
Abstract
Summary
The aim of the paper is to evaluate alcohol misuse among an inner city adult HIV clinic population with AUDIT (Alcohol Use Disorders Identification Test). A cross-sectional HIV outpatient clinic analysis between 28 February 2011 and 11 March 2011 was carried out. AUDIT, demographic and clinical data were collected. Univariate analysis was performed to look for the associations between variables. Backward stepwise multivariate analyses were performed on significant variables from the univariate analysis to assess for predictors of alcohol dependence. In total, 111 patients were included (60% uptake of clinic attendees); 66% were men and 26% were hepatitis C virus (HCV) co-infected. The median AUDIT score was 5 (within normal range). Thirty-four ‘AUDIT positive’ cases were identified: five (4.5%) indicated consumption of hazardous levels of alcohol; 21 (19%) indicated harmful levels of alcohol; and eight (7%) were likely alcohol dependent. Younger age (<40 years old) was significantly associated with AUDIT positivity (P = 0.006). On multivariate analysis younger age (P = 0.045, odds ratio 13.8) and lower level of education (P = 0.006, odds ratio 6.7) were predictive of scores indicative of alcohol dependence (AUDIT ≥20). In conclusion, younger age and lower educational levels were associated with scores consistent with alcohol dependence. AUDIT was well tolerated and easy to administer in this outpatient HIV clinic population.
BACKGROUND
Excessive alcohol consumption is implicated in many injuries, emergency room attendances and transmission of sexually transmitted infections. 1 –3 Alcohol misuse has numerous adverse health outcomes in both the general and HIV populations, and continues to play a large part in morbidity and mortality worldwide. 1,3 –5
The advent of combination antiretroviral therapy (ART) has transformed HIV to a chronic disease; morbidity and mortality from AIDS-related deaths have declined. 6 However, liver-related morbidity and mortality has increased over this time period. 7,8 Approximately 30% of HIV-infected individuals are also co-infected with hepatitis C (HCV), which poses a major health burden worldwide. 7 Co-infection with HIV and HCV has a deleterious effect on the outcomes of both viruses. 9,10 These patients have accelerated progression to cirrhosis and consequently increased rates of hepatocellular carcinoma and death. 8,10
The effects of alcohol on the immune system are well documented in the literature. Alcohol is an immunosuppressant and has direct effects on CD4 lymphocyte number and function. 11,12 It also affects macrophage phagocytic activity, T-cell apoptosis and inhibits T-cell responses. 12 The indirect effects of alcohol-related malnutrition and liver disease also suppress the immune system. 12
From a HIV perspective, excessive consumption of alcohol is linked to poor adherence with ART, and subsequently non-achievement of virological suppression in individuals in receipt of ART. 4,5,12 For HCV, continued alcohol consumption is associated with accelerated disease progression, higher HCV RNA levels, liver fibrosis and cirrhosis. 13 –15 It has also been found to decrease response rates to interferon/ribavirin therapy, and is a barrier to treatment. 14,16
There are many different tools to screen for alcohol problems and dependence. These include CAGE, AUDIT (Alcohol Use Disorders Identification Test) and MAST (Michigan alcohol assessment tool). 1,17,18 Currently there is no preferred/recommended tool. Although they all have benefits and disadvantages, they all require proper diagnostic and clinical evaluation. 17 The CAGE questionnaire is very quick to administer as it only has four questions. 17,18 It is an effective screening tool for alcohol abuse and dependence. 17,18
The AUDIT tool was developed specifically by the World Health Organization (WHO) to screen for excessive alcohol consumption and to help health-care professionals identify individuals who would benefit from abstinence or reduction. 1 It detects less severe forms of drinking than the CAGE. 1 This is especially of benefit in HIV/HCV co-infected individuals, who have a high risk of progressing to end stage liver disease. 9,10 It has been validated in HIV-infected individuals, and has been found to have a high sensitivity and specificity with DSM-III-R criteria for alcohol abuse and dependence. 19 –21
AIMS
To evaluate alcohol consumption and misuse among an inner city HIV outpatient clinic population using AUDIT.
METHODS
This was a cross-sectional analysis of adult HIV-infected clinic attendees who were registered for care at an inner city HIV specialist clinic. Between 28 February 2011 and 11 March 2011 all individuals attending six HIV clinics were invited to participate and self-complete the AUDIT tool. Clinic attendance lists and completed questionnaires were checked to ensure that no patients were included twice in the analysis. Demographic and clinical data were also collected. This study received approval by the Hospital Patient Advocacy Committee.
Data collection
Patients completed questionnaires, with assistance available from trained staff if required. Staff collected clinical and demographic data from case-note review. The data were entered onto a Microsoft Excel database and analysed in SPSS version 16.
Clinical and demographic data collected
Demographic data collected included: age, date of HIV diagnosis, gender, ethnicity, level of education, current employment status and mode of acquisition of HIV.
HIV-specific data collected included CD4 counts (cells/mm3), HIV viral load (copies/mL), hepatitis C antibody (HCV), HCV PCR RNA status (positivity/negativity) and current antiretroviral prescription.
Survey materials and instruments used
AUDIT is a 10-item questionnaire that takes about three minutes to administer, and is validated for use in many patient populations and in settings such as medical outpatient clinics and hospital wards. 1,18,22 It has also been validated in the HIV population. 19 It contains three questions assessing alcohol use and seven items on alcohol problems/alcohol dependence symptoms and subsequent consequences. 1 AUDIT classifies individuals who drink excessively as: hazardous drinking, harmful use or alcohol dependence. 1 Hazardous drinking is when alcohol consumption increases the risk of adverse consequences for the user. 1 Harmful use is when alcohol consumption impacts upon physical and mental health. 1 Lastly alcohol dependence is when repeated alcohol consumption is given a higher priority than other activities, with impaired control, increased tolerance and a physical withdrawal upon discontinuation. 1
Each question has five responses, which are scored from 0 to 4. 1 The total score ranges from 0 to 40. 1 A score of 8 or higher is abnormal (AUDIT positive). 1 A score between 8 and 12 in women and 8 and 14 in men indicates hazardous alcohol use. 1 A score between 13 and 19 in women and 15 and 19 in men indicates consumption of harmful levels of alcohol. 1 Scores of 20 or higher indicate possible alcohol dependence and warrant further medical review. 1
Statistical analysis
Relationship between AUDIT score and baseline demographics (n = 111)
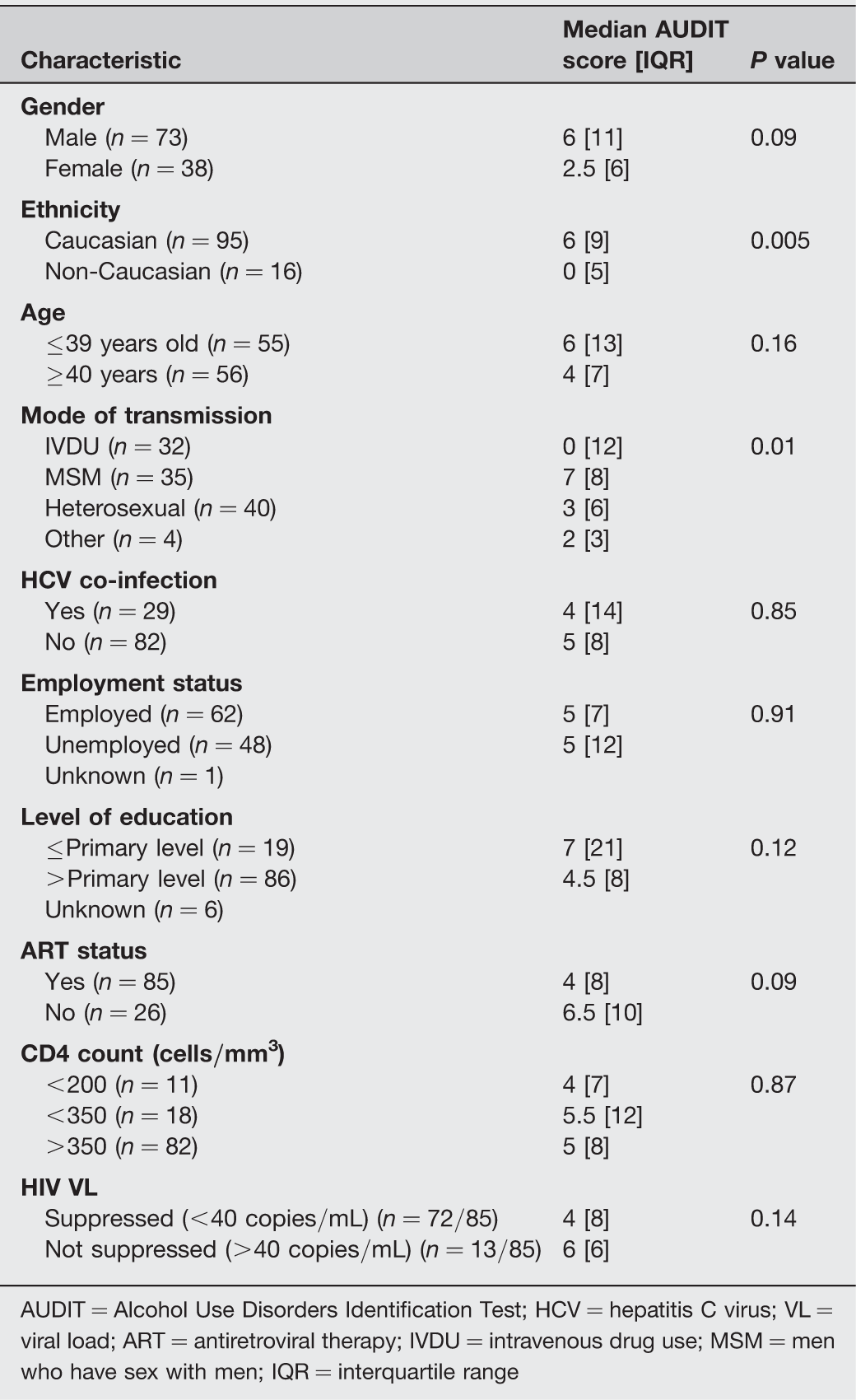
AUDIT = Alcohol Use Disorders Identification Test; HCV = hepatitis C virus; VL = viral load; ART = antiretroviral therapy; IVDU = intravenous drug use; MSM = men who have sex with men; IQR = interquartile range
Univariate and multivariate analysis of potential demographic and clinical characteristics associated with AUDIT scores ≥20 (n = 8)
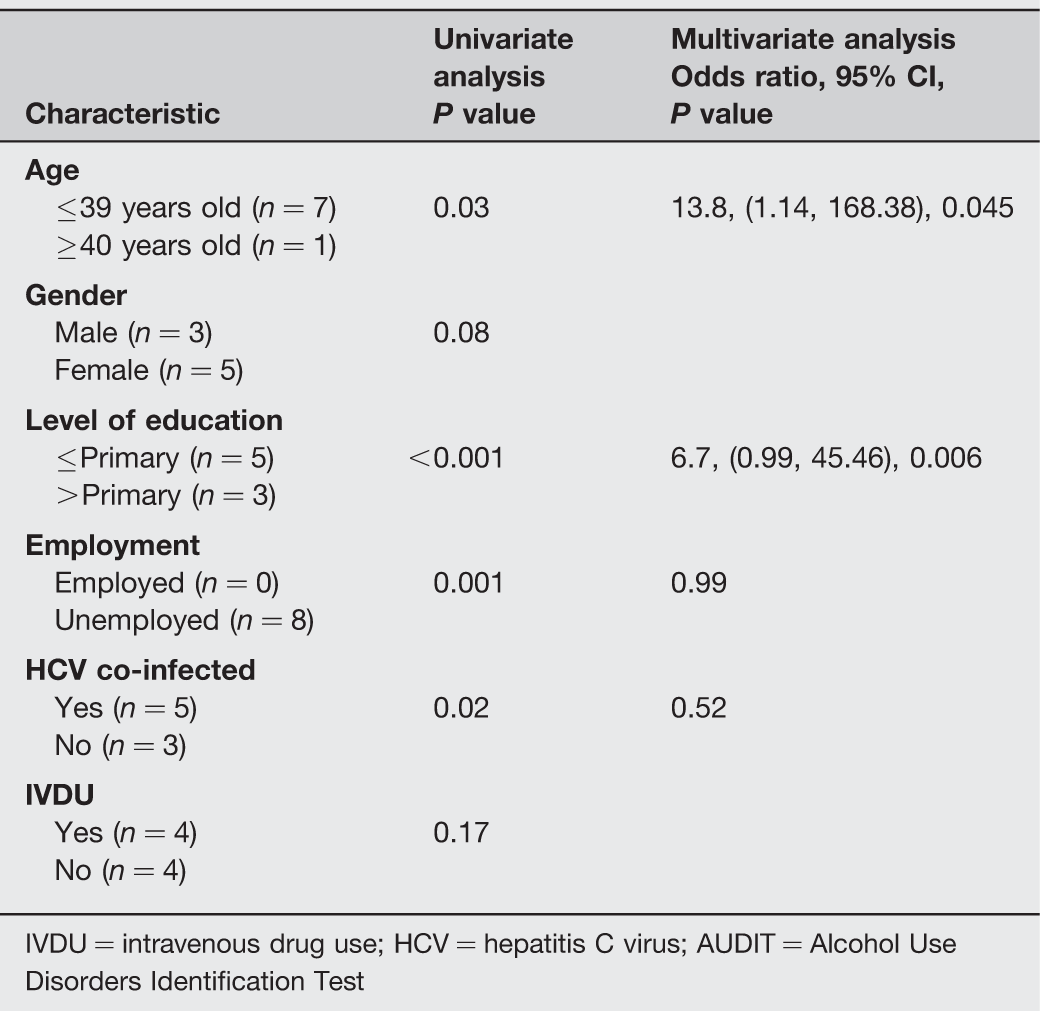
IVDU = intravenous drug use; HCV = hepatitis C virus; AUDIT = Alcohol Use Disorders Identification Test
RESULTS
One hundred and eighty-six individuals attended HIV outpatient clinics over the two-week sampling period. One hundred and eleven patients completed the AUDIT questionnaire and were included in this analysis. This gives a completion rate of 60%. Sixty-six percent of the patients were men, and the mean age was 39 ± 9 years (Table 1). Eighty-six percent of the population were of Caucasian ethnicity. Fifty-six percent were currently employed. The mean time since HIV diagnosis was 7 ± 5.9 years. Twenty-six percent were HCV co-infected. Seventy-seven percent of patients were in receipt of ART, of which 83% were virologically suppressed. The median AUDIT score was 5, which is within the normal range. Thirty-three patients had AUDIT scores of 0. Thirty-four ‘AUDIT positive’ (AUDIT scores ≥8) cases were identified. Of these five individuals (4.5%) had scores indicating consumption of hazardous levels of alcohol. Twenty-one patients (19%) were likely to be consuming harmful levels of alcohol, and eight were highly likely to be alcohol dependent.
Of the demographic data collected only younger age (<40 years old) was significantly associated with AUDIT positivity (P = 0.006). Ethnicity was significantly associated with difference in median AUDIT scores; Caucasian patients had higher median AUDIT scores than non-Caucasians and therefore were more likely to be misusing alcohol (Table 1). While mode of acquisition had a P value of 0.01, this represented a significantly lower median AUDIT score between people who reported their mode of acquisition as ‘other or unknown’ and those who reported it as MSM (men who have sex with men), IVDU (intravenous drug use) or heterosexual. There was no difference detected in AUDIT scores between patients who acquired HIV through IVDU, heterosexual or MSM.
Factors associated with possible harmful and hazardous alcohol consumption
On univariate analysis there were no significant correlations between AUDIT scores indicative of harmful drinking and clinical or demographic factors (age, gender, level of education, employment and mode of acquisition of HIV). With regard to scores highly suggestive of hazardous alcohol consumption, younger age (<40 years old) was the only significant factor on univariate analysis (P = 0.03).
Factors associated with AUDIT ≥20 (indicative of alcohol dependence).
Univariate analysis of patients with AUDIT ≥20 revealed significant associations with HCV co-infection, younger age, lower educational level and unemployment (Table 2). However, acquisition of HIV through intravenous drug use was not significantly associated with possible alcohol dependence. On multivariate analysis younger age and lower level of education remained significantly associated with possible alcohol dependence; HCV co-infection and employment status were not (Table 2).
DISCUSSION
The prevalence of AUDIT positivity (indicating alcohol misuse) was 31% in this study population. Rates from other HIV populations in the literature vary from 12% to 41%. 23 –28 Seven percent of this clinic population had AUDIT scores consistent with alcohol dependence, which is comparable to that found by McGinnis et al. 27 Of the published data on the use of AUDIT in the HIV population, the majority have used the ‘AUDIT-C’ tool. This is a modified version of AUDIT consisting of only the first three items. 19,27,29 –34 Thus, this study provides useful new data on full AUDIT scores from a representative population of HIV patients attending an inner city HIV service.
The aim of this study was to determine levels of alcohol misuse in individuals attending outpatient HIV clinics using AUDIT. This screening tool has been validated in HIV populations, is quick and easy to administer, and correlates well with psychiatric criteria for alcohol abuse disorders. 19 –21,35 CAGE is effective at identifying alcohol dependence and abuse. 17,36,37 In contrast, AUDIT was developed to identify individuals with lower levels of alcohol consumption. Therefore it detects significantly more patients with alcohol consumption that may result in harm, who should be more responsive to brief interventions. 36,37 The AUDIT tool was well accepted in this clinic population, with a completion rate of 60%, which is comparable to other non-HIV populations. 36
In this study only younger age (<40 years old) was significantly associated with AUDIT positivity. The prevalence of problem alcohol use is known to decrease with increasing age in the general population. 3,38 With regard to ethnicity, Caucasian patients had higher median AUDIT scores and were more likely to misuse alcohol than individuals of black ethnicity. Ethnic differences in alcohol consumption have also been well documented in the literature. 38 –40
AUDIT scores of 20 or higher (indicating possible alcohol dependence) were significantly associated with younger age, attainment of lower levels of education, unemployment and HCV co-infection. The link between alcohol consumption and unemployment/low levels of education has previously been documented in the literature. 41 In this clinic population unemployment was only significant on univariate analysis. A significantly lower median AUDIT score between people who reported their mode of acquisition as ‘other or unknown’ and those who reported it as MSM, IVDU or heterosexual was found. As no further information is available on this category of patients, the clinical significance of the finding is uncertain. Of more interest is that no difference was detected in our cohort in median AUDIT scores of patients with a history of IVDU and those who did not. This is in contrast to findings in other studies, of problem alcohol use in patients on methadone maintenance therapy. 22,42,43
The relationship between alcohol consumption and HCV is less clear. Some studies have found that individuals who are aware of their HCV status actually drink less alcohol. 44,45 This has been reported in both HCV mono-infected and HIV/HCV co-infected populations. 44,45 In contrast in this study HIV/HCV co-infection was associated with AUDIT scores of 20 of higher (likely alcohol dependence) on univariate analysis. This was irrespective of the mode of acquisition of HIV. Both HIV and alcohol consumption have been shown to increase progression of HCV, and so this cohort of co-infected patients who are drinking excessive levels of alcohol have an even higher risk of end stage liver disease and its complications. 8,9,13,14 The need for alcohol restriction and abstinence (if treatment is planned) for HCV-infected individuals is well documented in the literature. 14 This association was not found on multivariate analysis, and is likely due to the high correlation of HCV positivity and lower educational attainment.
Alcohol misuse has been found to reduce CD4 count and is associated with non-achievement of virological suppression in patients receiving ART. 12 With effective combination ART HIV-infected individuals are living for longer, and liver-related morbidity and mortality is increasing. 6,8 In this study HCV co-infection was a risk factor for AUDIT scores of 20 or higher (likely alcohol dependence) on univariate analysis. These individuals have a high risk of progressing to end stage liver disease. 8,9 Until relatively recently, treatment options and outcomes for HCV were limited, especially for co-infected patients with genotype 1-infection. However, the newer anti-HCV agents have substantially increased the success of HCV treatment in genotype 1-infected patients. 46 –48 The effectiveness of brief interventions for alcohol consumption is well recognized. 18,49,50 In 2011, A Cochrane review found brief interventions for heavy alcohol users to be beneficial in the short term. 51 Therefore, screening for alcohol misuse is recommended in HIV-infected individuals, and is especially important for HIV/HCV co-infected patients. 25,52
From a practical point of view the results of this outpatient study indicate that targeted screening of ‘at risk individuals’ is a viable option. In particular, screening individuals who are HIV/HCV co-infected, younger (<40 years old), unemployed and have achieved lower levels of education. AUDIT is a quick and easy to administer tool that can detect lower levels of alcohol misuse, which should be amenable to brief clinic-based interventions. However, onwards referral to specialist alcohol services for patients consuming higher levels of alcohol is recommended.
There are limitations to this study; the numbers included are small and it was outpatient-based. Alcohol consumption is known to contribute to many emergency room attendances and inpatient admissions. 3 It is therefore possible that some of the heavier drinkers were excluded from this study. Another confounding factor was that no extra assistance was available for individuals with learning difficulties or those whose first language is not English. Whilst no diagnostic interview was performed in individuals who were AUDIT positive, this tool has been found to correlate well with psychiatric diagnoses of alcohol use disorders in both the general population and HIV-infected individuals. 20,21,35
To summarize, the prevalence of AUDIT positivity indicating alcohol misuse was 31% in this cross-sectional outpatient HIV clinic sample. The AUDIT tool was well tolerated, with a completion rate of 60%, and has been found in previous studies to have a high discriminatory ability to detect alcohol use disorders. 35 This study found no relationship between CD4 count, HIV viral load and alcohol consumption. Younger patients (<40 years old) were more likely to be AUDIT positive and to misuse alcohol. Caucasian patients had significantly higher median AUDIT scores than black HIV-infected individuals. HCV co-infection (irrespective of the mode of acquisition) and unemployment were significantly associated with alcohol dependence scores on univariate analysis. Younger age and lower educational attainment predicted alcohol dependence scores on multivariate analysis and patients with these demographics should be especially targeted for assessment of alcohol misuse. AUDIT is a quick, easy to administer and well-tolerated screening tool for alcohol misuse in HIV outpatient clinic populations.