
Abstract
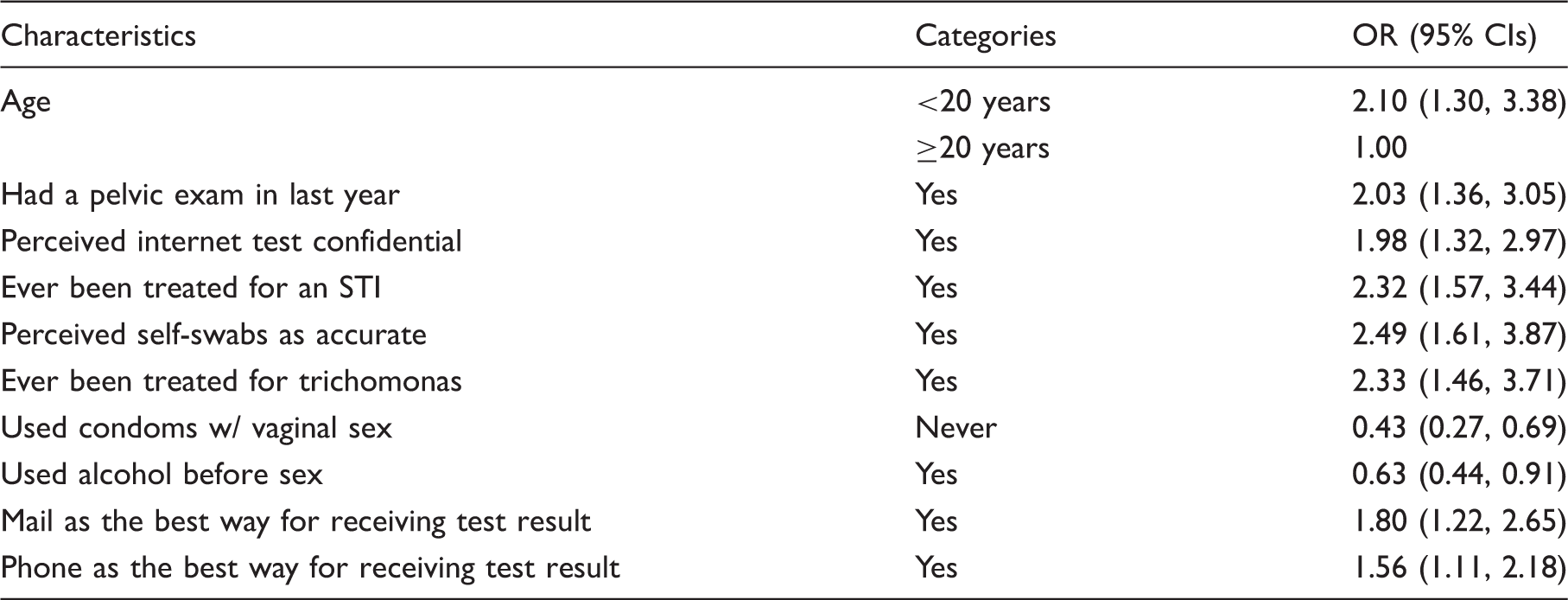
Professional organizations recommend rescreening chlamydia-infected women. The iwantthekit Internet-screening programme offered rescreening opportunities by using iwantthekit. Mailed, home-collected vaginal swabs were tested for chlamydia, gonorrhoea, and trichomoniasis by nucleic acid amplification tests. Demographics and risk behaviours of repeat users were determined from questionnaires. Predictors of repeat users were measured in a matched case–control study. Of 1747 women, 304 (17%), who used iwantthekit, indicated they had used the kit previously. Mean age was 24.7 ± 5.7 years and 69% were African-American. Repeat iwantthekit users were more likely to be aged ≥20 years (OR = 2.10); were more likely to have been treated for a sexually transmitted infection (OR = 2.32); less likely to drink alcohol before sex (OR = 0.63); and to never use condoms (OR = 0.43). Of repeat users, 84.2% had a negative prior test and 15.8% had a positive. At current test, 13.2% were infected. Previous trichomoniasis was associated with current trichomoniasis (p < 0.05). The iwantthekit may offer rescreening opportunities for previously infected women.
Introduction
Chlamydia trachomatis (CT) is the most commonly reported communicable disease in the United States, occurring most often among adolescent and young adult females. The Centers for Disease Control and Prevention (CDC) estimates there are approximately 2.8 million new cases each year. 1 Acute chlamydia infections often have no symptoms, leaving many cases untreated. Serious sequelae such as pelvic inflammatory disease (PID) are associated with untreated CT infections. The U.S. Preventive Services Task Force (USPSTF) and major medical professional organizations recommend an annual screening test for chlamydia for all sexually active adolescents and young women 25 years of age and under, for all pregnant women, and for women at high risk. 2 Yet, chlamydia screening remains an underutilized clinical preventive service with less than 50% of eligible women in commercial or Medicaid health plans being screened annually. 3 An USPSTF “A” rated recommended service, it is one of the 10 most beneficial and cost-effective prevention services. 4 However, there are approximately 10–11 million women aged 15–25 years who are not receiving screening for CT as recommended. The United States did not achieve, but has regressed, in meeting national health objectives by 2010 for chlamydia. 5
Neisseria gonorrhoeae (GC) infections are also highly prevalent with over 700,000 new infections every year in the United States and are also associated with the same serious sequelae as CT. 1 CDC recommends rescreening women who are infected with CT and GC in 3 months. 6
Trichomonas vaginalis (TV) infections are highly prevalent with estimates of 7–8 million infections annually in the United States, representing the most common curable sexually transmitted infection (STI) in sexually active women.7,8 There are no United States national surveillance data available for TV, because these infections are not reportable to CDC, but research studies have demonstrated high prevalences in both young and older populations, as well as in minority groups.7,8 Although screening for TV is not recommended for asymptomatic women, TV infections have been associated with poor reproductive outcomes such as low birth weight and premature birth9,10; as well as acquisition of and transmission of HIV infection.11–16 They are highly prevalent in Black women, ranging from 10 to 13% in reported studies compared to 1–5% in White women.17–20 Many research reports demonstrate high costs of TV infections 21 and call for more attention to be given to trichomonal infections.17,22,23
Screening for all of these STIs in women of reproductive age can impact these epidemics but many barriers exist. Self-collection of urogenital samples for testing has been promoted by public health officials. 24 Submission of such self-obtained vaginal samples (SOVS) collected at home could complement screening, especially rescreening programmes, as well as remove many barriers that women face in getting tested for STIs. 25 Since CDC-recommended repeat screening of CT and GC-infected women has been difficult to implement and to measure, 6 we sought to ascertain rescreening practices in the home-collection programme, iwantthekit (IWTK) Internet-screening programme for CT, GC, and TV.20,25
Methods
Mailed vaginal swabs from the Internet-recruited IWTK home-collection programme were tested for CT, GC, and TV by nucleic acid amplification tests (NAATs) (Aptima Combo2, Gen-Probe, Inc., San Diego, CA). The IWTK programme has been previously described and was approved by the Johns Hopkins Institutional Review Board.20,25 Briefly, users, including women and men, order kits via the website, which are mailed to their home in plain envelopes. After self-collection of genital and/or rectal swab samples, the specimens are returned to the testing laboratory in pre-addressed, postage-paid envelopes, and included a questionnaire. The service is free and all results are returned to participants by the method of their choice: email, letter, phone call, and since 2010 by short message service (SMS). All positive results are called so that treatment can be scheduled at participating clinics. The website is educational with sections about every STI, including chlamydia, gonorrhoea, trichomoniasis, HSV, HPV, HIV, HBV, and bacterial vaginosis, each of which have health-promotion messages regarding how to stay healthy and avoid these infections.
We determined demographic and risk behaviour characteristics of female repeat users from rescreening questionnaires with a matched case–control study. A case (N = 304) was defined as reporting having ever used IWTK before. A control was a user who reported never using the programme. Two controls (N = 608) were systematically sampled for each case by matching the date of use IWTK of the case within 3 months. A matched case-control study design and analysis was used because the time sequence between repeat tests was not possible to measure from our de-identified questionnaire data. Thus, questionnaire data from repeater women cases were compared to questionnaire data from non-repeater controls matched to the time of screening. Bivariate analysis and multivariate analysis by conditional logistic regression were performed using SAS® version 9.3 (Cary, NC) to determine factors that were over-represented among the cases as compared to the controls, followed by descriptive analysis. For variables with multiple categories, a category might be merged with next one if the number in the category was small before multivariate analysis. p Values of ≤0.05 were considered significant. Variables significant in bivariate analysis and other variables considered as potential confounders in the literature were entered into the logistic regression model.
Results
Characteristics of repeat iwantthekit (IWTK) female user cases (n = 304) and their controls (n = 608).

STI: Sexually transmitted infection.
p < 0.05
Not mutually exclusive.
Over 80% of repeat user participants stated that they thought Internet-based screening for STIs was confidential and private. Most said that testing using self-administered swab was accurate (83%) and safe (97%). Approximately 93% preferred collecting their own sample and 89% would use the Internet to access testing again. Radio advertisement (42%) was the leading source where they learned about IWTK program, following by surfing the Internet (31%), while only 2 (1%) participants were told by their sex partner.
Factors associated with repeat iwantthekit (IWTK) use by multivariate conditional logistic regression analysis in 912 IWTK female users.
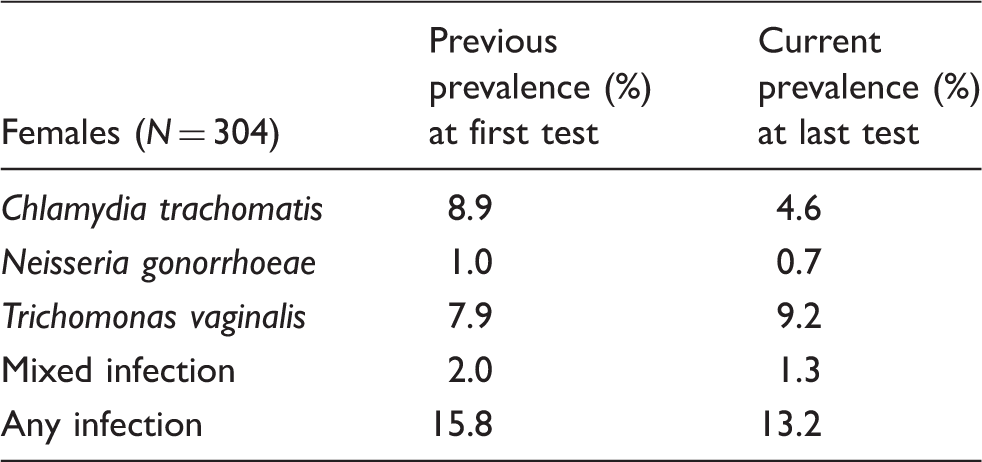
Prevalence of infection for women who submitted more than one vaginal swab for testing for sexually transmitted infections via the Internet-recruitment program.
Discussion
The Internet-screening programme, IWTK, attracted a considerable number of previously infected participants, who practiced high-risk sexual behaviours, to use the programme for repeat STI testing. Prevalences of CT and TV were high. Over 17% of 1747 women, who were screened previously, electively submitted samples for another test for an STI. These 304 women demonstrated a high reinfection rate (13.3%) for one of the three STIs. While prevalence for CT decreased from 8.9% to 4.6%, which may be considered a measure of success, the prevalence for TV actually increased from 7.9% to 9.2%. It is not known why trichomonas prevalence increased among repeat testers, but symptoms may have been a factor in submission of a repeat test. Unfortunately, overall not much change for infection with “any STI” occurred, with 15.8% being infected at first test and 13.2% being infected at second visit. The positive aspect is that those who were reinfected were diagnosed and were treated.
Repeat user women indicated on questionnaires that they practiced high-risk sexual behaviours. Since most were young, had multiple or new partners, and did not often use condoms, this rescreening method may be ideal for targeting women who have already had a previous infection with an STI. Rescreening of previously infected women is especially important for chlamydia, since multiple infections increase a women’s probability of developing serious sequelae, such as PID, infertility, and ectopic pregnancy.6,26–31
The women who retested were more likely in multivariate analysis to be single, be African American, and to perceive the method as safe, confidential, and accurate, as well as report that they had already been treated for an STI. Previous studies of the IWTK program have shown that users reported being highly satisfied with the methodology and demonstrated higher prevalences than elicited by women screened in family planning clinics.25,32
While professional organizations recommend annual chlamydia screening of females at risk of chlamydia,2,6,33 as well as repeat screening at 3 months for those previously infected, 6 repeat screening is often difficult to accomplish; use of home-collected and mailed screening specimens has been advocated as a method to promote screening and rescreening.34,35
Other studies have demonstrated that use of home-collected genital samples resulted in more women being rescreened, as well as a high degree of satisfaction.34,36,37 One report demonstrated that 75.7% of women, who were given a choice in a one-year follow-up contraceptive study that screened for STIs, chose the home-collection method over visiting a clinic or their own doctor. 34 In that study, women who chose home-based testing were more likely to complete a test compared to all clinic-based testers. The authors recommended that future interventions to increase screening for STIs should consider home-based or patient-controlled testing. 34 The recent home-screening randomized controlled trial for chlamydia and gonorrhoea rescreening indicated that home screening was acceptable and showed that women who received a home-testing intervention completed significantly more STI tests overall and more STI tests when asymptomatic as compared with women who did not receive the home-testing option. 37
We acknowledge that many young users of “iwantthekit” (IWTK) are devoted to SMS and later in the programme, we instituted an option to receive results by text message. We use it for negative results via a coded message that states “IWTK is negative,” for users who select that option. We have returned 1273 negative results by SMS since September 2010.
Our study has some recognized limitations. The data for risk history and positivity for STIs from the original test were elicited from questionnaires and may suffer from recall bias. It was also impossible to ascertain the time period between the original test and the repeater test. Additionally, while total prevalence of infection for an STI decreased in our study, it is not possible to say this would translate into future reduced incidence of infections on a large scale.
In summary, IWTK may offer an alternate option to retesting with home collection and the approach of not having to visit a clinic for rescreening to previously infected women. More research into this approach is needed and may have the potential to improve reinfection rates for STIs.
Footnotes
Declaration
The data from this manuscript were presented in part at the ISSTDR meeting in Quebec, Canada, July 2011.
Funding
This study was funded by NIBIB, NIH U54EB007958; NIAID, NIH HPTN U01 AI068613.