
Abstract
Background
Patient safety is an important aspect of quality of care. Physicians’ alignment with hospitals by means of financial integration may possibly help hospitals achieve their quality goals. Most research examines the effects of financial integration on financial performance. There is a need to understand whether financial integration has an effect on quality and safety.
Purpose
The aim of this study is to examine the association between hospital physician financial integration (employment, joint ventures, and ownership) and Adverse Incident Rate.
Findings
Contrary to our hypotheses, hospital physician financial integration does not influence AIR. Besides financial integration, hospitals need to have a high commitment towards quality and safety to influence a lower AIR.
Introduction
Patient safety is an important aspect of quality of care. 1 Patient safety has been defined as freedom from accidental injury or medical errors, 2 and its outcomes include complications, infections, deaths and adverse events that happen after medical treatments and surgeries. 2
The US Institute of Medicine (IOM) in its report ‘To Err is Human’ exposed medical errors as a leading cause of death in the US that resulted in approximately 98,000 deaths each year. 2 This report also indicated that the cost associated with medical errors is between $17 billion and $29 billion, making it a significant and costly healthcare expense. 2
According to IOM’s ‘Crossing the Quality Chasm’ report, one of the big challenges towards reducing medical errors and becoming a safer healthcare system is lack of ‘cooperation’ by clinicians and health care professionals. This report invokes a new breed of ‘citizenship’ by clinical professionals in work systems. 3 One potential mechanism to achieving collaboration from physicians is to financially integrate them with the hospital, for example, through employment, joint ventures, and ownership; this is also known as economic integration. 4 Literature suggests that congruence of goals between physicians and hospitals through economic integration is a way of improving clinical processes, quality of care and outcomes of care. 4 While studies in the past have examined the effects of financial integration on financial performance, hospital costs, clinical integration, and quality,5,6 there is a lack of studies that explore the effects of integration on patient safety. Therefore, this study aims to examine the relationship between financial integration of hospital and physicians and Adverse Incident Rate (AIR). This topic is of practical relevance as the U.S. healthcare system gradually shifts from a traditional model towards an integrated model of hospitals and physicians, in which providers are held accountable for achieving improvements in quality of care.
Background
Hospital–Physician financial integration
The traditional relationship between physicians and hospitals in the U.S. was such that physicians had independent relationships with hospitals, and regarded hospitals as work sites to provide patient care and do research, without much alignment of hospital-physician goals. 7 This relationship has evolved in recent times. Tremendous pressure to improve quality while keeping costs low led to an interdependent type of symbiotic relationship between hospitals and physicians where incentives are compatible and aligned. This relationship is also known as integration.
Integration is defined as the extent to which activities and functions are appropriately coordinated across units and is broadly classified into two types: non-economic, and economic. Of relevance to this study is economic integration, also known as financial integration. Financial integration is the extent to which physicians are economically related to the system, use its facilities and services, and actively participate in planning and management. 8 This collaboration may be of many forms including employment relationships with physicians, hospital ownership by physician groups, and joint ventures between hospitals and physicians. 8 Financial integration includes the alignment of incentives between hospital and physicians, and significant input by physicians in overall strategic decision-making. 9
Conceptual framework and hypotheses
Agency theory
This paper uses underpinnings of agency theory to assess the relationship between hospital physician financial integration and AIR. Agency theory, which has its foundation in financial economics literature, includes two entities, a principal and an agent. 10 A ‘principal’ is one who engages another person, an ‘agent’ to perform services on the principal’s behalf. In this process, some decision-making authority is devolved to the agent.10,11 In the U.S. hospital context, governing boards, who represent community’s issues and agendas are the ‘principals’. 12 Hospital governing boards assign certain tasks to management and medical staff, who represent ‘agents’, to serve the community. 12 Physicians are an integral part of management and medical staff in hospitals, regardless of their level of hierarchy, and thus they are surrogates for ‘agents’ within the framework of agency theory.
Agency theory has two prime tenets. First, agency theory assumes that the principals’ and agents’ interests may be incongruent because each party seeks to maximize their own welfare. 11 Several studies have looked at how interests of the principals and agents diverge. Second, information between the principal and agent is asymmetric, meaning agent has information that is not available to the principal. 13 Information asymmetry in the principal-agent relationship arises in situations when the agent has more specialized knowledge than the principals, regarding task performance. For instance, physicians may have a better knowledge about clinical tasks as compared to the governing board. 13
The above two tenets of agency theory give rise to the “agency” problem. The agency problem arises when desires or goals of the principals and agents conflict. 13 In the hospital case, board (principal) delegates the responsibility for patient safety to physicians (agents), and financial integration can facilitate the process of holding physicians accountable for patient safety. Hospital physician financial integration is an example of an attempt to encourage cooperative behavior among individuals with diverse interests.
We studied three strategies by which hospital physician financial integration can occur, thereby potentially alleviating the agency problems: 1) salaried employment as compared to contractual and other arrangements, 2) ownership of hospitals by physicians, and 3) financial integration through joint ventures. Our primary research question is- Are hospitals that use one or more of these hospital-physician financial integration strategies associated with lower AIR?
To examine the above question, we focus on the use of hospitalists and intensivists at U.S. hospitals. Hospitalists are specialists in inpatient medicine. They are responsible for managing the care of hospitalized patients in the same way that primary care physicians are responsible for managing the care of outpatients. 14 Intensivists are physicians that work in the intensive care environment. 15
Financial integration through employment
Physician employment is a form of financial/economic integration that includes physician salaried relationships with hospitals. 8 Employment economically ties physicians to the system, allowing them to use hospital facilities and participate more extensively in planning and management thereby promoting collaboration to achieve common objectives. 9 For example, studies have suggested that physicians’ employment, as a strategy, has the potential to contribute to hospitals’ objectives of improving quality. 16
Employed physicians who are a part of an integrated delivery system may be in a better position to provide collaborative and coordinated care that can potentially result in lower AIR. For instance, it is easier to set clinical priorities for physicians that are employed, and are more willing to provide emergency department coverage as compared to those who are not employed, because non-employed physicians seldom and unenthusiastically participate in hospital activities.
12
Specifically, employing hospitalists and intensivists has benefits that include reduced length of stay, reduced mortalities, ability to treat higher acuity, better resource use, and improved efficiency.12,16 A higher availability and participation of employed physicians in hospital activities can translate in better efficiency and lower AIR. Therefore, we suggest the following hypothesis: Hypothesis 1: Hospitals with a higher proportion of employed physicians will experience lower AIR as compared to other arrangements.
Financial integration through ownership
There has been a recent emergence and growth of physician ownership of hospitals, especially the ones that provide specialized treatments. 17 Direct ownership of hospitals is another way to integrate physicians into the hospital and includes either partial or full ownership. 17 Because physicians share financial risks associated with ownership, it is reasonable that there will be a greater integration of goals and objectives between physicians and hospitals including goals for quality and patient safety. 6 Studies have shown that, with ownership, both physicians and hospitals see the need to collaborate on service lines. In addition, through ownership, physicians have a focused set of clinical priorities, and respond to pay-for-performance incentives to improve safety and quality of care. 18
According to agency theory, information asymmetry in the principal-agent relationship is prominent when the principal lacks specialized knowledge that the agent has, which can be ameliorated with ownership as physicians become an integral part of the governing board.
11
Agency theory also confirms that goal conflicts are resolved through co-alignment of financial incentives. Agreement of hospitals and physicians on goals is especially critical on patient safety initiatives because such initiatives seek direction, guidance, and innovation from physicians.
18
Thus, we suggest the following hypothesis: Hypothesis 2: Hospital-physician financial integration through physician ownership of hospital is positively related to lower AIR.
Financial integration through physician joint ventures
Joint ventures refer to those ownership arrangements in which physicians own healthcare facilities to which they refer patients for services. 17 It is a stronger integration method (e.g., investment in medical office buildings, ambulatory centers, diagnostic imaging centers, service lines, and specialty hospitals) as compared to other weaker integration methods (e.g., renting facilities to physician groups).6,7 Approximately half of all hospitals that participate in Accountable Care Organizations go through joint ventures between physicians. 19 Empirical findings suggest that hospitals with joint ventures have shown progress in coordination of care across settings and safer transitions among care settings. 20
Joint ventures involve physicians in hospital governance, in terms of sharing common interests, resources, and meshing of hospital and physicians’ strategic objectives for quality goals, while bringing clinical perspective to board decisions.6,7 Furthermore, linking physicians with hospitals through joint ventures (clinical labs, ambulatory centers etc.) facilitates the coordination across the continuum of care and the provision of comprehensive care, which may reduce the probability of adverse events.
20
Thus, we hypothesize that: Hypothesis 3: Hospital physician financial integration through physician joint ventures is positively related to lower AIR.
Methods
Data and sample
This study includes panel data from 2013–2015. The sample contains all hospitals across the U.S. that provide acute care and are privately owned. Data for this study were obtained from the American Hospital Association (AHA) annual survey, U.S. Area Health Resource File (AHRF), and Centers for Medicare and Medicaid Services (CMS) Hospital Compare. The AHA data had the following hospital-year observations: 7,073 in 2013, 7,600 in 2014, and 7,107 in 2015. After merging with the AHRF and Hospital Compare data, we had 1,042 hospital year observation in 2013, 1,546 hospital -year observations in 2014, and 940 hospital-year observations in 2015. The final analytic sample had 3,528 hospital-year observations.
Variables
Dependent variables
CMS collects and reports data on AIR, or Patient Safety Indicators (PSIs), which are measures that screen for potential patient safety problems as a result of exposure to the healthcare system, and that could have been prevented at the system level. 21 Previous research has found that PSIs have sufficient validity for screening cases with a high likelihood of having quality of care problems. 21
For this study, we use the ‘Patient Safety and Adverse Events Composite’, PSI_ 90, a hospital-level composite measure or weighted average of a subset of PSIs as follows:
22
PSI 03 Pressure ulcer rate PSI 06 Iatrogenic pneumothorax rate PSI 08 In hospital fall with hip fracture rate PSI 09 Perioperative hemorrhage and hematoma rate PSI 10 Postoperative acute kidney injury rate PSI 11 Postoperative respiratory failure rate PSI 12 Perioperative pulmonary embolism or Deep Vein thrombosis rate PSI 13 Postoperative sepsis rate PSI 14 Postoperative wound dehiscence rate PSI 15 Unrecognized abdomino-pelvic accidental rate
Each PSI represents the rate per 1000 of at-risk individuals for the Medicare fee-for-service inpatient population. Weighting of indicators is based on the volume of adverse events and harm associated with adverse events. 23 Online Appendix A includes the numerator and denominator used in calculating each of the PSIs of the PSI 90 composite. The measure is a composite that captures the overall Adverse Incident Rate (AIR), higher AIR is an indication of worse patient safety outcomes.
Independent variables
Hospital-physician financial integration comprises measures of physician employment, physician ownership, and physician joint ventures from the AHA annual survey. Physician employment (hypothesis 1) consists of the ratios of hospitalists and intensivists employed by the hospitals as follows: [Total hospitalists (FTEs) employed/Total hospital inpatient days] *1000, and [Total intensivists (FTEs) employed/Total hospital inpatient days] *1000.
Control variables
Organizational characteristics of hospitals such as bed size, teaching status, system membership, ownership status, and staffing have been associated with lower mortality, adverse events, and lower AIR. 24 Proportion of Medicare and Medicaid patients’ accounts for patients’ severity of illness, and physicians who work as contractors with hospitals, may play a role in improving patient safety. The following organizational variables were used as control variables: 1) Ownership status- For profit, and Not-for profit, 2) System membership- Hospitals are considered system affiliated if they are members of a multi-hospital system, 3) Teaching status- Hospitals are considered to be teaching of they are either a member of the Council of Teaching Hospitals (COTH), or affiliated to a medical school, or provide residency training, 4) Bed size-measured as total number of inpatient beds. (Small = 0–99 beds, Medium = 100–299, Large = 300 and above), 5) Registered Nurse (RN) staffing ratio = (FTE RN/Total hospital inpatient days)*1000, 6) Proportion of Medicare patients and Medicaid patients:(Medicare inpatient days/Total inpatient days) *100, and (Medicaid inpatient days/Total inpatient days)*100, 7) Total contract hospitalists (Total hospitalists contracted/Total hospital inpatient days)*1000, and 8) Total contract intensivists (Total intensivists contracted/Total hospital inpatient days)*1000.
Geographic location, market competition and per capita income account for market characteristics that may influence hospitals’ policies regarding patient safety thus affecting AIR: 1) Geographic location- Metro, Urban, and Rural. Rural and Urban Continuum Codes (RUCC) were used to create the above categories. RUCC codes 1, 2, and 3 were included in the metro category, 4, 5, and 6 included in the urban category, and 7, 8 included in the rural category. A description of these codes has been given in online Appendix B. 2) Competition is measured by the Herfindahl-Hirschman Index (HHI) and consists of the sum of the square of the market shares for hospitals in the hospital service area (HSA). HHI values have a range between 0 and 1, with 1 representing monopolistic markets and values close to 0 indicating highly competitive markets, and 3) Per capita income represents the average income per person for the hospital county.
Analytical approach
Our dataset is a longitudinal (panel) data that is designed to investigate changes of inpatient AIR over time for each hospital. Given the relatively short study period, we did not expect large changes in the dependent and independent variables; therefore, a random effects (RE) regression model was chosen. The RE model assumes that variation across hospitals is random and not correlated with the independent variables included in the model. A Hausman test provided support for the use of a RE model. We also adjust for within-hospital variation or heteroscedasticity by calculating robust cluster standard errors. State and year fixed effects were included. Our regression model consists of: AIR (measured by PSI_90) it= β0+β1 phy_employment it +β2 phy_ownership it+ β3 joint_ventures it+β4 controls it + State i+ Year + Uit
Before running the random effects model, we conducted a pooled cross-sectional Ordinary Least Squares (OLS) regression model to assess if there was any significant relationship between AIR and financial integration because of the low within-hospital variability year by year for our independent variable. This was conducted to assess if no effects exists between AIR and financial integration or if our longitudinal data had insufficient variation to detect an effect.
Results
Table 1 presents descriptive statistics on all the variables included in the study. The AIR on average, was approximately 86 for all hospitals during 2013–2015. The average hospitalist employment in our sample was 0.4 FTE per 1000 inpatient days, a little higher than the average intensivist employment, which was 0.3 FTE per 1000 inpatient days. Approximately 4% of the hospitals were owned either in whole or in part by physician groups, and approximately 53% of the hospitals engaged in joint ventures with physicians or physician groups.
Descriptive characteristics of all variables in the sample (N = 3,528).
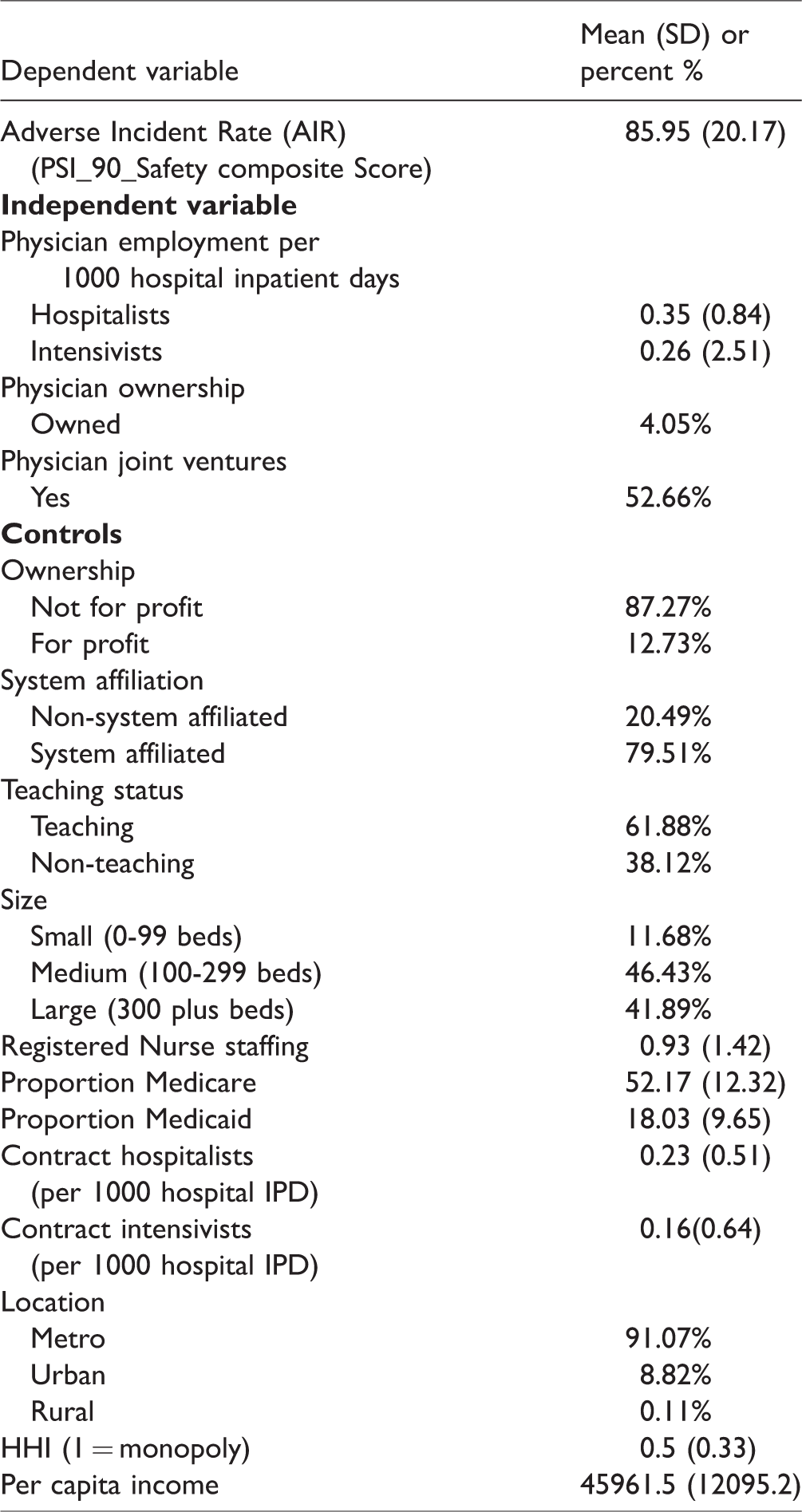
Among organizational characteristics, the majority of the hospitals were not-for profit (∼87%). Approximately 80% of the hospitals were a member of a system; and 62% had teaching status. The average RN staffing ratio was 0.9 RN FTE per 1000 inpatient days. Additionally, the proportion of Medicare patients was 52%, and the proportion of Medicaid patients was 18% in our sample. Among market characteristics, the majority of the hospitals in our sample were located in a metro area (∼91%). Furthermore, hospitals in our sample were predominately medium (46%) and large (42%) in size. Finally, the average score for market competition measured by the Herfindahl-Hirschman Index was 0.5, which indicates that hospitals in our study tend to be in more monopolistic markets with a mean per capita income of about $45,961.
Table 2 presents results of the pooled cross-sectional OLS regression between AIR and measures of financial integration. We conducted the OLS to account for year to year low variations in the financial integration measures. We found no association between the above two variables.
Multiple linear regression (OLS) results of the relationship between hospital physician financial integration and adverse incident rate (N = 3,528).

Table 3 presents results from random effects model. Hospitalist employment, physician group ownership, and physician joint ventures showed no statistically significant relationship with AIR. Therefore, our hypotheses H1, H2, and H3 were not supported.
Multiple linear regression results with random effects of the relationship between hospital physician financial integration and AIR (N = 3,528).
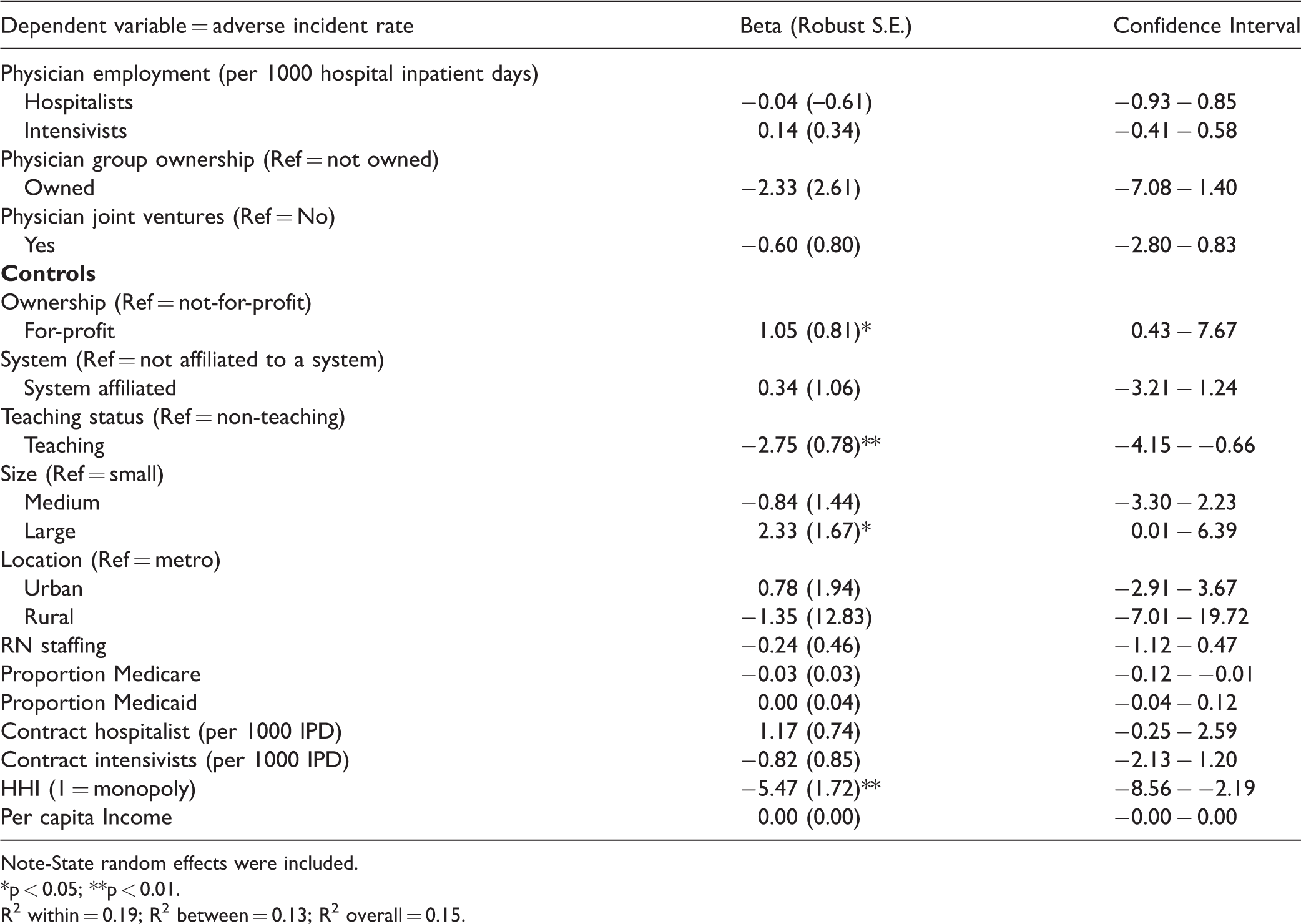
Note-State random effects were included.
*p < 0.05; **p < 0.01.
R2 within = 0.19; R2 between = 0.13; R2 overall = 0.15.
For-profit hospitals (β = 1.05, p < 0.05) compared to not-for-profit, and large (β = 2.33, p < 0.05) as compared to small hospitals, had a statistically significant higher AIR. On the other hand, hospitals that were teaching (β = −2.75, p < 0.01), were associated with a statistically significant lower AIR. Contrarily, hospitals located in more competitive markets (β = −5.47, p < 0.01) were associated with higher AIR.
Discussion
This study tested a model, based on agency theory, which examined the effect of hospital physician financial integration through employment, ownership, and joint ventures on AIR. Contrary to what we hypothesized, hospital physician financial integration does not influence AIR. This suggests that financial integration between hospitals and physicians, by itself, may not be sufficient to influence AIR. In addition to the financial strategies examined in this study, hospitals need to have a high commitment towards quality and safety to have lower AIR. Resource adequacy, physician involvement, and a positive nursing work environment may be needed to supplement financial integration’s effect towards patient safety improvement. Other strategies may include having good collegial physician nurse relations, adequate nurse staffing and a competent nursing leadership to create a conducive work environment for nurses to achieve a reduction in patient safety errors. Consistent with our study, other studies have found that despite a higher number of physicians, an organizational environment needs to be fostered for the implementation of evidence-based practices, where physicians are prepared to solve problems. 25
Even though we expect that with employment, a higher availability of physicians would translate to lower AIR; their objectives may not be in congruence with those of the hospital. Researchers have found that physician employment does not have a relationship with better patient care and a higher intensivist staffing is not related with improvement in outcomes such as mortality rates. 25 Consistent with prior studies, our study found no relationship between hospital employment and AIR. Prior studies only considered employment as a form of integration, 25 however we used a comprehensive construct that includes employment, ownership, and joint ventures. Nevertheless, our finding remained consistent with prior research that shows no relationship between financial integration and AIR. 25
In our study, the average intensivists staffing was only 0.3 per thousand hospital inpatient days, which may not be large enough to influence AIR. Besides having a higher number of employed hospitalists, it is imperative that hospitalists are motivated and collaborate to pay attention to the content, format and timely delivery of clinical information to avoid losing important information that may cause patient safety errors. 26
Hospital physician financial integration such as ownership and joint ventures align priorities between hospitals and physicians, where physicians bring clinical knowledge to decisions made by the governing board thereby removing goal conflicts. However, ownership of hospitals by physicians and physician groups has concerned hospital managers about added requirements from the governance. In addition, it has also concerned patients about referral restrictions to other hospitals. 18 While it is true that involvement of physicians in the hospital governance brings critical perspective to board decisions, simply bringing clinical guidance to board decisions may not necessarily mean that quality of care is being affected.
Our analyses found several significant relationships between certain organizational characteristics such as ownership, teaching status, and size with AIR. For-profit hospitals had higher AIR than non-profit hospitals. Our finding is consistent with results from previous studies that compared the quality of care at both for-profit and not-for-profit hospitals and found that for-profit hospitals were associated with lower quality (higher AIR) when compared across markets. 27 For-profit or investor-owned hospitals are required to pay taxes, their employees tend to have higher salaries and bonuses, and their shareholders expect return on their investments. 27 For these reasons, such hospitals may have an incentive to minimize expenses, potentially resulting in inadequate staffing and therefore lower quality and safety.
Our subsequent finding about teaching hospitals being associated with lower AIR is corroborated by the fact that teaching hospitals provide graduate medical education, and residents provide much of direct patient care. Such hospitals have an academic culture in which residents need to be certified as being proficient in performing a number of procedures. 28 Teaching hospitals also provide residents with workshops and training to improve their competence in performing procedures. 28 Our findings are reflective of a positive patient safety environment that engages residents in patient safety activities at academic medical centers.
Finally, large hospitals had higher AIR, which may be due to a large volume of patients with a wide variation in case mixes, that necessitates a range of complicated procedures, opening up possibilities of lower quality and patient safety. Future studies can evaluate an in depth understanding of the rationale behind large hospitals having higher AIR.
Our findings show that a higher market competition is related with higher AIR, which are consistent with prior research that have shown that a higher market competition is related with higher mortality rates. 29 However, other studies concerning competition in healthcare markets and its impact on quality have shown that competition increases quality of healthcare. 30 Higher competition may result in higher AIR (worse safety outcomes) because hospitals in more competitive markets may focus on aspects that are observed and visible to patients and attract physician referrals, for example, investment in high technological capabilities and reduction in patient wait times. However, it may take away resources that are needed for improvement in patient safety.
This study has some limitations. We used secondary data sources to measure hospitalist and intensivist employment, as well as AIR, which may sometimes be incomplete or available only for some years. This may cause issues of generalizability because the study population represents only those hospitals that have provided patient safety outcome data. In addition, the PSI 90 may not be a comprehensive measure that includes all the AIRs. Future studies can explore other staffing data and use longer study periods that would help draw more complete conclusions about associations examined in this study. Additionally, using data on other AIRs besides CMS’ PSI data, would shed more light on the research questions answered in this study. Finally, studies in the future should control for average DRG case mix in the data analysis.
For hospital managers, a take away from this study is that even though hospital physician integration can help increase the number and availability of physicians, it may not have far reaching distal effects on improving AIR. Besides integrating physicians into hospitals, organizations should consider increasing their commitment towards quality and safety. An organizational culture of patient safety can possibly be nurtured and fostered through physicians’ involvement in hospitals’ patient safety priorities. Healthcare quality and safety is an important issue that calls the attention of researchers, policymakers, and administrators in the years to come. Our study uncovers a gap that hospitals need to fill if they integrate physicians into hospitals with the goal of improving patient safety.
Supplemental Material
sj-pdf-1-hsm-10.1177_0951484820948647 - Supplemental material for The effects of hospital-physician financial integration on adverse incident rate: An agency theory perspective
Supplemental material, sj-pdf-1-hsm-10.1177_0951484820948647 for The effects of hospital-physician financial integration on adverse incident rate: An agency theory perspective by Soumya Upadhyay, Robert Weech-Maldonado and William Opoku-Agyeman in Health Services Management Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.