
Abstract
This paper discusses the UK’s National Programme for IT (NPfIT), which was an ambitious programme launched in 2002 with an initial budget of some £6.2 billion. It attempted to implement a top-down digitization of healthcare in England’s National Health Service (NHS). The core aim of the NPfIT was to bring the NHS’ use of information technology into the 21st century, through the introduction of an integrated electronic patient record systems, and reforming the way that the NHS uses information, and hence to improve services and the quality of patient care. The initiative was not trusted by doctors and appeared to have no impact on patient safety. The project was marred by resistance due to the inappropriateness of a centralized authority making top-down decisions on behalf of local organizations. The NPfIT was officially dismantled in September 2011. Deemed the world’s largest civil IT programme, its failure and ultimate demise sparked a lot of interest as to the reasons why. This paper summarises the underlying causes that lead to dismantling the NPfIT. At the forefront of those circumstances were the lack of adequate end user engagement, the absence of a phased change management approach, and underestimating the scale of the project.
Keywords
Large-scale healthcare IT projects
It is common for healthcare information technology (IT) projects to be implemented on a local level (within a single hospital or healthcare organization), and these implementations are usually filled with challenges. When healthcare IT projects are implemented on a larger scale, the associated challenges exasperate. Couple that with the workings of healthcare organisations and the complexities become insurmountable. Many IT healthcare projects in the public sector are done on a large scale, and usually span across a state, a region, or an entire country (when implemented on a national level). However, most of these large-scale projects are marred with failure despite massive expenditures. 1
Notwithstanding the costs involved, there is continued investment in IT projects without understanding the underlying causes of failures. Further to that, with every additional year spent on large-scale IT projects the cost overruns have been proven to increase by 15%. 2 Still, little is known about how to accomplish large-scale health care system change, 1 and the longer the project takes, the more likely it is to be overtaken by new technology. 3
Implementing large-scale IT systems in healthcare is not only about dealing with the technology, but is also about dealing with people. McCarthy et al. 4 estimate that only one third of healthcare IT projects achieve success, and they encourage the development of a change-enabled culture to ensure the success of IT healthcare projects. More arguments are being made that the behavioural and socio-cultural challenges of implementing healthcare IT projects are as overwhelming as the technical and logistical ones, if not more significant.5,6 There is no denying that healthcare systems significantly change the organisations in which they are introduced, and profoundly alter routine workflows within them. Subsequently, they have the potential to change the very cultures of those organisations. 6
Managing “IT” change in healthcare
Governments have realised that they cannot introduce change by edict, structural reform, or even by persuasion. Attempts to introduce change have backfired because they have been too mechanistic. So, instead, there is some recognition that change has to be managed. 7 The relationship between technological change and organisational change is interesting in which one of them drives the other or if they can be accomplished in parallel.8,9 Consistently, any type of change can be overwhelming, especially when this change occurs in large-scale healthcare organisations.9–16 Bloch et al. 2 suggest that half of all large-scale IT projects (those with initial costs exceeding $15 million) go well beyond their original budgets by 45%, and 7% over intended time, while delivering 56% less value than predicted. In their study conducted in collaboration with Oxford University, they found that the 5400 examined IT projects had a total cost overrun of $66 billion (more than the GDP of Luxembourg).
Developing an approach that suits everyone is not possible, as every implementation is unique. What works and does not work for one organisation might not have the same impact in others; however, many lessons still can be learnt keeping in mind the context of each experience when applying it elsewhere. 17 There have also been attempts at devising IT implementation strategy models for healthcare. 6 Some are change management strategies, others are project management approaches, but all have useful application when it comes to large-scale IT implementations in healthcare. Compiling a definitive list of the challenges that healthcare institutions face when implementing large-scale IT healthcare implementations is not possible. Healthcare providers are faced with IT projects of varying sizes and technical complexity and ensuring their success is crucial for organisational leaders and IT project managers alike. 18
There are numerous national IT initiatives in healthcare across the globe that can provide a wealth of experience in lessons learned or best practices. One case is Kaiser Permanente (KP); at one point the largest not-for-profit integrated health care delivery system in the United States, serving 8.7 million members across eight regions, and representing a $4 billion investment. Similarly, there is Canada’s Health Infoway, 19 MedCom in Denmark, and in the Middle East, one example is the Saudi Arabian Ministry of National Guard-Health Affairs project. 6 There is also the UK’s National Programme for IT (NPfIT); an initiative that has received much contention, and is observed in this paper as a valuable case study.
Dismantling the NPfIT
Early in 2002, the UK Government announced the award of eight major IT contracts with a combined value of more than £6 billion due to run for several years to implement new IT systems to Europe’s largest public sector organisation, the National Health Service (NHS) in England. The scale of this project was far greater than anything the UK public sector has ever seen.5,20–22 Known as the NPfIT, this ambitious scheme aimed to transform the NHS in England by implementing a centralised digitised health care record for its patients. It also aimed to provide secure access to these records by the general practitioners and authorised health care professionals in 300 hospitals. Connecting for Health (CFH) Agency was part of the UK Department of Health (DOH), and was formed with the role to maintain and develop the NHS’s national IT infrastructure, and ultimately adopted the responsibility of delivering the NPfIT.
Having a more centralised strategy and a substantial budget, the NPfIT was deemed the largest civil IT programme worldwide with an estimated original budget of £6.2 billion over 10 years.20–22 The full amount of expenditure on the National Programme is still not certain. The DOH’s 2013 statement reported a total forecast cost of approximately £10 billion. 23 Other reports have estimates close to £11.4 billion spent. At the time of the NPfIT’s launch, a large majority of health care IT projects ended in failure, and the history of IT in the NHS was mixed, with some notable successes interspersed with many more failures. After a history marked by delays, stakeholder opposition and implementation issues, the UK Government in 2011 dismantled the programme, almost 10 years after Prime Minister Tony Blair initiated it. This was followed by the demise of the CFH Agency, which ceased to exist on 31 March 2013. Some projects and responsibilities were taken over by the Health and Social Care Information Centre.
The core aim of the NPfIT was to bring the NHS’s use of information technology into the 21st century, through the introduction of integrated electronic patient records systems, online “choose and book” services, computerised referral and prescription systems and an underpinning network infrastructure. Despite the failure of many of these services to be delivered, the government, and ultimately taxpayers, incurred significant costs for the programme, including contract transition and exit costs, which continued to accrue in 2014. 3
The 2009 Public Accounts Committee report noted that the NPfIT had provided little clinical functionality to-date. The main issues could be summarised as the failure to deliver clinical benefits, data security risks, reservations of medical staff who were not adequately engaged, and contractual issues. 3
Summary of underlying causes
Campion-Awwad et al. 3 described in their case history some underlying questions about why major public sector IT projects go wrong. They identified three specific themes for the NPfIT project and cited the following reasons.
Haste
In their rush to reap the rewards of the programme, politicians and programme managers rushed into policy-making, procurement and implementation processes that allowed little time for consultation with key stakeholders and failed to deal with confidentiality concerns including unrealistic timetables, not allowing enough time to engage end users and failure to check progress against expectations.
Overambitious design
In an effort to reduce costs and ensure swift uptake at the local levels, the government pursued an overambitious and unwieldy centralised model, without considering how this would impact user satisfaction and confidentiality issues; highlighting the failure to recognise the risks or limitations of large-scale IT projects, not realising that the longer the project takes, the more likely it is to be overtaken by new technology and that the scale of the project in itself was too ambitious to manage competently.
Strategy and skills
NPfIT lacked clear direction, project management and an exit strategy, meaning that the inevitable setbacks of pursuing such an ambitious programme quickly turned into system-wide failures. Furthermore, the culture within the DOH and government in general was not conducive to swift identification and rectification of strategic or technical errors citing a lack of clear leadership, a lack of concern for privacy issues, no exit plans and no alternatives and lack of project management skills.
In a 22 September 2011 press release about dismantling the project, the UK government underlined the inappropriateness of a centralized authority making top-down decisions on behalf of local organizations. 24 They explain that the DOH calls instead for IT driven by local decision-making, hoping that the new approach would take a modular angle, allowing NHS organizations to introduce smaller, more manageable change, in line with their business requirements and capacity.
Piai and Hayward 24 eloquently summarise the reasons why explaining that the decision to create and implement the NPfIT was taken by politicians without the process and governance necessary for successfully implementing technology and business-change. The NPfIT was then imposed on the NHS with inadequate attempts to secure deep commitment and buy-in from the various stakeholders. The technology and process change were forced onto sceptical or alienated people at the ground level (the very people who would ultimately be the users of the system). For these reasons the NPfIT was officially dismantled in September 2011, and the NHS CFH ceased to exist on March 2013. The UK’s DOH called instead for a more plural system of IT; embodying “connect all”, rather than “replace all” systems. 24
Criticisms of the programme
There have been many criticisms of the NPfIT initiative over the years. Failure to identify and delineate between the perceived and actual benefits from these initiatives resulted in many of the NPfIT problems. 25 In their qualitative study, Hendy et al. 5 explore the challenges of the NPfIT in four acute NHS trusts in England. In it they conclude that implementing large-scale health service IT projects in the UK has proven difficult citing problems in achieving effective information flow between users, coupled with confidentiality and security issues. They categorise their findings under six main themes: multiple sites, communication, financial circumstances, performance, supporting legacy IT systems and timetables.
Much of the debate over the NPfIT could be characterised as a clash between those closest to it, who were committed to defending the programme and pushing through at all costs, and those who objected on practical, technical or professional grounds. The financial crisis of 2007–08 and the ensuing recession caused an obvious change in the surrounding political environment. Good governance was no longer associated with “investment”, while “waste” and “financial responsibility” dominated the national debate. This instigated a new line of attack on the NPfIT; with many lobbying to kill a failing programme to save money. 3 However, some of the aspects of the procurement process being hyped as advantageous by some (i.e. speed, centralisation and aggregation of services), were regarded as weaknesses by others, particularly in combination with a lack of proper testing and inadequacy of consultation with the hospitals, clinicians and patients who would ultimately be the end users of the NPfIT. 3
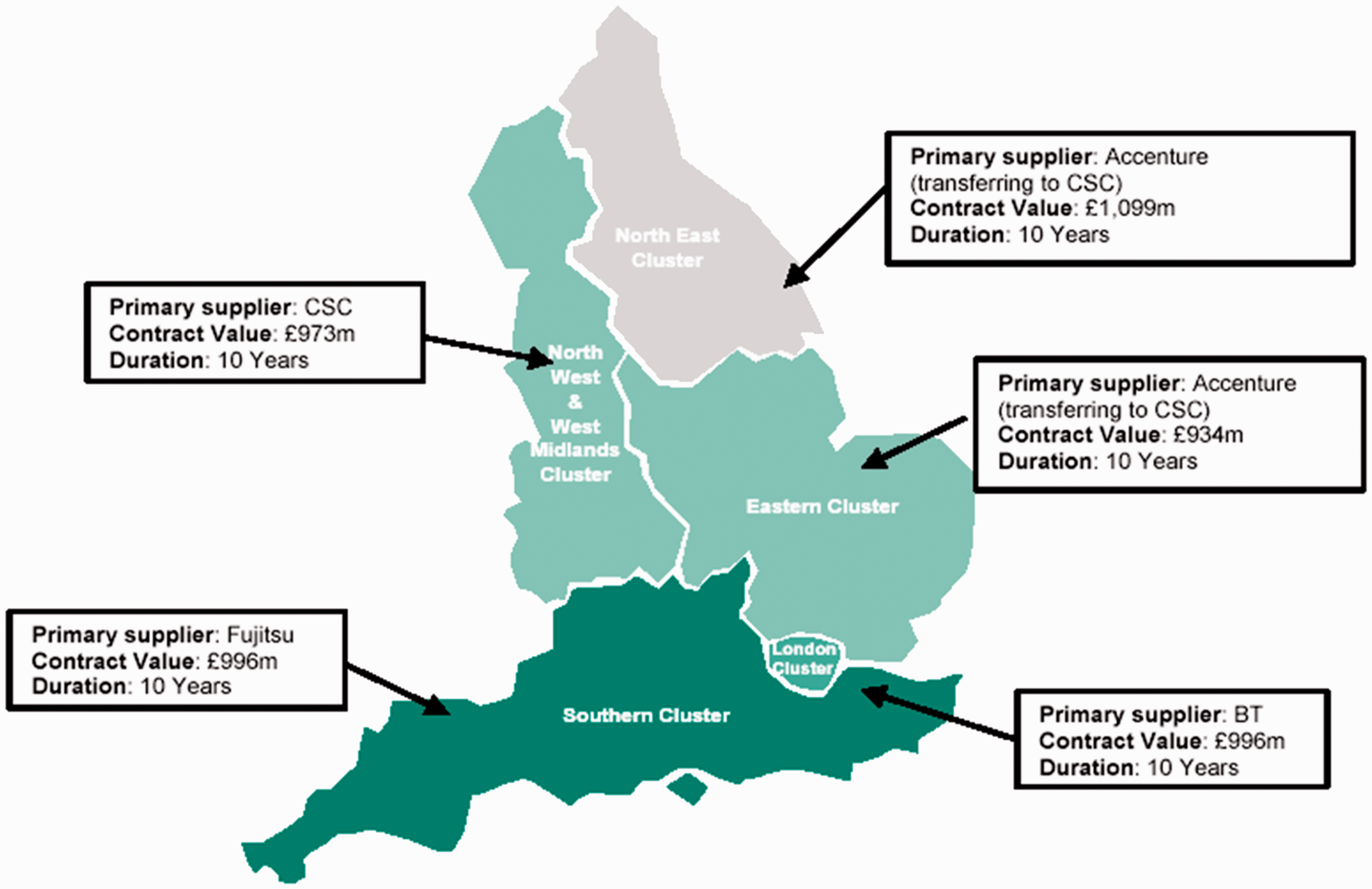
Problems continued beyond procurement and supplier departures through to the delivery and implementation of the NPfIT’s systems and software across the five Regional Clusters (Figure 1). The implementation featured some successes with elements of the programme that were on schedule and functioning well, however it was also marked by missed deadlines, unreliable software and a lack of engagement with end-users; particularly heath-professionals and patients.
3
Regional clusters and suppliers (Source: Select Committee on Health, 2007)
27
.
Socio-technical issues
Hendy et al. 5 conclude their study explaining that the socio-cultural challenges to implementing the NPfIT were as daunting as the technical and logistical ones. They recommend improving communication with front line staff. However, they maintain that it is difficult to convince users that the disruption and changes that they must experience are worth the potential benefits, and gaining users’ acceptance is at least as great a challenge as the technical one.
Protti 26 identifies many key factors for electronic health record (EHR) implementation in the UK’s NPfIT, but explains that the only two that are constantly associated with successful IT implementation are top management support and user involvement. He also explains in his report that the buy-in of the organisation is important, with a clear understanding that significant change occurs in multiple stages, and that errors in any of the stages can have devastating consequences. Furthermore, change champions must actively and enthusiastically promote the system, build support, overcome resistance, and ensure that the system is actually installed and used.
Lack of change management
It is increasingly evident that change management and organisational development approaches must accompany the introduction of an EHR adoption.
26
Stressing the role of senior leadership, Protti
26
recommends that organisations should not give up before the journey is over. He also explains that the trade-off between the healthy changes introduced by the EHR and the increased risk that its implementation will fail must be managed skilfully. In a nutshell, it is people, not technology, that make the difference between success and failure. When end users want to make IT tools work for them, even ‘poor’ tools can deliver real business value. (Protti,
26
p. 53)
Although there is wide agreement that the technological considerations and competence are necessary, they are not a condition of project success. 28 Commissioning massive IT infrastructures for national electronic health records require significant investments and careful planning5,25 yet, there is a general consensus in the field that the organisational and human factors have contributed to the success or failure of many IT projects more than the technical ones. Much of what has been published suggests that the technological issues are no longer at the forefront of problems leading to IT implementation failures, and the real causes need to be better understood.
In a quantitative baseline study on the NPfIT conducted by MORI Social Research Institute for NHS CFH, 29 the general focus of their study was on “human” factors. They only investigated five areas; awareness of NPfIT, favourability towards NPfIT, attitudes towards NPfIT, involvement with NPfIT and communication strategies. This absence of a review of the technological issues in such an extensive study shows the field’s enlightened awareness of the organisational and behavioural aspects of large-scale implementations with less focus on analysing the technological ones.
It is crucial to recognise that IT problems are usually the result of bigger business challenges and the focus should not be on the IT itself. What is more important is that technical success does not necessarily translate into implementation success. As Protti 26 explains, implementing an electronic health record is not about technology but more about a long-term cultural change programme. The technology is merely a tool that can enable that cultural change to occur. This suggests a complete paradigm shift in the way IT projects should be perceived by those who implement and use them within health care. Many have even changed the terminology associated with IT projects, shifting focus from the more technical terms, and using instead terms like “culture change” 26 and “innovation” 30 to describe these projects. The agency responsible for implementing the UK’s NPfIT was deliberately coined “Connecting for Health”, 20 without any mention of the word technology.
Project management
Project management is a critical factor in IT project implementation success. Norris 31 maintains that the most frequent causes of failure in Health care IT implementations are inexperienced project managers, inadequate methodologies, insufficient resources, low user involvement at the design stage, specification creep and a poor awareness of the cultural and organisational, rather than technical issues.
IT problems are usually the result of bigger business challenges and these business challenges should be the focus, not only the IT itself. Using the label “IT failure” to describe an unsuccessful program or project creates a perception that, if only the technology had worked, then the result would have been successful. Such a perception tends to excuse management from any responsibility that the IT failure was a result of their lack of proper project management. 25
User empowerment and engagement
People must feel ownership of their systems to appreciate the direction that they receive about the project. The NPfIT was led by a centralist approach and local health care providers were unable or unwilling to invest themselves on a national scheme for which they feel no ownership. 25
Lack of clinicians’ support has lead to project delays in the NPfIT, 25 while Brennan 20 confirms that lack of clinician engagement in IT projects can result in feelings of apathy. Rose et al. 32 equally maintain that there is a critical need to involve stakeholders in health care IT projects so that they feel ownership of these systems and are therefore less inclined to resist them. She suggests that involving users in decisions and processes should be meaningful and empowering. User involvement is a powerful tool that can change the philosophy of an organisation and all the roles within it. If managers get the processes right, users will be involved in the new changes and will have ownership of these changes. Users can become empowered because the process itself may bring about a change in the power of differentials of the various actors involved. 32
Technology and project scale
Security and confidentiality
The infrastructure for the NPfIT was an essential element in delivering the NHS plan for reform and was based on the web services architecture. This provided an IT platform to facilitate inter and intra-organisational data networks, 5 but gave rise to privacy concerns. Jeopardising privacy and security of patient data can lead to the ultimate failure of IT systems. 31 Many of the problems with the NPfIT implementation revolved around the protection of personal information, with opponents suggesting that NHS patients’ records would be connected to a more controversial e-Government initiative requiring all citizens to carry ID cards on their person. However, the NHS insisted that access to the system would be limited according to the requirements of the individual member of staff. 25 Ultimately, managing secure access to health information must be applied without interfering in daily activities. 33
Project scale
Implementing large scale public sector IT projects in the United Kingdom and other countries has in the past proved difficult. (MORI,
29
p. 9).
Project timetables
The NPfIT implementation has been described as suboptimal, leading to reports of low morale among NHS staff responsible for implementation. This is because the overall timetable for implementation was unrealistic, and trusts continued to face uncertainties directly impacting the culture of the people within. 5 Project delays are often times described as technology problems; however, Currie and Guah’s 34 study found that some delays could be described as cultural issues. These include differences in political objectives, poor communication, the problem of implementing new IT in conjunction with doing routine work, issues of security and confidentiality and the time lag between technology implementations and user training.
Recommendations
Healthcare IT projects involve more than a simple installation of a computer system within a healthcare organisation, they represent a significant change in the way healthcare is delivered, 35 and healthcare organisations must be equipped to handle this change from both logistical and behavioural aspects. Failing to acknowledge the need for healthcare IT project implementations, as “change” projects can be problematic. Currie and Guah 34 argue that the failure to implement a large-scale management change program in conjunction with the technical changes will only intensify the implementation. They further contend that there is no such thing as an “IT failure” because all technology failures are more appropriately described as “management failures”.
Capable leaders are also necessary to overcome over-managed and under-led cultures. Since management deals mostly with the status quo and leadership deals mostly with change, it is important to create and foster transformational leaders36,37 to deal with the change that the new systems will bring. Still, “managing” the project is equally as important as “leading” the change effort. Both leadership and management are required to keep change efforts and IT projects on track. For most organisations, the much bigger challenge is leading change. It has been recognised in the literature36–39 that effective leaders are needed, especially with the changing nature of management that has moved away from close control of the workforce towards environments of coaching, support and empowerment. 7
IT and healthcare strategists need to address the wider cultural imperatives and the extent to which the organisational climate and people are predisposed to adopting new IT-enabled workflows and practices. There is also general agreement that user involvement is crucial when managing large-scale change.6,40–43 Not only is user involvement valuable because of their input, but also because by involving the users, they can feel ownership of the system and better value it, leading to better acceptance and more success. Change must also be lead by local champions who feel the need to succeed and who can spread those feelings and motivate others to act upon them.12,41,42 Research in the area shows that the top-down approach for IT adoption and diffusion is likely to engender feelings of resentment and frustration among healthcare workers, rather than a willingness to adopt and adapt to these changes.22,25 Newton et al. 1 argue that quality large-scale health care IT improvement projects are feasible, only when supported by leadership on a state-wide or senior level, along with the support of a community infrastructure.
Leaders must conceive and communicate the vision for large-scale IT change, and that vision must be aligned with the overarching organisational vision.16,40,42 The organisational commitment and the objectives behind implementing any new systems must be transparent to everyone so that they have something to work towards. Successful leaders must also possess communication skills. They need to communicate on many different levels and must open different channels of communication. Positive transformational leaders must introduce change gradually and carefully.36,37,44–46 Leadership is necessary to motivate the actions needed to alter behaviour in any significant way. Once the change has been achieved, effective leadership is even more critical to get the change to persist, by anchoring it in the very culture of the organisation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.