
Abstract
Objective
To test the hypothesis that the fellow patient is a relevant dimension of patient satisfaction and has a notable influence on patient evaluations of hospitals.
Data sources/study setting
An empirical survey was conducted to collect primary data. In the study, patients in German hospitals were asked about their perceived satisfaction with fellow patients, physicians, nursing staff, and facilities.
Study design
Linear regression models were used to estimate the influence of each dimension on patient satisfaction. Various quality criteria further confirmed the quality of the extended patient satisfaction model.
Principal findings
The study confirmed fellow patient influence as a fourth dimension of patient satisfaction. The fellow patient had the highest impact on patient satisfaction and increases the variance of the patient satisfaction model significantly.
Conclusion
The findings suggest that patient satisfaction models should include the fourth dimension, “fellow patient.” In addition to the impact of the other satisfaction dimensions, both studies highlighted the significant influence of the fellow patient on patient satisfaction. Moreover, hospital managers should try to use the impact of the fellow patient to create satisfaction, which would benefit both hospitals and patients.
Introduction
In recent decades, the field of health research has focused intensively on how important it is to understand patients' assessments of the hospital environment. However, to understand patient assessments, researchers need to identify all relevant environmental factors that influence patient satisfaction.
Early patient satisfaction models focused mainly on patient satisfaction with physicians and nursing staff as relevant dimensions. Subsequent studies showed that, in addition to these dimensions, satisfaction with equipment, facilities, and catering also plays an important role. Investigations proved that these three dimensions influence overall patient satisfaction by enhancing their wellbeing and provoking positive or negative emotions, such as pleasure, anxiety, and self-esteem.1,2
Studies from other service contexts suggest that there could be another dimension that impacts patient satisfaction: fellow patients. Some researchers have found a positive relationship between customer-to-customer (C2C) interaction and satisfaction.3,4 In addition, numerous qualitative studies in hospitals have suggested that the fellow patient in a shared room has an impact on the focal patient’s satisfaction.5,6 However, despite calls for an extension of the existing model of patient satisfaction, 7 research on the impact of the fellow patient is still missing.
This study aims to contribute to the improvement of patient satisfaction models and to test whether examining the role of the fellow patient can increase these models’ reliability and significance. The assumption that the fellow patient is a significant dimension in patient satisfaction is tested in a regression study on the influence of the fellow patient in addition to the dimensions previously identified as relevant (physicians, nursing staff, and facilities). Within the study, a single-item measurement is used to answer the question of whether the fellow patient has a significant impact relative to the other dimensions. Additionally, the “classical” model and “new” one are compared to see whether adding the fellow patient dimension increases the validity of the information.
Theory and conceptual framework
In health care research, patient evaluation and perception of health care have been recognized as important parameters for both researchers and practitioners. However, it is important to understand on what basis patients form their opinions in order to improve caregiving and ensure patient satisfaction with the hospital. Hospital management has become increasingly aware of the significance of patient satisfaction. 8 A large number of studies make it clear that by increasing patient satisfaction, patients’ wellbeing and loyalty to hospitals can be enhanced. 9 Patient satisfaction also has been used as an indicator of quality and as a construct for measuring patients’ perceptions of good health care. 10
In recent years, researchers have developed various methods for measuring patient satisfaction and its influencing variables. It was revealed that the three (physicians, nursing staff, and facilities) influence patient satisfaction in particular. Physicians and nursing staff influence patient satisfaction in similar ways. Physicians, for example, influence patient satisfaction positively by establishing a good relationship with the patient, which includes communicating empathetically, providing detailed information, and asking about the patient’s feelings and opinions.10,11 Similarly, nursing staff influence patient satisfaction through caregiving, communication, and empathy. 12
The different characteristics of physical facilities and their influence on patients’ evaluations comprise the third relevant dimension. Elements of the dimension are able to hasten their recovery and reduce their stress. 13 Additionally, some features can improve patient perceptions of control and allow social support and distraction during hospitalization. 14 Furthermore, studies have revealed that satisfaction in hospitals correlates positively with the quality and quantity of food provided. 15
Baker et al.’s theory of environmental influences provides an explanatory approach to these dimensions and their effect on patient satisfaction with hospitals. 16 This theory implies that different environmental dimensions influence people’s perception of services and lead to positive or negative reactions. The main dimensions include environmental factors (temperature, lighting, smell, noise), design factors (architecture, color, materials), and social factors (employees and other customers). Previous studies in health care have investigated the effects of physicians and nurses (social factor) and physical facilities such as architecture, spaces, and facilities (design factor)17,18 in patient satisfaction models. However, the influence of the other customer, as per Baker et al.’s 16 theory, has been overlooked in most satisfaction models, and especially in health care research. Although analyses in different service settings—such as store environments, 4 tourism, 19 and other services3,20—have proven a significant influence from the other customer, few studies have tried to extend C2C research to health care settings. 7
A number of investigations have demonstrated that patients in a hospital influence each other. In the early 1950s, scientists became interested in the interaction of patients. Studies have shown that interactions can either be positive and helpful, or negative and a burden.21,22 Thus, fellow patient interaction can encourage patients, or increase the stress and insecurity they often feel.
Patients prefer a pleasant and balanced atmosphere. Album, 23 who used observation techniques to analyze patient–patient interactions, found that patients act according to rituals and try to avoid disputes, noises, and disturbances. Additionally, he discovered that patients share a variety of information, including about their diseases and the hospital staff. 23 These exchanges between patients can have a positive effect on their perceived anxiety; for example, Van den Borne et al. 24 found that how patients compare their situation with other patients in the unit can influence how they cope with their fears. In addition, fellow patients and their treatment of their disease are perceived as role models and, thus, can create hope and increase self-esteem. Kulik et al. 25 came to similar conclusions: they verified that contact with postoperative patients can decrease the anxiety of preoperative patients. Furthermore, their study pointed out that patients exchange information and develop a feeling of solidarity. Comparable illnesses, situations, and backgrounds create fellowship and reduce uncertainty and negative feelings.5,22 Furthermore, similarities between patients lead to satisfaction with the fellow patient. 20 Another study by Kulik et al. 26 showed that a high level of contact with fellow patients can lead to satisfaction with care and postoperative emotional wellbeing.
Besides these identified positive effects, patients may also influence other patients negatively. Reasons for a negative assessment of a fellow patient may be stressful behavioral characteristics, such as snoring or coarseness, or dissimilarities between patients. Severe illness in a fellow patient could also be a burden and lead to depression, increased stress, and reduced hope.20,27,28 The positive and negative influence of the fellow patient can affect not only the feelings of the patient but also his or her perception of the hospital. Therefore, Nicholls 7 pointed out that there is a need for further health care research on patient–patient interactions and their influence on satisfaction.
This study is a first contribution towards including fellow patients as a fourth dimension in patient satisfaction models. It is based on the patient-satisfaction model created by Olandt and Benkenstein 18 to study the impact of physicians, nurses, and facilities in a German hospital. The model is valid and reliable and includes the main influence factors mentioned in the literature. 17 With respect to facilities, Olandt and Benkenstein also distinguished between the influence of the room and the meals.
Based on the previous research, we hypothesize the following:
Furthermore, drawing on recent studies6,7,23 on patient-to-patient influences in hospitals, we expect that:
Figure 1 shows the two-step measurement procedure used. In the first step, only the known dimensions are included in the regression model, while in the second step, the fellow patient is added. This is to show that the fellow patient has a significant influence on patient satisfaction and that, therefore, the new model has an increased explained variance.
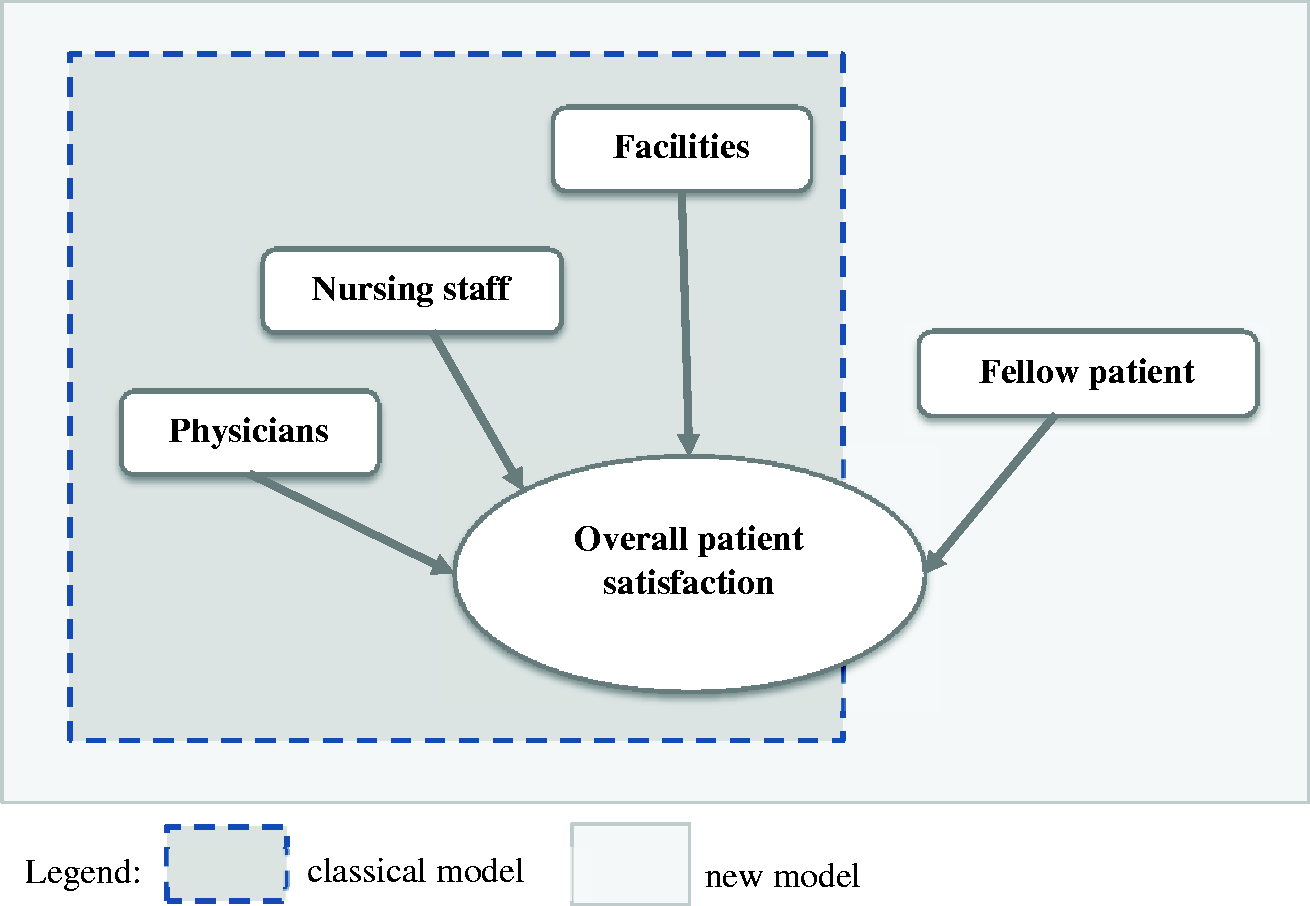
“Classical model” and “new” patient satisfaction model.
Method
For the study, patients of a German university hospital were asked to evaluate the hospital and their satisfaction with various factors during their stay. In the survey period from October to November 2015, a total of 133 patients of the orthopedic ward were asked to participate in the study. Some patients declined, while others were too sick to participate; thus, 73 patients ultimately participated in the study. In order to test patient satisfaction, three interviewers were familiarized with the contents of the study. In the orthopedic ward, the nurses told the interviewers whom of the patients placed in a two-bed room were to be interviewed. Subsequently, only patients who had been in the hospital for at least one night and who had shared their room with a fellow patient during their stay were included in the study. After expressing their agreement, the patient was taken to a private room and given the questionnaire. The interviewer was available for questions and, after completion of the questionnaire, asked if the patient had any further comments. Our scale questionnaire was taken from the study by Olandt and Benkenstein. 18 However, for the different dimensions (physicians, nursing staff, and facilities), only the global items were taken in the questionnaire, and the fellow patient dimensions were supplemented for the new measurement model. The questionnaire by Olandt and Benkenstein was validated and also for evaluations in German hospitals. The dimensions were queried with single items on a seven-point Likert scale.
The participants (female = 44%) stayed an average of four days in a two-bed room. The patients and their roommates had a similar average age of 54 years. A total of 66% of patients underwent surgery during their stay. When asked whether they would use the hospital again and recommend it to others, 84% of the patients said that they would use the hospital again and 82% that they would recommend it to others. To evaluate the results, we used multiple linear regression analyses via SPSS 25. The age, gender, and time in hospital of the focal patient and the age of the fellow patient were included as control variables.
Results
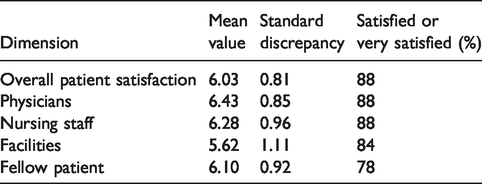
A comparison of the mean values shows that, as in other studies, the majority of patients were satisfied or even very satisfied. Very few patients indicated that they were dissatisfied with physicians, nursing staff, facilities, or fellow patients. A distribution of the mean values is shown in Table 1.
Mean value, standard discrepancy and percentage of satisfied and very satisfied patients.
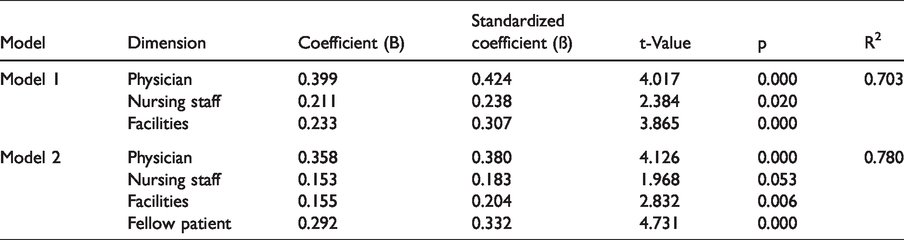
The analyses of the existing three-dimensional model (physicians, nursing staff, and facilities) showed an adjusted R2 of 70.3%. The influence of physicians (t = 4.017), nursing staff (t = 2.384), and facilities (t = 3.865) was found to be significant. Including the fellow patient in the measurement model led to an increase in variance of 7.7%, bringing the R2 to 78%. This change in value of the explained variance was significant. The new dimension (fellow patient) also had the highest significant influence on patient satisfaction (t = 4.731). H1 (a to d) and H2 are thus supported. After including the fellow patient in the model, every other dimension also had a significant influence (tphy = 4.126, tnurse = 1.968, tfac = 2.832). The control variables had no significant influence. The results are shown in Table 2.
Results of the linear regression “classical” model (model 1) and new model (model 2).
The results support the assumption that the fourth dimension improved the patient satisfaction model (see Table 2). Furthermore, the confirmed influence of the fellow patient in hospitals found in the study confirms Baker et al.’s theory. 16
Examination of the statements made to interviewers about patients satisfaction with the hospital shows that, despite predominant satisfaction, the patients also made negative statements. An overview of the responses to the open questions will be available upon request to the authors.
Discussion
The study shows that the fellow patient represents a relevant measure of patient satisfaction. In addition to the other known dimensions, such as physicians, nurses, and facilities, the fellow patient exerts an influence. The calculation of the satisfaction model by regression showed that all four dimensions have a positive effect on patient satisfaction. The separate measurement of the “classical” model and the “new” model clarifies that the addition of the fellow patient reveals further variance in patient satisfaction, and the change in R2 is significant. Therefore, it can be concluded that the fellow patient dimension should be added to future patient satisfaction models because they have a significant influence on patient satisfaction and, additionally, explain further variance. These results are supported by the study of Kulik et al., who found that the presence of other patients in a hospital room can increase satisfaction with care. 26 Additionally, the results are in line with past qualitative studies showing that the fellow patient in a shared room impacts the focal patient. 23
In addition, Baker et al.’s theory was transferred to and confirmed in the health care setting. 16 This theory also provides an explanatory approach as to why the fellow patient exerts an influence. Along with physicians and nursing staff, the fellow patient represents a personal influence—an influence that is, in fact, continuous, omnipresent, and interactive due to both patients’ presence in one room. The patient can hardly escape this influence because opportunities to move around are often very limited due to the hospital setting, and to disease. Therefore, the study also reveals that the influence of the fellow patient on the focal patient is very high. The different calculations of the model made it clear that the fellow patient enlightens variance. Thus, the addition of the fellow patient dimension improves the model and demonstrates a new approach to explaining patient evaluations of hospitals.
In addition to the hypothesis test, the other results show that the patients are predominantly satisfied with the hospital as a whole, as well as across all dimensions. This confirms the results of previous studies that patients have a very positive view of health services. However, the qualitative survey also shows that there are problems, despite overall satisfaction. The positive and negative statements were nearly in balance. This illustrates that it is difficult for patients to evaluate health services in detail, even if patients are increasingly confident and enlightened about these services. These problems were also demonstrated in the study of Simone et al., which criticized the previous satisfaction measurement as not sufficient to survey health services, noting that patients often only express satisfaction and do not describe their needs and problems. 29
Several limitations in this study should be acknowledged. The study asked patients about their satisfaction on the last day of their stay in hospital. It could be that the patients had not experienced all environmental influences at that time and would have provided different answers if the interview had taken place later. Furthermore, the interviews took place in the hospital. Although there were no staff or other patients in the same room during the interview, the patients may have perceived pressure or influence from the presence of staff or fellow patients nearby, or anxiety about receiving poorer treatment for “saying something wrong,” or been disproportionately grateful for the help and treatment received. These factors could have led to higher evaluations, and the results may have been different if the interviews had not taken place in the hospital.
Moreover, the patients in the study may have found it difficult to evaluate the global items for each dimension. Patients do not see all hospital procedures and are unable to make judgments about their implementation. Today, patients have the right to participate in decision making in health services, but in a hospital, this participation cannot be as high as in other services. There is, thus, a limitation to patient co-creation.
In previous studies, there has been some controversy about the usage of single versus multi-item measurements. 30 However, the most appropriate approach really depends on the context. Thus, researchers should consider their main research goals and then decide whether to use a single- or multi-item measurement approach. Lastly, the study concentrated on the fellow patient in the shared room and on patients in the fracture clinic. Influences could also be felt from other patients at the station.
In this study, it was shown that the patients are predominantly satisfied or even very satisfied. However, the qualitative statements partly show a different picture. This clarifies the fundamental questions whether it is sufficient to ask patients only about their satisfaction, 30 or whether further questions would have to follow, in order to raise the “true” satisfaction.
The results of this study require further review. Follow-up studies should consider the fellow patient as an influencing factor in patient satisfaction. The correlation should also be examined on other wards and for various diseases. The fact that the fellow patient is important in general units, and also in short interactions, confirms that more research is needed on the other customer in health care. This study makes a first contribution to this field in hospitals. In addition, the influence of the fellow patient could be investigated within other types of health facilities, such as rehabilitation clinics and nursing homes. In these cases, an in-care orientation provides higher patient contact than hospitals do, and more interactions could affect patients and their evaluation of services. Another area that could be investigated in more detail is why the fellow patient has such a large impact on patients’ evaluations. Kulik et al. revealed that postoperative patients can decrease the anxiety of preoperative patients. 25 It may be that a similar effect also influences patients’ satisfaction with a hospital. Furthermore, qualitative and quantitative studies have indicated that fellow patients are perceived as supportive, and that this influences the focal patient’s feelings, behaviors, and satisfaction with the hospital.1,24 Further research could examine whether an indirect effect on patient satisfaction exists, and whether there are moderators that affect the impact of the fellow patient.
In summary, satisfaction models can be improved via the addition of the further dimension of the fellow patient, thus producing a more detailed and precise measurement.
Implications for hospital management
As the study showed that the fellow patient has a significant influence on patient satisfaction, hospitals should use the fellow patient as a resource. Thus, units should provide additional opportunities and space for patients to meet each other. To reduce feelings of anxiety and discomfort, the hospital could use ambient and design factors to make it easier for patients to get along with each other. Architecture and equipment could help to create a private space in the room and also provide places in which patients can interact. 14 Since the study showed that the fellow patient has a significant influence on patient satisfaction, the fellow patient should be included in satisfaction measurement models. In addition, hospitals should use the fellow patient as a resource, as this can significantly increase patient satisfaction. Thus, units should provide additional opportunities and space for patients to meet each other. To reduce feelings of anxiety and discomfort, the hospital could use ambient and design factors to make it easier for patients to get along with each other.
To date, hospital management has only considered similar ages and diseases with respect to room management. 20 Our study’s patient information suggests that it is more than similar age that supports and drives patient–patient interaction. This should be the focus of future research, but hospital management and ward staff can also find out through discussions what creates a good room atmosphere. Creating a good atmosphere in a hospital room and enabling positive patient–patient interaction could also help to aid nurses’ and physicians’ work so they can concentrate on care giving and treatment. In addition to increasing satisfaction, fellow patients could support the treatment or recovery of focal patients. However, this can only be possible if the fellow patient feels healthy enough to face the situation, if the staff allow the fellow patient to support the treatment, and if the staff show the fellow patient how to help. These positive effects can influence treatment and may speed up the patient’s recovery. In addition, the positive effect on patient satisfaction will have other positive impacts, such as improving compliance or self-rated health. Ultimately, the hospital can then reduce costs because compliance and high self-rated health could make patients stay healthy for longer and overcome their illnesses more quickly, equating to shorter stays.
In order to integrate the fellow patient into organizational processes, quality managers should create guidelines to help hospital staff to identify a good or bad room atmosphere. This should include recommendations supporting patients’ interaction in shared rooms. However, further research is needed to obtain more information about the opportunities for employees to affect fellow patient interaction and patient satisfaction.
Alongside the study’s practical implications, it is important to expand the theoretical findings by including the fellow patient in future models of patient satisfaction. To date, patient satisfaction models have considered the influence of physicians, nursing staff, and facilities. However, our study supports the argument for involving the fellow patient in research in health services in order, eventually, to increase patient satisfaction with the hospital. Based on this study, patient management moves further into focus, and fellow patients might be used as a supportive resource.
Academics have highlighted a lack of research on the influence of the other customer in services. 7 This has been particularly noted in relation to health services. 7 Patients are shaped by the impact of others, and, more importantly, fellow patients are the contact persons patients spend most of their time with during their hospital stay.21,23 Our study represents a first step towards a new patient satisfaction measurement that considers the influence of the fellow patient.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.