
Abstract
Introduction
Awareness of sexual health in Malta – a small European Union member state started to gain momentum in the new millennium. Taboos and norms about sexuality pose strong barriers for the provision of information, and reproductive health services. A major contributor is the strong influence of the Roman Catholic Church, which holds fast to its prohibitions of sexual behaviours, albeit counterbalanced by the liberal standpoint adopted by the State in recent years.
Methods
Survey data were collected from 269 students aged 16–21 (response rate 89.7%) in a state post-secondary school. The sample was selected through convenience sampling within the school grounds.
Results
Women were more knowledgeable in relation to available services and risks when compared to men. No geographical differences were found. School was the most common source for information, while health professionals, namely general practitioners were considered trusted resources for their needs. Confidentiality was deemed to be the most requested and crucial feature of sexual health services.
Conclusions
Three important multisectoral needs emerged, namely adequate dissemination system of sexual health information, scientifically based sexual health education for professionals in contact with young people, and well-designed and accessible sexual health services. Implications for management include updating health sexual education and promotion strategies, as well as designing better services. Young people should be able to make informed choices regarding their sexual health, in line with contemporary needs.
Keywords
Introduction
Incidence rates of sexually transmitted infections (STIs), affecting mostly young people aged between 15 and 25 years, are increasing in Europe, Malta is no exception. 1 Indeed, the rising trend of reported STIs in Malta is a burden and far exceeds the capacity offered by current support services in health, education, social welfare and justice. 2 This creates the necessity for the evaluation of sexual health support services so as to increase the consciousness of policymakers on the subject. In the context of the European Union, sexual health service provision can be seen as both a national and international priority as movement of citizens across Europe underlines the need for adequate services in all member states. Malta, as a small island state with a population of 423,4173 and limited resources, faces huge challenges for utilising part of the annual budget on disease prevention and health promotion, amongst which preventing sexually transmitted diseases and promoting sexual health. 2
Awareness of sexual health in Malta started to gain momentum after 2001 but it was only in 2011 that a robust strategy was launched. 4 As part of the launch of the strategy that reported a national survey, the Minister of Health claimed that ‘a third of people engaging in sexual activity for the first time do not use contraception, this needs highlighting especially in a context where around 41% of 16 to 18 year olds are already exploring sexual activity’. 5 Schembri and Carabot stated that sexual health services in Malta are still in their embryonic stage with the only official services being that of the Genitourinary (GU) clinic at the main hospital. 6 Furthermore, as in most countries, taboos and norms about sexuality pose strong barriers for the provision of information, reproductive health services and other forms of support. 7 A major contributor is the strong influence of the Roman Catholic Church that holds fast to its prohibitions on sexual behaviours. 8 Despite the Church’s conservative approach on sexual health in Malta, the incidence and prevalence of STIs and teenage pregnancies have not shown any sign of a decline over a 10-year period. 9 This may be due to two main reasons. On the one hand, as in other rather conservative Catholic countries, sexual health has remained underdeveloped because the Roman Catholic Church has offered high resistance to changes related to sexual practices, even though it was on the Maltese government’s agenda for several years.9,10 On the other hand, the fact that the state is becoming more liberal in orientation, as evidenced by the enactment of laws that were noncompliant to Catholic teaching, 11 is a reflection of the population’s changing lifestyles that are less likely to be guided by the Roman Catholic Church.
It is of utmost importance that when planning sexual health services, one identifies the actual needs of service users through empirical research. 12 Additionally, education is an essential part in achieving sexual health, understanding the associated risks and making informed choices preventing teenage pregnancies. 13 Quality research is needed to reach young people, in particular those who are vulnerable, so as to identify effective tactics that would lead to better community acceptance of sexual health services for this age group in the community. 14
This study built on the 2011/2012 national survey and assessed the sexual health services’ needs of Maltese young people, in a post-secondary school, as part of needs analysis for the development of sexual health services in Malta, and therefore focuses on young people, who would have successfully completed secondary school education.
Bradshaw’s taxonomy of needs (Figure 1) and health belief model (HBM) form the theoretical basis of the study. Bradshaw describes four perspectives of needs, namely felt needs, expressed needs, normative needs and comparative needs. 15 This study investigated young people’s felt and expressed needs. Additionally, it explored comparative needs by analysing the different socio-demographic characteristics in the population under study. This study also explored normative needs through the literature.
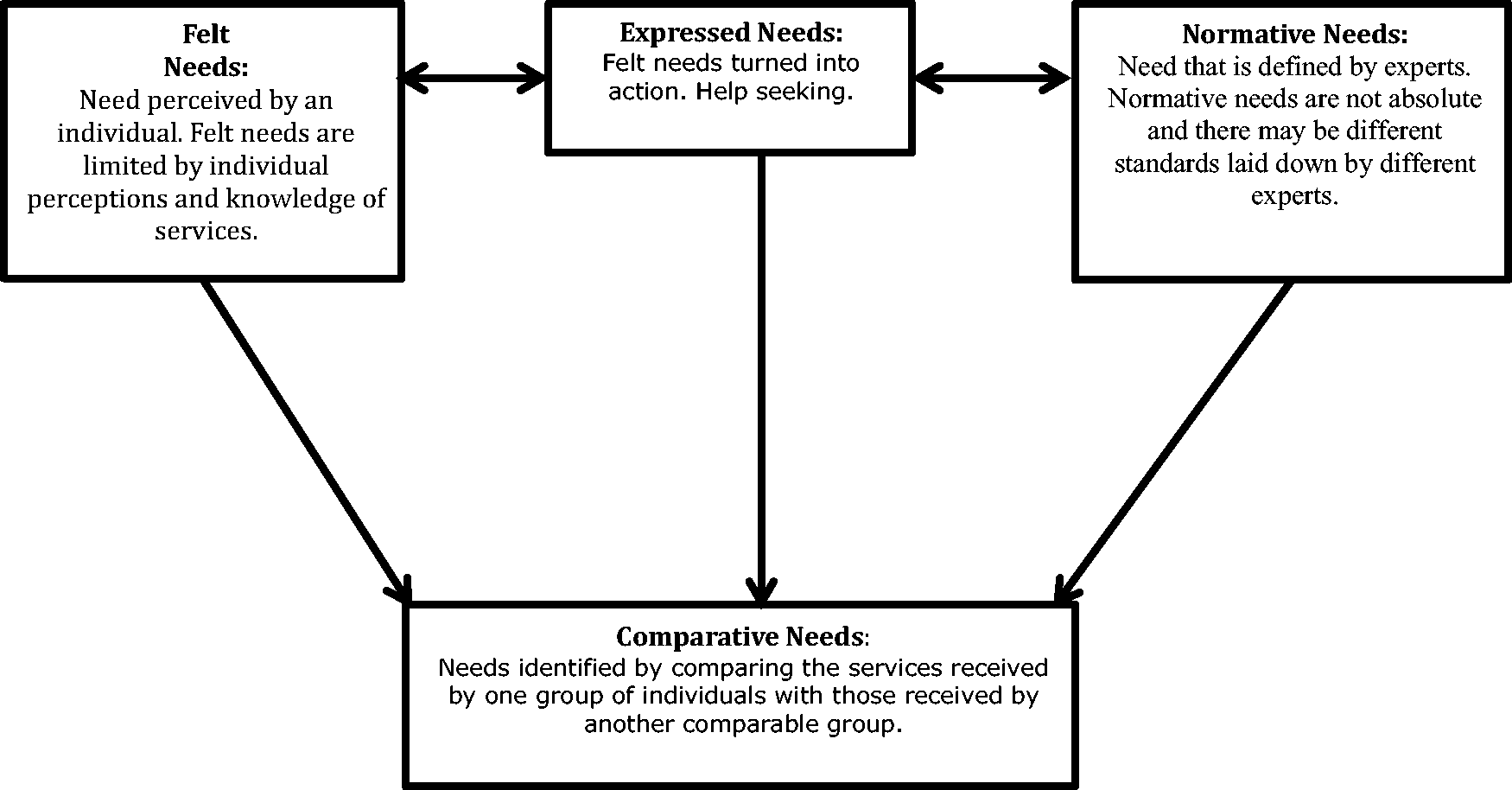
Dimensions of needs (adapted from Bradshaw 15 ).
The HBM,16 which accounts for the young people’s readiness to act on sexual health matters, proved useful to discuss the findings of the study. HBM explains health behaviours through four perceived constructs, namely susceptibility, severity, benefits and barriers, and which account for people’s ‘readiness to act’, which in this context would mean primary and secondary prevention or seeking sexual health services. Cues to action would then activate this readiness and stimulate manifest behaviour.
Methods
Research design
The study employed a cross-sectional design using self-administered structured questionnaires. Following an extensive literature review, the psychometrically tested questionnaire for conducting needs assessment of the sexual health needs of young people in the UK was chosen. 17 However, since this instrument was being used in a different geographical area, an expert panel reviewed it. Additionally, it was piloted and adapted prior to fieldwork. The questionnaire was composed of three sections, namely perceived risk level – including information about knowledge of STIs and their transmission; knowledge and accessibility of services-including knowledge about existent services and sources of information, and desired sexual health services–identification of services required by young people, and the running and provision of the services including opening times and location. The three sections therefore attempt to address the needs analysis in two ways, namely to assess what young people currently know about sexual health and STDs, as well as what services are available, in line with felt needs i.e. gaining perceptions and knowledge of services. In addition, the tool endeavours to capture the young peoples’ preferences on how they would like sexual health services to be run, thereby capturing expressed needs on help seeking behaviour. Comparative needs are captured through the analysis of demographics, so as to analyse statistically significant differences between groups.
Target population and sampling techniques
The target population for this study was young Maltese residents aged between 15 and 25 years in state post-secondary education. Permission to conduct the survey was granted by school authorities however due to data protection, they did not supply a list of students for the selection of a random stratified sample which only left room for non-random convenient sampling. Self-administered questionnaires were distributed to 300 out of the 2500 students attending the school (12%). To ensure anonymity and a better response rate, respondents were asked to deposit their questionnaires in a locked box located in a common area within the school. Data were analysed using the Statistical Package for Social Science (SPSS Version 22.0 for Windows®).
Ethical considerations
Ethical permission to carry out this study was granted by the University of Malta Research Ethics Committee. Permissions were sought from the authors of the tools and from the head of school where the research was conducted. The participants were also given covering letters to introduce the nature and purpose of the study.
Results
Description of study population
From 300 questionnaires distributed, 269 (89.7%) participants responded, of which 34.9% were men and 65.1% were women. The age of the participants ranged from 16 to 21 years (both ages included) of which 90% (n = 242) were between 16 and 17 years old and 10% (n = 27) were 18–21. In addition, 19% (n = 51) of the participants were living in the Southern Harbour, 23% (n = 63) belonged to the Northern Harbour, 20% (n = 53) came from the South-Eastern district, 25% (n = 68) resided at the Western district, while 12.6% (n = 34) lived in the Northern district of Malta.
Knowledge and perceived risks
Table 1 shows that students were most knowledgeable about HIV/AIDS when compared to the other STIs. The least known STI was Chlamydia. Chi-squared tests revealed statistically significant gender differences in knowledge about STIs with women being more knowledgeable than men. Only four respondents said they did not know what STIs are. Awareness was also analysed by district of residence. There was however no statistically significant difference of knowledge scores between the five districts (F = 1.056; P = 0.379). Table 1 also shows that the majority of respondents (n = 244; 90.7%) chose condoms as the best method to prevent STIs followed by abstinence (n = 103; 38.3%), which was identified more by women (n = 78; 44.6% of all females) than men (n = 25; 26.6% of all men) (χ2 = 8.363; 1df; p = 0.004). A proportion of respondents incorrectly identified the contraceptive pill (n = 51; 19.0%) and withdrawal (n = 38; 14.1%) as methods for preventing STIs. A significantly greater proportion of men incorrectly identified the pill as a method for preventing STIs (χ2 = 4.063; 1df; p = 0.044).
Gender differences in awareness of sexually transmitted diseases and in use of methods of contraception to prevent them.
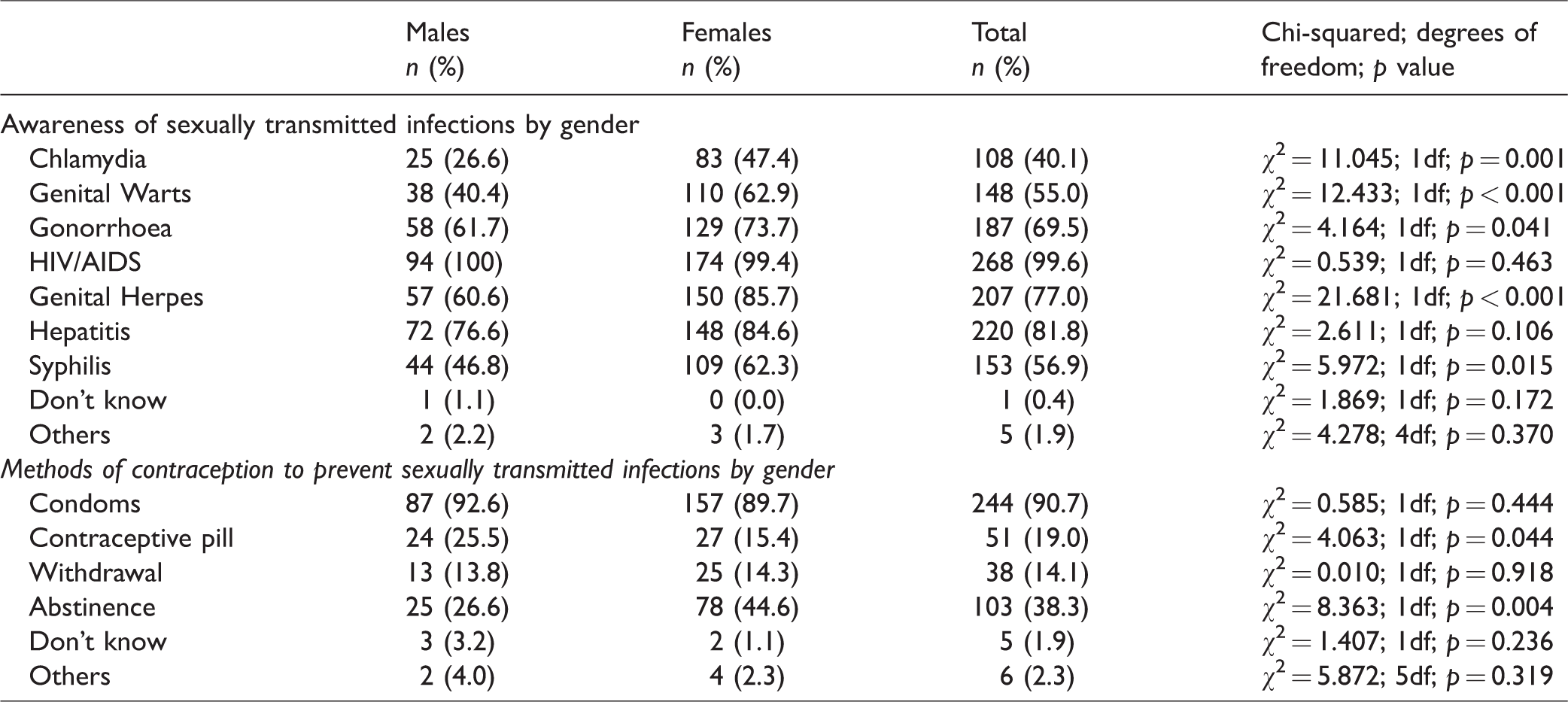
The first four questions of the questionnaire tested young people’s knowledge and modes of prevention of STIs and pregnancy. For this purpose, a knowledge score was created. For each correct answer given each participant was awarded a point while wrong answers got no points. This generated a total score for each participant. The maximum score obtained by participants was 94 while the mean score obtained was 57.4. Mean scores were analysed by gender and district. There was a significant gender difference in mean score; with men on average scoring 49.3 (standard deviation (SD) =0.21) and women scoring on average 61.6 (SD = 0.19) (t = −4.649, df = 164.3, p < 0.001 (two-tailed)). There were no significant differences across districts.
Table 2 shows the perceived risk of acquiring specific STIs from unprotected sex by gender. HIV/AIDS ranked highest for both sexes, with no statistical significance between men and women. There were however significant gender differences for Chlamydia, Syphilis, Gonorrhoea and Genital Warts with more women perceiving a risk of acquiring these STIs than men. When young people were asked to give a rating for their perceived risk of acquiring any STIs when having unprotected sex, more women (n = 84; 48% of all women) than men (n = 23; 24.5% of all men) perceived their risk as high, as shown in Table 2. This difference is significant. Furthermore 33.5% (n = 90) perceived being at high risk of becoming pregnant when having sex without using condoms. There was a significant gender difference with women reporting higher risk levels of pregnancy when not using a condom.
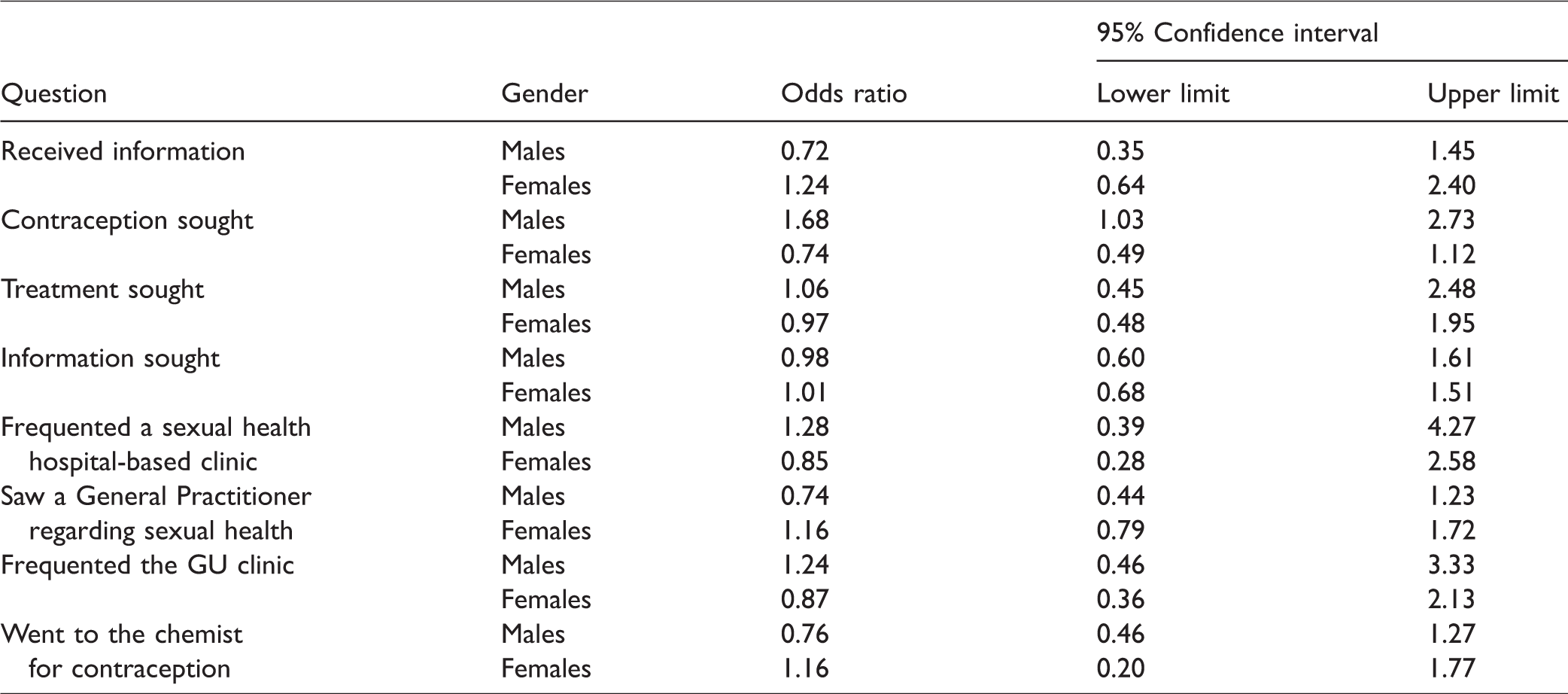
To assess the impact of knowledge on perceived risk of acquiring STIs, odds ratios (ORs) were calculated comparing risk level for those who had sought out information, contraception or treatment compared to those who did not (reference). ORs were calculated for both genders separately. The only significant difference found was between males who sought out contraception and those who did not. Those who sought out contraception had a higher perceived risk compared to those who did not seek out contraception: OR 1.68 (95% confidence interval (CI) 1.03–2.73), as shown in Table 3.
Gender differences in the perceived risk of acquiring sexually transmitted infections from unprotected sex including perceived risk levels of STIs and pregnancy when not using condom.
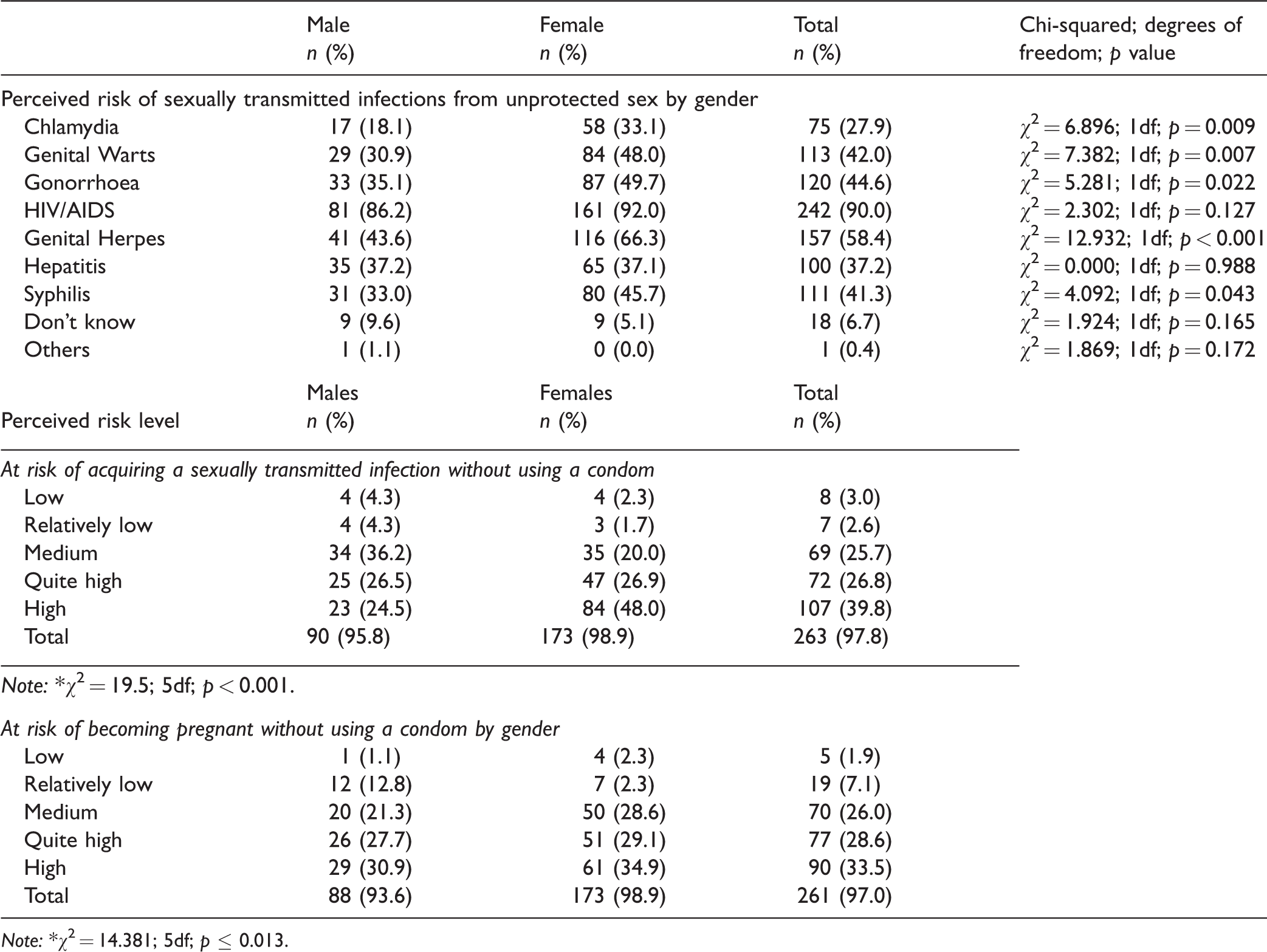
Note: *χ2 = 14.381; 5df; p ≤ 0.013.
Gender differences in terms of odds ratios and limits of 95% confidence intervals on choice of receiving/seeking sexual health information/treatment/service.
Sexual health importance and sexual activity among young people
Young people were asked to rank how important sexual health was to their lifestyle. Most men (n = 40; 42.6% of all men) and women (n = 104; 59.5% of all women) considered sexual health as being very important with both genders seeking advice related to sexual health. Contraception usage was higher amongst men with 47.9% reporting they sought contraception compared to 29.7% of women (χ2 = 9.360; 2df; p = 0.009).
Information sources and sexual health services
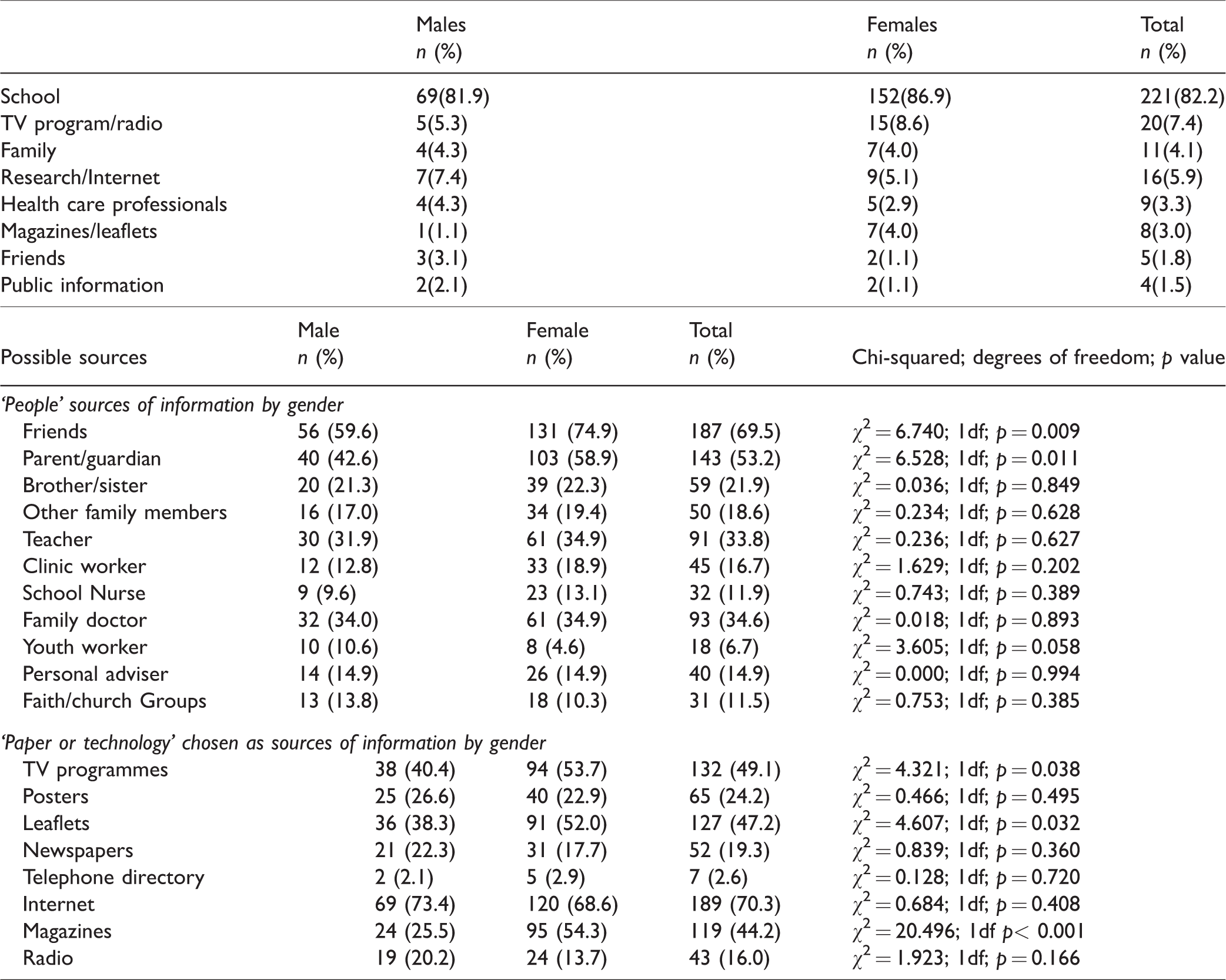
Table 4 shows that the most common source for information on STIs for both men (n = 67; 71.3% of all men) and women (n = 152; 86.9% of all women) was school. This was followed by television or radio programmes (n = 20; 7.4%), internet (n = 16; 5.9%) and family (n = 11; 4.1%). Table 4 also shows ‘People’ sources of information by gender, as well as ‘Paper or Technology’ chosen as sources of information by gender. The most preferred source of information from the ‘people’ category was friends followed by parents/guardians, with significant gender differences for both. On the other hand, the most popular source chosen from the ‘paper or technology’ group was the internet followed by television programmes, leaflets and magazines. Participants identified medical services such as GPs (n = 232; 86.2%), with 63.9% specifically mentioning the genitourinary clinic as presently available primary services. When asked to choose the services they had been to, participants again mostly chose health services such as GPs (n = 95; 35.3%) and chemist (n = 93; 34.6%), Confidentiality ranked highest (n = 127; 47.2%) among the important characteristics being offered by current sexual health services.
Gender differences in sources of information on sexually transmitted infections.
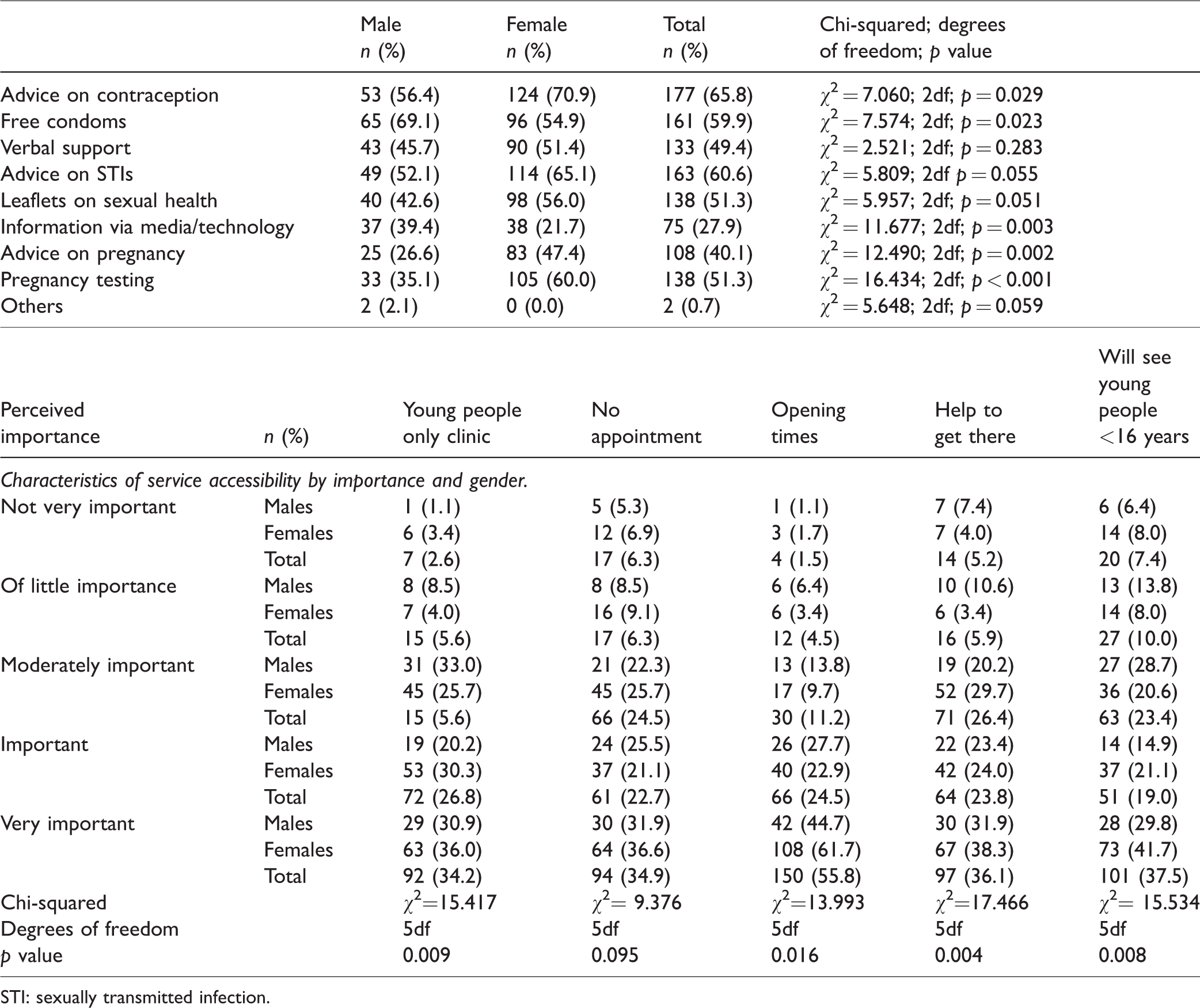
With reference to service accessibility issues, 16% (n = 43) stated that young people under the age of 16 years are always seen while 13.8% (n = 37) stated that the services are always open. Most of the participants showed that they were not knowledgeable enough about the current public sexual health services that are available. Specifically, 39.4% (n = 106) did not know whether services were free, while 13.4% (n = 36) said that services were never provided for free. This may be due to the practice of paying a fee-for-service when visiting private GPs. From the given options, the fact that the majority of young people chose ‘don’t know’ as their answer for these questions may indicate either lack of awareness of what is actually being offered or that, as of yet, they had no real need to make use of sexual health services. Respondents were asked to select the features they desire most from sexual health services, Table 5 shows that advice on contraception is the most desired service. Both women and men rated confidentiality as being ‘very important’. Friendly staff was also rated highly by all the participants. Quite a large number also mentioned free services, skilled staff, understanding staff and staff of the same sex as very important. When looking at gender differences, leaflets and posters were considered as ‘very important’ by women and of medium importance by men. Table 5 shows that in relation to service accessibility; the issue considered by most participants as ‘very important’ was opening times, followed by access for those under 16 years of age, ‘Not needing an appointment’, and having a ‘young people only clinic’. As regards location, 40.9% prefer services close to their residence, whereas 23% chose the option ‘near where I go to school’. As regards opening times, 42% preferred afternoons and a further 37.9% preferred evenings. Most participants, women in particular, preferred Monday to Friday (χ2 = 7.388; 1df; p = 0.007), whereas 40.5% of participants (n = 109) preferred Saturday morning.
Gender differences in types of services requested and perceived importance on some characteristics of service accessibility.
STI: sexually transmitted infection.
Respondents were given the opportunity to list further aspects of sexual health services, which they perceived as being important. A total 6.3% (n = 17) mentioned the importance of creating more awareness, knowledge, information and education in church schools, 2.2% (n = 6) insisted on the importance of abstinence, no sex before marriage and religious beliefs, and 1.9% (n = 5) mentioned more promotion of the use of contraceptives, condoms in particular.
Discussion
The World Health Organisation emphasises the importance of sexual health in young people’s lifestyles. 5 Sexual health and well-being of young people can only be ensured if they have access to youth friendly health services. 14 More than half of this study’s participants ranked sexual health as very important, thereby justifying the need for a thorough assessment in Malta. The literature provided an explanation of normative needs. The main shortcoming of basing health services planning solely upon normative needs is failing to consider the different needs of the service users. 18 This study therefore contributes to the needs assessment by providing results of felt and expressed needs on sexual health by the young people in the post-secondary school involved in the study. The participants’ expressed needs reflected the requirements based upon people’s use of services, for example waiting times and availability of services. Comparative needs, which were assessed by analysing the needs across gender and geographical location, should enable policymakers to focus their strategies and resources where they are most needed.
On the basis of participants’ incorrectly answered questions in the questionnaire and a mean of only 54% in the knowledge score on STIs, one can potentially draw the conclusion that there is lack of sufficient knowledge on sexual health. Furthermore, the lack of sufficient knowledge is reflected though the unchanging trend in teenage pregnancies in Malta over the past 10 years and increasing rates of STIs particularly in young people aged between 15 and 25. 10 The apparent insufficient knowledge contrasts with what some authors concluded, namely that young people in Europe have overall good understanding of issues related to sexual health.19,20 This highlights the differences across Europe in relation to sexual health knowledge and brings to the fore the need for cross-country comparisons. These differences could suggest that the current provision of sexual health education in Maltese schools is not adequately preparing young people to lead a healthy sexual life. However, the relatively high awareness of HIV and AIDS, which is similar to findings from previous studies is suggestive that intense media attention, as well as health promotion and education campaigns is effective.17,,21 The same cannot be said about Chlamydia infections, which in this study were the least known STIs, even though infection rates are increasing rapidly within EU countries including Malta. 1 Wakely, Cunnion and Chambers argued that the globally successful HIV and AIDS campaigns could have overshadowed the dissemination of information about other STIs. 17
This study has also highlighted various examples of gender differences on sexual health awareness and knowledge with regard to both STIs and service provision. By and large, women seem to be more knowledgeable than men. These findings, namely that women were significantly more aware of Chlamydia, Genital Warts, Gonorrhoea, Genital Herpes and Syphilis than men, are in accordance with findings from international studies.19,21,22 Therefore, in addition to addressing the whole population, health promotion and education campaigns, as well as service provision should strategically target the specific needs of men. On the other hand, this study did not reveal any significant geographical differences on awareness of STIs and on knowledge scores. This result should be taken in the context of the small size of Malta and contrasts with the geographical differences in sexual health reported in bigger countries like the UK. 23
As regards prevention, nearly all the participants identified condoms as the primary method to prevent STIs, followed by abstinence. Some participants erroneously chose other methods, confirming insufficient knowledge on the subject. These findings are in agreement with what was reported in the literature in and outside Malta, namely that knowledge about contraception was generally poor and misconceptions rife.4,24,25 This needs assessment therefore reconfirms the need for more awareness about contraception including abstinence to the younger age groups so as to increase their knowledge and eliminate misconceptions. 26 However, being knowledgeable about STIs and sexual health does not always result in safe behaviour, indicating the complexity involved in engaging in health-promoting behavioural choices.17,27,28 As explained by HBM, a health-related action, for example use of condoms, is taken if individuals feel that STIs can be avoided, or have positive expectations that by using condoms will be effective at preventing STIs, or believe that they can use condoms comfortably and with confidence. Various studies have demonstrated that young people are sexually active at a young age and the view of young people about contraception and their perception of risk of pregnancy are complex.27,29 Although in this study a direct question of whether participants were sexually active was not asked, due to resistance from the authorities of the school, a proxy question ‘have you ever sought contraception?’ was asked. The result that about 40% of participants had sought contraception is suggestive of engagement in sexual activity.
This assessment also focused on sources of information. The most frequently mentioned source being school and the least being family. Yet young people did not necessarily prefer school as their primary source of knowledge. 30 Although schools are considered main sources of sexual health education, proper delivery of information may still be lacking.30,31 Despite the family being the least chosen source of information, parents and guardians are still considered as primary sources of sexual health information. 26 Widman and her colleagues found that increased sexual communication between young adolescents and their parents was associated with more sexual communication with dating partner. 32 Youth who participated in more communication with their partner were found to use condoms more frequently than those who communicated less with their partner. Therefore, parents might be identified as yet another target group for parenting skills, health promotion and education campaigns. 30 Finally, the majority of participants chose the Internet as the prime source of information, similar to the results obtained by Buhi and colleagues. 33 Indeed, sexual health services and health authorities could make better use of the Internet, including information web sites, if they successfully want to target young people especially in the area of social media which has been found to have many benefits for the informal spread of health communication. 34
As regards current sexual health services, the fact that participants’ knowledge on the subject appeared to be incomplete is in line with findings from other international studies.17,35 However, in order to ensure that sexual health services meet the required needs of the population, one must ensure that they meet quality standards, namely efficiency, effectiveness, accessibility and equity. 35 On a positive note, this study showed that participants who knew about the services were aware of the confidentiality guaranteed. Still in general many were unaware of the availability and accessibility of sexual health services. Therefore, this finding might suggest that these services are not readily available and accessible, or have not been adequately promoted or may not be sufficient to cater for young people’s needs similar to findings in the literature. 35 This assessment therefore strongly recommends that health authorities should develop a robust marketing strategy on sexual health so as to make sure that the target population is being reached. Research shows that sexual health services must be provided by health professionals specifically trained in sexual health.17,31 The evidence on the effectiveness of young people’s friendliness training programmes for health workers is limited. 14 In particular, the fact that participants identified family doctors as reliable service providers highlights the need for adequate training of GPs. These findings are particularly striking when one considers that various studies have shown that young people are more likely to seek advice and information regarding their sexual health from friends and family rather than from health professionals.17,20 The gender differences highlighted previously also punctuate the need to focus the primary care sector towards targeting the sexual health needs of adolescent males which also seem to be largely unmet in this setting.
As regards expectations from services, the participants identified a number of desired components of a sexual health service mainly advice and information, free contraceptives, sexual health counselling and family planning as well as free testing for HIV and other STIs. These views are similar to findings in other studies.13,36 Additionally, participants suggested that services offered must be confidential, staffed with friendly, skilled and understanding personnel, as well as being run by same sex staff, which is also in line with other studies.35,36 Wakely, Cunnion and Chambers identified that young people must be provided with the right services that should be delivered in an empowering and non-judgmental way. 17 Meanwhile, confidentiality is an aspect that, if not maintained, could act as a barrier towards accessing sexual health services. 35 This confirms the finding from this study that a major priority for effective sexual health services provision is confidentiality.
In this study, only a small percentage of young people claimed that they preferred services, which cater for young people only, similar to other studies. 13 In balance, although the results do not clearly favour speciality clinics on the basis of age group, more studies should be undertaken to validate these findings. Participants preferred services to be offered during the afternoons and ideally Monday to Friday and Saturday mornings, similar to other studies, which identified preference for after-school hours and Saturdays and during free time.13,15 These findings suggest that there is a need for revising current opening times of sexual health services in Malta.
Respondents preferred sexual health services which are located close to where they live a finding similar to that found in the UK.1,17 This might indicate the need to further explore the possibility of providing sexual health services in various localities. However, considering Malta’s small size and limited resources, this may not be feasible and desirable. The best solution might be that sexual health services should be located where young people meet, close to nightlife and possibly avoiding the usual clinic settings.
Conclusions
Malta represents a compelling context to study the needs for sexual health services in young people for several reasons. It presents an interesting historical religious background in particular the conservative teachings of the Roman Catholic Church on sexual relationships, which have been increasingly challenged by the progressive liberal State and health promotion lobby. It is a small island European Member State with limited resources for preventing sexually transmitted diseases and promoting sexual health. In addition, its geographical location captures the southern European and Mediterranean perspective. On these bases, Malta provides an informative case study for sexual health needs in Europe. This study provides important implications for the sexual health policy agenda in Malta in that it reinforces the Maltese Sexual Health Policy’s principles of the young people and society’s rights and responsibilities based on the values of esteem and dignity of healthy human life. 5 It provides important findings that would enable policy makers in Malta to reach the targets, goals, measures and deliverables as specified in the policy document. 5
Limitations of the study
Since the sample chosen was a convenient one, the results obtained are of unknown generalizability and thus, there is no guarantee that the responses given by the participants represent behaviours of other groups. In addition, due to convenient sampling it was difficult to assess precision or reliability. Questionnaires were not completed under examination conditions and thus young people could have influenced each other potentially creating bias.
Recommendations
The recommendations are twofold. These mainly concern health promotion and education strategies, as well as those associated with the re-design of sexual health services. There appear to be gaps in the current health promotion strategies on sexual health, namely lack of success in targeting all the key players (e.g. men, parents, teachers, GPs, school nurses). Issues of accessibility must also be taken into consideration. In order to provide sexual health services of high quality one needs the required people for their delivery. Hence, this might lead to the need of training of new professionals in the sexual health field. Although in 2011, Malta launched its first sexual health policy and strategy, which gave increased visibility to sex education campaigns, more needs to be done and implemented. 2 One must recognise the need of this sexual health education strategy involving the multiple entities responsible for delivering primary information to young people. This strategy must also be further extended to all formal and informal organisations that have direct contact with young people and must be audited in order to ensure that the needs of young people are being met. Further research could include exploring the needs of young people coming from different post-secondary schools and comparing them. This would yield results with stronger statistical power which would in turn allow more in-depth statistical findings. Exploring the needs of young people coming from different cultural backgrounds and different strata of society would also be essential. In this manner one would be able to design services which cater equally for all. One could also propose studies to explore the effectiveness of the sexual health services currently being delivered in Malta, and compare these with benchmarks in Europe.
This study clearly shows the necessity for a multi-sectoral approach so as to ensure successful implementation of the sexual health strategy, as well as efficient and effective delivery of sexual health services. In addition, the wider religious and cultural context should be taken into consideration so as to successfully overcome barriers. The needs that emerged reflect this multi-sectorial line of action, namely adequate dissemination system of sexual health information, scientifically based sexual health education for professionals in contact with young people, and well-designed and accessible sexual health services. It is only through concerted efforts of various disciplines and sectors, will we be able to provide young people with the possibility of making informed choices regarding their sexual health, in line with contemporary needs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.