” were identified as the foundational filter group, with all other candidate keywords evaluated on the basis of their co-occurrence with at least one of these concepts. All candidate keywords were subsequently tested through iterative searches in Scopus; terms that broadened the corpus at the expense of relevance were excluded, as keyword selection in bibliometric research inherently requires balancing comprehensiveness against thematic precision. 56 For instance, “electronic health records (EHRs)” and “connected health” returned predominantly clinician-facing or infrastructure-oriented literature, while “patient experience” retrieved a substantially broader range of studies on general clinical service quality unrelated to patient-facing digital interactions. The final keyword set comprised two groups linked by a Boolean AND operator: a digital healthcare modality group (“digital health”, “e-health”, “telemedicine”, “telehealth”, “m-health”, “health information technology”, “wearable medical devices”, “smart health”) and a patient-engagement filter (“patient interaction”, “patient engagement”, “patient satisfaction”), ensuring that retrieved documents addressed both the service modality and patient-facing dimensions simultaneously. The complete search formula is shown in Figure 2.
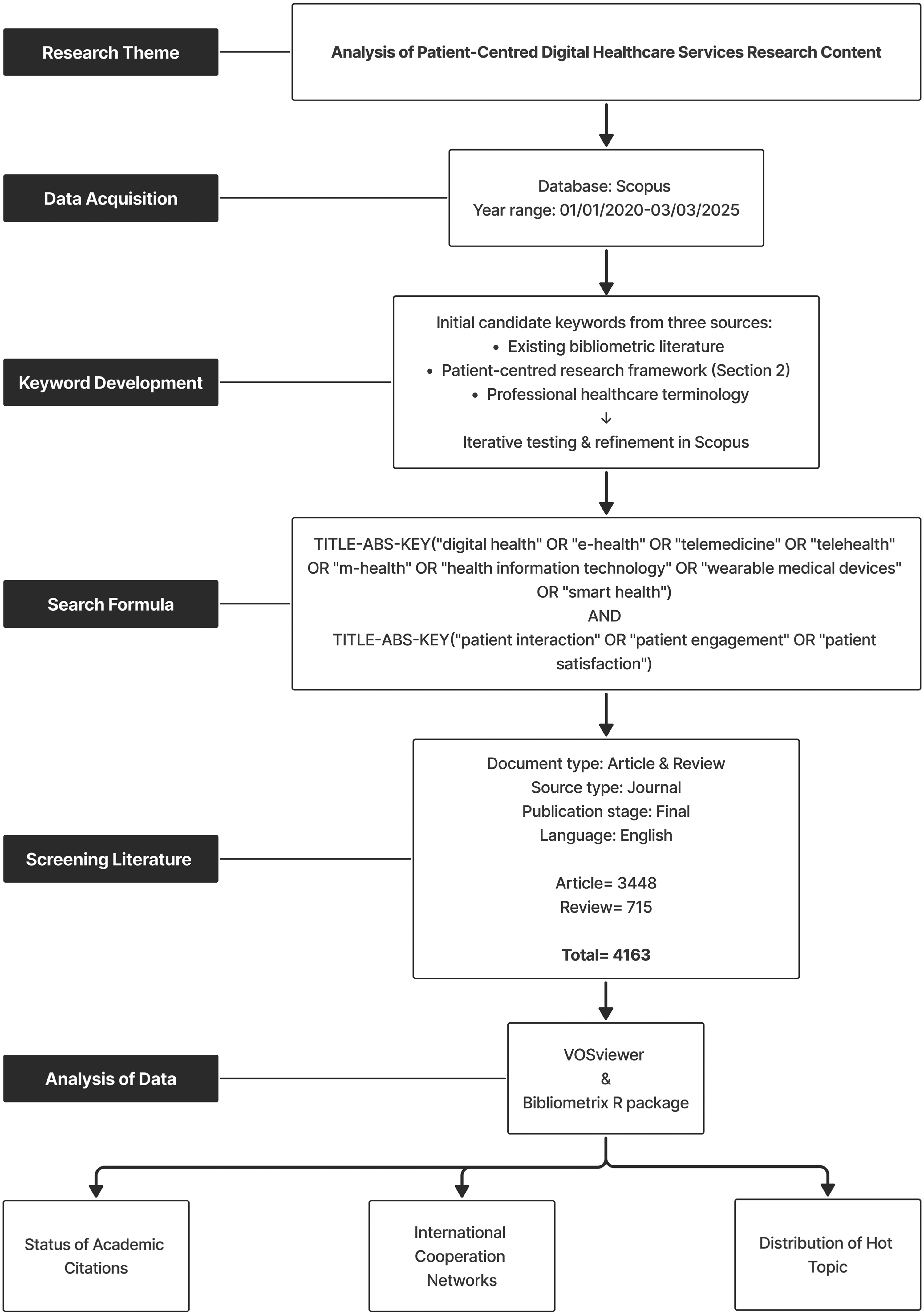
Literature screening and analysis flowchart.
The search scope was set to “TITLE-ABS-KEY”; the document language was set to “English” only; the document stage was set to “Final” to avoid retrieving incomplete documents; the document type was set to “Article” and “Review”; the source type was set to “Journal”. Since the COVID-19 pandemic in 2020 significantly accelerated the development of digital healthcare, the search period was selected from 1 January 2020 to 3 March 2025, to better understand the most recent advancements in the field. After data cleaning (removing duplicates, missing key metadata, and documents that were clearly irrelevant to the topic), a total of 4163 papers were obtained. In addition, during subsequent analyses, we merged conceptually congruent content (such as “COVID-19 pandemic” into “COVID-19”), removed words with too broad a meaning in the context of this study (such as “article”).
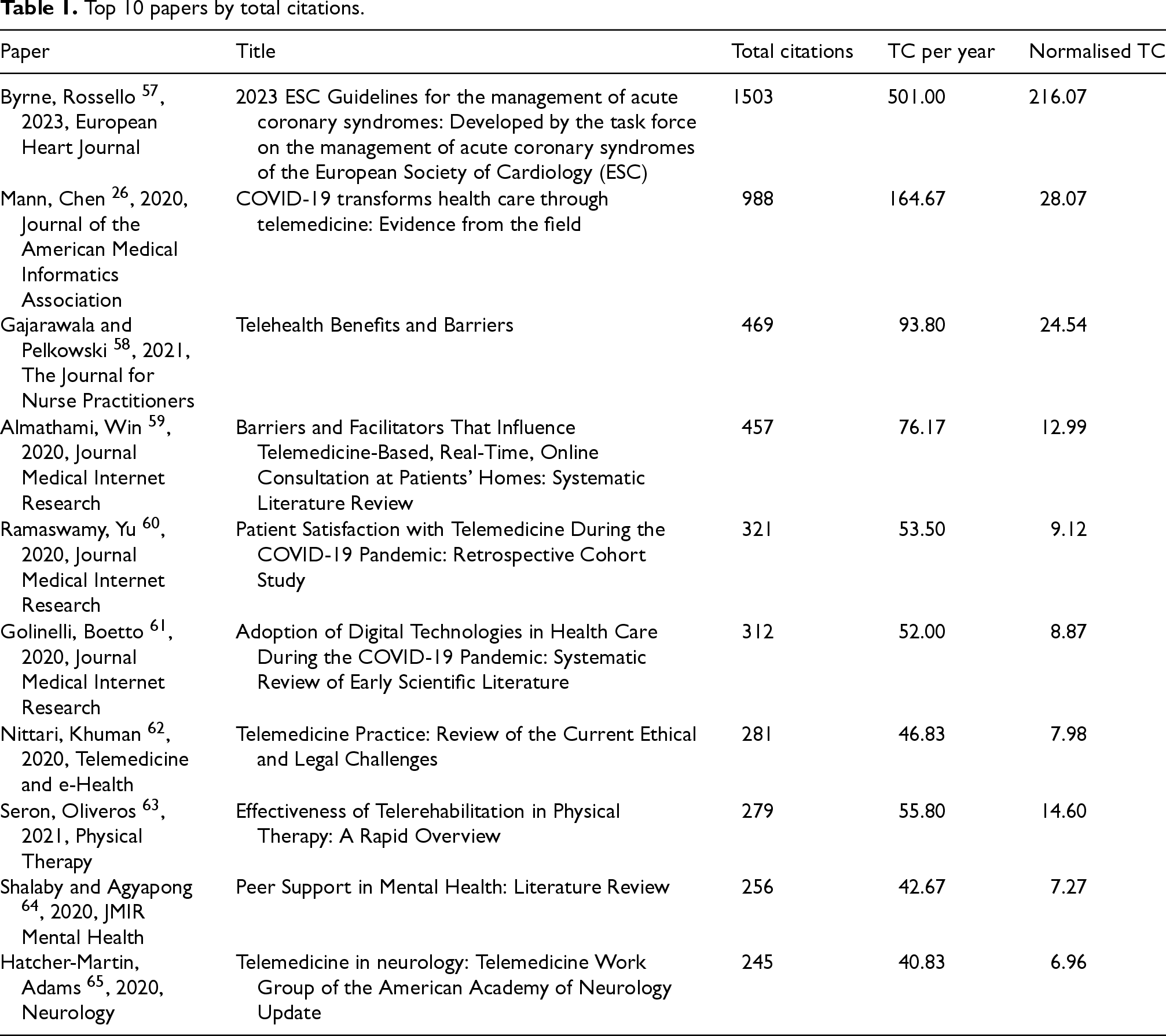
Hot papers can reflect the focus of research to a certain extent. We selected the papers (top 10) based on the citation frequency to reveal the aggregation pattern of research hotspots (Table 1). The sample papers primarily focus on four areas of research (note that some papers fall into multiple categories): quality of clinical care (n = 3), mechanisms for optimising DHCS in the context of the COVID-19 pandemic (n = 3), ethical risks in the context of telemedicine (n = 1), and efficacy assessment in the context of telemedicine delivery systems (n = 5). In 2023, the European Society of Cardiology issued the most cited paper (n = 1503), essentially a methodological framework for clinical practice guidelines.
Top 10 papers by total citations.
Top 10 papers by total citations.
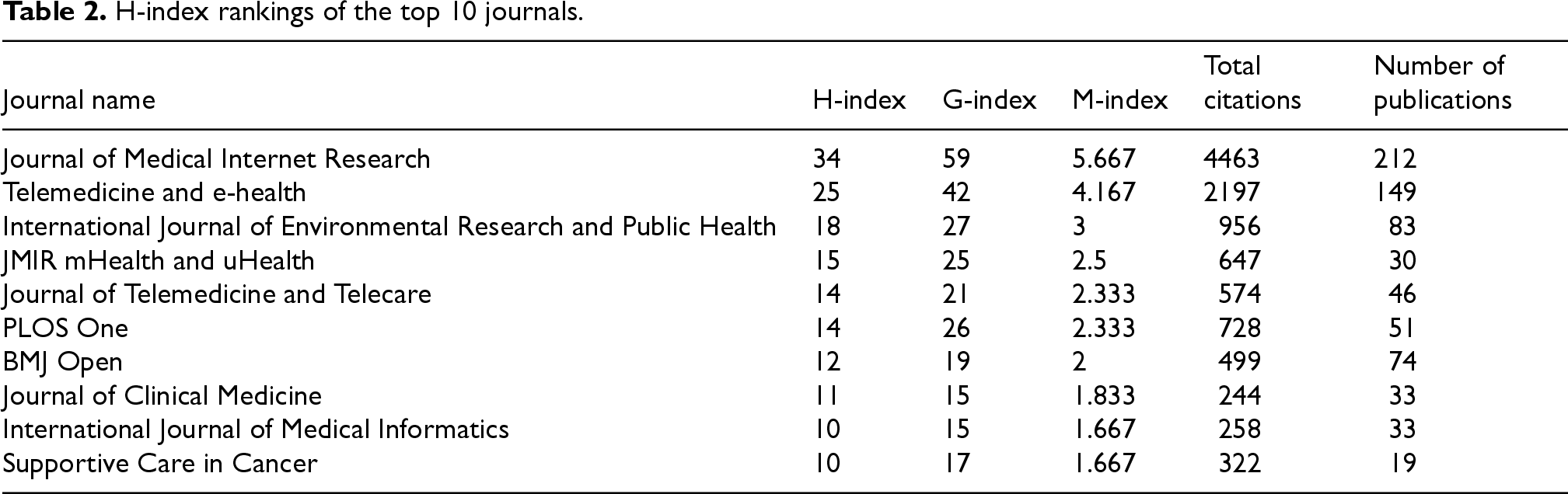
The journal effect should be evaluated using multiple indicators rather than a single statistic. 66 To evaluate the academic influence of the journals, three complementary bibliometric indicators were calculated using the Bibliometrix R package: the h-index, g-index, and m-index. For a given journal, the h-index is defined as the largest number h such that h of its published papers have each received at least h citations, providing a measure that balances publication volume with citation impact. 67 The g-index identifies the largest number g such that the top g papers of a journal have collectively accumulated at least g2 citations, giving greater weight to exceptionally highly cited papers that the h-index may undervalue. 68 The m-index normalises the h-index by dividing it by the journal's number of active years in the dataset (m = h/n, where n is the number of active years in the dataset), enabling comparisons of influence growth rate across journals regardless of their indexing history. 67 Table 2 presents the top 10 journals ranked by h-index. In terms of the number of published papers (n = 212), total citations (n = 4463), and average citations per paper (n = 21.05), the Journal of Medical Internet Research stands out as the most prominent journal in the sample. Furthermore, its h-index (h = 34), g-index (g = 59), and m-index (m = 5.667) values demonstrate its absolute leadership in both the sustainability and growth rate of its core influence. An analysis of the top 10 journals reveals a publication landscape concentrated in three distinct clusters. The list is dominated by journals specialising in digital health, with half of the top venues (5/10) dedicated to this field. This core group includes the Journal of Medical Internet Research, Telemedicine and e-health, JMIR mHealth and uHealth, Journal of Telemedicine and Telecare, and the International Journal of Medical Informatics, indicating a robust, specialised publication ecosystem for this research area. A second significant cluster (4/10) comprises major general medical and multidisciplinary journals, such as PLOS One, BMJ Open, Journal of Clinical Medicine, and the International Journal of Environmental Research and Public Health. The inclusion of these “mega-journals” suggests that the research topic also holds broad relevance and attracts interest from a wider scientific community. Finally, the presence of a highly specialised journal, Supportive Care in Cancer (1/10), underscores the significant application and impact of this research within a specific clinical domain, namely oncology.
H-index rankings of the top 10 journals.
Cooperation networks between countries can reveal patterns of academic collaboration and knowledge flow pathways between countries. Papers in the sample data came from 217 countries and regions, of which we assessed 63 (limiting the number of publications to ≥5). Country attribution followed the full-counting method, whereby any country affiliated with at least one author of a given paper was credited with one publication; thus, a multi-authored international paper contributes to the count of each participating country simultaneously. Citation counts reflect research impact, though they tend to correlate with publication volume and should therefore be interpreted alongside average citation strength. While the number of documents visually represents a country with a high research output, this does not necessarily mean the research is of high quality. To thoroughly evaluate the research influence of each nation and region, we use the country's publication amount as the primary ranking reference. Four indicators are used: the number of papers, total citations, average citation strength, and total link strength. Total link strength indicates the degree of network and activity, as well as the strength of international cooperation. Figure 3 and Table 3 present the collaboration network and associated bibliometric indicators respectively, with node size reflecting each country's publication volume, line thickness indicating collaboration strength, and node colour denoting cluster membership.
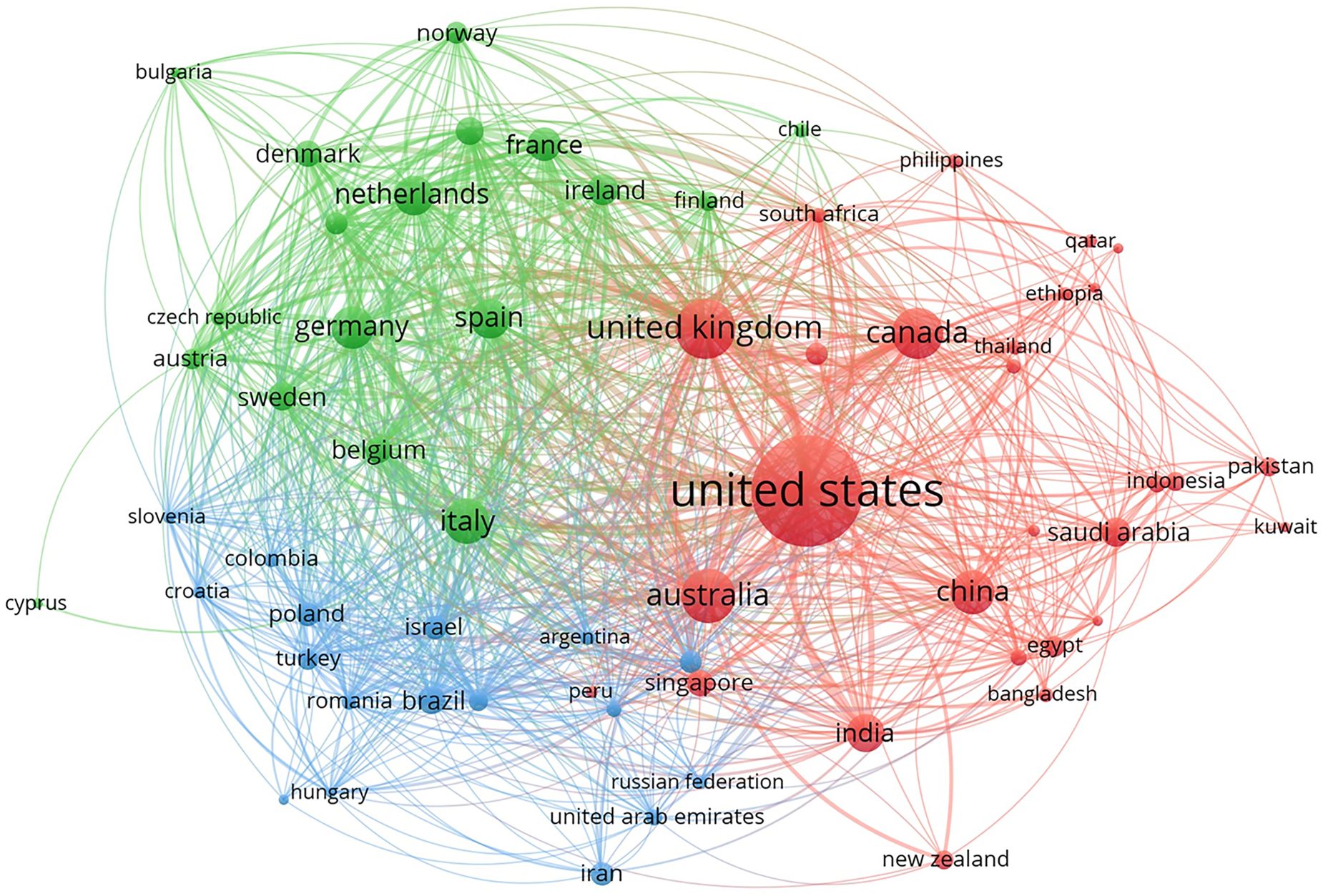
Mapping of country cooperation networks.
International research impact based on publications and citations (top 10).
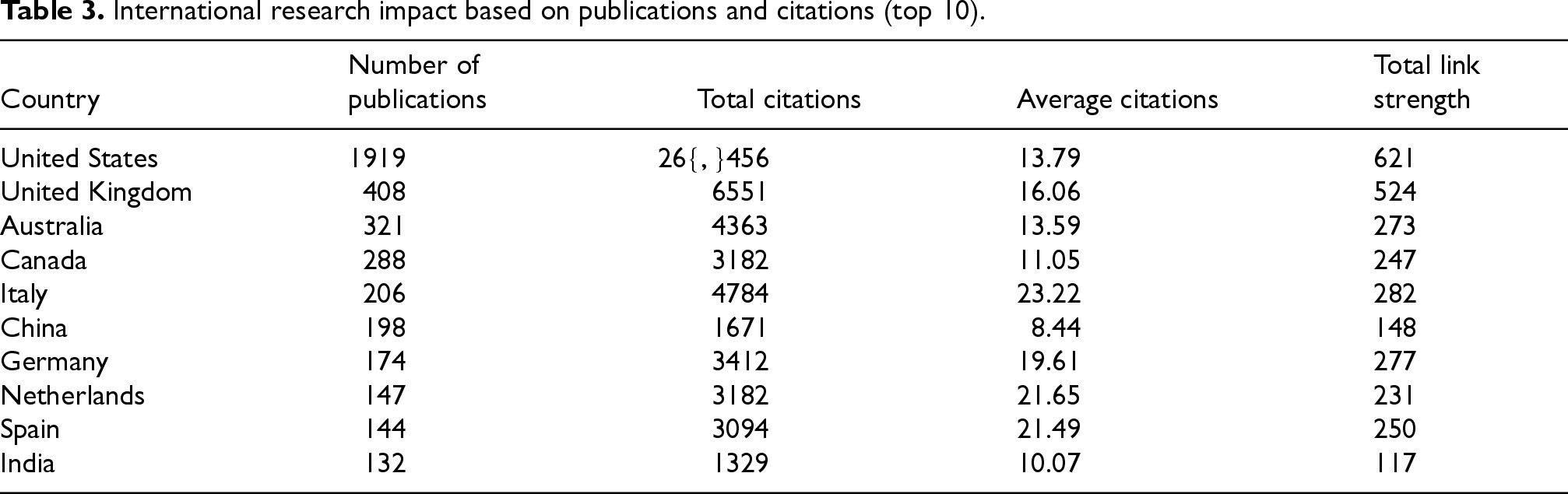
The United States was first in the number of publications (n = 1919), citations (n = 26,456), and active international collaborations (n = 621). Its major partner countries include Canada (link strength = 72), the United Kingdom (link strength = 63), China (link strength = 31), Australia (link strength = 29), and India (link strength = 24). The volume varies by nation, so we use the average number of citations to gauge the influence of papers to balance the countries with fewer publications and assess each country's contribution to this subject fairly. Table 3 shows the top 10 countries based on the number of papers issued. In contrast, Italy had the highest average number of citations (n = 23.22), meaning that, compared to the proportional number of documents (n = 206), the research outcomes obtained more citations (n = 4784). There is a significant disparity between China's ranking of 6th in terms of publications (n = 198) and 10th in terms of average citations (n = 8.44). The Netherlands and Spain experienced the most significant shifts in the gap, ranking only eighth and ninth, respectively, despite having relatively few publications (n = 147; n = 144); they were ranked second and third in average citations (n = 21.65; n = 21.49), a six-place difference in their number of papers rankings.
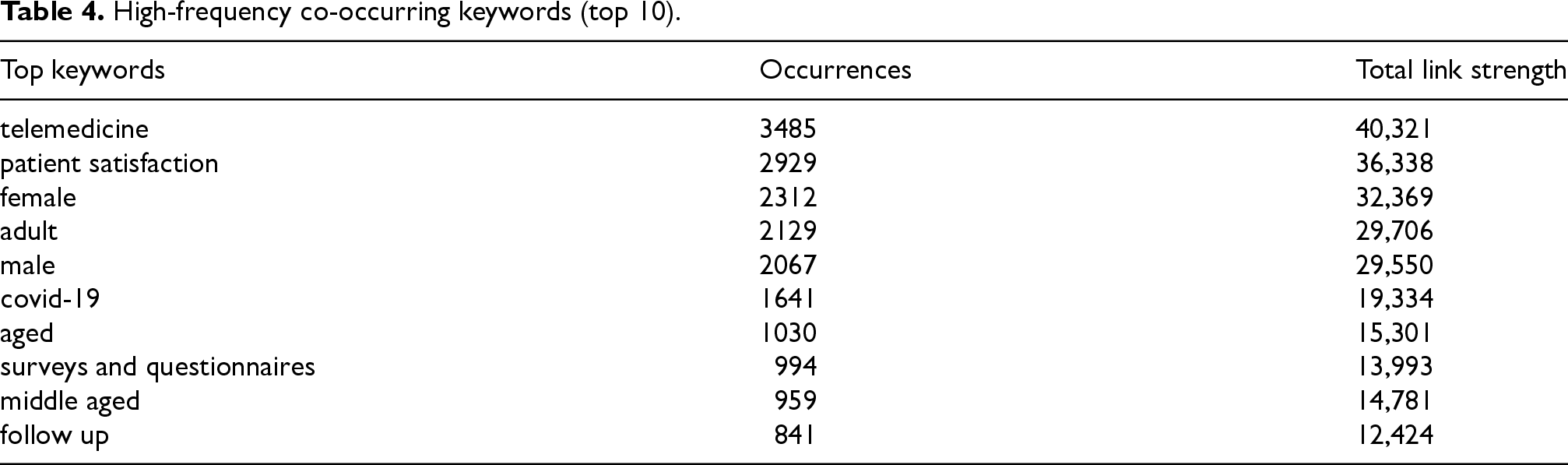
Keywords provide the most intuitive representation of what the research area is concerned with. We set keyword co-occurrence in VOSviewer and performed data cleaning (the specific way has been mentioned in Section 3.2). Due to the many keywords retrieved, we set the keyword occurrence frequency (≥100) to balance the display effect and screened 159 keywords. Table 4 lists the most common keywords (Top 10), where the total link strength indicates the connection strength between keywords.
High-frequency co-occurring keywords (top 10).
High-frequency co-occurring keywords (top 10).
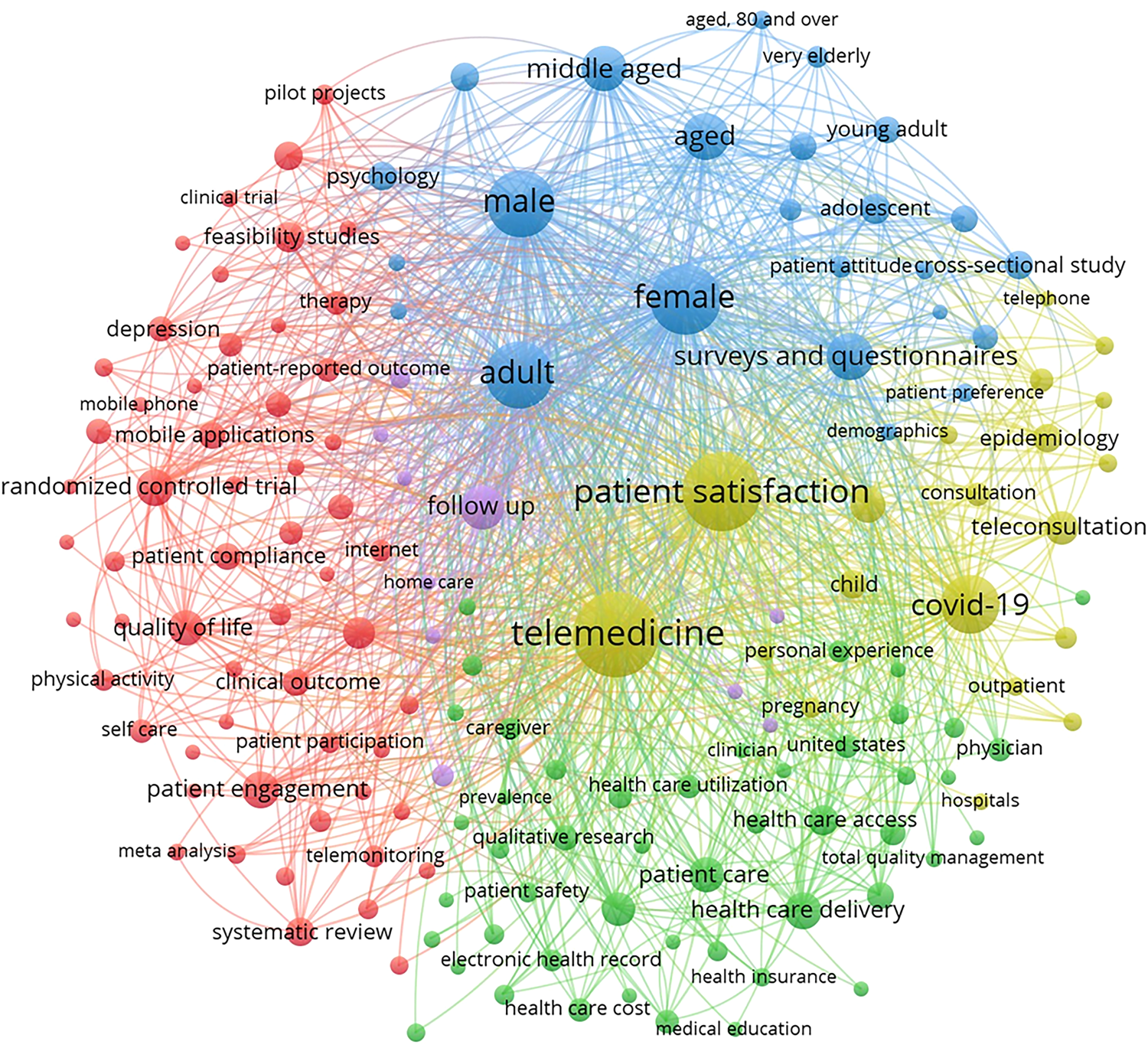
Network visualisation based on keyword co-occurrence.
Following the same visual conventions as Figure 3, this keyword co-occurrence network maps thematic relationships between research topics, where nodes positioned in closer proximity indicate stronger co-occurrence relationships between the corresponding keywords. The network mapping classified the keywords into five main clusters (Figure 4). Cluster 1 (shown in red) contains 57 keywords centred around investigating the promotion of active patient engagement in digital healthcare. The keywords are mainly “randomised controlled trial” (n = 600, where n denotes keyword occurrence frequency throughout this paragraph), “patient engagement” (n = 602), “outcome assessment” (n = 475), “feasibility studies” (n = 405), “systematic review” (n = 361), “pilot study” (n = 347), and “mobile application” (n = 321). However, this cluster's frequency of keyword occurrences and link strength were relatively even, with no significant differences. 48 keywords about the delivery and quality of healthcare services from an institutional perspective are included in Cluster 2 (highlighted in green). The keywords are mainly “health care delivery” (n = 610), “patient care” (n = 557), “health care personnel” (n = 534), “health care access” (n = 422), “health care quality” (n = 313), “health service” (n = 272), “health care cost” (n = 262), “electronic health record” (n = 229), and “semi-structural interview” (n = 195). Cluster 3 (shown in blue) mainly contains differences in research methodology and the population studied in terms of gender and age ranges and covers 24 keywords, of which the main ones are “female” (n = 2312), “adult” (n = 2129), “male” (n = 2067), “aged” (n = 1030), “surveys and questionnaires” (n = 994), “middle aged” (n = 959), “young adult” (n = 330), “very elderly” (n = 202), “cross-sectional study” (n = 351), “adolescent” (n = 415) and “psychology” (n = 384). Cluster 4 (shown in yellow) contains 20 keywords mainly related to “telemedicine” (n = 3485) and “patient satisfaction” (n = 2929), with “COVID-19” (n = 1641) being frequently linked to other keywords, highlighting its impact on digital healthcare delivery. In addition, the main keywords were “video consultation” (n = 573), “teleconsultation” (n = 508), “epidemiology” (n = 369), “child” (n = 368), “patient referral” (n = 260), and “outpatient department” (n = 138). Cluster 5 (shown in purple) contains fewer keywords, a low frequency of occurrence, and a low link strength. It is mainly a way of assessing DHCS from a clinical perspective and contains “follow up” (n = 841), “hospitalisation” (n = 198), and “comparative study” (n = 185).
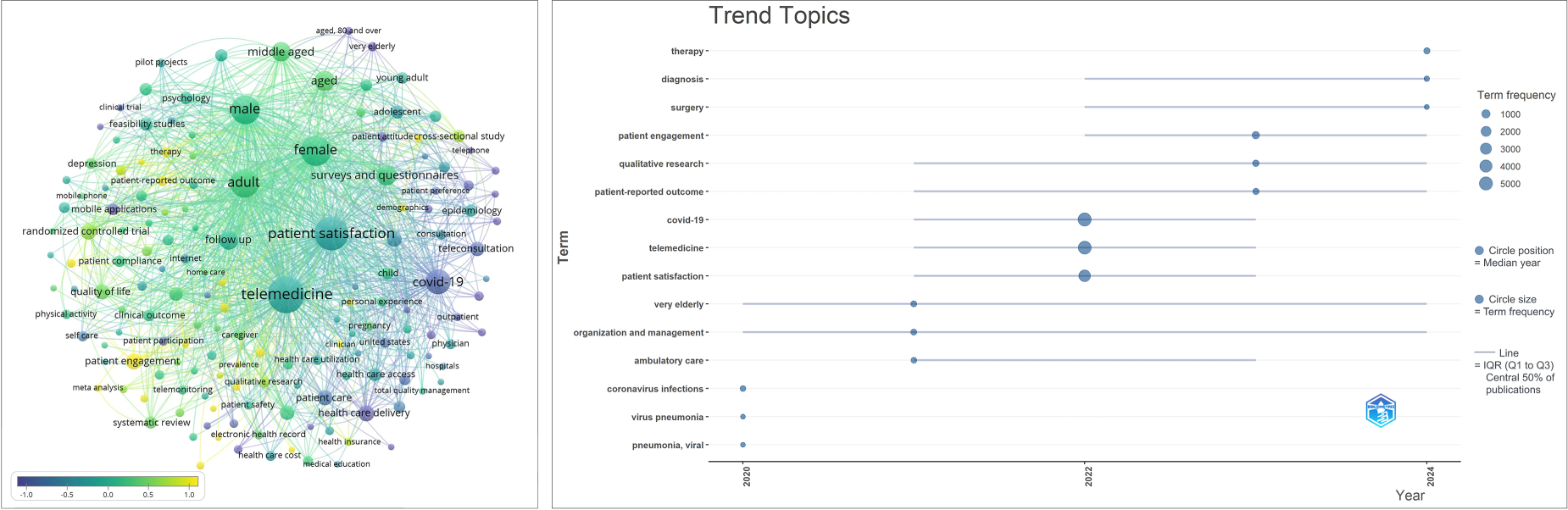
To gain insight into the temporal evolution of research hotspots, Figure 5 presents two complementary visualisations. The left panel shows a time-series overlay of the keyword co-occurrence network generated in VOSViewer, following the same visual conventions as Figure 4. Node colour encodes the normalised average publication year of each keyword, standardised using z-score normalisation (subtracting the mean and dividing by the standard deviation). Negative scores indicate keywords whose average publication year is earlier than the overall mean, representing foundational or declining topics, while positive scores reflect more recently active themes. The colour display range was set to (−1, 1) to ensure even visual distribution across the short retrieval timeframe (2020–2025); individual scores may nonetheless exceed this range, reflecting the actual dispersion of publication years within the dataset. In the right panel, generated using the Bibliometrix R package, each term is plotted along the horizontal time axis. The circle position represents the median publication year of the term, circle size reflects total term frequency, and the horizontal line spans the interquartile range (IQR) from the first quartile (Q1) to the third quartile (Q3), indicating the period within which the central 50% of publications on that term were concentrated. A shorter line, therefore, reflects a topic that emerged rapidly within a narrow timeframe, while a longer line indicates sustained discussion over a broader period.
Overlay visualisation mapping based on keyword co-occurrence.
As noted above, scores reflect z-score standardised values and may substantially exceed the display range of (−1, 1), particularly for terms with strongly skewed publication year distributions. The findings suggest that COVID-19 had a significant effect on the development of digital healthcare research from 2020, initially driving interest in pandemic-specific topics such as “coronavirus infections” (score = −5.67) and “virus pneumonia” (score = −5.86), which display narrow IQRs concentrated around 2020, reflecting their rapid emergence and subsequent decline as short-lived research responses. “Telemedicine” (score = −0.19) and “patient satisfaction” (score = −0.26) emerged as the two dominant and sustained research themes, reaching peak frequency around 2022 with wide IQRs spanning the full study period, confirming their role as core and enduring topics. Transitional themes such as “very elderly” and “ambulatory care” peaked around 2021 before gradually receding, reflecting the shifting research priorities as the acute pandemic phase subsided. In contrast, keywords such as “patient engagement” (score = 1.78), “patient-reported outcomes” (score = 1.40), and “qualitative research” (score = 0.66) recorded higher normalised scores with Q1 values commencing around 2022, indicating concentrated and rapidly growing research activity—a pattern consistent with the broader shift towards patient-centred care in the post-pandemic period. Keywords including “therapy” (score = 6.39), “diagnosis” (score = 2.40), and “surgery” (score = 1.84) show the highest normalised scores with IQRs extending towards 2024, suggesting these represent the most recently emerging frontiers yet to reach peak research attention.
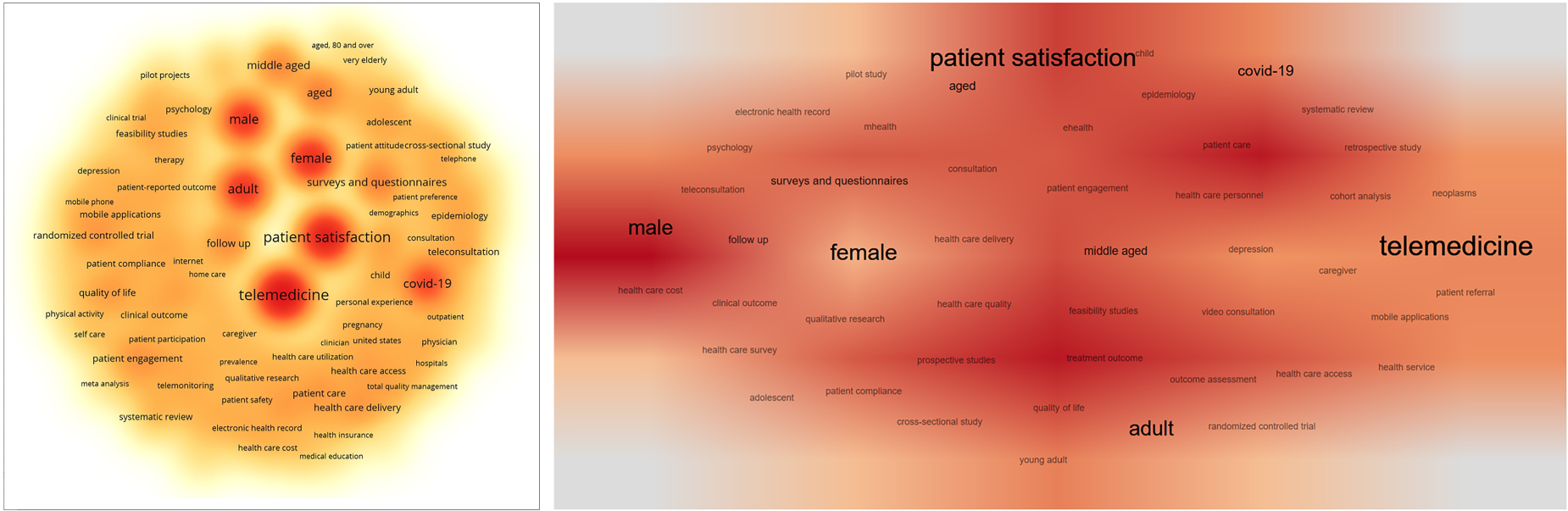
Figure 6 presents the density visualisation of research hotspots, in which colour intensity and font size reflect keyword frequency. The left panel (VOSViewer) provides a compact overview with discrete high-density clusters, sharply identifying the most heavily researched individual terms. The right panel (Bibliometrix R package) presents the same data with greater spatial dispersion, making the broader thematic landscape and transitional relationships between topics more visually accessible. Both panels consistently identify “telemedicine” and “patient satisfaction” as the dominant research themes in DHCS research.
Density visualisation mapping based on keyword co-occurrence.
Research priorities and gaps in service content
Insufficient attention to ageing groups
Keywords such as “female”, “male”, “child”, “adolescent”, “young adult”, “adult”, “middle-aged” and “aged” indicate that past studies have covered a wide range of age and gender groups. In contrast, however, insufficient research has been done on older adults, especially the very elderly (such as those over 80). However, older adults are the primary users of healthcare services in many countries, and their experience should be an essential consideration for DHCS. 69 According to earlier research, older adults’ reduced use of DHCS is caused mainly by their lack of digital skills and less acceptance of technology. 70 The emphasis on short-term attention following the COVID-19 pandemic correlates with the concentration of research on older adults, according to overlay visualisation mapping of keyword co-occurrence. This indicates that the public health crisis may have worsened health disparities in this group. The focus of existing research on ageing groups does not align with their significance in healthcare delivery, and this discrepancy warrants further investigation.
Diversity and empirical character of research methods
Features and drivers of international cooperation
Similarities in geographic location, language and cultural background drive academic partnerships between countries. 72 With partnerships with most nations (n = 60), including the United Kingdom, Canada, and Australia, the United States demonstrated the most substantial combined influence in the sample data. The core nations of European research cooperation are Italy, Germany, the Netherlands, Spain, and France. This is likely because they are members of the European Union, which provides them with greater access to intra-Union research opportunities, as well as a shared cultural background. Italy's research results were more widely cited, demonstrating greater international recognition in terms of citation impact. On the other hand, the Netherlands and Spain exhibit high citation efficiency, with their average number of citations significantly higher than the number of publications, indicating greater recognition of the quality and impact of their research within a relatively small body of work. In contrast, China and India are at the top of the list in terms of the number of publications. Still, their average citations are relatively lower, which indicates that their research results are not yet widely accepted as influential on an international scale or that there is still room for improvement in the quality of their research. It is crucial to remember that these findings are intended to serve as a guide, as the research data were sourced from English-language publications, which may skew the statistics for nations where English is not the primary language.
Patient engagement and service delivery approaches
Limitations
Several limitations to this study warrant consideration. Firstly, the analysis is based entirely on literature from the Scopus database. Although this database offers extensive coverage, it may not include the most recent journals that have yet to be indexed. Furthermore, the scope of the search was restricted to English-language literature, which inevitably introduces a language bias and excludes relevant research published in languages other than English. Secondly, concerning retrieval strategies, although this study subjected keywords and search formulas to repeated testing to maximise coverage of relevant literature, it may still have failed to capture all associated documents. For instance, differences in academic terms employed across various countries may result in specific publications failing to be retrieved. Thirdly, citation metrics are inherently time-dependent. Compared to earlier publications, those released shortly before the data retrieval deadline for this study have a shorter cumulative citation window, which may lead to an underestimation of their academic influence. Finally, this study did not account for self-citations, and the potential impact of authors’ and journals’ self-citations on overall citation metrics was not examined. Moreover, it must be acknowledged that even when analysing identical source datasets, different bibliometric software packages may yield divergent results. Such discrepancies typically stem from variations in their underlying computational algorithms and analytical emphases. 75 Nevertheless, despite minor variations in specific metrics, the overall trends and principal conclusions identified by these tools are generally consistent.
Conclusion
The study of DHCS is a multifaceted and intricate area. By examining the evolution of these services and integrating examples of regional practices in China, this study elucidates these services’ basic concept and reach. The current status of scholarly research on patient-centred DHCS is analysed from a macro viewpoint using bibliometric analysis, and the main findings are studied in depth.
This study found that telemedicine, as a central research theme, demonstrated a wide range of potential applications during the COVID-19 pandemic, but the optimisation of on-site healthcare scenarios and the integration of technologies still need to be further explored. The suitability and experience of these services for the ageing population as essential users of healthcare services have not yet received sufficient attention. The diversity of research methods reflects the coverage of different population characteristics and research dimensions. The uneven distribution of impact in international collaborations may be influenced by the limitation that only English-language publications were retrieved for this study. Overall, this study's findings reveal the gaps in research regarding patient-centred DHCS, and these findings provide essential reference content for future research in related disciplines. Future research should focus on optimising on-site DHCS, improving the applicability of digital healthcare to the elderly population, and strengthening international academic collaboration across continents. Meanwhile, research should pay more attention to patient engagement and the overall operational characteristics of the healthcare system to ensure the practicability of the research results and enhance patient satisfaction with the quality of healthcare services.
The findings carry practical implications for both healthcare providers and researchers. On the service delivery side, the sustained dominance of telemedicine and patient satisfaction in the literature points to continued demand for investment in teleconsultation infrastructure, while the relative neglect of on-site DHCS and elderly-focused services highlights areas where research attention and service development have yet to catch up. Looking ahead, the growing prominence of patient engagement, patient-reported outcomes, and qualitative methodologies signals a broader shift towards experiential and patient-centred approaches to DHCS evaluation. Future studies might productively examine the cross-cultural transferability of these services, the role of AI in enhancing personalised patient services, 76 the integration of privacy-preserving frameworks for sensitive patient data, 77 and the development of shared evaluation standards for patient-centred DHCS across varied healthcare contexts. The limitations of this study—including reliance on a single database, restriction to English-language publications, and the time-dependent nature of citation metrics—are discussed in full in Section 4.6 and should be borne in mind when interpreting these findings.
Footnotes
Acknowledgments
The author Lei Mao gratefully acknowledges the support of Xi’an Jiaotong-Liverpool University through the XJTLU Postgraduate Research Scholarship (PGRSB2306012).
Ethical considerations
There are no human participants in this article and informed consent is not required.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Lei Mao: Investigation, Software, Validation, Formal analysis, Data Curation, Writing - Original Draft, Visualization, Writing - Review & Editing. Ivan Parati: Conceptualization, Methodology, Supervision, Project administration. Cheng-Hung Lo: Conceptualization, Methodology, Supervision, Project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data of this study are available from the corresponding author upon reasonable request.