
Abstract
Immune reconstitution inflammatory syndrome is a clinical entity with a broad presentation, described in both HIV and non-HIV-infected patients. We report a case of Mycobacterium avium-complex pericarditis as a rare but life-threatening manifestation of this syndrome in a patient with AIDS.
Immune reconstitution inflammatory syndrome (IRIS), after initiation of antiretroviral therapy (ART), is the progression of subclinical disease or increased clinical severity of existent opportunistic infections.1,2 Mycobacterium avium-complex (MAC) infection, one of the first reported manifestations of IRIS in AIDS patients, occurs with CD4+ cell counts below 50–100 cells/uL prior to starting ART.3,4 Typically, MAC infection-related IRIS includes mediastinal lymphadenopathy, peripheral lymphadenitis, pulmonary disease and/or intra-abdominal disease.3,4 We report a rare occurrence of MAC pericarditis in an AIDS patient, in the setting of IRIS.
A 35-year-old Mexican immigrant was diagnosed with AIDS in August 2010 when hospitalized for cryptococcal meningitis. Throughout 2010 he was treated for recurrent cryptococcal meningitis, coccidioidomycosis oral fistula, cytomegalovirus infection and toxoplasmosis chorioretinitis. The patient had previously been prescribed ART in 2010 but had not taken his medication. Early in 2011, he became compliant with ART (emtricitabine-tenofovir-efavirenz) and opportunistic infection prophylaxis, including azithromycin 1200 mg/week and trimethoprim/sulfamethoxazole 1 DS (160mg/800mg)/daily. His HIV-1 RNA load decreased from 129,338 copies/mL to 484 copies/mL and CD4+ cell count increased from 7 cells/uL to 90 cells/uL over 5–6 months.
In July 2011, he presented to the hospital with shortness of breath, pleuritic pain and productive cough for two weeks. Review of systems was notable for 10 lb weight loss and orthopnoea. He denied haemoptysis, fevers, chills or night sweats. He stopped his emtricitabine-tenofovir-efavirenz when he became ill.
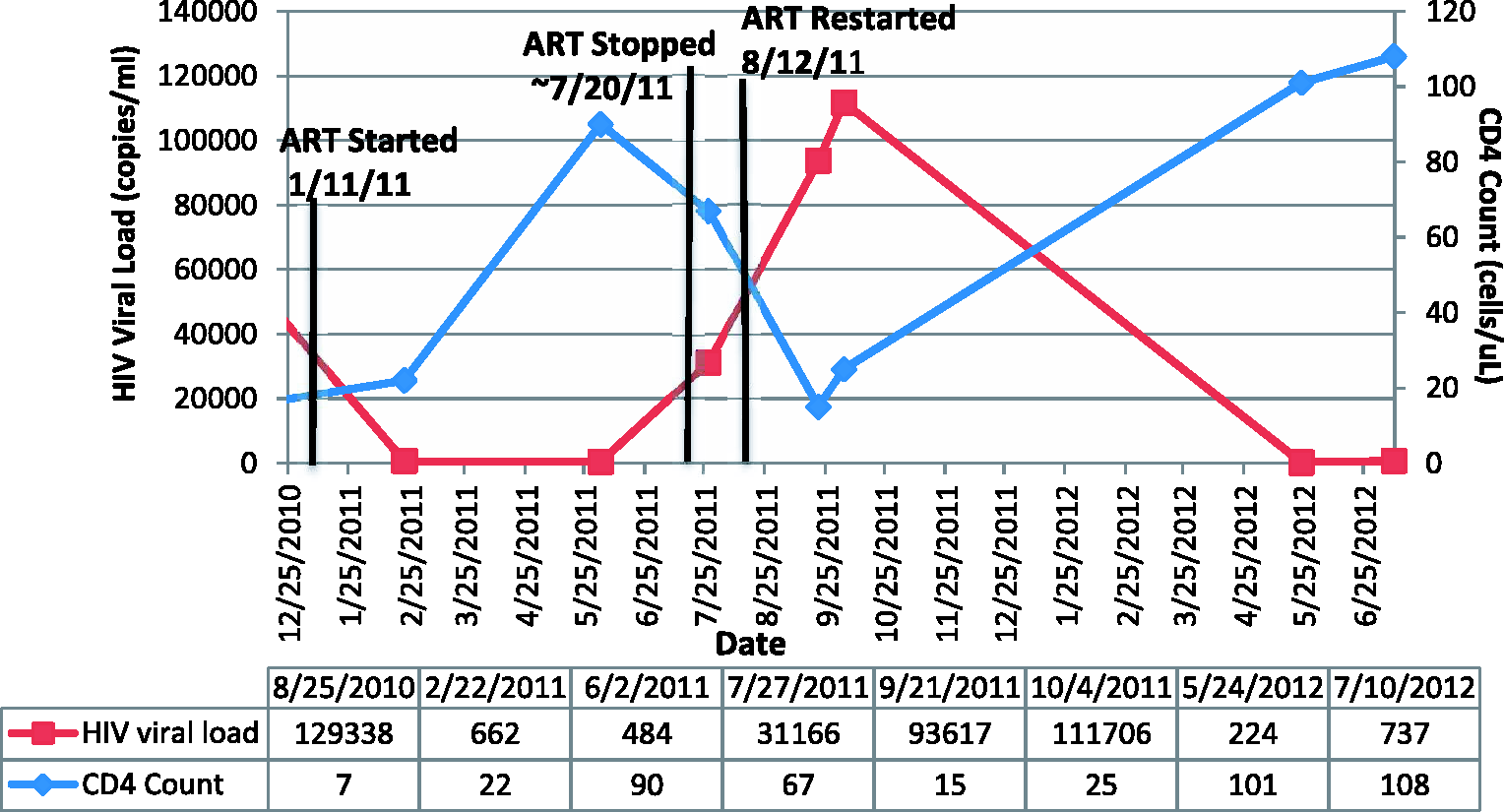
His vital signs were unremarkable except for a heart rate of 130. Jugular venous distension was noted on examination. The patient was tachycardic with a regular cardiac rhythm and a notable pericardial rub. No murmur was present. On pulmonary examination, rhonchi were noted in the right upper lobe without rales. Chest X-ray (Figure 1(b)) showed cardiomegaly suggestive of a pericardial effusion, and a right upper lobe consolidation. Chest computed tomography (Figure 1(c) and (d)) showed a large pericardial effusion with fluid tracking into the mediastinum, enlarged mediastinal lymph nodes, right upper lobe and multifocal consolidations. His CD4 count and HIV viral load trends are illustrated in Figure 2.
CXR and chest CT: (a) CXR one week prior to admission: normal, (b) CXR on admission: significant cardiomegaly (c) and (d): chest CT: right upper lobe infiltrate with high density mediastinal fluid tracking into the pericardium. Graph representing the patient’s HIV viral load and CD4 count on the y-axis over time. Included in the graph is when the patient began taking his ART with marked improvement in his CD4 count and decrease in his HIV viral load. Also indicated is when the patient self-discontinued his ART due to illness and was restarted on ART while in the hospital.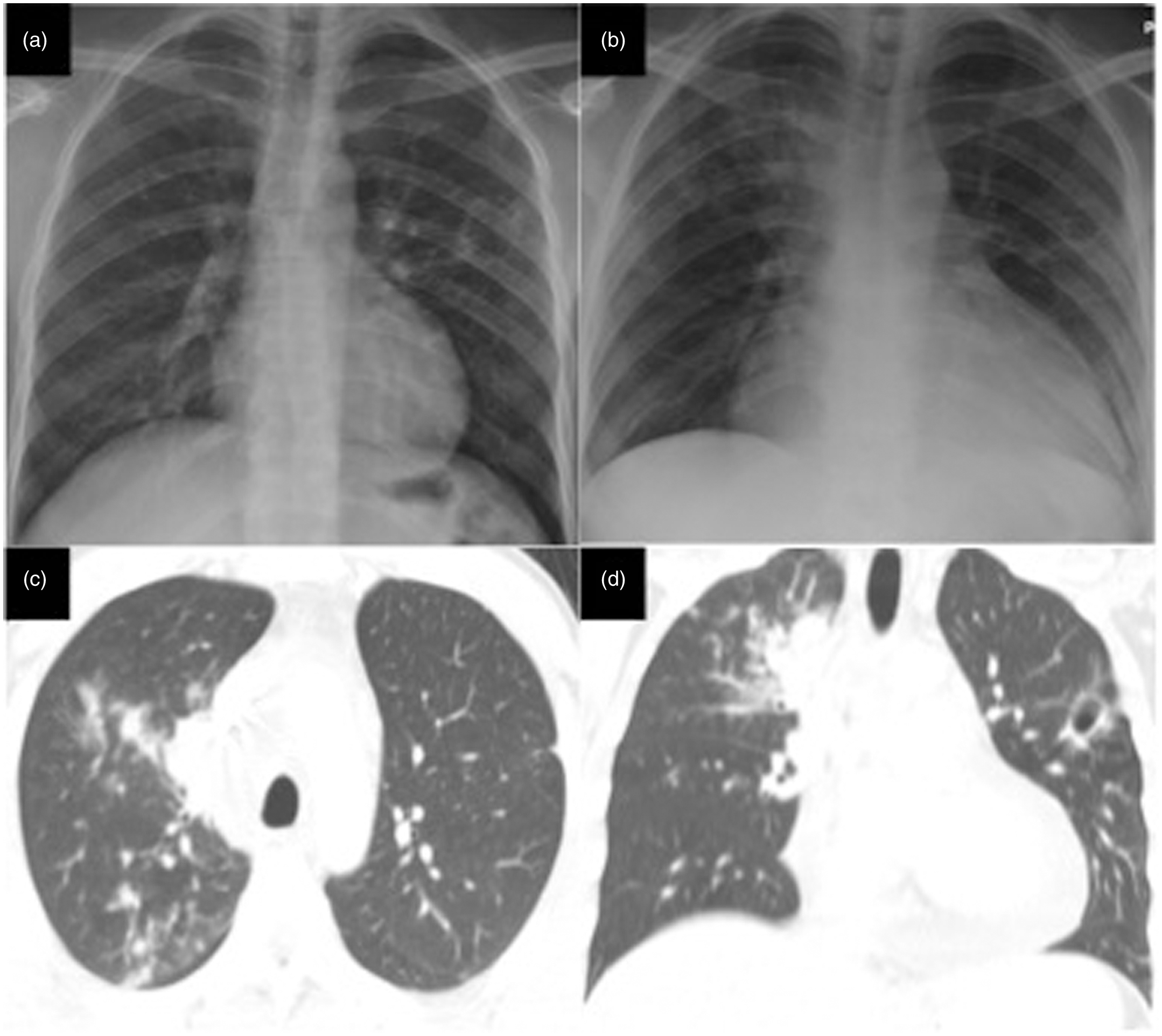
Transthoracic echocardiogram showed thickened pericardium, moderate pericardial effusion and tamponade physiology. He became hypotensive and underwent an urgent pericardial window. Approximately 500 mL of pericardial fluid was drained showing inflammatory infiltrates and reactive mesothelial cells. The operative note described a shaggy and thickened pericardium and inflamed epicardium. Surgical pathology showed fibrinous exudative pericarditis with macrophages and rare giant cells. Acid fast bacilli (AFB), Grocott-Gomori's methenamine silver, Truant’s and mucicarmine stains of pericardium showed no microorganisms. Sputum AFB stain was positive for organisms. AFB culture from pericardial fluid, pericardium and sputum were eventually positive for MAC. AFB blood isolator was negative.
The patient was diagnosed with MAC pericarditis and disseminated infection. Rifampin, ethambutol, isoniazid and pyrazinamide were started as part of four-drug therapy empirically for tuberculosis and once MAC was identified, antimicrobial therapy was de-escalated and azithromycin 500 mg daily and ethambutol 1200 mg daily were administered. Emtricitabine-tenofovir-efavirenz was re-started two weeks after MAC treatment. The patient improved clinically and also as evidenced on repeat echocardiogram.
This case illustrated the rare manifestation of MAC pericarditis in an AIDS patient. The patient had a rapid decrease in HIV-1 RNA load and increase in CD4+ cell count in response to ART. This quick recovery and timing of MAC pericarditis, several months after starting ART, was consistent with IRIS. MAC infection in the setting of IRIS is a well-known entity. 3 Phillips et al. 4 reported the incidence of MAC infection among patients initiating ART to be 3.5% over a 12-year period. A meta-analysis of IRIS reported that 16.1% of 13,013 HIV patients initiating ART developed IRIS-related infections. 2 The highest incidence of IRIS was reported in association with CMV retinitis, 37.1% of infections, while Kaposi’s sarcoma was the least common, at 6.4%. 2 This study showed patients with low CD4+ cell counts, particularly below 50 cells/uL, prior to ART were at risk for IRIS. 2
Onset of MAC-related IRIS following ART initiation was observed on average at four weeks, but ranged from 1–52 weeks.3,4 Most patients had rising CD4+ cell counts with decreasing HIV viral loads, reported in both non-nucleoside reverse transcriptase inhibitor-based and protease inhibitor (PI)-based ART regimens. 3 Phillips et al. 4 reported peripheral lymphadenitis in 33% of their cohort patients. However, fever and weight loss, not peripheral lymphadenitis, were most commonly reported in AIDS patients with disseminated MAC in the pre-highly ART era. 5 Among MAC infection-related IRIS patients, AFB smears were positive in 28% of tissue specimens submitted, but cultures were MAC positive in 60% of specimens. 4 Only one case of MAC pericarditis with IRIS was reported over a 12-year observation in the Phillips et al.’s 4 study. Another case of MAC pericarditis related to IRIS was described with a similar presentation to our case. 6 However, the reported patient was on a PI-based ART regimen. 6
Our patient, given his initial low CD4+ cell count pre-ART and rapid clearance of HIV-1 RNA load after starting ART, was at risk for IRIS. He had no history or documented symptoms of MAC infection prior to ART. He was taking azithromycin 1200 mg/week for primary prophylaxis for MAC infection. Our patient likely had a pulmonary infection which spread to his pericardium. Disseminated MAC infection with pericardial involvement is an important and life-threatening diagnosis to consider in patients at risk for IRIS.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.