
Abstract
As patients infected with HIV live longer due to effective anti-retroviral therapy, new disease manifestations are becoming apparent. We describe the case of a 59-year-old patient who presented to our unit with atraumatic splenic rupture secondary to chronic HIV infection. Given the high mortality associated with atraumatic splenic rupture, we believe it should be included in the differential diagnosis of HIV-positive patients presenting with acute abdominal pain.
Case presentation
A 59-year-old man with known HIV infection presented with a four-day history of left upper quadrant abdominal pain which later spread to the epigastrium and right upper quadrant. The pain was colicky, worse on lying flat and was associated with a pain across both shoulders. He had suffered one episode of presyncope with clamminess and diaphoresis. His bowels were opening normally, he had no dysuria, frequency, vomiting or nausea. He denied any history of trauma. His medical history included well-controlled HIV infection diagnosed 14 years previously, known splenomegaly, gallstones, asthma, reducible inguinal hernia, lymphogranuloma venereum, peripheral neuropathy and low testosterone levels. He had been on anti-retroviral therapy for 14 years with a current regimen of darunavir/ritonavir and raltegravir.
Splenomegaly had been discovered incidentally five years previously on ultrasound with the spleen measuring 18 cm in a craniocaudal dimension. An MRI 3 years later also made incidental note of splenomegaly (21 cm). No formal work-up for splenomegaly had been performed.
Examination revealed a Caucasian male who was afebrile and haemodynamically stable. His abdomen was tender over the left flank, left lower quadrant and right upper quadrant. There was no guarding or rebound tenderness and bowel sounds were present. There was no stool or masses in the rectum.
Blood investigations showed an initial haemoglobin of 14.9 g/dL, a raised white cell count at 15.8 × 109/L and an elevated serum creatinine of 159 mmol/L compared to a baseline of 120 mmol/L. CD4 T-cell count was 369 × 109/L and HIV viral load was undetectable. Serum amylase, corrected calcium, C-reactive protein and liver enzymes were within normal ranges. He was negative for Epstein–Barr virus (EBV) and cytomegalovirus (CMV) IgM although positive for CMV IgG. Hepatitis B and C virus serology was negative. Urinalysis revealed a trace of blood and protein. Erect chest radiograph showed no free air under the diaphragm.
Computed tomography of the abdomen revealed high attenuation fluid distributed predominantly around the spleen and extending in a peri-hepatic and right paracolic gutter distribution. The spleen was enlarged at 22 cm and a cleft was noted on its anterior aspect that was also evident on previous abdominal imaging.
After 24 h, the patient’s haemoglobin had fallen to 9.2 g/dL. Emergency laparotomy revealed an enlarged spleen, subcapsular haematoma and clotted blood within the abdomen. Total splenectomy was performed. The resected spleen weighed 744 g and measured 150 mm × 205 mm × 70 mm.
Sections from the spleen showed no macroscopic masses. Microscopically, the white pulp was atrophic and the red pulp was mildly congested.There was mild excess of small lymphoid cells within the red pulp cords of Billroth. These cells did not show any atypia, and they expressed CD3, CD8 and granzyme B (Figure 1). A small proportion of the lymphoid cells included CD56-positive NK cells. Features were consistent with changes associated with retroviral infection.
1
The volume of the infiltrate and the morphology of the cells did not warrant T-cell receptor gene rearrangement studies.
A/B – microscopic appearance of crosscut spleen. C – CD20 + B-cell staining. D – CD3 + T-cells showing excess of small T-cells. E – CD8 + staining showing prominence of CD8 + T-cells. F – Granzyme B + cell staining.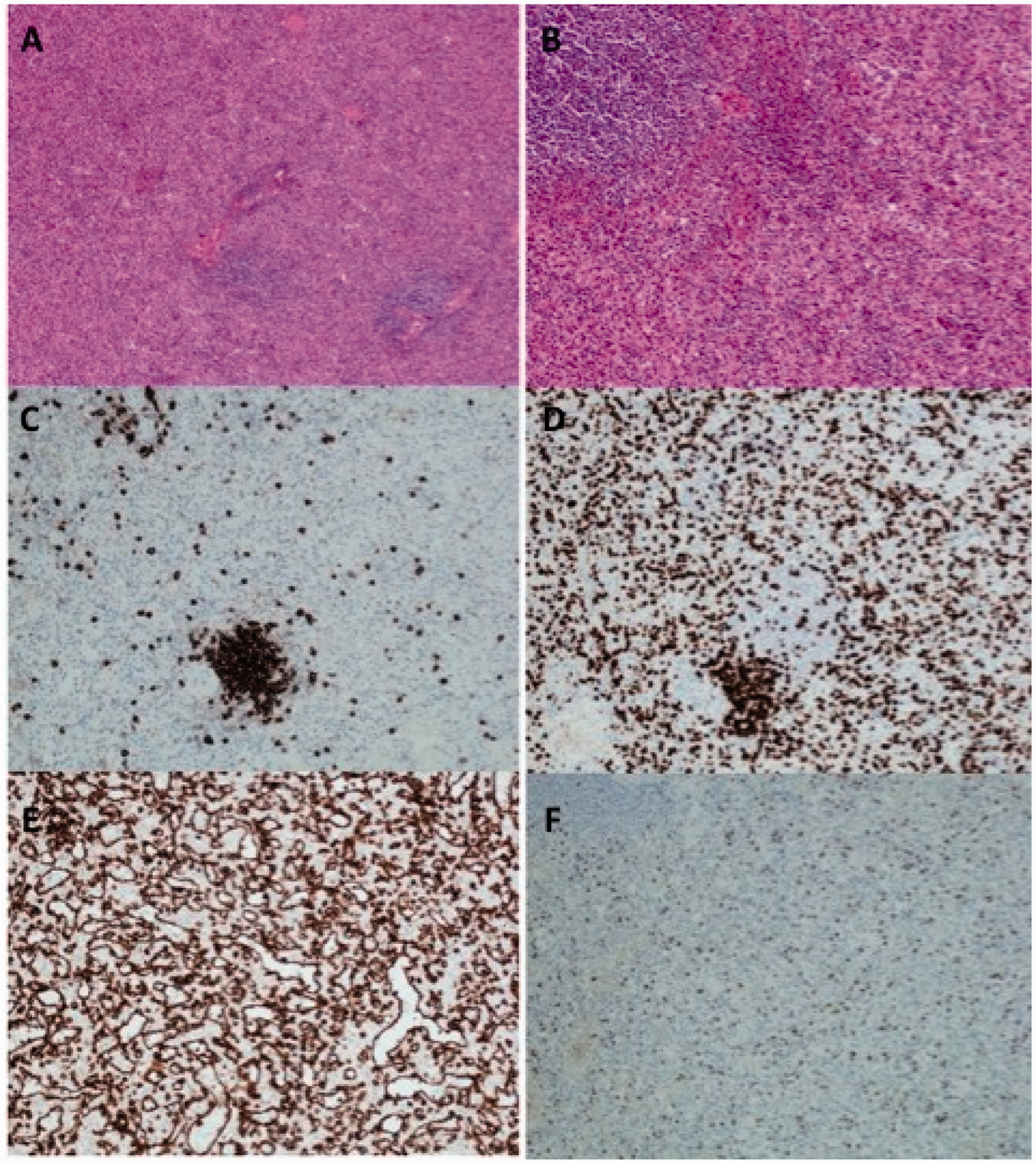
The patient recovered well, was educated regarding the risk of life-threatening infection post-splenectomy and was provided with appropriate vaccinations and prophylactic antibiotics as per UK guidelines. 2
Discussion
Atraumatic splenic rupture is a rare condition associated with a significant mortality risk in the region of 12%. 3 Neoplasms, infections, non-infectious inflammation and drugs account for approximately 70–80% of cases. 3 Early diagnosis can lead to life saving surgery and therefore the recognition of any risk factors is paramount.
Infectious disorders account for approximately 27% of atraumatic splenic ruptures with associations including EBV, CMV, tuberculosis (TB), malaria, infective endocarditis and typhoid. 3 Splenomegaly, affecting as many as 70% of patients with HIV, is a significant risk factor for atraumatic rupture (OR 2.34, P = 0.04). 4
Atraumatic splenic rupture has previously been associated with HIV infection through opportunistic infections such as TB and malignancy including Kaposi sarcoma. One previous case report implicated acute HIV infection as a cause of splenic rupture. 5 Our report is the first to describe atraumatic splenic rupture secondary to chronic HIV infection.
Limitations include the possibility that minor trauma the patient did not recall or superadded non-EBV/CMV viral infection may have contributed to the splenic rupture.
We therefore recommend that splenic rupture be included in the differential of patients with HIV infection presenting with an acute abdomen. HIV-positive individuals with splenomegaly should be advised of the risk of splenic damage with recommendations to present in case of abdominal pain.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare no conflict of interest.