
Abstract
How can we explain cross-regional policy variation? That is, how can we understand different policy outcomes within similar institutional and organizational settings? Scholars have recently reflected on the new institutionalist explanatory pitfall involved in assuming a causality link between institutional factors and policy outcomes and argue that such link needs to rely on evidence from policy variables. On this line, recent contributions have built a causal model that links types of institutional change to types of actors' roles and strategies, within particular contextual and organizational scenarios that favor or hinder their emergence. This paper pursues this explanatory interest by applying this model to the analysis of how decision-making by two regional governments in Spain has led to different institutional and policy change outcomes in the same policy sector, namely, public management reform in healthcare. This study confirms the explanatory relevance of the model's key variables, but provides evidence of how some of them may be reinterpreted to provide a dynamic explanation of their influence on the process and outcome of institutional and policy change.
Introduction
Comparative politics and public policy research share an interest about the politics of institutional and policy change. This interest has translated into different research issues, such as patterns of policy variation in the content of reform policies and the role of particular factors in explaining policy variation across territories. A case in point is the study of public sector reform, with a special focus on the public management policy domain (Barzelay, 2001; Barzelay and Gallego, 2006, 2010a, 2010b; Ferlie and Ongaro, 2015; Hood, 2000; Knill, 1999; Ongaro, 2008, 2009; Pollitt and Bouckaert, 2000; Sahlin-Andersson, 2002). This literature has largely benefited from the use of new institutionalist approaches in order to explain variation in institutional and policy change in a policy domain where redesigning institutions involves changing policy, namely, public management.
However, these research developments suggest at least two challenges. First, as Radaelli et al. (2012) have recently put forward, there is an explanatory pitfall involved in assuming a causality link between institutional factors and policy outcomes just because they appear repeatedly associated. They argue that such a missing explanation link needs to rely on evidence from policy variables, such as resource distribution among public and private actors in that particular policy sector, network relations among them, or actors' prevailing discourses and normative assumptions.
Second, we need to improve our understanding of incremental institutional and policy change, because a substantial part of change processes occur that way. New institutionalism relies on assumptions that reinforce the idea of stability and are ill suited for explaining change. Change is explained not as an incremental, endogenous process, but as an abrupt shock fostered by external factors. Recent contributions provide useful theoretical tools that could help advance on these lines. Hacker (2004) and Streeck and Thelen's (2005) elaborated typologies of institutional change that, despite some variations, were based on the identification of external and internal barriers to change. Despite being useful for analytical purposes, this sort of contribution only provides help for classification of empirical examples of institutional change. As Radaelli et al. (2012) highlight, there could be an explanatory pitfall if we attributed causal arguments in the use of typologies.
In this sense, Mahoney and Thelen (2010) develop a theoretical model that tries to build causality arguments by linking contextual and organizational properties (which partly fit Radaelli et al.'s policy variables) to types of institutional change expected. They define a combination of variables—characteristics of the political context, characteristics of targeted institutions, and typology of actors and their strategies. They argue that particular contextual and institutional features facilitate the emergence of particular types of agents—with their associated type of strategies—in the pursuit of particular types of institutional change. This logic has been applied to numerous empirical analyses, providing insights in the explanation of incremental institutional change (Falleti, 2010; González, 2013; Jacobs, 2010; Kwamena, 2010; Marshall, 2014; Sheingate, 2010; Slater, 2010).
This paper pursues this search for a causality link by addressing the question of how can we explain different policy outcomes within similar institutional and organizational settings? We analyze how decision-making by regional governments in Spain leads to different policy outcomes in the same policy sector; namely public management in the health sector. These policy differences develop within (and in spite of) similar institutional settings: all the regional political institutions created from anew have the same design patterns and all the health institutional and organizational structures transferred by the central government to the regional governments shared the same institutional design.
The case studies analyzed here concern the health management policy trajectory in Andalusia and in Catalonia. The health institutional and organizational structures transferred to them by the central government at the onset of decentralization, as well as the management regulations attached to them were originally the same. These structures were to be the foundations of their regional health systems. However, both regions consistently pursued different health public management models since then and until the turn of the century, thereby deepening preexisting differences between them in terms of resource distribution among public and private actors, network relations among them, and actors' prevailing discourses and normative assumptions.
This study focuses on the first decade of the 2000s, when important external shocks posed new challenges and created a new scenario for policymaking, but such different strategies still persisted. In Andalusia, the same political party (Spanish Workers' Socialist Party—PSOE) has been in office since 1983, when the first Andalusian elections under democracy were held, to date. In this case, the health public management policy trajectory shows features of incremental institutional change. Since the turn of the century, though, public management changes were triggered but only to reinforce the chosen model. In Catalonia, the same Catalan nationalist party coalition (Convergence and Union—CiU) ruled between 1981, when the first Catalan elections after the democratic transition were held, until the elections of 2003, when a governmental turnover brought to power a coalition of independentists and centre-left parties. After more than two decades of incremental institutional change, the new government initiated an institutional reform involving public management policy change that had been considered almost impossible to address until then, and which they finally passed as a law in 2007, under a second legislature.
The empirical data used in this study include official documents and semistructured interviews to 30 key informants who, either were directly involved in the processes analyzed, such as, public officials (both politicians and top bureaucrats), managers of health providers, and health professionals, or have privileged knowledge about it (researchers), as well as hard data on the factors relevant for our hypotheses (financing model, electoral results, etc.). We rely on the analytical dialogue between theory and empirical data to provide an interpretation of the two selected processes of institutional and policy change.
In this paper, we first lay the theoretical approach of the study and then apply Mahoney and Thelen's (2010) theoretical model to the analysis of the incremental institutional and policy change pursued in the public management of the Catalan and Andalusian health sectors. The following section then shows a comparison of the two case analyses and identifies some relevant research questions Mahoney and Thelen's model does not address. We argue that whilst they acknowledge that the types of agents they define are not fixed identities but roles (Mahoney and Thelen 2010, footnote 7: 23), an explanation is needed as to how and why actors may shift between roles and strategies, namely, dynamic processes which turn out to bear explanatory weight in the two cases analyzed. The concluding section highlights the main contributions of this study to the research interest about institutional and policy change.
The theoretical approach: Context, institutions, and change actors
According to Radaelli et al. (2012), the explanations for variations in policy outcomes across countries and for policy continuity and change within countries often rely on analytically questionable arguments. Specifically, they identify four explanatory pitfalls in the use of new institutionalist interpretations: considering institutional characteristics as determinants of policy outcomes, attributing explanatory power to typologies, not including policy-level variables in the explanatory argument of policy variation, and not identifying mechanisms through which particular institutional settings lead to observed policy outcomes. As a result, they claim, some comparative public policy research tends to gather evidence of institutional variation associated with policy variation but does not provide hindsight on causal relationship between institutional-level variables and policy-level variables.
However, including policy-sector variables into that causal link involves identifying them and justifying their selection in the framework of a theoretical model. This task is complex at least for two reasons. First, analytically relevant policy-sector characteristics may not be the same across all policy sectors: for example, the private–public mix in service provision or professionals' labor market regulations may be highly relevant for explaining policy outcomes in the health policy sector, but not in the transport policy sector; similarly, the degree of concentration of private financing entities may be relevant for policy outcome in the telecommunication policy sector but not in the education policy sector. Second, policy sector-level characteristics may vary considerably across countries and within countries: for example, professionals' labor market regulations may differ substantially between Spain and the United Kingdom (UK), but not so the public–private provision mix; or there may be more variation in both such characteristics between two Spanish regions than between Spain and the UK as whole countries.
Exploratory case studies may help identify the policy-sector characteristics that are relevant for explaining policy outcomes. On this line, this paper seeks to build explanatory arguments for variation in public management policy in the health sector in two Spanish regions—the autonomous communities (ACs) of Andalusia and Catalonia. As in the rest of ACs, they have a similar institutional setting: the formal design of their regional governmental institutions is similar, following the requirements of the Spanish multilevel legal framework. But most relevant, the health institutional and organizational structures that were transferred by the central government to the regional governments shared the same institutional design, as they were homogeneous across all the country. Those health structures included public service providers (primary care and hospitals) as well as management rules, such as health professionals' civil service labor regulation, financial management, and organizational rules, all under the integrated, hierarchical, direct provision model, and within an administrative law framework. Despite that similar institutional and organizational context, the health public management policies they have pursued and targeted to those similar public health structures are strikingly different. Following Radaelli et al. (2012), other policy-sector features that are markedly different in those ACs shall also be taken into account, such as the existing private–public provision mix, the number and nature of organized interest groups, and the patterns of relationship between them and the political elite.
Contextual and institutional sources of change agents
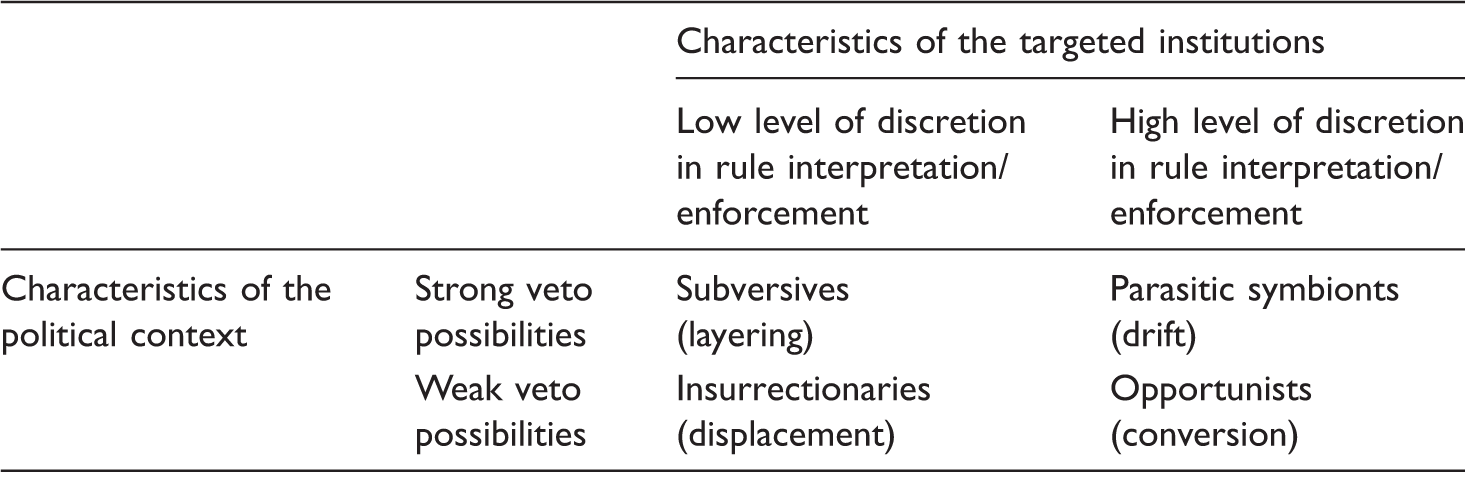
Source: Mahoney and Thelen (2010: 28).
This model does not define types of actors as fixed identities but as roles (Mahoney and Thelen, 2010: 23, footnote 7), and foresees potential coalitional dynamics among actors that embody them. This prevision does not make all actors opportunists, but endogenizes actors' preferences, goals, and strategies within the change processes. However, this model does not elaborate on how and why actors may change roles at a particular point in time and work for different types of institutional change. The model does consider veto possibilities and level of discretion to be variable—they may change over time for different actors—but it does not provide insights on the mechanisms that explain actors' shifting roles as an answer to those changes. In the next two sections, we apply this model to understand the Catalan and the Andalusian cases.
Explaining change in public management policy in the Catalan health sector
Policy precedents of the Catalan government
The trajectory of the health policy in Catalonia started with the devolution process in the early 80s of the twentieth century. Overall, while the rest of ACs maintained the organization of their regional health services on the basis of the public, direct provision model transferred by the Spanish government (with hierarchical integration of purchaser and providers), the Catalan government developed a health system based on an extensive, publicly funded, indirect provision model (arm's length relationship between purchaser and provider), with a complex network of providers of different public and private ownership formulae (Gallego 2001, 2003; Gallego and Subirats, 2011, 2012; Gallego et al., 2005).
However, within that network, the public providers transferred in 1981 by the Spanish government to the Catalan government (over 90% of primary care providers and a third of the hospital beds in Catalonia) remained as units of a single organization, the Catalan Health Institute (ICS), that operated under the direct provision model—a single provider with over 35,000 workers, most of whom civil servants. While the contracted network—Hospital Network of Public Utilization (XHUP) created in 1985—was substantially expanded and strengthened as an explicit political option to develop the Catalan health model, the ICS did not experience formal changes in its legal nature, but external conditions (particularly relationships among contracted providers, but also the introduction of “new public management” logic in the system) changed the ICS's situation in the health system, confining it outside the prevailing rules of the game. The evolution of the ICS fitted the Mahoney and Thelen's (2010) category of drift, as incremental and significant changes were mainly caused as a result of “nondecisions” by policymakers.
With the 1990 “Law of Healthcare of Catalonia (LLOSC)”, 1 the ICS lost its purchasing functions, in favor a newly created unit within the Catalan government, thus eliminating the integration of purchasing and provider functions embodied in the ICS and strengthening the contract-based model. The strategy of strengthening a management model different and parallel to the ICSs could also be interpreted as layering, in Mahoney and Thelen's (2010) terms. The ICS lost its purchasing functions after the LLOSC, which mitigated the rest of non-ICS providers' mistrust for ICS being both purchaser and provider. But the ICS still kept its differentiated public regulation in general and in civil service and labor relations regulations in particular, with different financing mechanisms, and therefore was still seen by the rest as an opaque isle of obsolete privilege. Research has provided evidence that, over almost three decades, the Catalan political and managerial elite in the health sector had persistently criticized the ICS management model as deeply inefficient (Gallego et al., 2014; Ibern, 2006; Lamata and Ortega, 1998; Moreno, 2009). Some top officials interviewed for this analysis argued that administrative law, such as civil service and contracting regulations, constrained cost-effective and efficient management. For this reason, some of them would have preferred a fast and direct change toward a private management framework, namely, a displacement in terms of Mahoney and Thelen's (2010) typology. According to numerous political and executive officials interviewed, several previous ICS's directors–managers had tried to address this issue with or without legal changes, but over two decades they had not found political support. A common interpretation these interviewees made of this lack of support is that CiU identified ICS as an example of Spanish centralist politics, on one hand, and of bureaucratic and obsolete management model, on the other. Those interviewees argue that CiU was not only convinced of the impossibility to modernize or reform ICS into an efficient organization, but would have no interest in trying, just in case a public provision model could prove manageable effectively and efficiently, which would contradict the assumptions in CiU's discourse.
In this context, actors both internal and external to the ICS interviewed for this study considered an overall reform as not worth pursuing, because it was too difficult both from a political and from a juridical point of view. They perceived high veto possibilities among external actors, such as the unions, the Treasury of the Catalan government, the contracted providers, and the local governments involved in the contracted network. Also, successive ICS's director–managers had perceived a high degree of discretion for improving management by low-visibility changes in tools and organizational practices, without a need to make formal authoritative changes. So, why was such a change finally made through a law in 2007 that transformed the ICS from an administrative body into a public enterprise?
Context, actors' strategies, and institutional change
The reformulation of the ICS's legal nature and the need to modernize its management tools had been permanent issues in the discourse of a large part of actors related to the Catalan health policy sector (politicians, managers, and professionals), attracting varying degrees of attention throughout that time. However, published research also highlights that these same actors consider that such changes had not been addressed over those years because: (a) from a legal point of view, it was very difficult to change regulations from a social security management body form to a publicly owned enterprise or to autonomous body forms; (b) the Ministry of Economy and Finance of the Catalan government, and particularly its Intervention Unit, due to the institutional bias derived from its control role, opposed a management model that might involve ex post economic and financial control; and (c) unions would probably mobilize a strong professional opposition if that proposal involved a change in labor relations (Gallego et al., 2014). Some arguments also point out that a legal redefinition of the ICS required an injection of economic resources (to balance budgets) that could not be affordable by the budget of the Catalan government. Taking into account that these arguments are based on factors that could be expected to remain stable over time, because they refer to institution-biased roles, the question is: Why were these factors not an obstacle to the passage of the 2007 ICS Law?
The Catalan regional elections of November 2003 brought the first ideological turnover in the Catalan government since the Spanish democratic transition of the late 1970s. The nationalist, center-right party federation Convergència i Unió (CiU) had ruled the Catalan government over 23 consecutive years, since the first regional election in 1980, and with an absolute majority between 1984 and 1995. As a result of the 2003 Catalan elections a postelectoral center–left coalition formed to add up to an absolute majority in parliament and took office. The coalition included the Party of the Socialists of Catalonia (PSC), the independentist Republican Left of Catalonia (ERC), and the eco-socialist coalition Initiative of Catalonia-Green (ICV-Verds).
The tripartite government promoted a different view of ICS. The PSC Minister for Health of the Catalan government, Marina Geli, made her intention explicit 2 : to address the ICS's modernization through a change in its legal nature and the improvement of its management tools and autonomy, with an aim to make it closer to the way of operating of the contracted providers, all with an aim to ensure its sustainability as a central piece of the public health system. She was aware that in order to take this path, she had to gain credibility in the eyes of the Minister of Economy and its Intervention Unit. The ICS had a differentiated budget within the government's budget, a unitary organizational structure, and strict ex ante control routines, which were considered to facilitate expenditure and deficit control by the Intervention Unit, that is ensuring a low degree of discretion in the enforcement of spending and financial management rules. According to most officials interviewed for this research, Economy's top officials commonly thought that decentralization or ex post controls would weaken their inspection capacity, and that this option should be avoided, as the health budget was, for structural reasons (technology costs, age structure of the population, etc.), potentially unstoppable. Therefore, Geli had to pursue a strategy for making their veto possibilities lower by influencing their perception on the level of compliance of spending and financial management rules.
Geli also weakened veto possibilities coming from top officials within the ICS by appointing director–managers with a favorable profile. The first one was a doctor and previous top executive of the health services of the AC of Andalusia. He had a reputation for an experienced, pragmatic, and strict manager, who was committed to the sustainability of the public sector through the development of quality, efficiency, and management modernization strategies. The second one was a lawyer and the secretary of the Hospital Consortium of Catalonia, an association which had represented the interests of local governments in the health sector over the previous 20 years, with a clear preference for strengthening non-ICS contracted network in which they participated. His profile was associated with decentralized, public corporate health management and his explicit preference was for introducing significant changes in the ICS, such as its disaggregation into different units across the territory and the progressive incorporation of noncivil service staff.
Having been an active voice in the “municipalist” discourse in Catalonia, Marina Geli explicitly clarified her option for getting local governments more involved in health policy making and management and for opening new channels for citizens' participation. 3 This stance could help weaken veto possibilities coming both from local governments and from the contracted providers' network. The reason is that the Catalan health system's design lied on the support of major pressure groups: the Catalan Union of Hospitals (representing managerial interests from contracted providers) and the Hospital Consortium of Catalonia (representing the interests of those local governments that had management responsibilities in contracted health providers). Both had a preference for the ICS “playing under the same rules as them”—that is, as the contracted network, which involved disaggregating it and placing it under a private law framework. Also, both groups had strong and explicit connections with political parties in the Catalan Parliament, which made that venue a major veto point itself.
High veto possibilities came from the unions, which, according to union leaders interviewed for this study, would fight for the preservation of professionals' acquired labor rights. This was relevant because most ICS workers were civil servants, and civil service and labor relations were under the jurisdiction of the Catalan Ministry of Interior, under government party ERC, which introduced a parallel venue for issue-specific negotiation within the executive.
Explaining institutional change: From layering to displacement… or conversion?
The 2007 ICS Law 4 formally sought both an authoritative institutional change and a policy change: it transformed the ICS from an administrative body into a public enterprise—institutional redesign—with the corresponding change in the public management model—new tools, practices, and routines, that is a change in the public management policy. At first sight, it could be argued that this change amounted to displacement, and that it derived from the critical juncture created by the ideology shift in the Catalan government in 2003. Over the previous decades, the strong veto possibilities from a multiplicity of actors had converged on a lock-in situation. The government ideological shift boosted a new context of low veto possibilities where ICS internal actors, both executive and unions and professionals, could develop opportunist strategies. Also, this new situation would have facilitated the emergence of actors playing insurrectionary roles which would have led to displacement.
However, deeper analysis of the content and enforcement of the ICS Law places this institutional and policy change closer to conversion. In principle, shifting from administrative body to public enterprise involves higher degree of discretion in rule interpretation and enforcement, which was in line with what challengers of the status quo defended. However, the existence of numerous veto players and the need of parliamentary consensus as a veto point made it difficult for decision makers and executive officials to force displacement. At the same time, defenders of the status quo, despite having the power to press for the preservation of existing rules, were unable to prevent the introduction of small modifications.
According to the top officials interviewed for this study, the negotiations centered on four issues: legal personality, degree of financial autonomy, (non-)civil service status of health professionals, degree of organizational unity or disaggregation. Each issue had its own veto players and veto points. First, the Ministry of Economy and Finance of the Catalan government and its Intervention Unit opposed to any loss of ex ante financial control, so the result of the negotiation led to choose the alternative of quarterly permanent auditing, which meant an increase in the existing ICS's financial and accounting autonomy, but less than that which is usually enjoyed by public companies. Second, the negotiation with respect to the staff employment regimes and the degree of organizational unity or disaggregation of the future ICS were more complex. This process involved not only the Department of Economy and Finance and the trade unions but also the Department of Interior (responsible for civil service regulation). An agreement was reached with the trade unions in which the government would not change the employment civil service status of ICS's staff. There would be the possibility of contracting new staff with noncivil service status but only in certain circumstances and as an exception. The issue of organizational unity or disaggregation of the future ICS confronted several alternatives: disaggregating the ICS into different public companies, creating a public holding company (organizations with different legal statuses), or maintaining the existing legal unity. The alternative chosen was transforming the ICS into a unitary public company, its provider units (hospitals and primary care centers) would not have independent legal personality, and the use of the ICS's premises and services for private healthcare would be prohibited.
For the great majority of agents interviewed, the law had a limited impact on the specific management of ICS's activity. It was seen more as a formalization of pressures for specific management improvement practices that came from the organization itself but which did not aimed to revamp it. For defenders of the status quo, the law would demonstrate that it is possible to halt some of the inertia opposed to reform through gradual improvements and, at the same time, legitimize the place of the ICS in the Catalan health system. In other words, the ICS Law introduced amendments to existing rules just to ensure that the main structures remained stable. For challengers of the status quo, this law was the first step to deeper reforms toward disaggregation and privatization in a near future.
Explaining public management policy change in the Andalusian health sector
Policy precedents of the Andalusian government
Since Andalusia received the competencies on healthcare in 1984, its regional government preserved the public, integrated, direct provision model of health system as it was initially transferred by the Spanish government. In a region where at that time private actors did not exist in healthcare provision—only some religious entities offered charity healthcare services—the Andalusian government centralized the healthcare system almost exclusively to one organization: the Andalusian Health Service (SAS) (MSPSI, 2010). The SAS was the counterpart of the ICS in Catalonia and embodied the institutional and organizational structures transferred by the central government. The SAS was an autonomous, administrative organization that performed planning, contracting, and health service provision roles in the areas of both primary and hospital care. The SAS was placed under the jurisdiction of the Ministry of Health of the Andalusian government, but the role of this ministry was limited and its functions were not clearly differentiated from those of a number of SAS departments.
The continuation of the Spanish Workers' Socialist Party's (PSOE) in government since the first Andalusian regional elections of 1982—occasionally with an absolute majority—resulted in healthcare policy decisions that were supported by government majorities—and less by parliamentary consensus—as well as by their ideological preferences. Outside parliament, veto players were limited in number, although some accumulate significant power, such as professional unions (representing a mostly civil service labor force of health professionals within SAS). Criticisms to the inefficiency of the integrated, direct public provision model were recurrent, but much linked to the same arguments highlighted in the rest of regions—such as contending interpretations about the level of discretion of health professionals and managers in terms of spending routine decisions.
The consolidation of this model, though, did not prevent the regional government from exploring the introduction of organizational innovations toward the end of the decade (Martín, 2003; Palomo et al., 2012). On the one hand, these innovations included individual legal personification through the creation of certain state-owned companies outside SAS, but on the other, punctual agreements with private entities—both for-profit and non-profit—for the provision of hospital care. In this sense, the 1998 Health Law of Andalusia 5 laid the foundations for a possible—and future—separation of functions between the Department of Health and SAS. In 1999 SAS published its Strategic Plan, entitled “A differentiated proposal of public management” (Torrubia Romero and Higuera González, 2011), which recommended the introduction of clinical and administrative management strategies. However, none of these processes at the time involved structural changes in the management of the healthcare system, although they did form the basis for institutional changes which were put in place at the beginning of the 2000s.
Therefore, what happened to the healthcare management model in Andalusia in the early 2000s that fostered a reform—particularly, the introduction of new forms of provision and management models? Is it accurate to interpret such a reform as institutional change? If so, of what kind? How can we explain such a change?
Context, actors' strategies, and institutional change
The changes in the Andalusian public healthcare system during the first decade of the 2000s were numerous and diverse—including quality strategy, a clinical management model, and a change in labor policy at SAS, among other initiatives. According to policymakers interviewed for this research, these changes were conceived as ways of improving and strengthening the SAS public management model. Here, we focus on changes in a particular aspect of public management policy—namely, in the structure of service provision: the creation of a network of new hospitals by the regional government, with unique characteristics, which was to coexist with SAS providers. This was a decentralized network of high resolution hospitals (Hospital Centres of High Resolution or CHAREs) that took on the legal status of state-owned companies. The aim of these hospitals, which are smaller than SAS hospitals, was to improve access to, and efficiency of, the healthcare system.
Which type of institutional change did this process involve? The answer is multifaceted. The legal status of state-owned company (and the resultant regulations) had been introduced during the 1990s. Formally, these regulations remained unchanged, although they were interpreted and enacted in new ways. It was decided that the CHAREs would organically depend on the Department of Health—just like the existing state-owned companies—and not on the SAS, a decision that reinforced the government's general aim of separating, at least in part, the functions of these two organizations.
The Department of Health gained greater political visibility in the general governance of the healthcare system with its planning and contracting functions, while healthcare provision was centered at SAS, state-owned companies and certain state-subsidized centers. In turn, the decision to develop the CHAREs network under the legal status of state-owned companies reflected the need to improve the efficiency of the public system. Policymakers interviewed for this study conceived and justified this choice as an alternative to cooperation with private centers. According to a former senior politician of the Andalusian government interviewed, “We have developed CHAREs; we have demonstrated that private management is not more efficient than public management.”
However, the development of this network of unique hospitals can also be explained by the conditions of the policy sector itself, interpreted as problems to be resolved: the expansion and territorial dispersion of the population with consequent difficulties in access to specialized care, high hospitalization costs, and the need to speed up diagnoses and care. From this perspective, the establishment of the CHAREs reflected a layering process (Mahoney and Thelen, 2010): a new type of hospital complemented the existing healthcare system. New rules were linked to existing ones, bringing substantial change to the institution but without removing the old regulations. In fact, the Andalusian government continued to construct different types of hospitals that organically depend on SAS.
Explaining institutional change: Political context, institutions, and agents
As we have pointed out, the Andalusian political context, where only a few veto points exist and where the institution offers a significant amount of discretion for actors to interpret and implement rules, conditioned the development of the CHAREs network. From this perspective, we observe a conversion process, where the interpretation of existing institutional rules—the status of the state-owned company—involved a change in the order of the healthcare system as a whole. In fact, it is important to highlight that the new hospitals did not take on their own, separate legal personality, but rather attached themselves to existing state-owned companies.
That said, who were the agents triggering the change? Mainly, they were senior actors in the Andalusian government, including the Andalusian President and those at the highest levels in the Department of Health. Mahoney and Thelen (2010) refer to these actors as opportunists, mainly because they have ambiguous preferences about institutional continuity. The CHAREs network was at the same time an opportunity to reinforce—and complete—the model of direct public service provision, as well as to drive changes in the global governance of the healthcare system. At the same time, it is important to bear in mind that the concept of the state-owned company has become increasingly ambiguous since its introduction in Andalusia in the 1990s: it implies greater administrative flexibility but also allows a certain level of political control. 6
Thus, institutional challengers did not need to pursue insurrectionary strategies. In this sense, the creation of these new hospitals was not faced with any great opposition. This was because, on the one hand, certain actors who could see their interests displaced—such as the private sector—did not have sufficient veto power. On the other hand, in a context of an expanding economy and public expenditure—“a period of implementation of new services,” according to a former senior politician from the Andalusian government interviewed for this study—it became difficult to openly oppose the creation of new hospitals. 7 As can be interpreted from our interviews to Andalusian top officials, one of the few groups of actors with significant veto power in the healthcare system, the unions, was a defender of the status quo and a potential symbiont, but did not oppose this project on the condition that it would not change institutional rules. The process did not lead to the unionization of healthcare workers but rather to the creation of new jobs. In addition, it was a gradual, diluted change that foresaw the construction of the hospital network spanning over the whole decade. This construction is in fact still in progress, with some projects currently halted.
Finally, it is worth noting that this process of institutional change did not evolve in isolation from other modifications. The senior levels of the Andalusian government were not the only agents involved in these changes. During the 1990s, and before the unions gained significant veto power, global changes in SAS were explored and ruled out, such as, for example, the conversion of the organization into a state-owned company—a public firm, like ICS since 2007. In that context, agents with considerable professional scope in the health arena—for example senior politicians, but above all, managers—disguised the extent of their preferences for change, instead working within the system and adopting the role of subversives (Mahoney and Thelen, 2010). These actors accepted the development of the CHAREs network while also driving institutional change in the health system as a whole and, more specifically, in SAS. Among these changes, the introduction of a quality strategy, a model of clinical management, and a new labor policy are particularly noteworthy. As a former senior politician from the Andalusian government acknowledged when interviewed for this study, they were “working as if SAS was a state-owned company and taking advantage of the legal weaknesses that would allow us to keep going ahead.” 8
In short, institutional change in Andalusia was perceived by the actors involved as a process of relegitimization of the public healthcare system in the face of a particular context. Until the year 2001, economic resources for healthcare came from a specific state subsidy that was not part of the general model of regional financing. From that year onward, and with the transfer of healthcare competencies to the ACs that still had not taken them on, hear-marked funding for health disappeared and the corresponding resources were integrated into the AC general funding. 9 As a result, the parliaments of each AC became responsible for deciding the percentage of resources that would be allocated to policies such as those of health.
In this context, during the first decade of the 2000s, the issue image of institutional change in public healthcare management in Andalusia combined the promotion of a quality, public, direct provision system with the help of political autonomy—that is organizational innovation, ideological positioning, and separation of competencies from the central government. According to top officials interviewed for this research, it is crucial to remember that health policy is perceived by Andalusian policymakers as one of the policies that most influences the electorate and as an element of acceptance of a territorial identity that is historically associated with a lack of innovation and economic development.
Comparing institutional and policy change in Catalonia and Andalusia: The role of agents and their strategies
Mahoney and Thelen's (2010) theoretical model has helped us to interpret the roles played by change actors, their strategies, and the type of institutional change that came about in the public management policy in healthcare in Catalonia and Andalusia over the first decade of the 2000s. However, as previously shown in Table 1, the variables identified by Mahoney and Thelen as relevant for explanation (external actors' veto possibilities, level of discretion in rules interpretation and/or enforcement within the targeted institution, and actors' roles and strategies) are conceptualized into a classification that provides little room for a dynamic explanation. Our analysis, though, has led us to go beyond a static interpretation of this model's main theoretical layout.
The two cases analyzed here provide insights into additional relevant factors that may complement the explanatory power of Mahoney and Thelen's model. First, our analysis shows that actors' roles are not to be taken for granted just because of the institutional bias inbuilt in their organizational or institutional position, instead, other features such as preferences, ideology, or formative background may be as influential. Second, this study shows that actors' veto possibilities are not an invariable feature but can be modified—strengthened or weakened—either by themselves or by other actors. Third, this analysis shows that the level of discretion in rule interpretation or enforcement is not an objective feature, but a matter of actors' perception, which may in turn influence the roles and strategies they are prepared to play and develop. Thus, this study shows that we need to go beyond interpreting change roles and strategies in order to understand the type of institutional change brought about. Instead, we need to account for how and why actors may shift between roles and strategies on the basis of how they perceive and relate not only with the contextual and the organizational variables but also with the other change actors.
Comparison of institutional and public management policy change in healthcare in Catalonia and Andalusia, 1998–2007
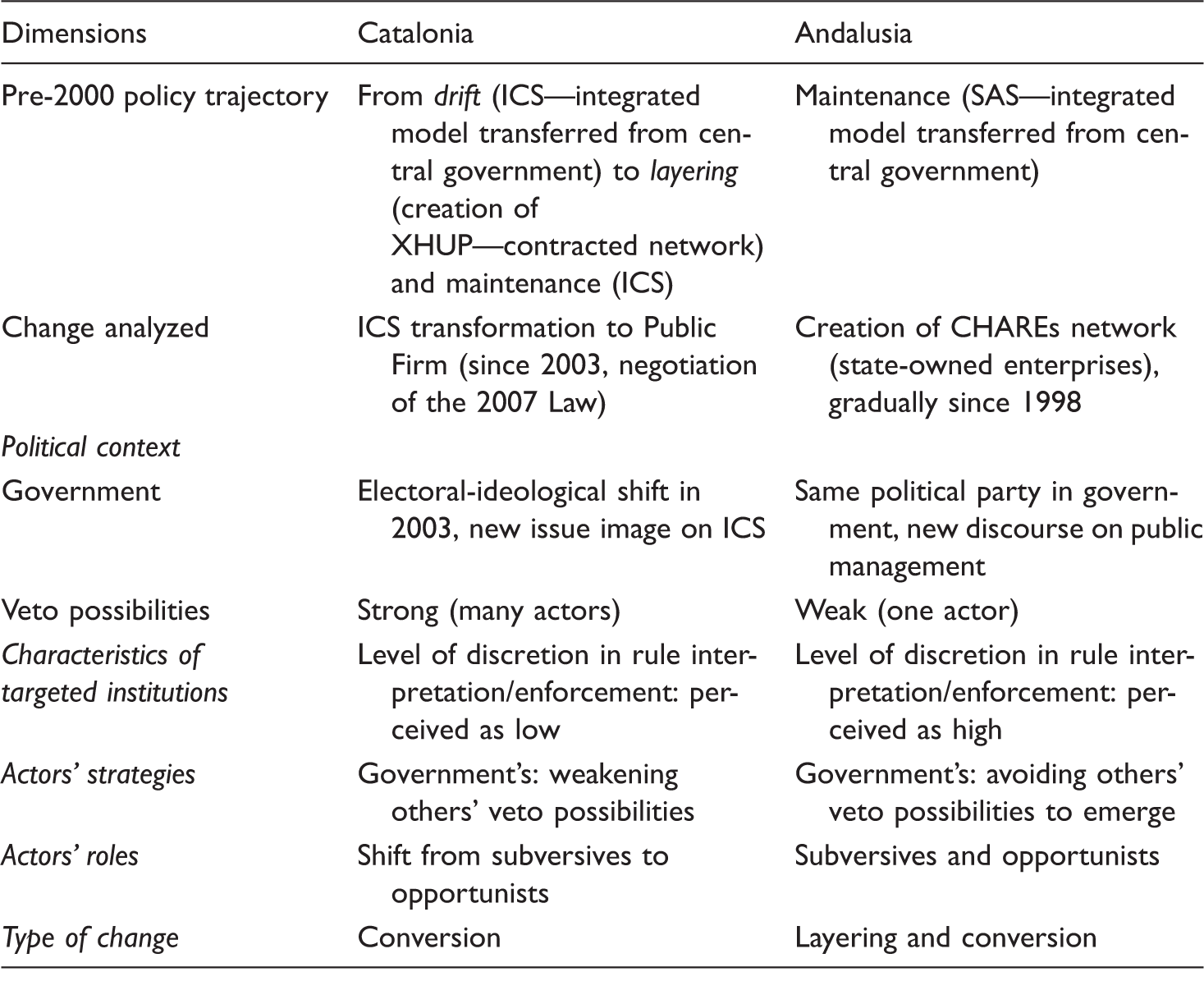
Source: Own elaboration.
As stated before, the institutional setting in which the change analyzed here took place was similar in both ACs, that is the regional political institutions and the organizational and management structures of ICS and SAS, which were transferred to them by the central government, were originally similar. Both ICS and SAS were to initially be the bases of their regional health systems. However, the public management policy trajectories followed by the Catalan and the Andalusian governments in relation to these institutions, previous to 2000, consolidated different scenarios in terms of resource distribution among public and private actors, network relations among them, and actors' prevailing discourses and normative assumptions—namely, what Radaelli et al. (2012) refer as policy variables or characteristics of the policy sector. Thus, in the Catalan case, the level of discretion in rules interpretation and enforcement had come to be perceived to be low—the possibilities for management improvement within the ICS inherited management model were openly questioned. By contrast, in the Andalusian case, the possibility for improving the SAS management was part and parcel of the defense of the public health sector—thus the level of discretion in rules interpretation and enforcement was perceived as high.
In this context, as Table 2 shows, while the new Catalan government pursuing change was faced with strong veto possibilities from many external actors, the Andalusian government was faced with weak veto possibilities—potentially strong from only one actor, namely, the unions. Change actors' strategies in the Catalan case were geared to weaken veto possibilities from the rest of actors—Department of Economy, unions, local governments, contracted providers, other political parties, etc., whereas change actors in the Andalusian case sought to minimize the possibilities that the only actor that could oppose change—the unions—could perceive any threat in the reform. In the Catalan case, governmental change actors shifted roles from subversives (while pursuing layering in the previous phase) to opportunists and achieved conversion as type of change in 2007. In the Andalusian case, governmental change actors simultaneously performed subversive and opportunist roles and achieved layering and conversion as types of institutional change.
This comparative analysis supports Mahoney and Thelen's argument that the characteristics of the political context (veto possibilities) and characteristics of the targeted institutions (level of discretion in rules interpretation and enforcement) did condition change actors' roles and strategies in these two cases, thus explaining why a particular type of change was achieved. However, this analysis also shows that actors' roles and corresponding strategies are not necessarily biased in a particular direction by the institutional or organizational position they hold—such as, Minister of Economy, Minister of Health, manager, etc. Instead, their profile—namely, past experience, formative background, ideology, and perceptions—may explain their roles and strategies to a large extent. This analysis also shows that actors may not only shift between roles but also try to change other actors' roles by deliberately changing their perception of the relevant variables in the model. Last, this analysis shows that veto possibilities and level of discretion are not objective factors—as they can be perceived differently by different actors, or invariable factors—as they can be modified.
Conclusions
This analysis of cross-regional policy variation in Spain has focused on two cases of institutional change that involved a redefinition of the public management policy in the health sector in Catalonia and Andalusia. The study shows how, within similar institutional and organizational frameworks, governments may pursue divergent policy options. These case outcomes are partly explained by policy sector-specific variables that these exploratory case studies have shown to be analytically relevant: the relative weight of private and public provision, the number and characteristics of pressure groups, and their relationship with the political elite. Both Catalonia and Andalusia show opposite characteristics in all of these variables and their governments have pursued different policy options, which would reinforce Radaelli et al.'s (2012) argument for policy divergence explanation.
However, this datum by itself does not mean that policy-sector characteristics are the causal link between institutional-level and policy-level variables. This analysis also shows the substantial influence of a non-sector-specific variable—namely, the political ideology of policymakers. Moreover, it is important to note that successive governments' and other actors' (in)actions have contributed to incrementally modify or intensify the characteristics of some of those policy sector-specific variables. Thus, the main explanatory factor of the type of change that comes about is the type of roles and strategies actors' pursue. This study confirms Mahoney and Thelen's (2010) point that the type of roles actors play and the strategies they follow are conditioned by contextual veto possibilities and by the degree of discretion in rule enforcement within the organizations that are the object of change. However, this analysis also provides evidence that it is the perception change actors have of these two variables what influences most of their entrepreneurial actions, and that such actions may change the nature of those variables—namely, veto possibilities and level of discretion.
Therefore, institutionally biased roles are not to be taken for granted. Instead, actors in the same institutional position may pursue different strategies depending both on their ideology or preferences and on their perception of factors relevant in the model (veto possibilities and level of discretion in rule interpretation or enforcement). For example, an actor may try to weaken or strengthen other actors' veto possibilities depending on how they perceived them to be or may pursue different change strategies depending on their perception of degree of discretion within the institution. This may be particularly relevant in decentralized states, such as Spain, where veto actors may be external to the immediate regional political system leading the change process. The central state government, for example, may not influence the regional change process directly, but regional change agents may build their own discourses and strategies on explicit references to the political contention about characteristics of the country's political and governmental systems.
Last, this study also shows that change actors may (un)intentionally weaken or strengthen veto possibilities of other actors, therefore paving the way for developing change strategies. Thus, Mahoney and Thelen's (2010) theoretical model would improve its causal argument by integrating a dynamic interpretation in the analysis of cases of incremental institutional and policy change. This approach would help understand how and why actors interact with relevant situational factors in a model of entrepreneurial strategy for institutional continuity or change. At the same time, it would allow to endogenize the dynamic evolution of contextual and institutional features into the analysis of the process of institutional and policy change.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript integrates findings from two research projects, one funded by the Spanish government (CSO-2011-27547) and one funded by the Catalan government (Ordre GRI/6/2012, Resolució 20 Juliol 2012).