
Abstract
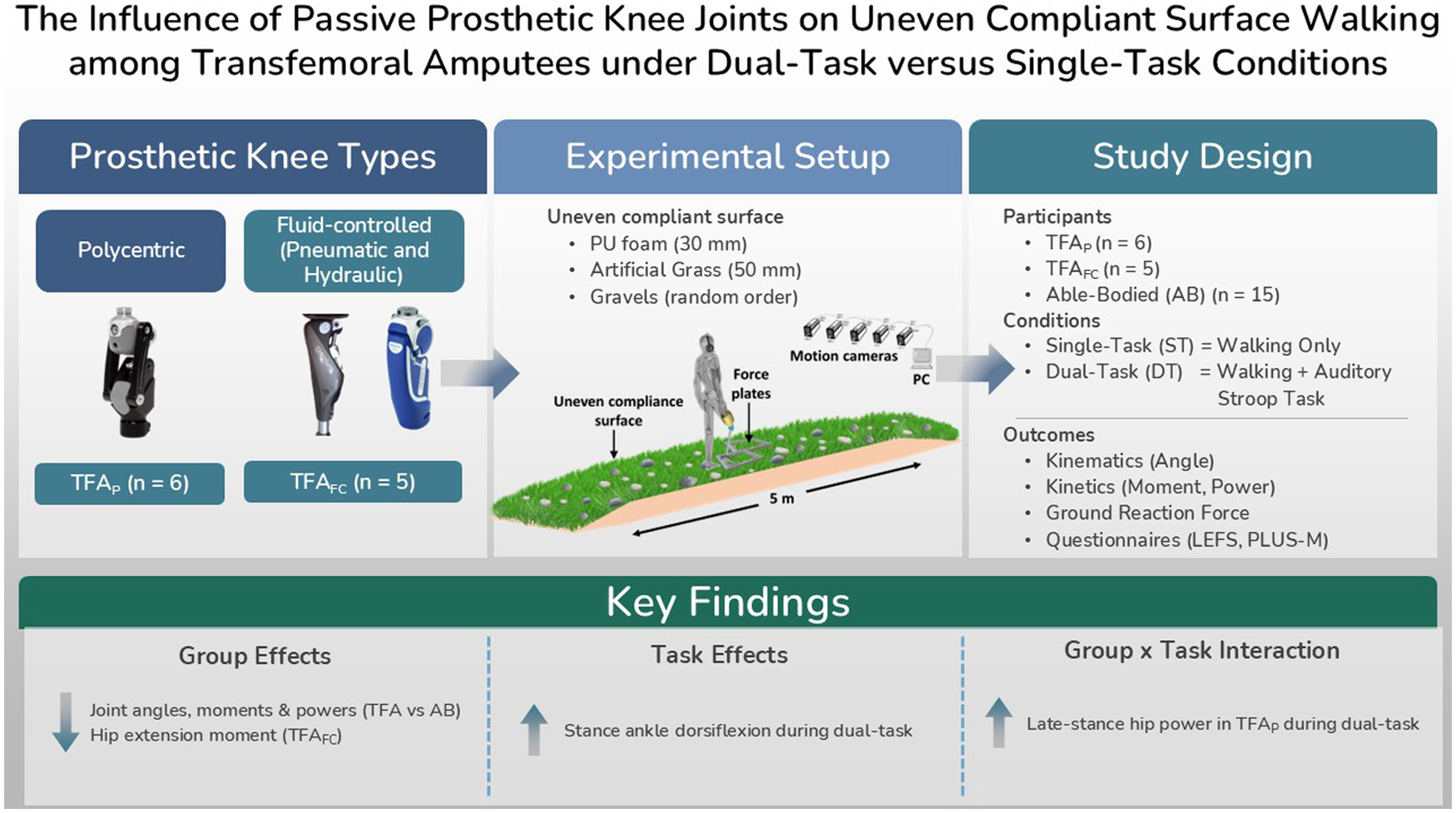
Individuals with transfemoral amputation (TFA) often experience gait adaptations when walking under environmental and cognitive challenges. This study examined the influence of passive prosthetic knee mechanisms on self-reported mobility and gait biomechanics during single-task and dual-task walking over an uneven compliant surface. Participants were grouped as able-bodied individuals (AB; n = 15), individuals with TFA using polycentric knees (TFAP; n = 6), and individuals with TFA using fluid-controlled knees (TFAFC; pneumatic/hydraulic; n = 5). The dual-task condition involved walking while performing an auditory Stroop task. Outcome measures included self-report questionnaires, joint kinematics, joint kinetics, and ground reaction forces. Biomechanical variables were analysed using linear mixed-effects models to examine group, task, and group × task interaction effects. Self-reported outcomes indicated reduced functional mobility in individuals with TFA compared with AB. Biomechanical findings showed altered gait patterns in both TFA groups compared with AB, particularly reduced knee flexion and ankle plantarflexion. For kinetic outcomes, significant group effects were observed for selected joint moment and power variables, although Bonferroni-adjusted pairwise differences were identified only for maximum stance hip extension moment (HM1), with lower values in TFAFC compared with AB. A significant task effect was observed for maximum stance ankle dorsiflexion (AA2) during dual-task walking across all groups. A significant group × task interaction was found for maximum hip eccentric power during late stance (HP2), with increased hip power during dual-task walking in TFAP. Overall, passive prosthetic knee mechanisms showed limited differences, although task-specific adaptations were evident under combined uneven surface and cognitive demands.
Keywords
Background
Walking is a fundamental activity used to assess functional mobility and overall health. Individuals with transfemoral amputation (TFA) experience significant challenges following limb loss due to the absence of biological knee and ankle function. Individuals with TFA rely on compensatory muscle and joint function to generate movement and maintain gait. 1 Prosthetic knee devices with various functional features have been developed to mitigate these impairments and improve gait performance. 2
Despite these advancements, individuals with TFA exhibit characteristic gait adaptations compared with able-bodied (AB) individuals, including reduced knee flexion during swing, diminished ankle push-off power, and increased reliance on proximal joints, particularly the hip, to generate propulsion. 3 These adaptations are strongly influenced by the mechanical behaviour of the prosthetic knee, which plays a central role in controlling stance stability and swing-phase motion and shaping overall lower-limb biomechanics.
Environmental and cognitive factors further influence gait performance. Walking on uneven terrain introduces unpredictable perturbations that require continuous adjustments to maintain balance and forward progression.4,5 In addition, walking requires cognitive resources for maintaining balance and coordinating movement. When an additional cognitive task is introduced, attentional resources must be divided, leading to dual-task interference that can alter gait performance. Individuals with TFA may be particularly susceptible to these effects due to reduced sensory feedback and increased reliance on active control of the prosthetic limb. The auditory Stroop task is commonly used in dual-task gait studies, as it imposes executive cognitive demands while minimising visual interference during walking and has been shown to induce cognitive–motor interference.6–8
Previous studies have shown that dual-task walking affects gait performance in individuals with lower-limb amputation, including reductions in walking speed and changes in gait variability.7,9,10 However, findings across studies remain variable and are often dependent on the type of secondary task and outcome measures used. While dual-task paradigms such as the auditory Stroop task have demonstrated good reliability in gait studies, 8 most research in individuals with amputation has primarily focussed on spatiotemporal parameters, providing limited insight into joint level biomechanical adaptations and failing to fully capture the complexity of gait adaptation under different environmental conditions.
More recent work has also largely focussed on spatiotemporal measures such as walking speed, cadence, and stride characteristics.11,12 Consequently, the underlying biomechanical mechanisms of gait adaptation are not yet fully understood. In particular, few studies have examined both kinematics and kinetics, especially in relation to prosthetic knee function. Furthermore, the combined effects of cognitive load and environmental challenges, such as walking on uneven surfaces, remain insufficiently explored.
Prosthetic components, particularly knee mechanisms, play a crucial role in determining gait performance.13,14 Although individuals with higher functional levels may achieve walking speeds comparable to able-bodied individuals, 15 biomechanical differences remain evident. As the prosthetic knee regulates limb support and progression, its mechanical properties influence movement across the entire lower limb, with changes at the knee closely linked to compensatory adjustments at the hip and ankle. In addition, walking on uneven terrain further alters gait kinematics, kinetics, and stability, and these effects may be amplified under dual-task conditions. 16 Experimental uneven terrain walkways are commonly used to simulate real-world environments and assess locomotor adaptations.17–19
The selection of prosthetic knee components is often influenced by economic and practical considerations. While microprocessor-controlled knees offer advanced functionality, their high cost may limit accessibility.20,21 As a result, passive prosthetic knees remain widely used in clinical practice.
To address these gaps, the present study investigates how different passive prosthetic knee mechanisms influence joint level gait biomechanics during combined cognitive and environmental challenges, specifically single-task and dual-task walking over uneven surfaces in individuals with TFA. By integrating kinematic and kinetic analyses, this study provides insight into adaptive strategies beyond conventional performance measures and advances understanding of prosthetic knee function in real-world walking conditions.
Materials and methods
Participants
This study used convenience sampling and included 11 individuals with TFA and 15 AB participants. All participants were aged 18 years or older, able to walk independently without assistive devices, and had no neurological or musculoskeletal conditions affecting gait. Inclusion criteria for the TFA group required unilateral amputation and the use of a passive prosthetic knee for at least 6 months.
The TFA group was categorised into polycentric knee users (TFAP, n = 6) and fluid-controlled knee users (pneumatic or hydraulic; TFAFC, n = 5). The sample size was determined based on participant availability during the recruitment period, which is common in studies involving clinical populations with specific inclusion criteria. Recruitment of individuals with TFA is often limited due to the relatively low prevalence and strict eligibility requirements.
Participants completed the Lower Extremity Functional Scale (LEFS) and Prosthetic Limb Users Survey of Mobility (PLUS-M). Ethical approval was obtained from the Medical Research and Ethics Committee (MREC; KKM/NIHSEC/P19-2206(11)), and all participants provided informed consent.
Prosthetic components
Prosthetic knees were categorised as polycentric or fluid-controlled based on their mechanical characteristics. All participants with TFA used their own prosthetic limbs, which had been fitted and aligned by certified prosthetists according to standard clinical procedures. The present study specifically focussed on the type of prosthetic knee joint, while other components such as socket design and suspension systems were not included in the analysis.
Experimental setup
Data were collected in a single laboratory session using a motion capture system (Vicon Nexus, UK) synchronised with two force plates (Kistler, Switzerland) embedded in a 5 m walkway. Sixteen retroreflective markers were placed on predefined lower-limb locations, with additional markers on the prosthetic components for the TFA group.
A custom uneven surface was constructed using polyurethane foam (30 mm; 65 kg/m3), covered with artificial grass (50 mm) and randomly distributed gravel to simulate irregular outdoor walking surfaces. 17
Cognitive tasks
An auditory Stroop task was used as the dual-task condition. The stimuli were generated using PsychoPy software (Version 3.1.5, UK). Participants listened to the words “low” and “high,” presented in either low or high pitch through a Bluetooth headset (Sony CH5100, Japan), and were instructed to verbally identify the pitch as quickly and accurately as possible. This task imposes executive cognitive demands while minimising visual interference and is commonly used to assess cognitive–motor interference during walking. 6 In addition, auditory Stroop tasks primarily engage executive control processes, including attention and response inhibition, which are associated with activation of the prefrontal cortex and anterior cingulate cortex. Compared with visually based tasks, the auditory modality reduces interference with visual feedback required for safe locomotion, making it suitable for dual-task gait assessments.
Walking protocol
Participants performed walking trials under two conditions: single-task (ST) and dual-task (DT). All trials were conducted at a self-selected walking speed along the uneven walkway. Each participant completed at least three successful trials per condition. Trials were considered successful when natural walking was achieved with full foot contact on the force plates. Additional trials were performed if necessary. Task order was randomised.
Outcome parameters
Kinematic and kinetic data were sampled at 100 and 1000 Hz, respectively. Kinetic variables were normalised to body weight. Outcome measures included joint angles (degrees), moments (Nm/kg), and powers (W/kg) of the hip, knee, and ankle, as well as ground reaction forces (N/kg) during the stance phase.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics (version 27.0, IBM Corp., Armonk, NY, USA). Descriptive statistics are presented as mean ± standard deviation for each group and task condition. Non-parametric tests (Kruskal–Wallis and Mann–Whitney U) were used for questionnaire data (LEFS and PLUS-M) due to the ordinal nature and non-normal distribution of the data. These tests are appropriate for small sample sizes and are robust to unequal group sizes.
A linear mixed-effects model (LMM) was used to examine the effects of group (able-bodied (AB), individuals with TFA using polycentric knees (TFAP), and individuals with TFA using fluid-controlled knees (TFAFC)) and task condition (single-task (ST) and dual-task (DT)) on each biomechanical variable. Group and task were included as fixed effects, and participant was treated as a repeated factor to account for within-subject variability.
This approach was selected instead of traditional repeated-measures ANOVA, as it is more suitable for unequal group sizes and does not require assumptions such as sphericity. It also allows both group-level and individual-level effects to be considered and handles repeated measurements more flexibly.22,23 A compound symmetry covariance structure was applied, and parameter estimation was performed using Restricted Maximum Likelihood (REML) with Satterthwaite approximation for degrees of freedom.
Main effects of group and task, as well as the group × task interaction, were evaluated for each dependent variable, with post hoc pairwise comparisons performed using Bonferroni adjustment when appropriate. For significant interaction effects, additional analyses were conducted to examine differences between groups within each task condition and differences between task conditions within each group. Model assumptions, including normality and constant variance of residuals, were assessed by examining residual plots. Statistical significance was set at p < 0.05.
Results
Participants
Eleven individuals with TFA (all male; age 29.4 ± 6.1 years; height 170.3 ± 5.8 cm; mass 72.2 ± 17.6 kg) participated, with a mean time since amputation of 4.6 ± 2.4 years. The AB group included 15 participants (8 males, 7 females; age 29.3 ± 5.3 years; height 163.8 ± 9.2 cm; mass 79.7 ± 20.8 kg). A significant difference in BMI was observed between groups (p = 0.036; Table 1).
Means, standard deviations, and p-value of participant demographics.
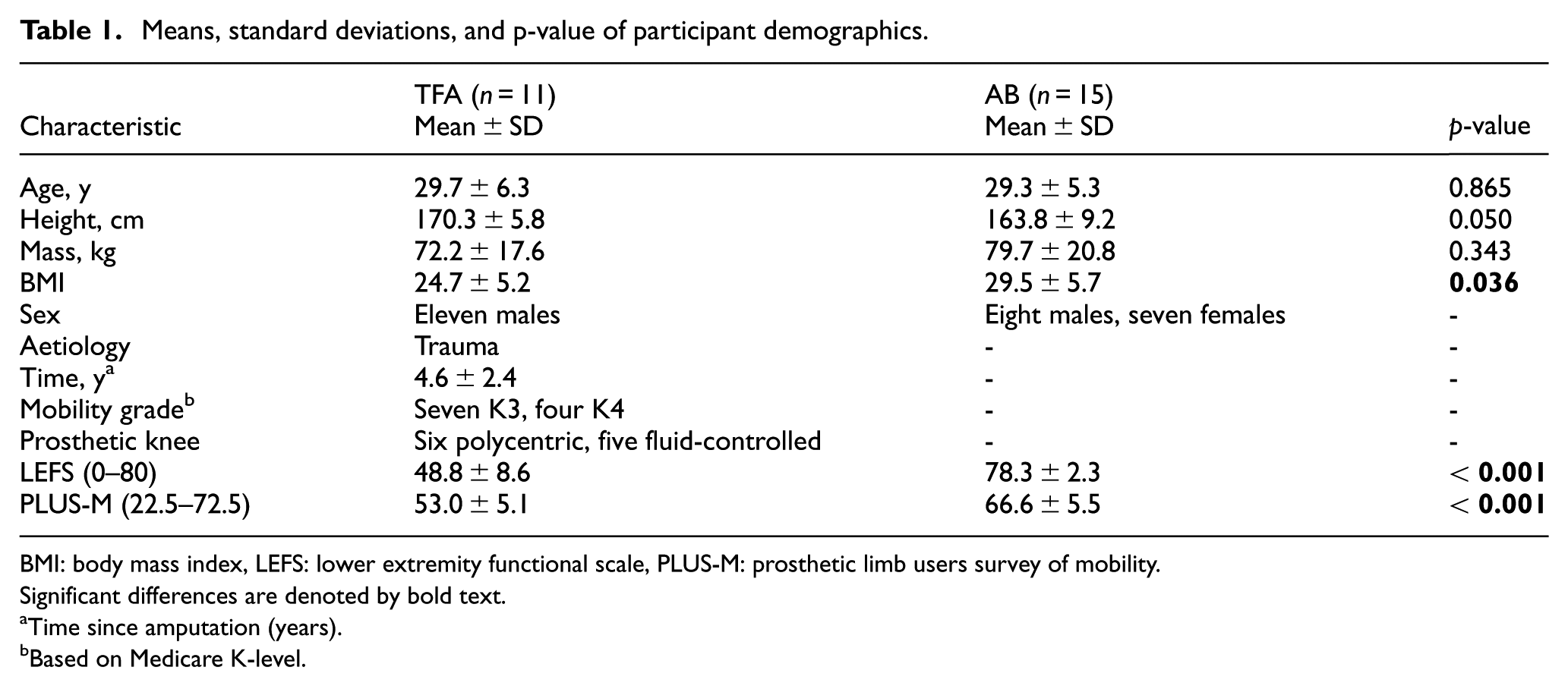
BMI: body mass index, LEFS: lower extremity functional scale, PLUS-M: prosthetic limb users survey of mobility.
Significant differences are denoted by bold text.
Time since amputation (years).
Based on Medicare K-level.
Self-report measurement outcomes
Self-report measures using LEFS and PLUS-M revealed that the TFA group had significantly lower scores (all p < 0.001) than AB respondents.
Kinematic joint angle outcomes
For kinematic outcomes, significant main effects of group were observed for maximum stance knee flexion (KA1; F(2, 23) = 38.091, p < 0.001) and maximum swing knee flexion (KA2; F(2, 23) = 11.723, p < 0.001). Both TFA groups demonstrated significantly reduced values compared to the AB group (p < 0.001), with no significant differences between prosthetic knee types (p = 0.371 and p = 1.000, respectively).
Similarly, a significant group effect was found for maximum swing ankle plantarflexion (AA3; F(2, 23) = 5.933, p = 0.008), with both TFA groups showing reduced values compared to the AB group (p< 0.05), and no significant differences between prosthetic groups. No significant task or interaction effects were observed for these variables. A significant main effect of task was observed for maximum stance ankle dorsiflexion (AA2; F(1, 23) = 5.089, p = 0.034), with higher values during dual-task walking compared with single-task walking across all groups.
Kinetic joint moment and power outcomes
Significant main effects of group were observed for selected kinetic variables. For maximum stance hip extension moment (HM1), there was a significant main effect of group (F(2, 23) = 4.565, p = 0.021). Bonferroni-adjusted pairwise comparisons showed that the TFAFC group had significantly lower HM1 compared with the AB group. No significant differences were found between the TFAP and AB groups, or between the TFAP and TFAFC groups.
A significant main effect of group was also observed for maximum stance knee flexion moment (KM2; F(2, 23) = 4.401, p = 0.024). However, Bonferroni-adjusted pairwise comparisons did not show significant differences between specific group pairs. The pairwise comparisons were AB versus TFAP (p = 0.080); AB versus TFAFC (p = 0.082); and TFAP versus TFAFC (p = 1.000). Therefore, KM2 showed an overall group effect, but no specific between-group difference was identified after adjustment. A significant main effect of group was also observed for maximum ankle plantarflexion moment (AM2; F(2, 23) = 4.635, p = 0.020). However, Bonferroni-adjusted pairwise comparisons did not identify significant differences between specific group pairs (Figure 1).
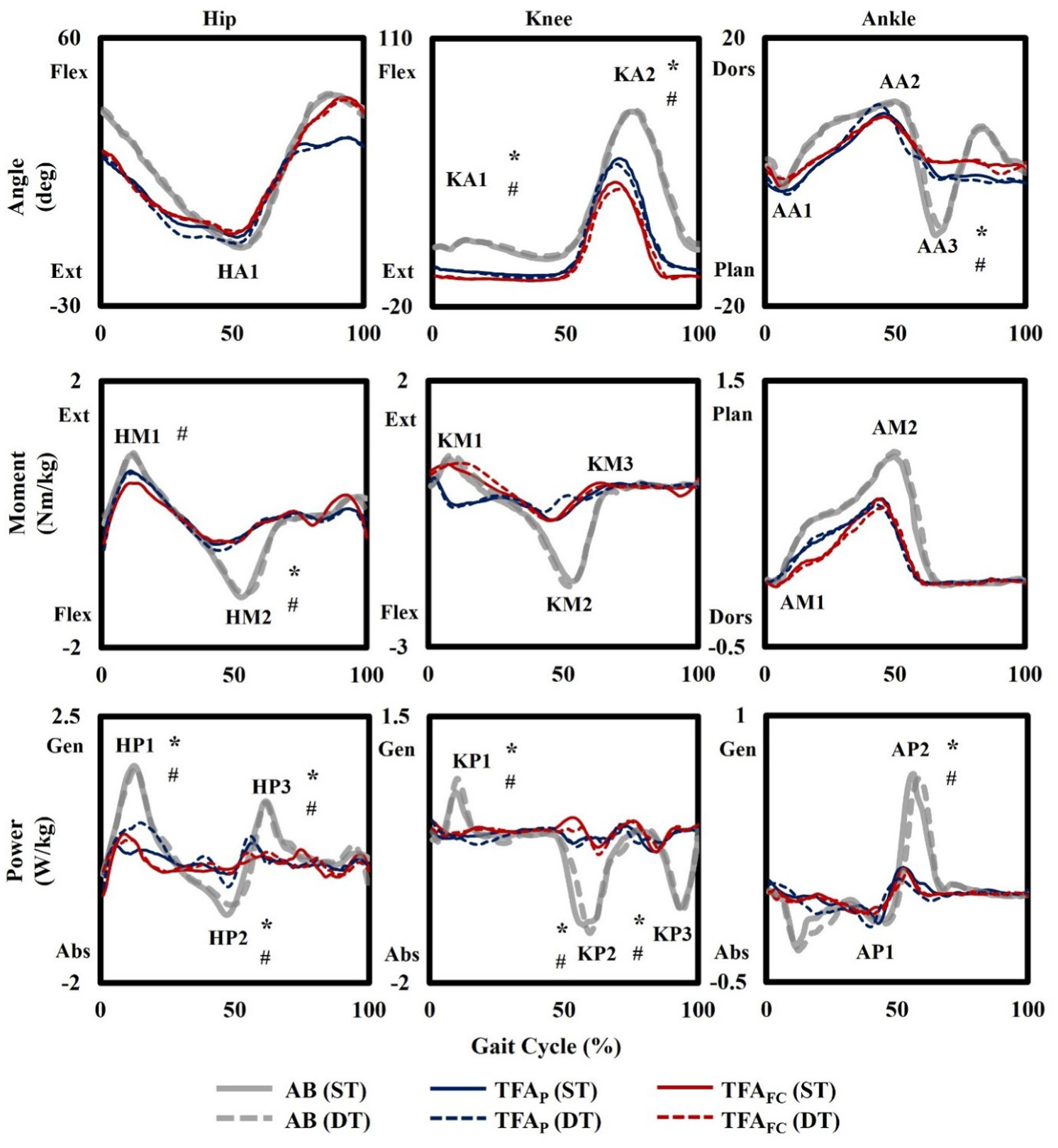
The figure above shows the comparison of the kinematics and kinetics of the prosthetic leg for the polycentric group (TFAP; blue, solid/dash), the fluid-controlled group (TFAFC; red, solid/dash), and the able-bodied group (AB; light grey, solid/dash) during single-task (ST, solid line) and dual-task (DT, dash).
For maximum late stance hip eccentric power (HP2), a significant main effect of group was observed (F(2, 23) = 11.834, p < 0.001). The main effect of task was not significant (F(1, 23) = 0.457, p = 0.506). However, a significant group × task interaction was observed for HP2 (F(2, 23) = 3.739, p = 0.039). Post hoc analyses showed that HP2 increased significantly during dual-task walking compared with single-task walking in the TFAP group (p = 0.019). No significant differences between task conditions were found in the AB group (p = 0.294), or the TFAFC group (p = 0.246).
Overall, the kinetic results showed a clear pairwise group difference for HM1, an overall group effect for KM2 without significant pairwise differences, and a significant group × task interaction for HP2. The task-related change in HP2 was evident only in the TFAP group.
Vertical ground reaction force outcomes
No significant effects between groups and tasks were observed in all conditions (Table 2). The vGRF patterns of all groups showed the typical M-shape. From the analysis, all groups had a greater impact peak (FZMax1) than the active peak (FZMax2) in all conditions. The TFAP group obtained an impact peak (FZMax1) at 40% of the stance cycle. FZMax1 in the TFAP group was greater than in the TFAFC and AB groups. However, these differences were not statistically significant (Figure 2).
Means, standard deviations, and statistical results of dual-task gait for kinematics, kinetics, and vertical ground reaction forces.
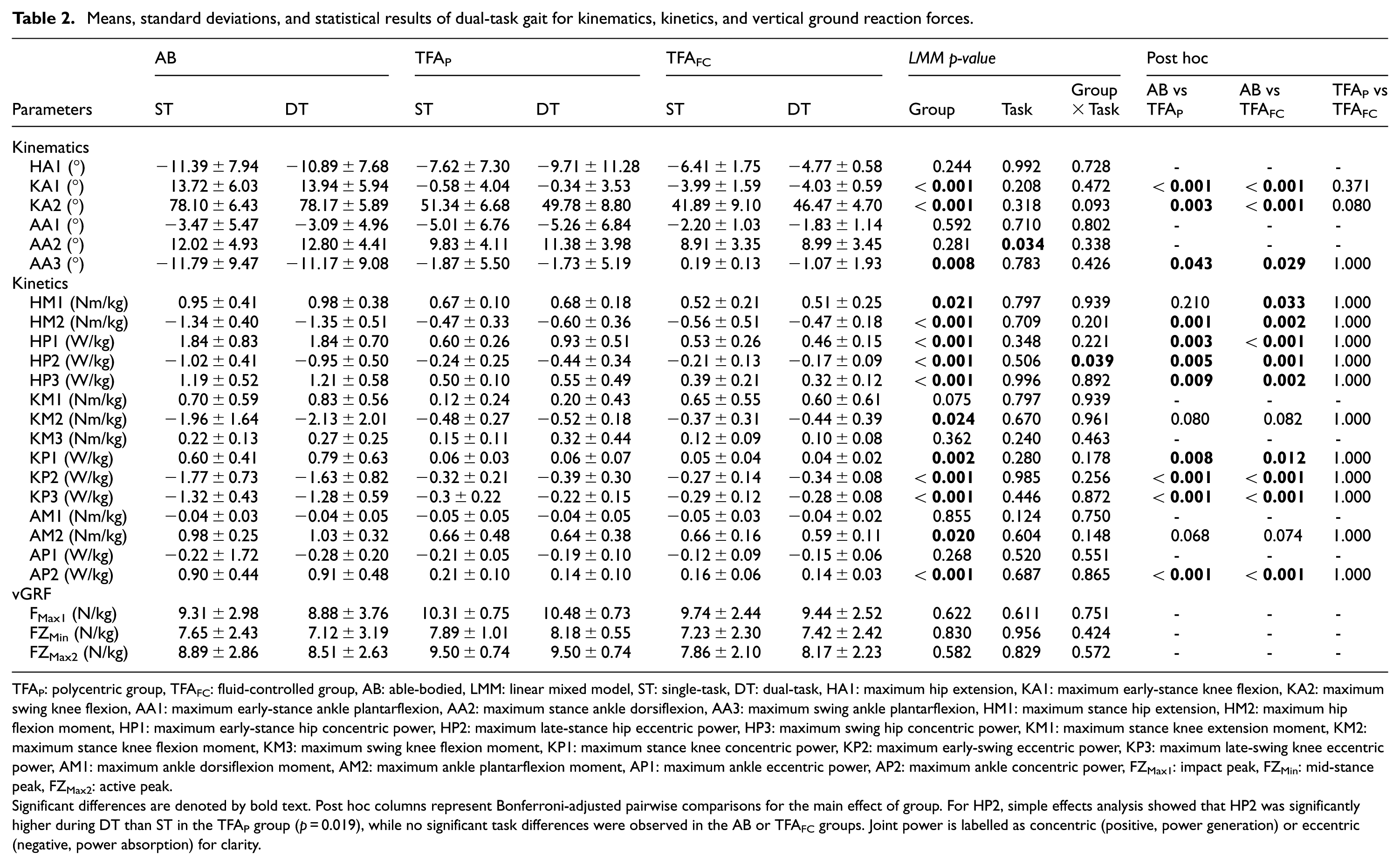
TFAP: polycentric group, TFAFC: fluid-controlled group, AB: able-bodied, LMM: linear mixed model, ST: single-task, DT: dual-task, HA1: maximum hip extension, KA1: maximum early-stance knee flexion, KA2: maximum swing knee flexion, AA1: maximum early-stance ankle plantarflexion, AA2: maximum stance ankle dorsiflexion, AA3: maximum swing ankle plantarflexion, HM1: maximum stance hip extension, HM2: maximum hip flexion moment, HP1: maximum early-stance hip concentric power, HP2: maximum late-stance hip eccentric power, HP3: maximum swing hip concentric power, KM1: maximum stance knee extension moment, KM2: maximum stance knee flexion moment, KM3: maximum swing knee flexion moment, KP1: maximum stance knee concentric power, KP2: maximum early-swing eccentric power, KP3: maximum late-swing knee eccentric power, AM1: maximum ankle dorsiflexion moment, AM2: maximum ankle plantarflexion moment, AP1: maximum ankle eccentric power, AP2: maximum ankle concentric power, FZMax1: impact peak, FZMin: mid-stance peak, FZMax2: active peak.
Significant differences are denoted by bold text. Post hoc columns represent Bonferroni-adjusted pairwise comparisons for the main effect of group. For HP2, simple effects analysis showed that HP2 was significantly higher during DT than ST in the TFAP group (p = 0.019), while no significant task differences were observed in the AB or TFAFC groups. Joint power is labelled as concentric (positive, power generation) or eccentric (negative, power absorption) for clarity.
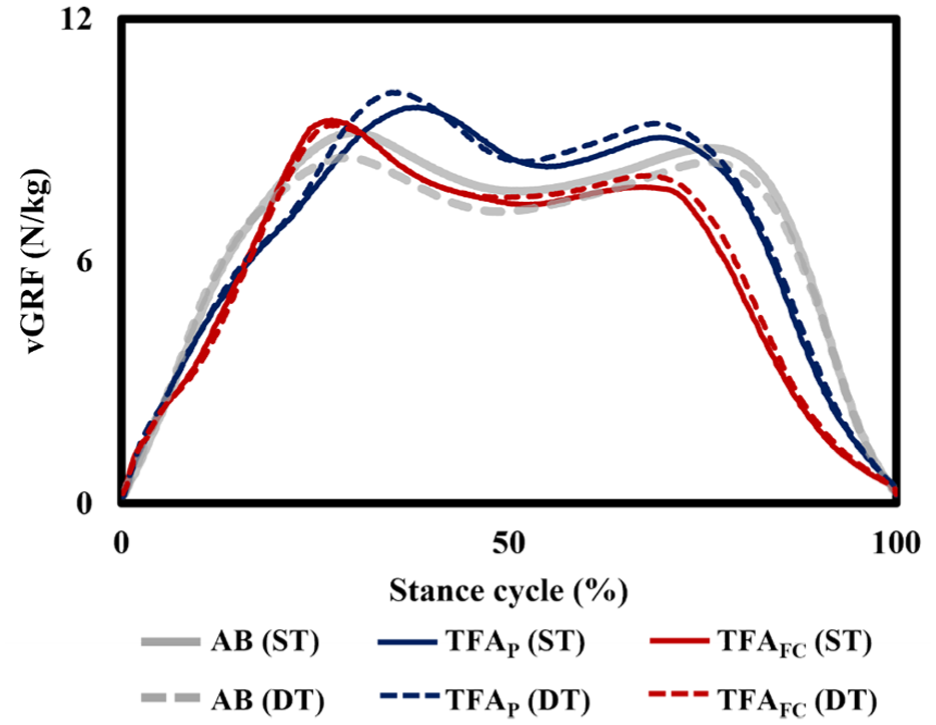
Vertical ground reaction forces (vGRF) of the polycentric (TFAP; blue, solid/dash), fluid-controlled (TFAFC; red, solid/dash), and able-bodied (AB; light grey, solid/dash) groups during single-task (ST, solid line) and dual-task (DT, dash).
Discussion
The present study investigated the influence of passive prosthetic knee mechanisms on gait biomechanics during single-task and dual-task walking over an uneven surface in individuals with TFA, compared with the AB group. The findings suggest that gait differences are primarily driven by amputation-related biomechanical constraints, with prosthetic knee type having a limited influence, while certain parameters are affected by cognitive demand and its interaction with prosthetic design.
Consistent with previous literature, individuals with TFA demonstrated altered gait patterns compared to the AB group, particularly in joint kinematics and kinetics. These differences are expected due to the loss of active biological knee and ankle function on the amputated limb, resulting in reduced joint motion and diminished power generation.1,3,13 Previous dual-task studies have largely focussed on spatiotemporal parameters,7,9 whereas the present study expands on this by examining joint level kinematic and kinetic responses during uneven surface walking with added cognitive demand. Furthermore, individuals with TFA have been shown to modify their gait across different walking tasks, indicating that task demands can influence gait adaptation in this population. 24
A significant main effect of group was observed for several kinematic variables, including maximum stance knee flexion (KA1), maximum swing knee flexion (KA2), and ankle plantarflexion (AA3), with both TFA groups demonstrating reduced values compared to the AB group. Reduced swing knee flexion reflects limitations in achieving sufficient limb shortening for toe clearance, while reduced ankle plantarflexion is consistent with diminished push-off capability. As a result, individuals with TFA may rely more on proximal joints, particularly the hip, to compensate for reduced function at the knee and ankle.1,3,13 Similarly, reduced stance knee flexion may reflect a more extended knee posture during weight acceptance to enhance stability. 3
No significant differences were observed between the TFAP and TFAFC groups across these kinematic variables. Although previous work has shown that prosthetic knee type may influence gait kinematic patterns in individuals with transfemoral amputation, 25 the present study did not detect significant kinematic differences between TFAP and TFAFC. This suggests that, despite differences in mechanical design, both passive prosthetic knee mechanisms may provide broadly comparable kinematic performance during walking in the present study. The absence of differences may be related to the passive mechanical nature of both systems, where gait performance remains influenced by prosthetic knee stance-control characteristics and user adaptation during loading and unloading phases of gait. 26 Nevertheless, the relatively small and functionally similar sample of participants may have reduced the ability to detect subtle differences between prosthetic knee types.
A significant main effect of task was observed for maximum stance ankle dorsiflexion (AA2), with higher values during dual-task walking across all groups. This indicates that the addition of cognitive demand influences ankle behaviour in a consistent manner regardless of prosthetic use. Increased dorsiflexion during stance may represent a cautious gait strategy to enhance stability and foot clearance, particularly when attentional resources are divided and when walking on uneven surfaces. This finding suggests that ankle level adaptations may reflect a general response to cognitive and motor interference, rather than changes related to a specific prosthetic knee mechanism.7,9
The kinetic results showed differences across groups in selected joint moment and power outcomes, although these differences were not consistently reflected in the pairwise comparisons. For maximum stance hip extension moment (HM1), lower values in the TFAFC group compared with AB group suggest altered hip joint kinetics during stance, consistent with kinematic differences observed across several joint angles, reflecting altered lower limb control and compensatory strategies.1,3,13
For maximum stance knee flexion moment (KM2) and maximum ankle plantarflexion moment (AM2), significant overall group effects were observed. However, pairwise comparisons with Bonferroni adjustment did not identify significant differences between specific group pairs. This suggests that KM2 and AM2 varied across groups overall, but the differences were not strong enough to localise to specific group comparisons after adjustment. This may be partly explained by the small and unequal sample sizes and individual variability in prosthetic gait patterns.
The key kinetic finding was the significant group × task interaction for maximum hip eccentric power during late stance (HP2), indicating that the effect of dual-task walking differed between groups. Specifically, HP2 increased significantly during dual-task walking in the TFAP group, whereas no significant changes related to task condition were observed in the AB and TFAFC groups. Hip eccentric power during late stance may contribute to controlling limb progression and body stability before toe off, particularly when walking conditions become more demanding. The uneven compliant surface may have increased the demands on balance, limb placement, and motor control, making task-specific adaptations more apparent under dual-task conditions. Therefore, the increase in HP2 among TFAP users may reflect a task-specific adaptation to cognitive and motor interference during uneven surface walking, rather than a general difference between prosthetic knee types.7,9,24
Reduced ankle power generation during terminal stance (AA2) has been reported in individuals with transfemoral amputation, reflecting the limited ability of passive prosthetic components to reproduce physiological push-off. 3 This limitation may increase reliance on proximal joints, particularly the hip, for forward progression and stability. Although variations in ground reaction force patterns were observed, these did not reach statistical significance. This suggests that overall loading patterns were generally maintained, even though joint level biomechanical differences were present.
The limited differences between TFAP and TFAFC may also be explained by the passive mechanical nature of both systems. Unlike microprocessor-controlled knees, which can actively regulate stance phase knee resistance and have been reported to influence level walking mechanics in individuals with TFA, 27 passive prosthetic knees provide limited real-time adjustment. Although fluid-controlled knees are designed to provide smoother resistance and movement control, 28 these potential advantages may not have produced clear measurable differences under the combined demands of uneven surface walking and dual-task performance. Within the context of passive prosthetic systems, individual functional ability, prosthetic alignment, and compensatory movement strategies may have contributed substantially to the observed gait outcomes.
Several limitations should be acknowledged. First, the sample size of individuals with TFA was relatively small and unequal compared to the AB group, which may limit the generalisability and statistical power of the findings. Second, the study cohort consisted only of male participants with traumatic amputation and relatively high functional levels. Since physical performance may differ according to functional classification among unilateral lower-limb prosthesis users, 14 this relatively homogeneous sample may not represent the broader TFA population, particularly individuals with vascular conditions, lower functional levels, or higher comorbidities.
Although sex differences in spatiotemporal gait parameters have been reported in lower limb prosthesis users, evidence specific to dual-task gait adaptation in individuals with TFA remains limited. 29 Therefore, the absence of female participants limits the ability to explore potential sex-related differences in gait adaptation. Additionally, the control group was not sex-matched, which may influence gait characteristics. In line with the SAGER guidelines, future studies should aim to include a more balanced sex distribution and explore sex-specific differences in gait adaptations where feasible. 30
Variations in prosthetic fitting and alignment, performed according to routine clinical practice, may also have contributed to variability in gait outcomes. However, this reflects real-world prosthetic use and enhances the ecological validity of the findings. Furthermore, the experimental setup, including the uneven walking surface and auditory Stroop task, was designed to simulate community relevant conditions, although it may not fully capture the complexity of real-world environments or higher cognitive demands.
Future studies should include larger and more diverse populations, including both male and female participants and individuals with varying aetiologies and functional levels, as well as comparisons with advanced prosthetic technologies such as microprocessor-controlled knees.
Conclusions
The present study examined the influence of passive prosthetic knee mechanisms on self-reported mobility and gait biomechanics during single-task and dual-task walking over an uneven compliant surface in individuals with TFA. Overall, individuals with TFA demonstrated reduced self-reported functional mobility and altered gait biomechanics compared with AB individuals, particularly in joint kinematics and selected kinetic outcomes. Both TFA groups showed reduced knee flexion and ankle plantarflexion, reflecting persistent biomechanical constraints associated with transfemoral amputation.
Comparison between TFAP (polycentric knees) and TFAFC (fluid-controlled knees) showed limited differences across most biomechanical outcomes, indicating that these passive knee mechanisms provide broadly comparable gait performance under the present walking conditions. A clear kinetic difference was observed only for maximum stance hip extension (HM1), with lower values in the TFAFC group compared with AB. Maximum stance knee flexion moment (KM2) and maximum ankle plantarflexion moment (AM2) showed overall group differences without significant pairwise differences. Dual-task walking increased maximum stance ankle dorsiflexion (AA2) across groups, indicating that cognitive demand influenced gait adaptation during uneven surface walking.
A significant group × task interaction was observed for maximum hip eccentric power during late stance (HP2), with the TFAP group showing increased hip power during dual-task walking. This indicates that task-specific proximal adaptations occur in individuals using polycentric knees when walking under combined environmental and cognitive demands. No significant differences were observed in vertical ground reaction force outcomes, suggesting that overall loading patterns were generally maintained despite joint-level biomechanical differences.
In conclusion, passive prosthetic knee type had a limited overall influence on gait biomechanics, although specific task-related adaptations were evident. Future studies should include larger and more diverse samples, including different functional levels, amputation aetiologies, and sex distributions, and compare these findings with advanced prosthetic knee technologies.
Footnotes
Acknowledgements
This study is supported by the Ministry of Education Malaysia through the Fundamental Research Grant Scheme (FRGS/1/2017/ SKK06/UM/02/1). The authors thank all participants for their involvement. Artificial intelligence tools were used for language refinement and clarity, and the authors take full responsibility for the content and accuracy of the manuscript.
Author contributions
The authors confirm the equal contribution in each part of this work. All authors reviewed and approved the final version of this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Ministry of Education Malaysia through the Fundamental Research Grant Scheme (FRGS/1/2017/ SKK06/UM/02/1).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.