
Abstract
Genitourinary case records of 42 pregnant women with syphilis were reviewed as part of a regional audit following the re-emergence of congenital syphilis in the north east of England. National standards, from the British Association of Sexual Health and HIV guidelines on managing syphilis in pregnancy, were met in the majority of cases with 69% being treated according to national guidance and all cases completing treatment. Locally developed standards on multidisciplinary working and communication were met less well, with particular issues regarding the documentation of pregnancy outcomes in GUM records and communication between specialities being highlighted. A regional good practice guide has been developed and implemented to address standards not met, reduce adverse outcomes and prevent future cases of congenital syphilis.
Introduction
The north east of England has the smallest regional population in England; however, in 2010 it had the third highest rate of sexually transmitted infections, including syphilis. An increase has been seen in the number of syphilis cases in heterosexual women over the last decade in this region 1 resulting in the re-emergence of cases of congenital syphilis. These cases prompted a local review of care pathways and syphilis in pregnancy management within Genitourinary Medicine (GUM).
Method
A series of audit standards, based on British Association of Sexual Health and HIV (BASHH) guidelines2,3 and locally agreed good practice, were developed by members of a multidisciplinary group. BASHH guidelines have no specific pregnancy standards, so local standards covered areas thought important in pregnancy care such as preventing re-infection, receiving nationally agreed treatment, communication between specialties and documentation of pregnancy-specific syphilis advice. In addition to audit data, demographic and clinical details (including appointment and pregnancy outcomes) were collected.
A retrospective case note audit was carried out in 10 of the 12 GUM services within the north east of England. This was undertaken by each service in autumn 2011. Three services had recently been transferred to a private provider, and there was difficulty in accessing patient records from two of these sites. Women diagnosed with syphilis of any stage (excluding previously known and treated syphilis) between 1 January 2006 and 31 December 2010 were included in the audit, by searching GUM systems for all syphilis KC60 codes. This audit was restricted to those who were pregnant.
Results
A total of 98 women were diagnosed with syphilis in the time period, 42 of whom were pregnant (46%). Data are presented for pregnant women only.
Auditable standard results.
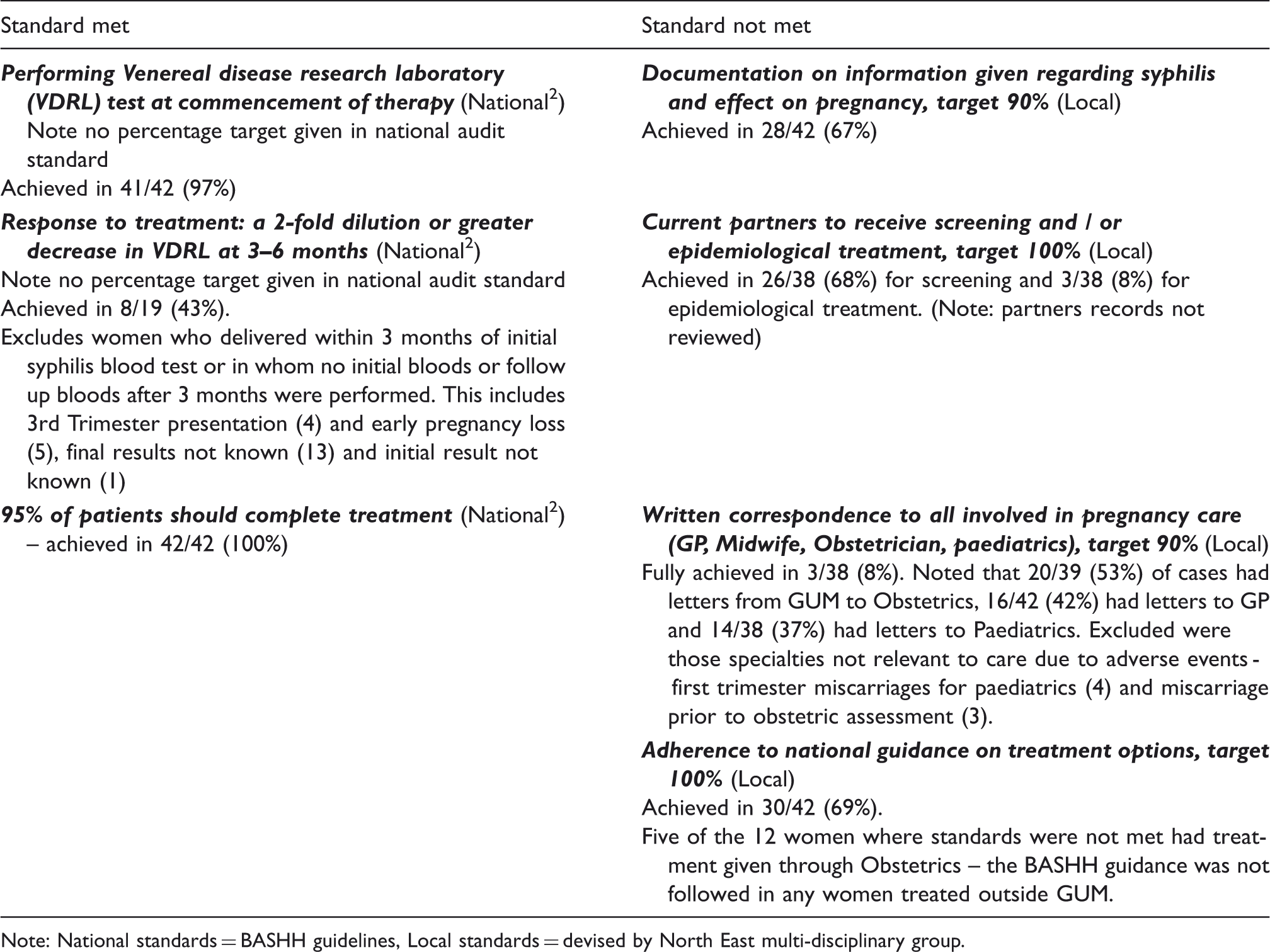
Note: National standards = BASHH guidelines, Local standards = devised by North East multi-disciplinary group.
Twenty-three (55%) pregnant women were white British. Seventeen (40%) had early syphilis (primary, secondary or early latent) and 23 (55%) had late syphilis. In two cases, the stage was not clear from the clinical records. Four women were already under GUM follow-up for treated syphilis when they became pregnant (range 4 weeks to 1 year since treatment). Although 38 (90%) had a regular partner, seven (18%) of these women had a partner who worked away from home and four (10%) of all women had a casual partner in the last 12 weeks.
The majority of women 24 (57%) were seen in GUM within seven days of their result being available to the antenatal team, nine additional women were seen within four weeks, but one woman took eight weeks. In four cases, the date of the result being available to the antenatal team was not clear in the GUM notes. When they first attended GUM, 13 (31%) were in their first trimester, 20 (48%) women were in their second trimester and four (9.5%) were in their third trimester. Nine (21%) women were lost to follow-up during their pregnancy for monitoring of syphilis serology. In three (7%) cases, the child protection team were involved, and one of these women was co-infected with HIV.
Pregnancy outcomes were poorly recorded in the majority of GUM records. In 21 (50%) cases, there was no record of any outcome, nine (21%) cases had ‘healthy baby’ documented in the notes and three (7%) sets of notes had ‘congenital syphilis excluded’ recorded. Adverse outcomes affected nine (21%) of pregnancies (five miscarriages, one stillbirth, one ‘unhealthy baby’ and two cases of proven congenital syphilis).
In the first case of congenital syphilis, the mother’s booking bloods were negative for syphilis. During her pregnancy, she was imprisoned, and as Prison Healthcare could not access her booking blood results, they were repeated at 28 weeks and returned positive (VDRL 1:64, IgM positive). She reported three previous pregnancies. Referral into GUM services was delayed and she was not seen until 32 weeks when she received two doses of benzathine penicillin one week apart. She delivered at 33 weeks, a few days following her second dose. Her regular partner tested negative.
In the second case, the mother was diagnosed with syphilis on her antenatal booking bloods and was referred into GUM. Her initial bloods in GUM at 15 weeks showed her IgM to be positive and her VDRL was 1:64. She was treated with a single dose of benzathine penicillin. She attended follow-up, and her VDRL and IgM were both negative by 32 weeks. She delivered at 36 weeks. At delivery, her baby’s blood results showed a VDRL of 1:4 and a negative IgM. The baby had bloods repeated at four weeks, by which time the VDRL was 1:32 and the IgM was positive. Both mother and baby were then lost to follow-up with child protection involved. It was concluded that the mother had become re-infected in late pregnancy as five months post-partum she re-attended and her repeat VDRL was 1:64 and her baby’s had risen to VDRL >1:256 with a positive IgM.
Discussion
Although national BASHH audit standards were met, local standards, which were developed for this audit and not known at the time of managing the women, were not. There are many reasons as to why this may have occurred. Local standards addressed multidisciplinary communication, specific patient information relating to pregnancy, partner notification to prevent re-infection and 100% adherence to national treatment guidance standards to reduce risk of treatment failure and litigation in the case of congenital infection. Some of the delays in referral into GUM services were due to bloods being repeated in antenatal services and no clear pathway existing between specialties.
Syphilis in women has been a rare occurrence in non-GUM specialties, so low levels of awareness exist. The national guidance documents that have been developed are specialty-specific and no ‘single pathway’ document is available.2,4,5 There is the potential for cases to ‘fall through the gaps’ and the use of anonymised GUM patient numbers makes it difficult to match maternal and infant laboratory specimens.
This audit was limited by not reviewing current partners’ clinical records and relying on information provided about partners in the index patient’s records. The number of current partners screened and treated may actually have been higher but not documented in the women partners notes. Obstetric and neonatal records were similarly not reviewed. These could potentially have provided additional information regarding pregnancy outcomes.
This audit focussed on pregnant women seen in GUM services; however, for a more complete understanding of the data after completing the audit, we looked at whether all women who were positive for syphilis on their antenatal booking bloods were seen in GUM. A discrepancy was seen between the number of positive antenatal screens (reported to Public Health England directly from antenatal screening coordinators and/or laboratories), number of enhanced surveillance forms returned (completed and returned to Public Health England from GUM services for each syphilis patient) and national syphilis code numbers (coded in GUM services and sent quarterly to Public Health England to assess national and regional trends). It is possible that some of these women were seen in GUM services but either felt to have been adequately treated for syphilis in the past or simply not given the appropriate clinical code in error. It is, however, also possible that some women who may have required treatment never actually reached GUM. To determine whether women had missed opportunities for syphilis treatment, an audit within antenatal services would need to be undertaken and the fact that these data are not included is recognised as a limitation of our audit. A national code for ‘pregnant women attending GUM with previously treated syphilis and no further action required’ would be helpful in determining if women were not being referred into GUM.
Subsequent to this audit, a regional document entitled ‘Good practice arrangements for the management of women and babies with syphilis’ has been developed and implemented. Representatives from GUM, Health Protection, Obstetrics, Paediatric Infectious Diseases, Microbiology and Antenatal services were involved and it is hoped that it will help to raise awareness of increasing syphilis rates in women, improve communication, reduce women lost to follow-up, ensure treatment is given according to BASHH guidelines within level 3 GUM services and ensure current regular partners receive screening and epidemiological treatment. The document sets out who is responsible for the overall care of the patient at various stages of the patient journey as detailed below:
Antenatal screening: Confirmatory bloods should be undertaken in GUM to reduce any delay in referral.
GUM: Maternal syphilis serology samples should be requested under the patient name and not the GUM number (with informed consent) to make comparison to baby samples more straightforward. There should be written correspondence from GUM to colleagues in Obstetrics, Paediatrics, Midwifery and General Practice and a copy should be kept in the antenatal hand held records. BASHH national guidance should be followed, particularly regarding treatment options. GUM should take responsibility for anyone who defaults their follow-up appointments. The management of syphilis in pregnancy should be confined to level 3 GUM services.
Paediatrics: A protocol for assessment of the baby with the recommendation that paired blood samples are taken within 24 h of birth from mother and baby should be followed. Any older siblings should also be tested.
Health protection surveillance: The enhanced surveillance system has been updated to collect prospective data on all pregnant women diagnosed with syphilis to monitor whether standards are being met and to record pregnancy outcomes. From this, analysis and feedback from public health should occur annually to address any issues. Some higher prevalence areas are also considering screening partners for syphilis in antenatal services and re-screening women in the third trimester.
Other audits undertaken in England have commented on similar findings regarding inter-specialty communication.6–8 The use of a multidisciplinary good practice arrangements document could be used in other regions in the UK and in other countries where similar multispecialty care applies to the management of pregnant women with syphilis. We recommend some pregnancy-specific standards be incorporated into the national BASHH syphilis guidelines, particularly around communication between specialties.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgements
The authors thank all members of northern BASHH group for their input and support of this audit.