
Abstract
Global data on cervical lesion incidence and progression in HIV-positive women are essential for understanding the natural history of cervical neoplasia and informing screening policy. A systematic review was performed summarizing the incidence and progression of cervical lesions in HIV-positive women. Of 5882 HIV-positive women from 15 studies, incidence ranged from 4.9 to 21.1 cases per 100 woman-years for any cervical lesion and 0.4 to 8.8 cases per 100 woman-years for high-grade cervical lesions. HIV-positive women showed a median three-fold higher incidence of cervical lesions compared to HIV-negative women. Of 1099 HIV-positive women from 11 studies, progression from low- to high-grade lesions ranged from 1.2 to 26.2 cases per 100 woman-years. Both incidence and progression rates increased with lower CD4 counts. The effect of antiretroviral therapy on the natural history of cervical neoplasia remains unclear. HIV-positive women have higher incidence and progression of cervical neoplasia. Cervical cancer screening should be integrated into HIV treatment programmes.
Keywords
Introduction
In 2008, an estimated 33 million people were HIV infected worldwide, with 2.7 million newly-acquired HIV infections, most of which occurred in less developed countries. 1 HIV prevalence continues to rise due to both the high rate of new infections and the beneficial increase in life expectancy from antiretroviral therapy (ART). HIV is increasingly becoming a disease of women, with almost 50% of prevalent cases occurring in females. 1 This trend is particularly noticeable in sub-Saharan Africa where females have approximately three times the HIV prevalence of males. 1
Many resource limited nations that have high HIV prevalence also have high rates of cervical cancer because of limitations of screening and treatment. Cervical cancer is caused by infection with carcinogenic human papillomavirus (HPV) genotypes 2 and HIV infection is strongly associated with a higher prevalence, incidence, and persistence of HPV infection.3–6 Women with HIV have a higher prevalence of cervical squamous epithelial lesions (SIL) and invasive cervical cancer.7–13 Recognizing this connection, the US Centers for Disease Control and Prevention (CDC) declared invasive cervical cancer as an AIDS-defining illness in 1993. 14 Additionally, reducing cervical cancer in HIV-positive women is a primary focus of a joint public–private international initiative launched in 2011, the Pink Ribbon Red Ribbon initiative. 15
The large number of women living with HIV underscores the need to better understand the natural history of cervical precancer and cancer development in this high-risk population. While reports have linked HIV-related immunosuppression with an increased incidence of cervical precancer lesions and invasive cervical cancer,3,16 there is no global review compiling data on rates of incidence and progression of cervical neoplasia in HIV-positive women. Thus, we systematically reviewed the current literature on cervical precancer and cancer among HIV-positive women worldwide and examine important factors related to immunosuppression, including CD4+ T-cell count and ART use.
Methods
In order to identify studies related to cervical lesion incidence, a systematic literature search was conducted in MEDLINE for all studies indexed through 31 January 2012, with no specified start date, using the following search terms: (uterine cervical neoplasms [MeSH term] OR pap abnormality OR squamous intraepithelial lesions) AND cohort studies (MeSH term) limited to AIDS (keyword for HIV-related studies). Articles written in languages other than English were translated and reviewed for inclusion criteria. References of identified publications were also used to identify additional published articles for review. For cervical lesion incidence, studies were included if: (1) the study sample included 20 or more HIV-positive women; (2) a cohort design was used to assess incidence of SIL or greater and/or cervical intraepithelial neoplasia (CIN)1 or greater; and (3) study participants had normal cervical screen at baseline. Where possible, incidence rates were split for high-grade versus low-grade SIL and CIN (HSIL/CIN2-3 and LSIL/CIN1, respectively).
Articles reporting on cervical lesion progression were selected from the chosen incidence articles as well as through a separate MEDLINE search. The MEDLINE search was conducted for all studies indexed by 12 January 2012, using the following search terms: uterine cervical neoplasms (MeSH term) AND progression limited to AIDS (which limits the search to HIV-specific publications). Studies were included in the progression analysis if: (1) the study sample included 20 or more HIV-positive women; (2) a cohort design was used to estimate progression to SIL or greater and/or CIN1 or greater; and (3) study participants had atypical cells of unknown significance (ASCUS), low-grade SIL (LSIL), or low-grade CIN (CIN1) diagnosis at baseline.
Incidence and progression rates were reported as stated in the articles or estimated from reported number of cases, subjects, and median or mean follow-up time. Additionally, study cumulative risks of incidence and of progression were reported. Risk ratios were reported as stated in the articles or estimated using the ratio of the study cumulative risks. In this review, the term ART is broadly used to mean any ART use (monotherapy or greater). However, in the tables and results, ART and highly active antiretroviral therapy (HAART) were labeled as written in the individual articles with ART typically referring to monotherapy or dual therapy and HAART referring to triple therapy or greater. When the study included both women using ART and HAART, the term “mixed ART” is applied. When more than one article based on the same study population met the selection criteria for inclusion, the article with the largest number of women was used, unless multiple articles could contribute to separate analyses.
Results
Incidence of cervical lesions
Incidence rate estimates of cervical neoplasia from HIV-positive populations.

ART: antiretroviral therapy; HAART: highly active antiretroviral therapy; HIV: human immunodeficiency virus; SIL: squamous intraepithelial lesion; LSIL: low grade SIL; HSIL: high grade SIL; ASCUS: atypical cells of unknown significance; CIN: cervical intraepithelial neoplasia; STD: sexually transmitted disease; NS: not specified.
HAART.
Some cases confirmed by histology.
Estimated from [incident cases/(N normal at baseline × mean or median follow-up time)] × 100.
HIV+ / − combined.
For larger cohort.
Mixed ART/HAART, additional reference used. 32
From personal communication with author.
Mixed ART/HAART.
ART.
Cervical lesions were identified through cytology in all of the studies, with eight confirming some or all diagnoses with histology. Incidence rates of any SIL for HIV-positive women who had normal cytology at study entry ranged from 4.9 to 21.1 cases per 100 women-years (Table 1). In all studies that included HIV-negative populations (N = 6, 40%), the incidence rate of any SIL was greater in HIV-positive than HIV-negative participants, with a median three-fold increase in incidence (range 1.5–10.0). Incidence rates of LSIL ranged from 2.0 to 16.2 cases per 100 women years (Table 1 and Figure 1). Rates of HSIL/CIN2-3 for HIV-positive women varied from 0.4 to 8.8 cases per 100 women-years. Studies with both HIV-positive and HIV-negative populations showed higher rates of HSIL/CIN2-3 for HIV-positive participants. As an additional measure, study cumulative incidence of LSIL and of HSIL, though not comparable between studies as study length was variable, also consistently showed higher risk for HIV-positive participants than for HIV-negative participants within the same study.
Incidence rates reported or calculated for LSIL (A) or HSIL (B) in HIV-positive women. Rates are reported as cases per 100 woman-years. Solid lines show unweighted mean rate. Dotted lines show 95% confidence intervals around the unweighted mean. *This study reports CIN2-3. LSIL: low-grade squamous epithelial lesion; HSIL: high-grade squamous epithelial lesion; CIN: cervical intraepithelial neoplasia.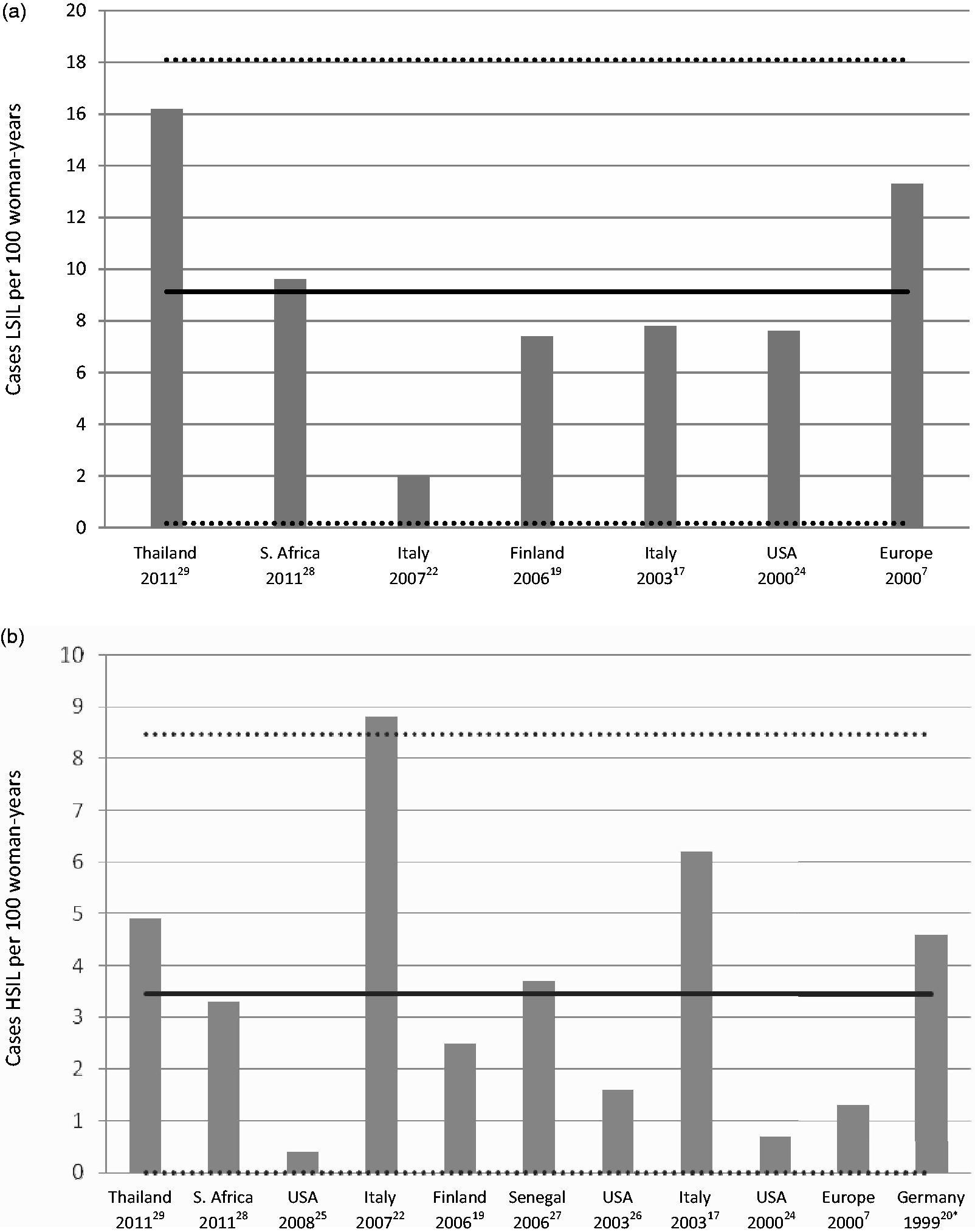
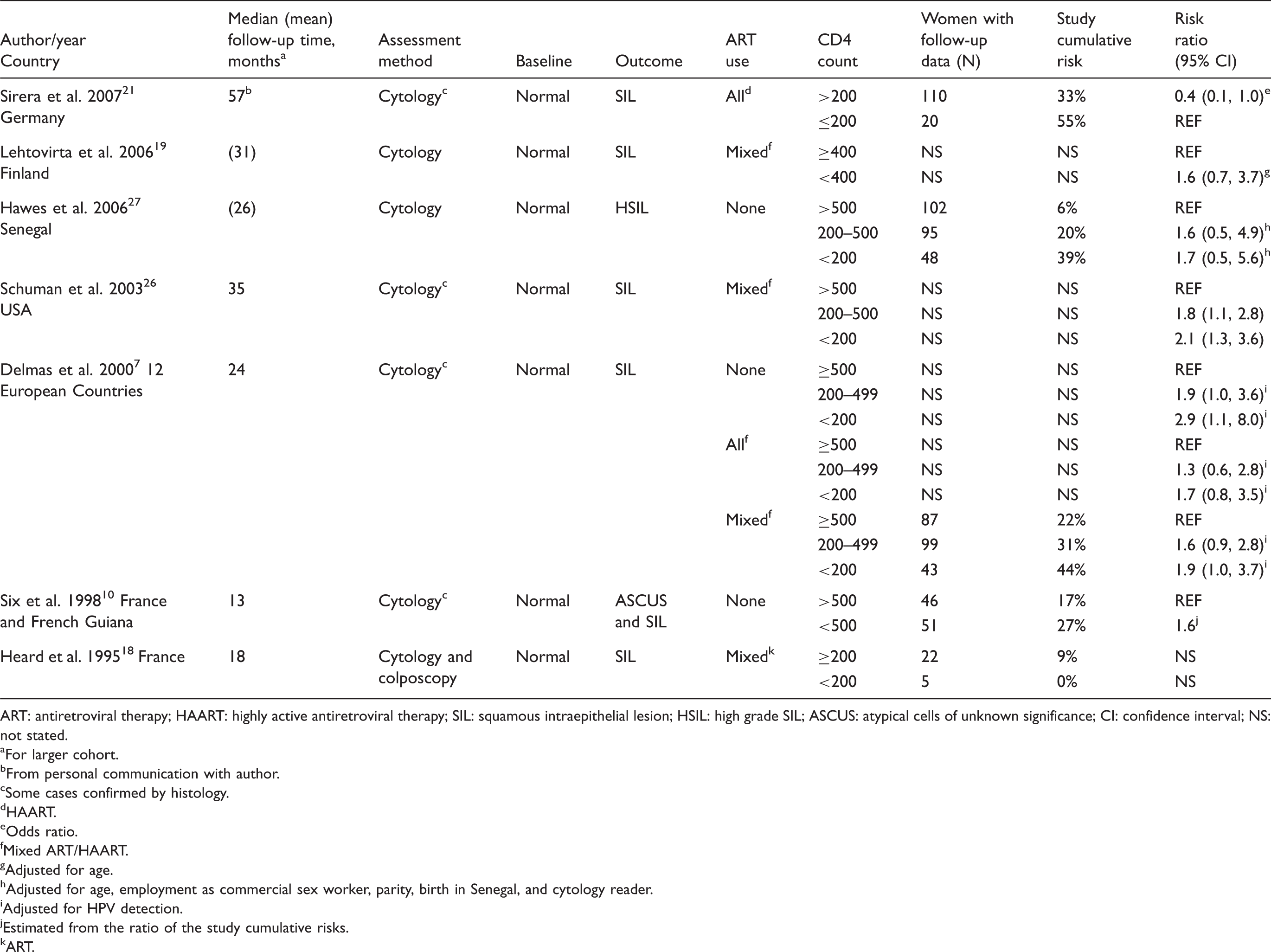
Incidence stratified by CD4 counts and antiretroviral use
Cervical neoplasia incidence estimates stratified by CD4 count in HIV-positive populations.
ART: antiretroviral therapy; HAART: highly active antiretroviral therapy; SIL: squamous intraepithelial lesion; HSIL: high grade SIL; ASCUS: atypical cells of unknown significance; CI: confidence interval; NS: not stated.
For larger cohort.
From personal communication with author.
Some cases confirmed by histology.
HAART.
Odds ratio.
Mixed ART/HAART.
Adjusted for age.
Adjusted for age, employment as commercial sex worker, parity, birth in Senegal, and cytology reader.
Adjusted for HPV detection.
Estimated from the ratio of the study cumulative risks.
ART.
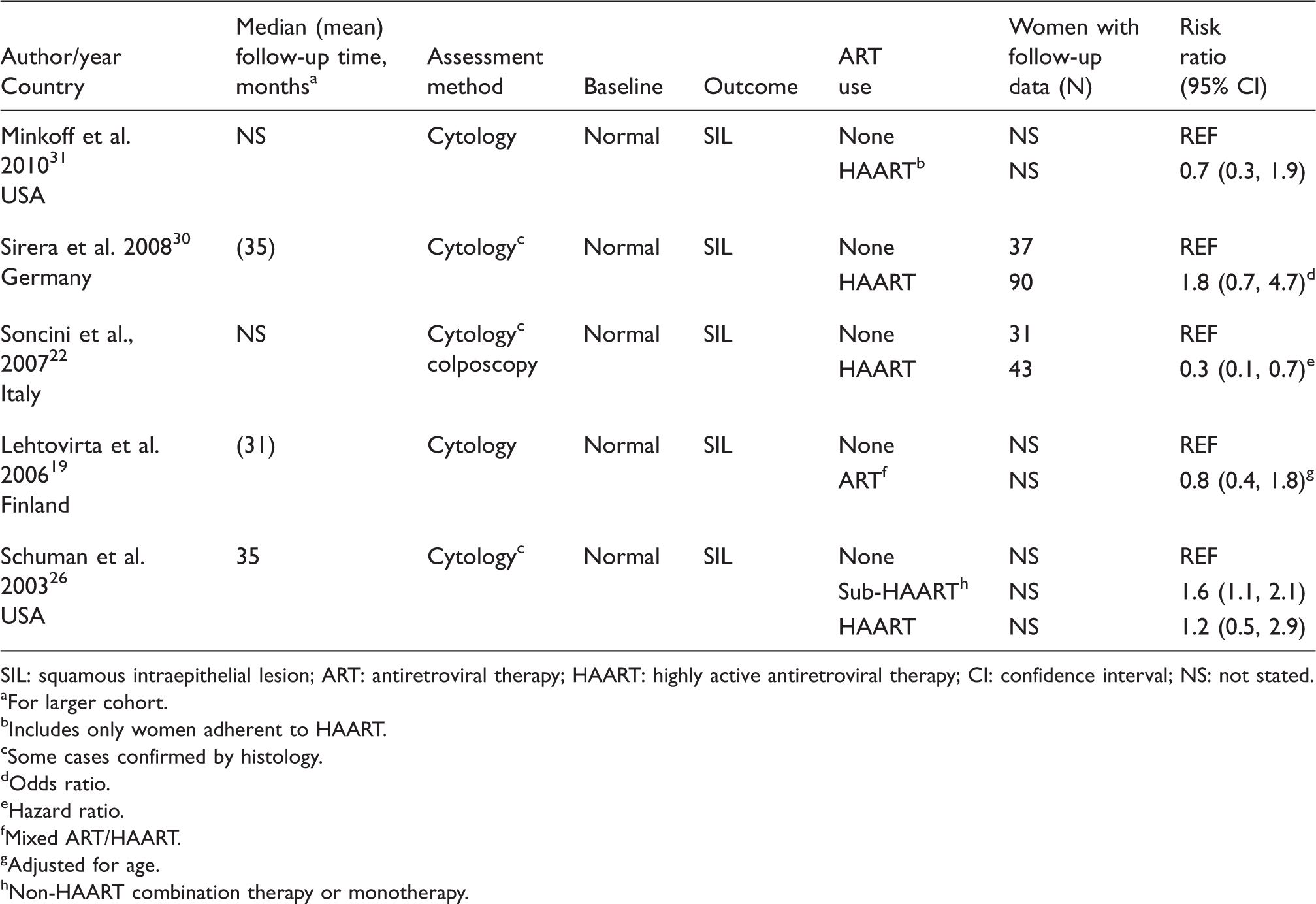
Cervical neoplasia incidence estimates stratified by anti-retroviral use in HIV-positive populations.
SIL: squamous intraepithelial lesion; ART: antiretroviral therapy; HAART: highly active antiretroviral therapy; CI: confidence interval; NS: not stated.
For larger cohort.
Includes only women adherent to HAART.
Some cases confirmed by histology.
Odds ratio.
Hazard ratio.
Mixed ART/HAART.
Adjusted for age.
Non-HAART combination therapy or monotherapy.
Progression of low-grade lesions
Progression rate estimates of cervical neoplasia from HIV-positive populations.

ART: antiretroviral therapy, HAART: highly active antiretroviral therapy, HIV: human immunodeficiency virus, ASCUS: atypical cells of unknown significance, SIL: squamous intraepithelial lesion, LSIL: low grade SIL, HSIL: high grade SIL, CIN : cervical intraepithelial neoplasia, NS: not specified.
For larger cohort.
HAART.
Additional reference used. 26
Mixed ART/HAART.
Estimated from [number progressed / (N at baseline × mean follow-up time)] × 100.
Some cases confirmed by histology.
ART.
HIV+/– combined.
Control arm.
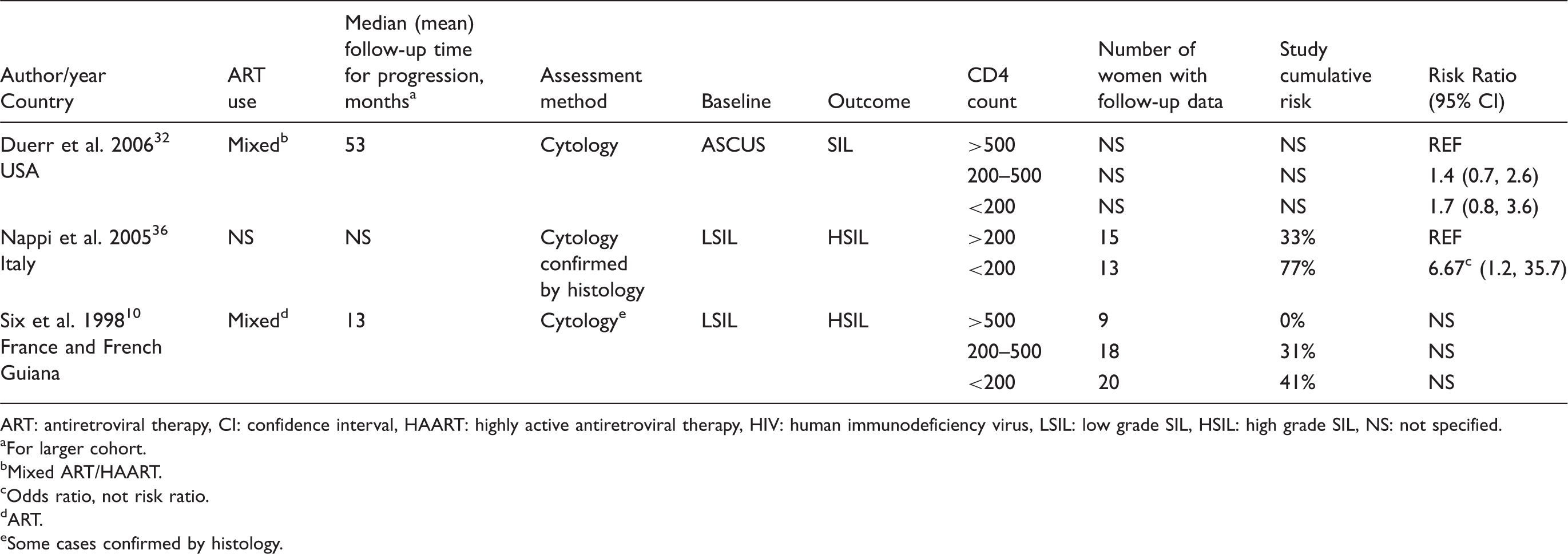
Cervical lesion progression rates from LSIL/CIN1 to greater than LSIL/CIN1 (most commonly HSIL/CIN2-3) for HIV-positive women ranged from 1.2 to 26.2 cases per 100 women-years. Two studies followed women with ASCUS at baseline,32,33 finding a rate of 13.7 cases of SIL per 100 women-years and 3.2 cases of HSIL per 100 women-years. Study cumulative risks, though not comparable between studies, were higher for HIV-positive participants than for HIV-negative participants in all five studies that included both populations.10,32,34,36,39
Progression of lesions stratified by CD4 counts
Progression estimates for cervical lesions stratified by CD4 count in HIV-positive populations.
ART: antiretroviral therapy, CI: confidence interval, HAART: highly active antiretroviral therapy, HIV: human immunodeficiency virus, LSIL: low grade SIL, HSIL: high grade SIL, NS: not specified.
For larger cohort.
Mixed ART/HAART.
Odds ratio, not risk ratio.
ART.
Some cases confirmed by histology.
Discussion
Our comprehensive search identified 15 studies reporting incident cervical lesions and 11 studies reporting progression of cervical lesions for HIV-positive women. These studies showed a wide range of incidence and progression rates for cervical lesions in HIV-positive populations. In studies with both HIV-positive and HIV-negative populations, the incidence rate of cervical lesions was a median three-fold higher in HIV-positive women as compared to HIV-negative study participants. HIV-positive women were also at least twice as likely to have cervical lesions that progressed in severity as compared to HIV-negative women. The majority of studies showed that lower CD4 counts were associated with increased incidence and progression of cervical lesions in HIV-positive women; however, this relationship was usually not statistically significant, often due to small sample size per strata of CD4 counts.
The evidence on ART use and cervical lesion incidence was less consistent. Though one study showed a reduction in incidence with HAART use versus non-HAART use, 22 most studies found no significant difference between HAART/ART use and non-use.19,26,30,31 Associations may be confounded by the practice of initiating ART use only in patients with low CD4 counts or lack comparability due to differences in CD4 count recovery, HIV viraemia, and follow-up time after ART initiation. Additionally, ART treatment has evolved since its introduction so it is important to note that many of the study populations that received ART were receiving single or dual drugs as compared to current standard of triple drug combinations (HAART) currently in practice. Life expectancy of HIV-positive individuals on HAART is also increasing and thus a greater number of HIV-positive women may be susceptible to cervical cancer and associated diseases in the future. In addition, an important gap in the literature is the effect of HAART use and progression of cervical lesions. Minkoff et al. 31 found a significant increase in clearance of SIL among adherent women on HAART (adjusted odds ratio 2.4; 95% confidence interval 1.1–5.2) as compared to pre-HAART. 31 Two more recent studies, published after the cut off for this analysis, also found a reduction in progression or increase in regression for consistent users of HAART.40,41 The relationship of HAART use and progression may become more defined when additional analyses are done in cohorts of women only on HAART and when HAART adherence and effectiveness are considered.
As both HIV and HPV are sexually transmitted infections, the increase in cervical lesions found in HIV-positive women may be due to shared behavioural risk factors such as high number of sexual partners or high-risk sexual partners. However, biological mechanisms have also been implicated. The increased risk of cervical lesion development and progression seen in women with HIV is postulated to be due to both an impaired immune system and an increased potential for unregulated cell growth. For example, cervical molecular profiles of HIV-positive women show alterations in oncogenic and immunogenic protein expression.42–44 Additionally, there is evidence linking the HIV-1 transactivator protein (Tat) with increased expression of HPV oncogenes and proliferation of HPV-infected cells. 45 Together these data indicate an altered immune response to HPV infection and an altered natural history of cervical cancer in HIV-positive women. In alignment with the hypothesis that impaired immune function reduces the ability to clear HPV infection, thus increasing the probability of developing cervical precancer and cancer, most studies found an inverse association between level of immunosuppression, as indicated by CD4 counts, and the incidence and progression of cervical lesions.7,10,19,21,26,27,32,36
Our review is limited, however, by the small number of studies reporting rates for cervical lesion incidence and progression, making between-study comparisons difficult. Where possible, rates were approximated based on median follow-up time. This review identified gaps in the literature on incidence and progression of cervical precancer in HIV-positive women. Most studies had a median age for study participants in the low 30s; few studies reported on older populations. Given the increased life expectancy of HIV-positive women due to HAART, assessment of this growing demographic of women 30 years and older is needed. Additionally, HIV viral load was not systematically extracted in this analysis due to the general lack of consistent data throughout the studies. Also, we did not find studies meeting our criteria that addressed the effects of HAART use on progression risk from low-grade lesions. A recent large study, which was not included in our literature review, reported that HAART use reduced the rate of cervical lesion progression from LSIL (rate ratio 0.52 for HAART users versus ART non-users). 40 HAART use has also been associated with a reduction in the combined rate for incidence and progression of cervical neoplasia (rate of any progression from normal or LSIL baseline), though not always reaching statistical significance.28,40,46–48 Additionally, evidence shows that HAART use increases the rate of regression of precancerous lesions.31,49,41
The compiled research highlights the high risk of cervical precancer development and progression in HIV-positive women. This risk appears to be greater in women with reduced immune function but more evidence is needed to determine how HAART use modifies risk of incidence and progression. Our findings reinforce the importance of screening for cervical lesions in HIV-positive populations, particularly those with lower CD4 counts that are at a higher risk for both incident and progressive cervical disease outcomes. Given the healthcare resources focused on HIV care, integrating cervical screening with HIV treatment programmes is essential to reduce untimely death of women from this preventable cancer.
Footnotes
Contribution to Authorship
SD performed the literature search, extracted data, and prepared the manuscript. AR helped with manuscript preparation, contributed subject matter expertise, edited and reviewed the manuscript. CF provided subject matter expertise, edited and reviewed the manuscript. JT checked the data extraction, edited and reviewed the manuscript. JS provided subject matter expertise, edited and reviewed the manuscript.
Conflict of interest
The authors declare no conflict of interest.
Funding
This manuscript was supported by CFAR development award AI50410.