
Abstract
Employees are a very important source of innovation and essential for the generation, dissemination and implementation of these ideas throughout the organization. This is especially relevant when considering innovation in services during service (co-) creation such as within the healthcare sector. However, perceived employee involvement in innovation (EII) and between stakeholder group interactions in hospitals has not yet been studied in detail. This paper addresses the following research questions: “How do different employee groups perceive their involvement in the innovation process in hospitals and how do their actual involvement levels differ?” and (2) “How do different employee groups perceive their interaction with other employee groups in the innovation process and how do their actual interactions differ?” We analyzed a single typical German research hospital and conducted episodic interviews with employees representing different staff groups. We revealed that while all groups of employees are involved in innovation activities, perception of their involvement in innovation activities differs widely. There is a gap between perception and actual involvement particularly for lower level employees such as nurses. Further, their interaction differs among employee groups and innovation takes place in-group, rather than through group interaction. With our paper, we add to the understanding of perceived EII in hospitals and discuss measures for hospital management to increase EII.
Introduction
The German healthcare system and its hospitals have undergone diverse reforms in the last 20 years. While cost containment has been improved, hospitals still struggle to meet the demands of patients, payers, and other stakeholders. Recent developments show changing customer or patient needs and demand for a more patient-centered and value-based approach to healthcare. 1 Hospitals, as complex service organizations, engage various stakeholder groups and need to ensure their viability in a consolidating market while delivering the highest treatment quality within tight economic constraints and an institutionalized, bureaucratic environment. Thus, next to policy initiatives and reforms, innovation and a reputation for being innovative become more important for hospitals to cope with future challenges. 2
It is widely accepted that employees are a very important group for innovation and value co-creation in a multi-stakeholder service environment.3–5 Thus, the topic of employee involvement in innovation (EII) has been extensively studied in the literature,6,7 and practices to foster innovative behavior amongst employees along the innovation process have been adopted across different organizations.
However, current observations on EII in healthcare stem predominantly from medical technology and pharmaceutical companies. 8 There have been continuous calls for research on the topic at the hospital level. 9 So far, few papers are concerned with the different stakeholder groups involved in innovation in hospitals and their interaction. 10 Their focus lies on specialized groups such as nurses, 11 physicians 12 or on specific innovation activities (IA) such as R&D 13 and the implementation of medical innovations. 14 To our knowledge, perceived involvement in innovation processes has not been studied extensively in the healthcare sector despite its importance for healthcare organizations.6,15,16 This poses an apparent gap in current research. The aim of our study is to analyze IA in hospitals through the lense of perception of involvement and to better understand how stakeholders within hospitals interact when it comes to IA. Thus, this paper adds to the understanding of the topic by answering the following research questions: (1) “How do different employee groups perceive their involvement in the innovation process in hospitals and how do their actual involvement levels differ?” and (2) “How do different employee groups perceive their interaction with other employee groups in the innovation process and how do their actual interactions differ?”
We conducted an in-depth case study of a typical German research hospital on perception of EII and interaction in the innovation process. We add to the literature on EII in hospitals in the following respects: (a) we highlight the importance of perceived involvement of employees in IA in hospitals and confirm self-determination theory for this setting; (b) we show a gap between perceived and actual involvement and interaction for different stakeholder groups within a hospital department and offer potential reasons why this may be the case; and (c) we derive suggestions for hospital management to foster innovative behavior among employees. Our case study design using episodic interviews can also provide a typical example for further analysis of perceived vs. actual involvement in innovation activities.
Employee involvement in innovation activities
Involving employees in innovation has a long tradition 17 culminating in the foundation of the human resources management perspective as well as the participative or so called high involvement perspective. 17 Employee involvement has been defined as “the participation of the entire firm’s workforce to improve the working environment, product quality, equipment productivity, and eventually, company competitiveness” 18 and is naturally linked to innovation, as companies aim to harness employee ideas to gain a competitive advantage. 19 Innovations in this sense are “qualitatively new products, services or processes that differ significantly […] from what existed before” 20 and can be classified according to their impact into incremental and radical innovations. 21 EII has received significant attention amongst researchers, which lead to a vast literature base drawing on social, behavioral as well as management sciences.4,17,19,22–25 The success of EII involves an interplay of behavioral and psychological factors such as personality traits of employees, creativity and motivational factors, influence of management and colleagues, but also organizational factors such as participatory management, organizational practices, organizational climate and culture as well as organizational learning.19,25,17 Parts of EII are routed in self-determination theory and research shows that employees realize innovation opportunities best when they thrive as a means of being willing (psychological factors and individuals’ perceptions) and able (organizational factors) to engage in innovation activities. 23 Thus, an employees’ perception of being involved in innovation activities impacts their willingness to innovate 16 and in turn influences innovation output,15,23 which eventually has an impact on business performance.26,a Research 30 has also shown, however, that there is often an “involvement gap” between different groups of employees. Investigating an individual’s perception of involvement in IA and comparing it to the actual involvement and to the involvement of other staff groups can therefore provide relevant insights into how IA are carried out and how organizations can best harness the skills all employees.
More recently, EII has gained traction in the services innovation literature with employees acting as value co-creators within the service delivery process. With close proximity to the customer, employees can provide in-depth insights on customer needs and opportunities for new services generation 31 and such are able to identify customer needs and ways to optimize service delivery. Thus, EII provides significant opportunities for innovation in service-intensive environments such as hospitals.
The main objective of a hospital is to provide medical treatment for patients. However, hospitals are also part of the health innovation system and play an integral role in generating, adopting and reproducing medical knowledge. 9 They are connecting knowledge domains and sources, bridging different modes of learning and connecting healthcare systems along the stages of the innovation process. 9 As such, they play an important role for innovation. Hospital departments are often function-oriented and operate in a silo-mentality, coordination is done based on hierarchy and the culture is frequently described as traditional and physician-centered. 32
Applications of the research base on (perceived) EII to the specific case “hospital,” are increasing, but still rare and hospitals are often seen as a “black box.” 9 Notable examples of research on the topic include: Djellal and Gallouj 33 deriving a framework for analyzing hospital innovation output, Salge and Vera 34 focusing on the link between hospital innovation and hospital performance, Benzer et al. 35 focusing on innovation and organizational change in hospitals, or Cucciniello et al. 36 describing a health innovation implementation process. Existing literature on EII in healthcare rarely covers all employee groups, their perceived involvement in activities or their perceived interaction with one another (with the exception of Ciasullo and Cosimato 10 ), but rather focuses on physicians or nurses only.11,12,37
As EII occurs through interaction of various groups, especially in a multi-stakeholder setting, we argue that the innovative potential of employees in hospitals has not been fully analyzed in the literature yet. Additionally, Thune and Mina 9 suggest that the organizational capacity of hospitals and their employees to produce innovation is currently underemphasized in research. This is surprising as it is of high practical relevance of innovation for high-quality provision of medical services at reasonable cost.
Research design
We conducted a qualitative single case study in order to get an in-depth understanding of the process and interactions under study. 38 The sampling was theoretical and purposive. We found a typical German university-linked research hospital, b which can be contrasted with extreme cases, both positive and negative, in future research projects. After an initial literature review, we derived two research questions and a guideline for semi-structured interviews. We performed episodic interviews in order to better understand EII and interactions within the innovation process. Episodic interviews focus on meaningful experiences in relation to the interview topic and are used to recount change, routines and situations in everyday life of the interviewee. This is facilitated by asking the interviewee to tell a story about situations that are good examples for the topic at hand 38 . Episodic interviews are particularly useful for group comparisons and the analysis of social constructs, 38 which makes them the method of choice for the research questions at hand. We thus combined the benefits of a semi-structured approach with the depth of information of a narrative, while also triangulating different approaches of data collection. 38
We prepared a list of stakeholder groups necessary to construct the case. These include physicians, nurses, functional diagnostic staff, IT administration, medical technology management, laboratory staff, pharmacologists, central services, administrative staff, the medical director of a department and the economic director of a department. We contacted the head of a clinic department to discuss the project and to obtain ethical consent. We were provided with initial points of contact for the stakeholders on the list and the head of the clinic department sent a letter to the respective parties. Afterwards, we contacted the potential partners for interview appointments.
Overall, we conducted 11 interviews, which lasted between 30 and 60 minutes. An overview of the interviewees can be found in Table 1:
Overview of interview partners.

The interviews were conducted in German during a personal meeting or through a phone call. Following the interview, the researchers’ perception of the interview process was documented in a research note and the interviews were transcribed.
All data was imported into MAXQDA and coded. The coding followed a qualitative content analysis procedure with deductive category application. 40 Involvement was coded based on Shadur et al. 15 Main and subcategories for involvement and interaction levels, stakeholder groups and steps of the innovation process were defined. The deductive categories were “perceived involvement,” “actual involvement,” “perceived interaction” and “actual interaction.” We derived the subcategories of “no (perceived) involvement,” “low (perceived) involvement” and “high (perceived) involvement” based on the employee involvement continuum as presented by Shapiro.30,c We define perceived involvement as the subjective conviction of involvement and actual involvement as the situational involvement in IA. c We further coded for hierarchy level (“employees,” “middle management,” “upper management”), process step (“idea generation,” “idea selection,” “design,” “testing” and “implementation”) and stakeholder group. The definitions, examples and coding rules were collected in a coding agenda and coding was done independently by two authors. The coding agenda was revised before final coding of the material and interpretation of the results. Comparing the results of final coding lead to a Cohens Kappa κ = 0.88, indicating strong interrater agreement. 42 The base questionnaire for the semi-structured interviews can be found in Appendix 1, an excerpt of the coding agenda can be found in Appendix 2.
Results
(Perceived) Involvement in innovation activities
All respondents agreed on the importance of innovation and stated that they were motivated to try new things. A nurse said “I am open for everything, so if someone has a new idea that provides a benefit, I am very happy to look at it. I would never say ‘This does not make sense, leave it as it is’ right from the start.” e Overall, staff at employee level tends to be more involved in incremental innovation, while staff at management level is more involved in radical innovation. While all groups of employees are involved in the innovation process to a certain extent, the perception of their involvement in IA differs immensely between employee groups and between hierarchy levels (Figure 1).
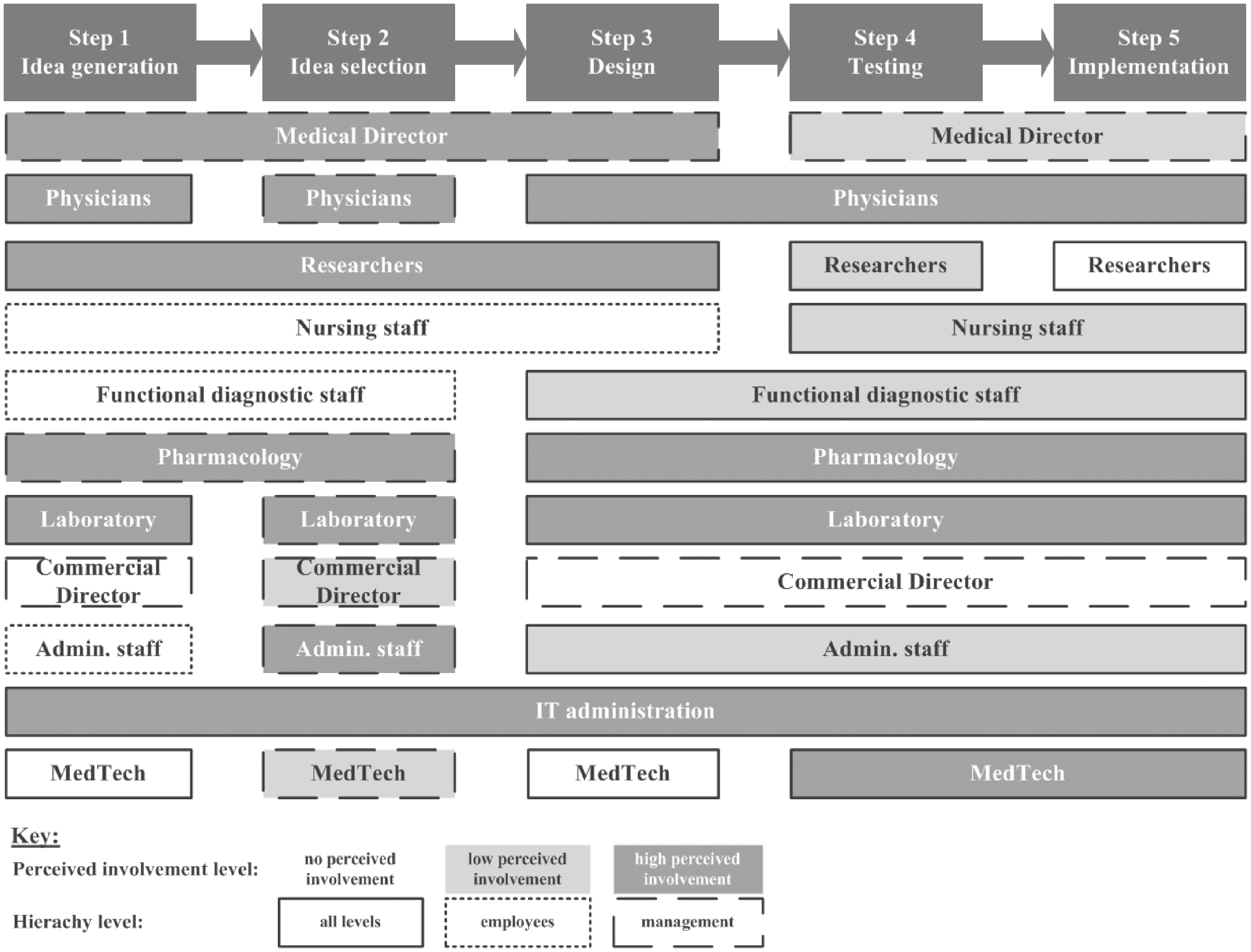
Overview of perceived involvement in innovation activities based on interview results.
Physicians reported high involvement levels, such as “as chief resident I am critically involved [in IA],” while another physician described optimizing the patient management process in an outpatient clinic and further stated multiple joint research projects that he takes part in. Other groups with a perception of high involvement include researchers, pharmacology staff, laboratory staff as well as the IT department. On the other hand, nursing staff, functional diagnostic staff, the commercial director or members of the administrative staff seem to perceive only limited or no involvement in multiple phases. A nurse stated: “Especially such small things, where a nurse would be asked: ‘What would you improve?’ — that is not done often enough.”
High perceived EII is linked to a high position within the hierarchy. This was acknowledged by most participants, with an anesthesiologist stating: “I think this is because I am, let’s say, further up in the hierarchy, so that if I have a good idea, I know who I need [to pursue it] and which network I have to create by myself to implement it.” The Head of Pharmacology stated “100 percent, this is my job,” while the Head of IT said that “We are always involved, because almost nothing works without IT support anymore.” The Head of Laboratory stated “[My involvement] is very high, which even leads to some suffering […] as a lot of innovation [means] a lot of change.” On the other hand, regular employees and even middle management, especially within the nursing and administrative departments recount no or only very little involvement without prompting. Nurses said: “I think, the lower you are in the hierarchy, the less you are involved and the less you are consulted.” and “We are generally not involved in the idea process.” Interestingly, when prompted about specific IA such as talking about potential process improvements with colleagues, taking part in training on innovative technology or taking part in research projects, even participants who had previously stated no involvement were able to recount an episode from their daily work that showcased at least low levels of involvement. A nurse said in this regard “Those were not really my ideas, but rather suggestions how we can transfer processes from others, that are more modern, to our department.” Some even exhibited high involvement e.g. within research projects such as a nurse working directly on project to improve oral care. She stated “[A doctor] was very engaged and worked with me, because I [work with] the patient group.”
Finally, as portrayed in Figure 1, perceived involvement levels also differ along phases of the innovation process. While the IT and the laboratory departments recount high perceived levels of involvement throughout the whole process, other department stakeholders perceive their involvement being tied to certain phases of the process. The department for medical technology reported to be mainly involved in testing and implementation of innovation, with the Head of the department saying “We are integrated in the process. Certainly not in the primary phase, but rather in the secondary phase” and “Yes, we are involved, but the idea does not come from us.” The administrative staff perceived their involvement to mainly happen within the idea selection stage by contributing through e.g. cost-benefit analyses or market analyses, with a respondent stating “We do a cost-benefit analysis, calculate the cases, the profits, the costs.” Interestingly, an upper management level anesthesiologist reported that “[Within the administrative staff] there are a lot of people, whose main goal is not to innovate, best case they tolerate it.” Nurses and lower level administrative staff perceive no involvement in the early stages of the innovation process, even though they are able to recount episodes that clearly point to involvement, such as developing ideas and communicating them to their superiors.
Overall, staff perceiving high EII appears very active in their pursuit of implementation through forming networks of support or engaging with other stakeholders to push the desired project, leading to a positive influence on innovation output. Staff levels with no or very low levels of perceived EII frequently reported obstacles to innovation, often linked to the phase of idea generation and idea selection. A nurse said “We have this suggestion system. But I have never used it, because I do not know what happens to my idea.” They often report a lack of motivation to participate in IA due to a high workload, a lack of time, no or negative feedback in the past or lack of management support. This in turn negatively impacts innovation output as innovative ideas may not be expressed or pursued.
(Perceived) Interaction between stakeholder groups along the innovation process
All respondents highlighted the importance of interaction and collaboration between the different employee groups to create and implement innovations. The Head of Pharmacology stated in that regard: “Without physicians, nurses and pharmacology [cooperating] you cannot succeed.”
Perceived interaction, however, differed widely amongst the stakeholder groups, hierarchy levels and phases of the innovation management process. The Head of Pharmacology underlined this by stating: “We are ahead when it comes to interdisciplinarity in medicine. However, this ends with the physician. If they [were to] start to take other groups more seriously, not just formally, but really seriously — but we are not there yet.” Physicians reported interactions with functional diagnostic staff and nursing staff, such as an anesthesiologist who stated “Chemists and physicians [working on the proposal], during implementation functional diagnostic staff will be involved” and when asked about another project: “Physicians and outpatient clinic staff. This is mainly nursing staff. [.] oh yes. And the IT department.” The medical technology department reported interactions with “Nursing staff for sure. The functional diagnostics staff, the pathology department and the laboratory department […] and the IT department of course.” This indicates high perceived interaction with a multitude of stakeholder groups. However, another physician stated: “Mainly with doctors […] not with nursing staff at all. Not in this aspect” and “Well, it is hard to get connected to the right people. Sometimes I feel like there is not a lot of cooperation within the university. And sometimes, there are colleagues that define themselves through dissociation. […] they just take an [idea for an] innovation opportunity from you and do it themselves, rather than cooperating.” The administrative staff reported low interaction levels with other groups, indicating that they mainly follow established feedback protocols, while the upper management of the administrative department mainly interacts with physicians, the IT department and external partners.
Respondents of the nursing staff mainly reported low levels of interactions (often one-off) and mainly with physicians. Interestingly, they attributed it to their standing in the hierarchy. A nurse stated “It is difficult, because [it is] such a hierarchically organized company with no intention of reducing hierarchies.” Another nurse recounted an episode of a task force: “I think [the medical director] was more of an autocratic decision maker. I do not know how far it could be considered an equal task force.” Interestingly, EII of nursing staff is sometimes overlooked by other stakeholders and hierarchy levels. An anesthesiologist stated: “I would not make a big fuss about it. If it comes to fine tuning and process improvement, of course we talk every day. No question. And for the recovery room […] we talked with the middle management nursing staff, because they are directly involved.” The Head of Laboratory recounted: “Well no. We have a lot of contact, but not about the topic [innovation]. Actually, we do interact with all stakeholder groups. If we talk about innovation in transporting samples, we talk with nursing staff, because they are more involved.”
Finally, perceived interaction differs along the stages of the innovation process. Idea generation often occurs within a stakeholder group rather than following a joint ideation process. A nurse said “I talked to my colleagues about [my idea] and they said ‘do it, it is a very good idea.” The Head of Medical Technology said “Firstly within my department and then, if there are friends from other departments, I may talk with them.” A notable exception is the pharmacology department as the Head mentioned a joint ideation effort together with physicians, IT and the Board in order to draft a proposal for an innovation fund. Several department heads mentioned cooperation with industry in the idea stage. Interestingly, collaboration and co-creation with patients as external partners was only mentioned by nursing staff. One nurse stated: “This was not a big idea we implemented, but rather the patients and their families demanded it and we complied with the request over time.” Interaction within the idea selection and innovation design stage depends on the type of innovation. With incremental innovation, there is usually within-group communication, often with undesired outcomes. A nurse reflected: “If you try to improve something for the ward, my ideas are always nipped in the bud or my ideas were not good enough.” For more radical innovations, the idea selection stage involves high levels of management interaction as projects often need to be approved by multiple department heads and the Board, sometimes leading to long delays of the process. A physician stated “There is an idea that was communicated to the Board, to the IT department, to external partners, to the health ministry […] everybody is excited, but nothing happens.” Interestingly, he also stated “Everybody is wary of the others. If you have a good idea, someone will just come and steal it. This culture inhibits fruitful interactions.” High levels of interaction are perceived in the testing and implementation stage. Physicians, nurses and functional diagnostics staff recount being involved in clinical trials or research projects, often with external partners such as industry or other research institutions. A nurse stated: “We treat patients according to clinical trial protocols.” The implementation of innovation is often linked to training and with that interaction with other stakeholder groups, with a nurse stating “I am trained on every new technology,” indicating an interaction with the medical technology and IT department staff.
Overall, staff with a perceived high involvement in innovation also tends to report high interaction levels with other stakeholders, even though idea generation is usually done within a certain stakeholder group.
Discussion and implications
Overall, we show that while all employees are involved in innovation activities, the perception of their involvement in differs largely amongst the groups. Our results show a gap between perception and actual involvement specifically for lower level employees such as nurses. They are less involved in IA and even if they are involved in IA, they perceive it as part of their job and not an innovative activity. Further, interaction differs among employee groups and innovation takes place in-group, rather than through group interaction.
Strict hierarchy levels, physician centricity and high workload limit EII of certain stakeholder groups in hospitals
EII differs amongst the different stakeholder groups of a hospital department. Employees in management positions are more likely to classify IA as innovations, while employees lower in the hierarchy, especially within nursing, functional diagnostics or administrative staff often see their activities as part of their jobs and not particularly innovative. This may be due to differences in the understanding on what innovation is based on education and socialization of the stakeholder group. Employees in management positions may receive specific training on innovation in their base education and may be more likely (or even mandated, such as physicians) to partake in continuing education programs. They may also be more personally inclined to view innovative projects as a way of fostering their career and improving their standing within their peer group. There may also be additional incentives such as extra compensation in relation to how much grant money was acquired. A change in compensation schemes taking contributions of lower level employees into account may increase participation in IA by this stakeholder group. Our results indicate that management level employees tend to employ a network outside the organization, which also makes them more prone to interacting with innovative solutions developed in different organizations. Respondents on all hierarchy levels mentioned that they see a need for cultural change and opening up the strict hierarchies and diverge from the physician-centricity still prevailing in the hospital culture. Next to a high workload and low levels of freedom for creativity, lower level employees often mentioned a lack of management support which is in line with O’Donoghue et al. 43 This observation is in line with the hierarchical and physician-centric structure of a research hospital. Wallace et al. 23 show that an employee involvement climate is essential for innovation and is most effective at lower organizational levels. Thus, providing middle management with the tools and skills to create and support innovation activities through a high involvement climate may not only improve innovation, but may also help cope with staff shortages and high workloads due to the increased effectiveness of the work done. With creating an employee involvement climate as a starting point, cultural change may provide a positive impact on the individual’s readiness for change and innovation and foster individual engagement. 35 Providing additional education for lower level employees on creativity and innovation may help bridge the gap in understanding what innovation is and alter the perception of involvement. Combining this with continuous digitalization of the hospital may lead to more democratization and decentralization of the innovation process and allow for more employee participation in all phases of the innovation management process. Our results suggest that lower level employees are often left out of early stages of the innovation process. This may be due to decisions on innovative ideas being undertaken by management and introduced through a top-down, rather than a bottom-up approach. Involving all stakeholders from the beginning of the project allows for incorporation of their needs and different perspectives and eases acceptance of the innovation during the implementation phase. Using this approach for the digital suggestion system in our case may have improved acceptance and use of the system. Since there is no transparency about the process, respondents prefer personal interaction within their network over submitting a suggestion into the system.
There is a significant gap between perceived involvement and actual involvement in innovation activities, which lowers employee motivation and inhibits innovation output
While it seems that all employees are contributing to IA, albeit to varying degrees, and within different stages of the innovation process, not all perceive their contribution as actual involvement. This is particularly the case for nursing, functional diagnostic or administrative staff — staff that directly interacts with the patient in front-line service provision. As stated above, this may be routed in personal factors such as willingness to try new things or motivation, but also the organizational environment in which IA are facilitated. A lack of education on innovation and creativity may also lead to a misclassification of activities as (not) innovative. (Middle) management belittling or discouraging obvious IA may lead to a reduced motivation for IA in general and thus a misperception of one’s own tasks. Further, IA performed by lower level employees focusing on incremental improvements of the workplace or fulfilling patient needs may seem insignificant and might often be overlooked when compared to the more radical innovations resulting out of e.g. a large cancer research project.
Given the importance of (service) co-creation in service intensive environments 4 this gap in perception suggests a lot of untapped potential for hospitals in their search for improving patient care and internal processes. By empowering (front-line) employees and helping them recognize that their actions are actively contributing to innovation and improvement, management could leverage this potential to provide more tailored and more efficient patient care. Concrete measures could include: training staff on the basics of idea creation and idea management, 44 providing a transparent suggestion and feedback system or facilitating systematic ideation workshops or think tanks, as suggested by a participant from the nursing staff. These think tanks should include participants from all stakeholder groups and emphasize an open culture, where hierarchy is not important and all participants are able to speak and interact freely without fear of negative repercussions. These measures would increase the perceived involvement, especially in the idea creation and idea selection phase, leading to more potentially fruitful ideas entering the innovation management process. The implementation of such measures, however, demands a move towards a more innovation-friendly, high employee involvement culture, especially at lower levels of the organization. Our results suggest that the perception of EII and the overall involvement of the peer group in the hospital have an impact on employees’ willingness to partake in IA. This is in line with findings change management research and findings from Amo 11 and Shadur 15 in a healthcare setting. When employees perceive that they are not involved in IA or that their ideas are not worth to even be discussed, such as mentioned e.g. by nursing staff, they often keep ideas to themselves or even try to interfere with ideas of others as indicated by physicians.
Pursuing an open innovation approach and increasing perceived hierarchy-independent interaction with internal and external stakeholder groups may increase innovation output
Our results show that between-group interaction is limited along the innovation process - notable exemptions being the joint ideation for large research projects at management level and some interaction within the implementation phase. Stakeholders seem to perform IA at peer level and rarely interact with staff outside the peer group or hierarchy level. This may be due to a lack of time routed in high workload, which was also indicated by our results with interviewees frequently mentioning a lack of human resources and time as inhibiting factors for innovation. Another reason may be the hierarchical nature of the hospital, and perceived mistrust amongst staff members and fear of ideas being “stolen” or projects being taken over by other departments, as reported by some interviewees. As internal supporting networks are very important for innovation, 7 this poses a clear barrier to successful IA. There is a need for organizational and cultural change. Recognizing and communicating the potential and importance of all groups regardless of their standing within the hierarchy for their contributions to the innovation process may be a first step management can undertake to employee empowerment. Furthermore, an investment in communication training could decrease the inhibitions of lower level employees to participate in the ideation phase and collaborate in other phases. Interestingly, while a lot of respondents report interactions with industry, other researchers or hospitals, only members of the nursing staff report interaction and co-creation with patients. However, research has shown that co-creation with users, especially within service environments, can lead to significant improvements. 1 Hence, management should consider implementing open innovation approaches such as joint ideation activities and frequently ask for ideas from front-line employees.
Overall, our data shows that there is untapped potential for innovative ideas within certain groups of hospital staff. Management may be particularly interested in the results of this study, as these ideas may have the potential to reduce costs and provide better patient care. It is important to know who perceives to be involved in the innovation process and who interacts with whom. Management should create a common understanding and awareness for all types of innovation by providing training for all staff groups on the importance of this topic and aim to increase the innovation awareness, involvement, interaction and output by the hospital staff in order to achieve the overarching goal of providing the best possible patient care. With our paper we shed light on innovation management in the “blackbox” hospital. 9 We further highlight the influence of perception of involvement in IA and confirm literature on self-determination theory in a hospital setting.
Limitations and opportunities for further research
We conducted a single exploratory case study; our findings are limited to a specific setting. The gathered data is subjective to the respondents and perceived and actual involvement and interaction are assessed using the same interview base. Unfortunately, we were not allowed to shadow our interview respondents, which would have allowed for a more objective assessment of real vs. perceived involvement. We aim to counter this by using episodic interviews and triangulating with publicly available sources. For further research, it would be interesting to conduct a multiple case study using the present case as a base case within a national setting. Measuring and comparing the innovation output of hospitals that are implementing EII initiatives before and after implementation may also lead to informative results for management. We explored EII in a large public research hospital. Contrasting privately owned hospitals may further add to the understanding of EII.
Conclusion
Employees are an important source of innovation, especially in multi-stakeholder service environments such as the healthcare sector. Perceived involvement in innovation activities leads to a higher motivation and engagement in those activities and should be fostered at company level. We analyzed a single typical German research hospital and conducted episodic interviews with employees representing different staff groups.
We revealed that while all groups of employees are involved in innovation activities, perception of their involvement in innovation activities differs widely. There is a gap between perception and actual involvement particularly for lower level employees such as nurses. They are less involved in IA and even if they are involved in IA, they perceive it as part of their job and not an innovative activity. Further, interaction differs among employee groups and innovation takes place in-group, rather than through group interaction. In order to achieve the best possible patient care, management should emphasize the importance of understanding innovation and enhancing participation in innovation activities through decreasing hierarchy, creating innovation awareness and foster cross-hierarchy and stakeholder group interaction within a hospital.
Supplemental Material
sj-pdf-1-hsm-10.1177_0951484820943600 - Supplemental material for Employee involvement in innovation activities in hospitals: How perception matters
Supplemental material, sj-pdf-1-hsm-10.1177_0951484820943600 for Employee involvement in innovation activities in hospitals: How perception matters by Julia Busch-Casler, Simone Haubner and Andreas Pinkwart in Health Services Management Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.