
Abstract
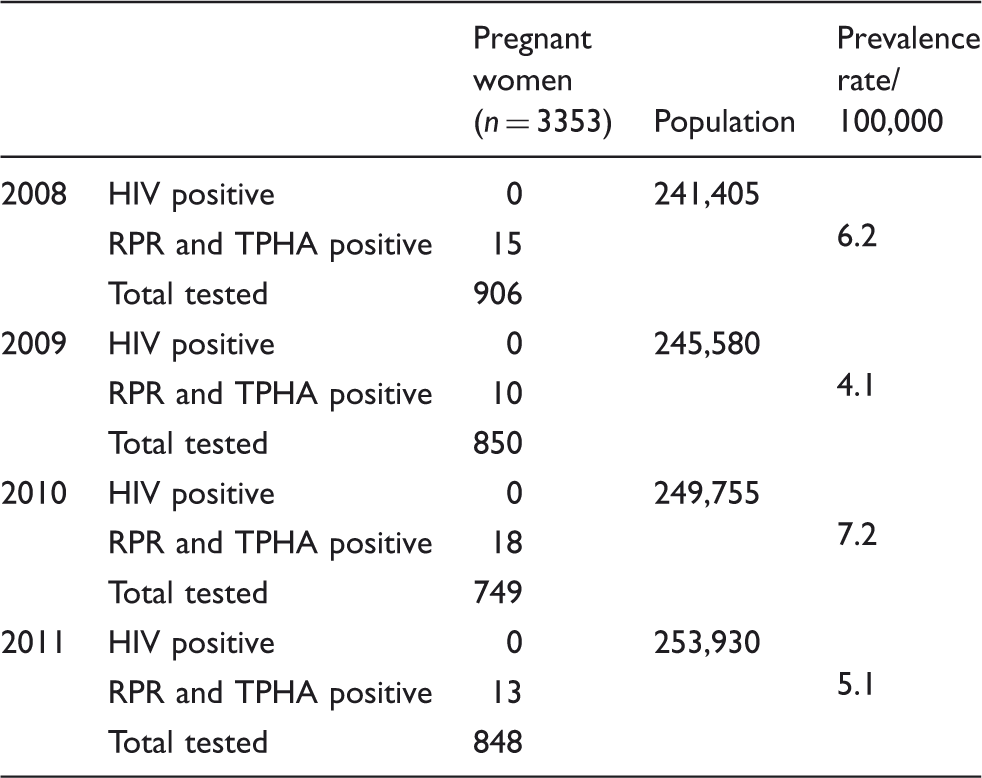
Sexually transmitted infections have been described as one of the major health problems in several countries of the Pacific Region. The objective of the study was to estimate the prevalence of pregnant women infected with HIV and/or syphilis in New Caledonia. HIV and syphilis test results were obtained from women attending antenatal clinics. From 2008 to 2011, 3353 pregnant women were tested with a mean prevalence of active syphilis found at 5.6/100,000. No pregnant women tested positive for HIV. Despite available resources and public health strategies similar to those existing in France, active syphilis prevalence is high in New Caledonia. Surprisingly, HIV seroprevalence remains far below the figures reported in mainland countries. However, social and economic changes as well as the looming referendum on independence scheduled in 2014 may have a potential negative impact on public health resources. The need for action to control syphilis and other curable sexually transmitted infections is pressing in order to prevent further spread of HIV in New Caledonia.
Introduction
Sexually transmitted infections (STIs) have been described as one of the major health problems in several countries of the Pacific Region.1–4 New Caledonia is an overseas French-administered territory located in the South Pacific and located 1500 km East of Australia. According to the 2009 census, the population comprises 245,580 inhabitants with a mean increase of 1.7% per year since 1996. One quarter of the population is aged less than 15 years old. After several immigration waves, the population, primarily of Melanesian origin, is now multiethnic and multicultural including Melanesian (40%), European (30%), Polynesian (11%), people of mixed ethnicity (8%), Indonesian (2%) and other ethnic groups (9%). The majority has an urban life style while one-third live in rural areas. The official language is French, although most non-western people speak a Melanesian or Polynesian dialect.
STI acquisition in New Caledonia is associated with STI-related risk behaviours including the neglect of the threat of STIs and of condom use, associated with underage sex (15–40%) and sex with multiple partners (5–25%). 5 Neglect of condom use is reported by 60% during casual sexual encounters 5 and by 40% during commercial sex. 6 Surveillance of STIs in New Caledonia has been limited to non-exhaustive passive reports of laboratory-confirmed STI cases from hospitals and health centres 7 or from limited sample size studies. 8 The aim of the study was to estimate the annual prevalence rates of HIV and active syphilis infections in pregnant women in New Caledonia from 2008 to 2011. HIV and syphilis testing is offered in New Caledonia within the framework of the national pregnancy follow-up scheme. Routine prenatal screening for HIV has been implemented since 1986. All pregnant women are encouraged to seek care in the first two trimesters of their pregnancy.
Methods
Blood samples were collected by midwives from women presenting for routine pregnancy screenings in 10 public antenatal clinics covering the whole population during a four-year period (2008–2011). HIV and syphilis tests were performed on a routine basis after collecting individual informed consent. After collection, specimens were transported daily in cool boxes for processing at the Institut Pasteur in New Caledonia. Sera were screened with rapid plasma reagin (RPR) (BioRad, Marne La Coquette, France) and reactive specimens were tested with Treponema pallidum haemagglutination (TPHA) (Siemens, Marburg, Germany). Serum HIV-1 and HIV-2 antibodies were measured by ELISA (Abbott, Wiesbaden, Germany; Biomérieux SA, Lyon, France), and reactive sera were confirmed by Western blot (Innogenetics, Ghent, Belgium). New cases of active syphilis were identified through the lab database. Laboratory definition of active syphilis was an RPR titer >4 and a TPHA titer >80. Patients found to be positive for HIV or found with active syphilis were referred to clinics for clinical assessment, counselling and treatment for both patients and partners. Risk factors for the acquisition of STIs were not assessed.
Results
Number of new patients tested positive for syphilis or HIV in antenatal clinics in New Caledonia, 2008–2011.
Discussion
The study demonstrated complete absence of HIV seroresponse and a high syphilis seroprevalence in more than 3000 pregnant women presenting for routine pregnancy follow-up. Our finding contrasts with the much lower syphilis seroprevalence found in general population of Western Europe and the USA. 9 This discrepancy may be explained by cultural factors including different attitudes, knowledge and practices regarding STIs. Although specific risk factors for the acquisition of STIs could not be analysed in our study, young age, multiple sex partners and poor education were independent risk factors for STI in the general population in New Caledonia. 5 The syphilis prevalence in our study population is still considerably lower than in New Caledonian risk groups, as 6% Treponema pallidum seropositivity was detected among 1983 STI clinic attendants in Noumea. 6 Interestingly, the occurrence of active syphilis was highest among Melanesian people, suggesting that syphilis disproportionately affects minority populations. Resurgence of syphilis has been observed among specific communities in several settings, such as in the USA 10 or in European countries. 11 There is an urgent need for implementation of culturally-customised public health programmes focused on safe sexual practices, syphilis awareness, and screening.
Our data showed that HIV seroprevalence has not increased in pregnant women over the study period. According to the national surveillance of HIV and AIDS, the prevalence per 100 000 people was 167 in 1996, 152 in 2003 and 140 in 2010. The total number of HIV-infected people in New Caledonia was calculated at 208 in 2011. Half of infected individuals were from European backgrounds. This low HIV seroprevalence likely reflects the sporadic pattern of infection that is found throughout most of the South Pacific. 3 The exact reasons for the current difference in syphilis and HIV spread remain unclear as specific risk factors are already present in New Caledonia. Lack of mixing between ethnic communities, adequate counselling and accessibility to treatment may explain the hitherto limited local HIV expansion. Future epidemiological studies might focus on the differential distribution of partners’ ethnicity in high-risk sexual group practices. Further, social and economic changes, high mobility of the population and increase in the number of sex workers subsequent to natural resources mining developments are major causes for alarm. Moreover, the looming referendum on independence scheduled in 2014 might negatively impact public health resources. Finally, other potential factors that render New Caledonia vulnerable to the spread of HIV include limited knowledge about how HIV is transmitted, unsafe sex, low rates of condom use, particularly among young people, high rates of multiple and casual partners and existence of commercial sex in the main cities. 7
Although HIV prevalence is still low in pregnant women, routine screening for HIV during pregnancy follow-up should remain a priority to detect in a timely manner, an emerging outbreak. Similarly, the syphilis routine screening for pregnant women in combination with a therapeutic strategy should be maintained for New Caledonia, especially considering the risk of congenital syphilis. During the study period, one congenital syphilis case was recorded in New Caledonia. In addition to controlling syphilis, it is important to be able to monitor other STIs, which are acknowledged to play a key role in the dynamics of HIV epidemics. 12
There are significant limitations to these data. First, not all pregnant women attended the study centres for antenatal follow-up leading to a potential underestimate of STI cases. Some women attended private clinics, while others had no follow-up at all facing numerous obstacles to early antenatal care, including cultural barriers, economic barriers, and misconceptions about the perceived and actual benefits of early antenatal care. Second, our study was relatively small and retrospective. However, it offered a unique opportunity to observe this paradoxical situation in a relatively isolated population of 250,000 in a small geographic area. The need for action to control syphilis and other curable STIs is pressing, in order to prevent further spread of HIV in New Caledonia. Innovative strategies for syphilis prevention are urgently required to address this public health issue in a country with geographical, linguistic and cultural diversity. Coordinated public health strategies, including strong case finding, disease surveillance and innovative culturally appropriate interventions for high-risk groups are required. Local and regional leadership are crucial to implement, monitor and evaluate intervention efforts to promote STI prevention and treatment in New Caledonia.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.