
Abstract
Introduction
Appropriateness is an essential element of quality of care. Several methods and tools have been developed to measure the appropriateness of care, however, none of these could be used to systematically support providers in keeping the appropriateness under control. Our study aimed to develop a framework to evaluate the appropriateness of care that took into account four dimensions of appropriateness: clinical dimension, equity, service delivery model, outcome.
Methods
We employed mixed-method approaches. These included a retrospective analysis of administrative data collected from Kinetika Sardinia (Italy) and a qualitative analysis of stakeholders’ experiences and perspectives aimed at supporting data collection, identification of improvement actions and definition of performance indicators. We used arthrodesis as a paradigmatic example of potentially inappropriate elective surgery.
Results
We collected data from 2,584 patients that underwent arthrodesis between January 1, 2010 and April 30, 2015. Based on the analysis and the exchanges with professionals, we identified 11 improvement actions. Monitoring and evaluation actions were finally conducted for 171 patients that underwent spinal fusion during the first semester of 2016 in order to assess if the improvement actions identified were put into practice and acquired desirable outcomes.
Conclusions
Our work provides a definition of appropriateness that goes beyond the clinical perspective and includes other perspectives (equity, service delivery and outcome); develops a framework and an approach that can be a valid help to systematically assess the appropriateness of elective surgery, adopt improvement actions, and monitor their impact; discusses what are the competencies necessary for measuring the appropriateness.
Keywords
Background
Healthcare systems face significant and rapid changes in response to changes in population needs, increasing costs 1 , 2 and advances in surgical technology. Some studies estimate that a large proportion of the healthcare offered is inappropriate or unnecessary, ranging from 15 to 30 percent in many countries and as much as 40 percent in some private clinics. 3 , 4 Worldwide every year millions of patients go under knife, but many of them are enduring great pain and shelling out huge amount of money for surgeries they don’t really need. 5 According to a review of in-depth studies and data generated by both government and academic sources, unnecessary surgeries might account for 10 to 20 percent5–7 including a wide range of cardiac procedures — not only stents, but also angioplasty and pacemaker implants — knee replacements, hysterectomies, 8 caesarean sections, 9 as well as many spinal surgeries.
These findings have led to calls for measures of appropriateness to be used by purchasers and other actors to regulate or influence the delivery of surgery and assess when surgical and medical procedures are “appropriate.” But what does “appropriate” mean? And what are the methods and tools that health care organizations can employ to measure and manage the appropriateness of care?
First of all, appropriateness is a recognized element of health care system performance 10 and an important element of high quality of care delivery alongside with other universally accepted core dimensions of quality of care such as effectiveness, patient safety and responsiveness/patient centeredness. 11 Although the recognition of the appropriateness as a key element of quality of care, and many efforts made by researchers and policy makers to conceptualize and measure the appropriateness both prospectively through the development of evidence-based guidelines 12 and retrospectively by assessing guideline adherence for specific conditions, 13 the perception is that appropriateness remains a patchwork concept with no uniform scope or meaning. 14 Traditionally, the concept of appropriate care has been linked to the clinical perspective and is more concerned with the prevailing view within health care professions as to those interventions that most contribute to health gain. In this context, appropriate means that “the expected health benefit exceeds the expected negative consequences by a sufficiently wide margin that the procedure is worth doing.” 15
However, there is a wider consensus that other dimensions should be taken into consideration to have a more comprehensive approach that goes beyond the clinical perspective. A recent literature review,
16
of the practices, goals and perspective of emerging themes of appropriate care, highlighted five categories of appropriate care: evidence-based care, resource use, clinical expertise, patient-centeredness and equity. Looking at these emerging themes from a managerial and organizational perspective, we highlighted four dimensions of appropriateness:
Clinical: in this sense appropriate means first of all to provide Evidence-based medicine that according to Sackett definition is “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. It means integrating individual clinical expertise with the best available external clinical evidence from systematic research and patients’ choices and values”.
17
This dimension incorporates three elements highlighted also by Robertson-Preidler et al.
16
evidence-based care, clinical expertise and patient-centeredness. As a bottom up approach that integrates the best external evidence with individual clinical expertise and patients' choice, it cannot result in slavish, cookbook approaches to individual patient care. Equity: appropriate means the absence of avoidable or unfair variations among group of people in resource use, health related outcomes and access to health care services within the same organization or among different organization. This is related to the fact that individuals with similar characteristics should be granted the same access to healthcare services and same indication for treatment regardless of demographic and geographic or other means of stratification. Service delivery model: this dimensions relates to the allocation of resources, included variation in resource use, cost-effectiveness, delivery practice and health care setting to reduce waste and unnecessary care and ensure proper provision and equity in health care delivery practices. This dimension relates to the components of care delivered, encompassing the use of resources in terms of what is done in giving and receiving care, divided into patient-related processes (prescription patterns, intervention rates, referral rates, etc.) and organizational aspects (supply with drugs, management of waiting lists). Outcome: this dimension relates to the relationship between tools/methods and outcomes. Appropriate means that for comparable target group (for same specific characteristics but taking into account individual variability) the expected health outcomes following a specific procedure are similar. In this context outcomes refers to both final outcomes, such as mortality, morbidity, disability or quality of life, and intermediate outcomes, for instance, blood pressure, and functional ability.
Regarding the second questions, what are the methods and models to measure the appropriateness, different methods and tools have been developed to measure the appropriateness of care and develop both valid criteria and recommendations for healthcare providers. 1 , 2 , 18 However, in line with the definitions of appropriateness provided above, the methods to evaluate the appropriateness of care are highly intertwined only with the clinical perspective. Our literature analysis has not identified, indeed, tools or approaches that could systematically support providers in keeping the appropriateness of elective surgery under control. One of the most widely used and cited method is the RAND Appropriateness method (RAM), 1 , 12 , 19 , 20 a multistep process that incorporates both the existing evidence and the results of clinical consensus among key experts. The RAM method is used to identify which types of health care were overused and/or underused; nevertheless, it has the limitation to be based mostly on the opinions of experts, which are formed, by their own memories, interests and perspectives. In most of the cases, indeed, panels depend heavenly on the opinions of experts and therefore, may not be representative. 14 As a result, the composition of the expert panel matters and the assessment depends in large part on the background mix of clinicians involved in the deliberations. In this direction, Fraser et al., 21 found that surgeons’ panels were more likely to agree on indications for cholecystectomy while mixed panels (made not only by surgeons), were more conservative.
Based on these findings, we designed a systematic approach aimed to evaluate the four dimensions of appropriateness taking into account the existing literature, the opinion of mixed experts panel (as for RAND method) and the information retrieved from medical and administrative databases. In developing our approach we considered a procedure appropriate when: i. the expected health benefit (e.g., increased life expectancy, relief of pain, improved functional capacity) exceeds the expected negative consequences (e.g., mortality, morbidity, pain, time lost from work) by a sufficiently wide margin that the procedure is worth doing 12 ; ii. comparable target groups receive treatments and/or procedures with no significant differences in terms of outcomes (equity and service model).
We used the elective surgical procedures to test the model as surgical procedures are highly codified, and these codifications are widely used and standardized among the scientific community. Therefore, considerable variations in rates of procedures generally indicate that there are wide variations among health professionals that cannot be explained by epidemiological factors or availability of resources.
Among the elective surgical procedures, we used the spinal fusion (arthrodesis) as a paradigmatic example of potentially inappropriate surgery.
Spinal fusion: An introduction
Spinal fusion is a procedure designed to permanently immobilize the spinal column vertebrae to treat debilitating spinal disorders. 22 Spinal fusion is indicated for scoliosis, spondylolisthesis, congenital deformities, spinal instability in trauma or by iatrogenic causes (e.g. extensive laminectomy), infection and neoplasm. However, the use of spinal fusion for patients presenting with low-back pain, in the absence of stenosis or spondylolisthesis, remains a controversial subject. 23 In fact, the available evidences in this field are still, with few exceptions (e.g. Lumbar spondylolisthesis of various aetiologies), particularly weak 24 and they do not support a benefit from spine fusion compared to non-operative alternatives for back pain associated with degeneration or for fusion thoracolumbar burst fractures. 25 Similarly, the outcomes of spinal fusions, such as functional health status or quality of life, remain uncertain and it is still difficult to identify which surgical approach yields the highest results. 26
In line with this, a recent systematic review 25 carried out to summarize the current level of evidence for spinal fusion highlighted that better evidence is required to determine more accurately the effectiveness of spine fusion surgery for all indications.
Despite little high-quality evidence to support the use of spinal fusion for most back-related conditions and the disagreement between surgeons on when spinal fusion should be performed, over the last 30 years, a number of reports have indicated that the number and cost of spinal fusion procedures have increased significantly worldwide, with marked variations among countries. 27 , 28
The United States has the highest rates of spinal surgery in the world, despite incidence and prevalence rates of spine disorders are similar to those found in other countries. Weinstein et al. 24 have identified a steadily increase in lumbar fusion surgeries between 1992 and 2003 in patients over the age of 65, from 0.3/1000 to 1.1/1000 enrolees. A 20-fold variation in regional rates among enrolees was also identified, representing the largest coefficient of variation seen with any surgical procedure. Deyo et al. 29 identified a 15-fold increase in the frequency of complex fusion procedures for spinal stenosis between 2002 and 2007 (from 1.3 to 19.9 procedures for every 100,000 beneficiaries) although they described a slight decline in the number of lumbar fusion procedures performed among Medicare beneficiaries (from 137.4 in 2002 to 135.5 in 2007).
A variety of factors have contributed to this increase: the overall increase in the life expectancy, the advancements in surgical technology (less invasive approaches) and better perioperative support. 30 However, the increase in the aging cannot completely explain the increase in spinal fusions; other procedures, such as joint replacements increased at a lower rate during the same period (from 1998 to 2008): hip replacements yielded 49.1 percent increase and knee replacements saw a 126.8 percent increase, compared to the 137 percent increase of spinal fusions. 30
According to the data from the Dartmouth Atlas Project, this increase has also resulted in an increase of costs: the annual direct costs for lumbar fusions rose from 75 million dollars in 1998 to 482 million dollars in 2003. In 1992 lumbar fusion represented 14% of total spending for back surgery but by 2003, lumbar fusion accounted for 47% of spending. 24 Rajaee et al. 30 also found that average total hospital charges associated with spinal fusion discharges tripled from 1998 to 2008 and that national bill for spinal fusion increased 7.9-fold.
The increase of spinal fusion procedures was also related to an increase in morbidity, complications and treatment failures often attributed to poor patient selection and inappropriate treatment. 27
Spinal fusion geographical variations, 31 scientific uncertainty and insufficient evidences regarding different spinal fusion procedure, financial incentives and disincentives to surgery, differences in clinical training and professional opinions, 24 relationships with device companies, influence of key opinion leaders, and the desires of surgeons to be local innovators 29 de facto, contribute to variability in clinical decision-making and raise concerns about the appropriateness of this procedure worldwide.
Concerns about the appropriateness of fusion surgery have been raised also in Italy (ERA - Epidemiology and Applied Research). 32 The high number of spinal fusions, especially in some regions such as Valle D’Aosta Region and Sardinia Region, highlighted the potentially inappropriate use of this procedure with some patients undergoing procedures that they needed, and others undergoing procedures that they did not need. 33 The ERA Report, indeed, analysing the discharge rates for 2008 for fusion surgery, highlighted that discharge rates were 44% higher in Sardinia Region than in Italy for both male and female (+49% and 37% respectively). The standardized rate of hospital discharge per 10,000 inhabitants for fusion surgery in Sardinia Region was 5.68 for male (compared with an average of 3.82 for Italy) and 4.74 for female (compared with an average of 3.45 for Italy). 32 These elements have led to calls for care providers in Sardinia Region to adopt measures for regulating the delivery of spinal fusions.
Methodology
Development of the framework
The aim of the study was to develop a framework that could be systematically used to evaluate the appropriateness of elective surgery. In this light, the aim of the study is rather to provide a tool to evaluate the appropriateness then to give insights about the appropriateness of a specific procedure. We therefore developed a four-dimension conceptual framework for evaluating appropriateness (Figure 1) that took into account the four dimensions of appropriateness described above and two essential questions: Do people need the care they get? Do people get the care they need? 34
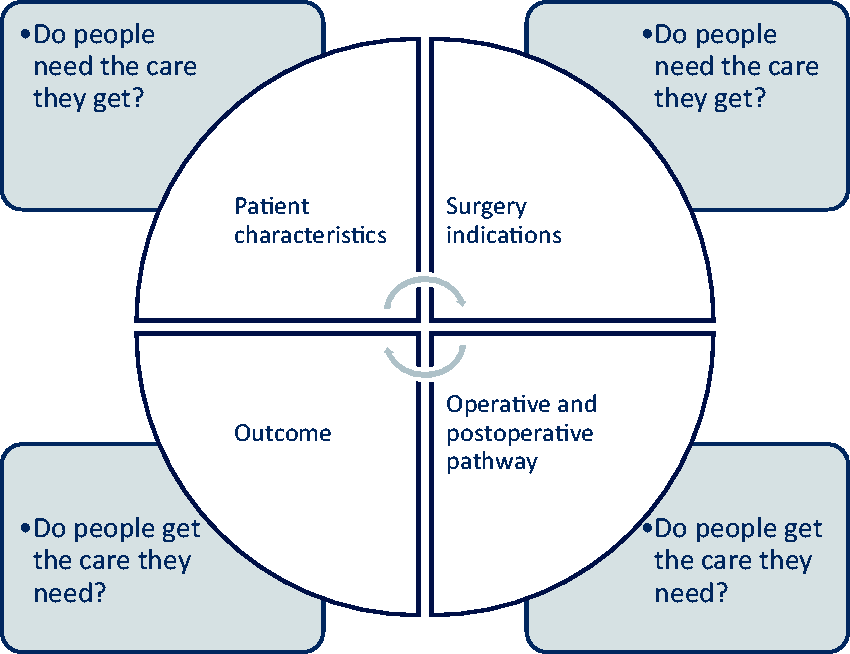
Framework for the evaluation of appropriateness.
Patient characteristics relates to the clinical dimensions and it answers the sub question: in light of current best evidence, do people need the care they get?
Indication for surgery relates to the dimension of equity and it answers the sub question: are target patient with same characteristics receiving similar treatment or procedures between and within similar healthcare organizations?
Operative and postoperative pathway relates to the service model and the components of care delivered and organizational aspects.
Outcome relates to the relationship between target patients and outcomes (e.g. readmission within 30 days).
We used spinal fusion as a paradigmatic example of a potential inappropriate procedure.
Cohort identification and evaluation
We developed the study in cooperation with a private provider, Kinetika Sardinia (KS), recognized by the Italian society of spinal surgery as a centre of excellence for spinal surgery and elective surgery. KS delivered more than 2,500 surgeries between 2010 and 2015. We employed a mixed method approach for the evaluation of appropriateness criteria that consisted of four steps: situational assessment, engagement of stakeholders, identification of the improvement actions and the desired outcome, monitoring and evaluation.
A. Situational assessment: We carried out a retrospective analysis of administrative data collected from KS between January 1, 2010 and April 30, 2015 to identify patients using the diagnostic related group (DRG) code 498 (spinal fusion surgery except cervical, without complication) for the following International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 CM) procedural code: 81.06 (fusion surgery, anterior, lumbar/lumbosacral), 81.07 (fusion surgery, lateral, lumbar/lumbosacral), 81.08 (fusion surgery, posterior, lumbar/lumbosacral). Data were collected from three surgical teams, operating in two different clinical centres: Team A (Sant’Elena), Team B (Città di Quartu) and Team C (operating in both clinical centres Città di Quartu and Sant’Elena).
Patients were retrospectively associated to the surgical team who performed the procedure.
We therefore analysed the baseline patient characteristics (i.e. age, health condition), the indication that led to surgery (i.e. imaging examinations, clear indications for surgery), the operative and postoperative pathway in terms of length of hospital stay, medical devices used and surgical approach, and the surgical outcomes in terms of pain and readmission within 30 days.
B. Engagement of stakeholders: We involved internal stakeholders both in a working group and in a focus group aimed to support the project development and to improve the professionals experience exchange. The working group was composed by the Medical director, Operation management head, Quality department head and a surgeon with high expertise on the topic. The working group supported data collection, data processing and information dissemination.
The focus group was conducted by an external expert in healthcare management and involved chief surgeons from three different teams (Team A, B and C) and representatives from the working group.
C. Identification of the improvement actions and the desired outcomes: Based on the critical area emerged during the analysis, the discussion within the focus group allowed to identify improvement actions and define a set of performance indicators. Benchmarks were based both on literature and on iterated consensus among professionals. Performance indicators were subsequently operationalised to fit with hospital information system and administrative records.
D. Monitoring and evaluation: Monitoring and evaluation actions were finally conducted in order to assess if the improvement actions identified were put into practice and acquired desirable outcomes. Monitoring data were collected from the hospital discharge records (SDO) for the first semester of 2016 and benchmark analysis with previous data were conducted.
Data were analysed by descriptive and analytical statistics including mean, median, standard deviation and correlation using SPSS 24.0. Data were analysed also separately for each surgical team.
Results
Do people need the care they get? Patient characteristics (age and pathologies)
We collected data for 2,584 patients (1,356 – 52.5% females and 1,228 – 47.5% male) that underwent spinal fusion between January 1, 2010 and April 30, 2015: 1,769 (68.5%) patients were operated by Team A, 657 (25.4%) by Team B and 158 (6.1%) by Team C.
The average age for patients receiving spinal fusions was 59 years (56.9 men, 60.9 women), with the major concentration of cases between 68 and 71 years. There were no differences between the characteristics of patients associated to each team.
The analysis of the ICD-9 CM Classification, based on administrative databases, revealed three diagnosis groups: pathology of the sacrum (67%), lumbar stenosis (20%), and other conditions (23%). Mainly Team A used the “pathology of the sacrum” diagnosis code. These differences among teams were not related to patient characteristics but to different coding style of the conditions that led to the surgery (see improvement actions).
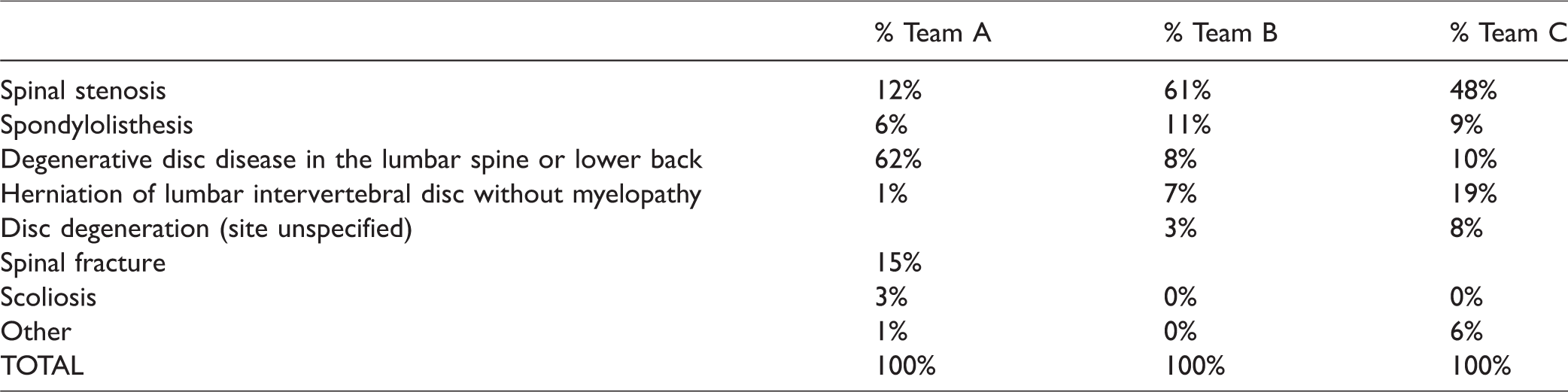
The analysis of clinical records showed five main pathological conditions: Degenerative Disc Disease (DDD), spinal stenosis, spinal fractures, spondylolisthesis and herniation of lumbar disc (Table 1).
ICD9-CM diagnosis that led to spinal fusion (01/01/2010 – 04/30/2015).
Do people need the care they get? Indication for surgery
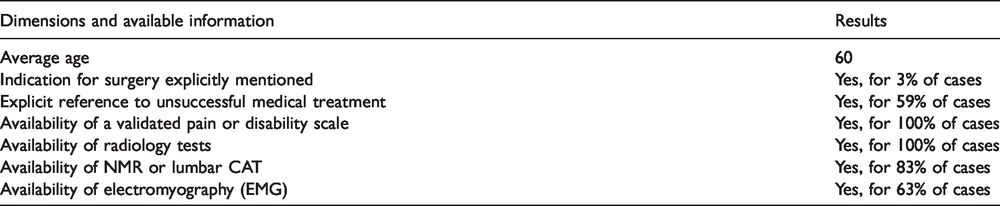
We analysed a sample of 59 medical records referred to hospitalizations in 2014 to evaluate indications for surgery. The analysis was conducted using a grid of questions aimed to highlight several dimensions of appropriate indications for spinal fusion (Table 2).
Appropriateness assessment of 59 medical records.
This cohort of patient was randomly selected from the universe (2,586 patients in the study): 23 patients (39%) were operated by Team A, 22 patients (37%) were operated by Team B, and 14 patients (24%) were operated by Team C.
Do people get the care they need? Operative and postoperative pathway
We analysed two dimensions: the medical devices used in spinal fusion and the postoperative pathway in terms of average length of stay (ALOS).
Fusion techniques and medical devices
The analysis of the medical records and the focus groups with the professionals showed differences among teams in the selection of surgical techniques that can be deduced also from the types of medical devices used.
Average length of stay
ALOS was 5 days, with great variations among teams: 4.5 days for Team A, 3.9 for Team C, and 7.3 days for Team B. We found a statistical significant difference (p<0.01) in the ALOS between Team A/C and B (see improvement actions).
Do people get the care they need? Outcomes
Persistent pain and non-responsiveness to analgesic treatment is one of the main reasons leading to surgery. All the teams carried out the evaluation of the pain expressed and perceived before the surgery using the Numeric rating scale (NRS); however, no evaluation was carried out after the surgery. The percentage of patients with a readmission within 30 days from surgery was 5%.
Improvement actions
Based on the analysis and the exchanges with professionals we identified for each dimension specific improvement actions.
Use of ICD 9 CM codes: precise and homogeneous coding of the conditions that led to surgery. Teams are supposed to improve the accuracy of the coding within the hospital discharge record. Herniation of lumbar disc: reduce the number of spinal fusions for lumbar intervertebral disc herniation without myelopathy. Presence of an explicit statement about the need of surgery: clearly state the reasons that led to surgery in all medical records. Previous pharmacological and conservative therapies: report ineffective pharmacological and conservative therapies in all medical records. NMR (or lumbar CAT): all patients are supposed to be evaluated by lumbar NMR (or lumbar CAT) imaging before surgery. EMG: teams are required to share the criteria for EMG use before surgery. Information on the medical devices used: it is necessary to connect the information on medical devices not only to the operator but also to the patient and integrate the information codified within the hospital discharge record. Length of hospital stay: according to the literature, teams should reduce the average length of stay to less than 5 days. Pain scale: NRS is a unidimensional pain scale with 0 representing “no pain” and 10 representing “pain as bad as you can imagine” and “worst pain imaginable”. However many high-quality clinical trials have shown that spinal fusion provides significant clinical improvements in most lumbar disc degenerative patients, measuring improvements across the VAS scale and the Oswestry disability index.
35
Follow up: professionals should use VAS scale and ask patients to express their satisfaction with surgery (score 0 to 10) categorized as follow: low satisfaction (0–3), medium satisfaction (4–6) and high satisfaction (7–10). The aim is to assess the impact of spinal fusion in terms of both pain reduction and patient satisfaction. Patient outcome: it is useful to monitor the number of readmissions within 30 days of surgery.
Monitoring
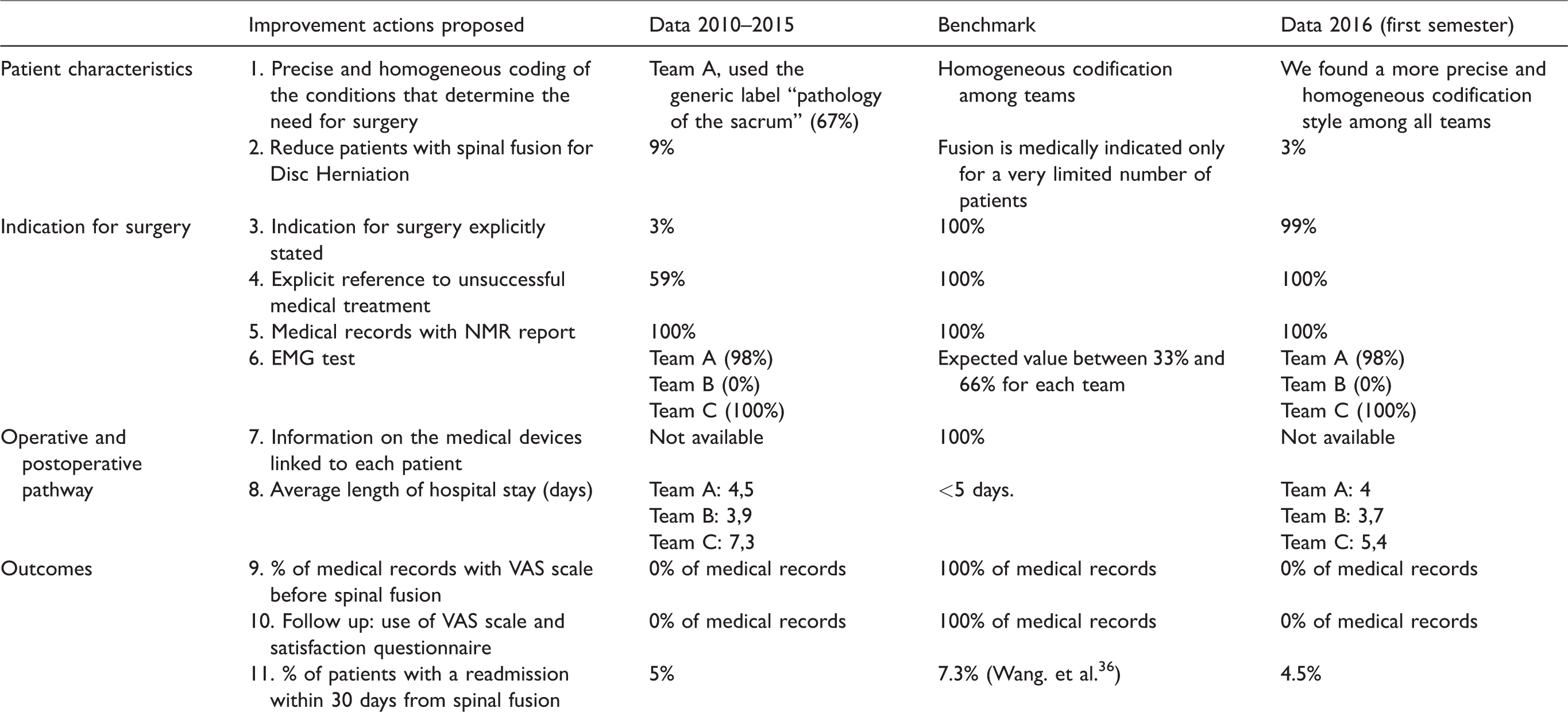
We collected monitoring data for 171 patients that underwent spinal fusion between January 1, 2016 and June 30, 2016. The results are in Table 3. These patients were similar to the 2,584 patients that underwent spinal fusion between January 1, 2010 and April 30, 2015 for several characteristics (i.e. age and sex). The average age of patients receiving spinal fusion was 59 years for the cohort 2010-2015 and 58 years for the cohort of 2016.
Summary of improving and monitoring actions.
Discussion
Do people need the care they get? Patient characteristics (age and pathologies)
Average age is consistent with data by Rajaee et al., obtained from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample between 1998 and 2008. They observed that the average age for patients receiving spinal fusions increased from 49 in 1998 to 54 years old in 2008. 30 Bones and joints degeneration is part of the aging process and often results in lumbar instability or stenosis and can benefit from surgical treatments, including spinal fusion.
DDD is the most frequent condition leading to surgery for team A (62%), but it was spinal stenosis for team B (61%) and C (48%). This is only an apparent heterogeneity among teams, as the most common cause of spinal stenosis in older people is DDD.
Guidelines state that surgery for herniation of lumbar intervertebral disc without myelopathy should be considered only after several months of non-surgical treatment, all teams, albeit with different frequencies (1% Team A, 7% Team B, 19% Team C), performed spinal fusion for Disc Herniation.
Do people need the care they get? Indication for surgery
The analysis revealed the presence in all medical records of a self-assessment validated pain scale, however the score was not reported in the medical records, therefore no comparison was possible between the differences in reported pains across groups of patients associated to different teams. The NRS is an extremely useful tool to assess the cause, severity, and nature of the pain and is a baseline for subsequent pain and disability measurements. In all records, we also found lumbar NMRs or lumbar CATs.
We found a completely different approach in the use of electromyography (EMG) test among surgical teams. EMG is not a routine test for spinal disorders and must be ordered only when someone is showing symptoms of muscle or nerve disorder (i.e. tingling, numbness, or unexplained weakness in the limbs). In spite of that, we found that team A and C performed EMG test almost every time, while it was rare for team B.
Finally, only 3% of the medical records reported an explicit formulation of clear indication for surgery.
Do people get the care they need? Operative and postoperative pathway (surgical techniques, length of stay)
The selection of surgical techniques is susceptible to both surgical competences and alignment with the international literature. We found that data regarding the medical devices were available only per operator but not linked to the patient. An understanding of the types of devices used in the different procedures is necessary as it gives a lot of information on the motivation that led to surgery and facilitates the choice of an appropriate modality for imaging of the postoperative spine. 37 This data should therefore integrate the information codified within the hospital discharge record.
The ALOS was 5 days, Rajaee et al. 30 in their study reported a lower ALOS (3.9 days). Differences between teams were linked to the rehabilitation procedure used: team A and C allowed the patient to stand up and walk immediately after surgery, while team B allowed the patient to stand only after three days from surgery.
Do people get the care they need? Outcomes
The outcomes can be evaluated measuring the readmission rate within 30 days of hospital discharge. A retrospective cohort study conducted in the United States (a sample of 343,068 Medicare beneficiaries who underwent cervical and lumbar spine surgery for degenerative conditions from 2003 to 2007) showed that 30-days readmissions were 7.3% after lumbar surgery. 36 The most common reasons for readmissions were complications of surgery (26%–33%) and musculoskeletal conditions in the same area of surgery (15%). Significant predictors of readmission included older age, greater comorbidity, greater number of fused levels, and an anterior surgical approach.
In a subsequent study, Pugely et al. 38 identified the following predictors of readmission: age more than 80 years, recent weight loss, chronic obstructive pulmonary disorder (COPD), history of cancer, creatinine more than 1.2, operative time more than 4 hours and prolonged hospital length of stay more than 4 days.
These factors need to be carefully considered to minimize the risk of 30-days readmissions after elective spine surgery and to put in place specific actions to reduce avoidable readmissions.
Monitoring
Monitoring data showed improvements about case selection (e.g. surgery for Disc Herniation decreased), medical records quality, and ALOS. However, margins for improvement remain wide in other critical areas such as quality of data about medical devices, and follow up. Managing appropriateness require a change management approach including the introduction of dedicated organizational positions for managing appropriateness; the development of IT system; the improvement of professional training and professional exchange to foster performance, process and outcome monitoring; integrating patient perspective in the performance measurement system; and improving patient flow management in all the steps (pre-hospitalization, hospitalization, operative, postoperative and follow-up).
Limitation
Data were collected from three surgical teams operating in two different clinical centres; however, the main limitation of this study is that it focused only on a single institution and only on a single procedure, namely spinal fusion.
Conclusions
Understanding and measuring appropriate care delivery can help decision makers to take a comprehensive approach that puts together system, clinical expertise, and patient perceptions. This can improve patient outcomes and experiences in a sustainable way.
Our work has three main implications. Firstly, regarding the definition of appropriateness, it goes beyond the traditional clinical definition including some other perspectives and dimensions, that need to be taken into account such as metrics to measure performance and monitor progress towards achieving key goals. These dimensions comprise clinical evidences, with equity, services delivery model and outcomes.
Secondly, regarding the metrics to measure the appropriateness, our work shows that no other frameworks were available in the literature to evaluate the appropriateness of elective surgery from an organizational perspective. The RAM method is one of the most cited framework and it is used to identify which types of health care were overused and/or underused, nevertheless, it has the limitation to be based mostly on the opinions of experts which are formed by their own memories, interests and perspectives and in most of the cases, may not be representative. 14 Several studies have shown that mono specialist panels (i.e. surgeons’ panel) were more incline to endorse indication for surgeries, while mixed panels were more conservative. 21 As a result, the composition of the expert panel matters and could have an impact on the assessment of the appropriateness.
The framework and the approach we developed has several strengths:
It allows to systematically assess the appropriateness of care: the framework for the evaluation of appropriate elective surgery and the identification of the dimensions to put under observation was done through focus groups involving healthcare professionals, the medical director, the Operation management head and the Quality department head. Once defined, the framework has been routinely used by support staff and techno structure. The study also suggested which actions should be considered to support change management and improve appropriateness in elective surgery. This is not a one-time evaluation but it requires recurrent evaluation to take the appropriateness under control and to determine the extent to which new actions or improvement interventions actually work and improve appropriateness as expected or if there are also adverse effects related to these changes. It is a low-cost approach based on three elements: evidences from the existing literature, cooperation between professionals and managers (opinion of mixed experts panel as for RAM method), and data retrieved from medical and administrative databases which are not primarily generated for quality or research purposes but, by definition, for administrative and management purposes (for example, billing data, routine documentation) but they have the advantage of being readily available and easily accessible in electronic form. Moreover, many healthcare providers, in particular hospitals, are usually already mandated to maintain administrative records, which are used in many countries for quality measurement purposes. Therefore, there is no added cost to use administrative data for evaluating appropriateness. Administrative database provides relevant, complete, accurate, timely and accessible information able to support decision-making and the health care management. Measuring the appropriateness of care is important for a range of different stakeholders within healthcare systems, and it builds the basis for numerous quality assurance and improvement strategies: accreditation and certification, audit and feedback, public reporting and pay for quality. All these strategies rely heavily on the availability of reliable information about the care provided by different providers and/or professionals. Therefore, these measurements could not be devolved neither to the opinion of experts, neither to simply the perception of patients and require the development of approaches and dedicated organizational structures or functions. The study is replicable. Although it focused only on spinal fusion surgery we believe that our approach can be replied in other surgeries at elevated risk in terms of appropriateness starting from the ones with highest volumes such as hip and knee replacements, and cataract surgery.
The third implication of this study is that the healthcare organization should reflect on who is responsible for defining metrics, and what competences he/she may need. Our study highlighted that it is important to develop specific competences blending clinical perspective and ability to interact with healthcare professionals, but at the same time being able to use all the potential of the administrative databases and prospectively big data. These are multifaceted competences which are in the realm of the clinical governance and help organizations to strengthen their own decision-making system.
List of abbreviations
Supplemental Material
sj-pdf-1-hsm-10.1177_0951484820952331 - Supplemental material for Evaluating the appropriateness of elective surgery: The case of spinal fusion (arthrodesis)
Supplemental material, sj-pdf-1-hsm-10.1177_0951484820952331 for Evaluating the appropriateness of elective surgery: The case of spinal fusion (arthrodesis) by Valeria D Tozzi, Guglielmo Pacileo and Lucia Ferrara in Health Services Management Research
Footnotes
Acknowledgements
This study would not have been possible without the support of Kinetika Sardinia who contributed to the research and especially without the great work done by Medical Director Korian Italy MD Aladar Ianes, Kinetika Sardinia Management and healthcare professionals who participated in the focus group. We are sincerely grateful to all of them.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The funding body was involved through the Medical Director, the Kinetika Sardinia Management and healthcare professionals in the data collection and in the focus group. However, the funding body had no role in the design of the study, analysis and interpretation of data and in writing the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research has been founded by Kinetika Sardinia (Italy).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.