
Abstract
Summary
The cause of posterior reversible encephalopathy syndrome (PRES) is often multifactorial. It is uncommon in patients with human immunodeficiency virus (HIV) infection. However, if the cause of PRES is left untreated it can cause significant morbidity and mortality. Thus, we believe it should be included as a differential in immunosuppressed patients presenting with neurological signs. This case report describes such a patient with acquired immunodeficiency syndrome (AIDS) who developed hypocalcaemia secondary to disseminated histoplasmosis.
Keywords
Introduction
Histoplasmosis is rare in the UK. This case describes a patient with hypercalcaemia secondary to disseminated histoplasmosis who developed posterior reversible encephalopathy syndrome (PRES) which presented as seizures.
Case reports for PRES in patients with human immunodeficiency virus (HIV) infection are few, being associated with hypertension, end-stage kidney disease, combination antiretroviral therapy (cART) and opportunistic infection (tuberculosis, Mycobacterium avium intracellularae [MAI], blastomycosis and varicella zoster virus infection).1–6 Hypercalcaemia has been associated with PRES in patients with HIV: an adult with MAI 5 and a child with advanced HIV. 2
Case description
A 26-year-old Nigerian woman with no medical or medication history presented with vomiting, abdominal pain and cough for three weeks.
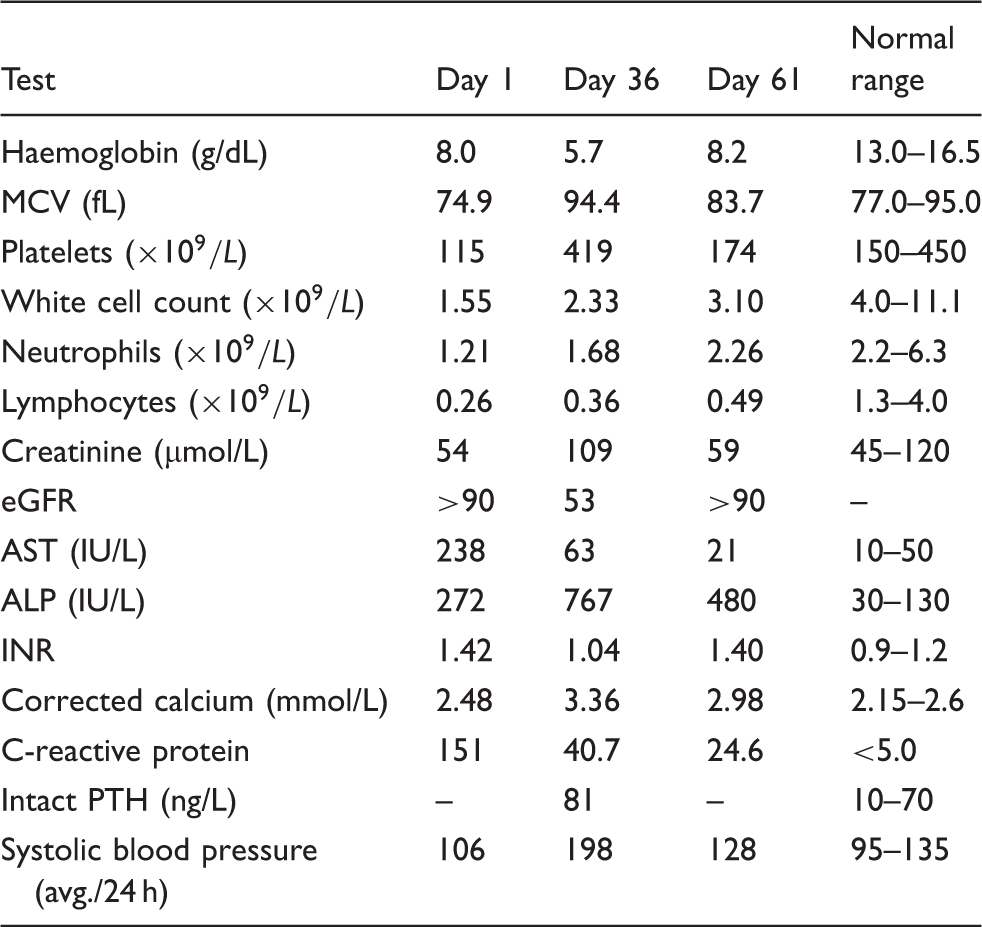
Laboratory results (note seizures on day 36 and day 61).
An HIV test was positive for antibodies to HIV-1, with a CD4 count of 2 cells/μl (1%) and an HIV-1 RNA of 5.5 log copies/ml. A computed tomography (CT) scan of the abdomen, pelvis and thorax showed hepatosplenomegaly. A diagnosis of Histoplasma capsulatum was confirmed on Grocott staining of a cervical lymph node and bone marrow trephine. She was started with liposomal amphotericin B 3 mg/kg OD. No other opportunistic infections were identified on bronchoalveolar lavage, cerebrospinal fluid (CSF), blood or bone marrow cultures. CSF analysis was normal. She was transferred to critical care with worsening renal and liver functions. She became anuric on day 11 and commenced on haemofiltration (creatinine 204 µmol/L, eGFR 26).
The patient subsequently suffered two generalised seizures on day 36. A magnetic resonance imaging (MRI) of the brain showed features suggestive of PRES (see Figure 1) with bilateral parieto-occipital oedema affecting predominantly the white matter. Hypercalcaemia was thought to be secondary to histoplasmosis infection and treated with prednisolone 40 mg daily.7,8 Hypertension was treated with amlodipine and metoprolol. Tenofovir, emtricitabine and raltegravir were commenced.
MRI scan (T2 weighted) showing parietal-occipital PRES (left). MRI scan (T2 weighted) showing resolution of parietal-occipital PRES (right).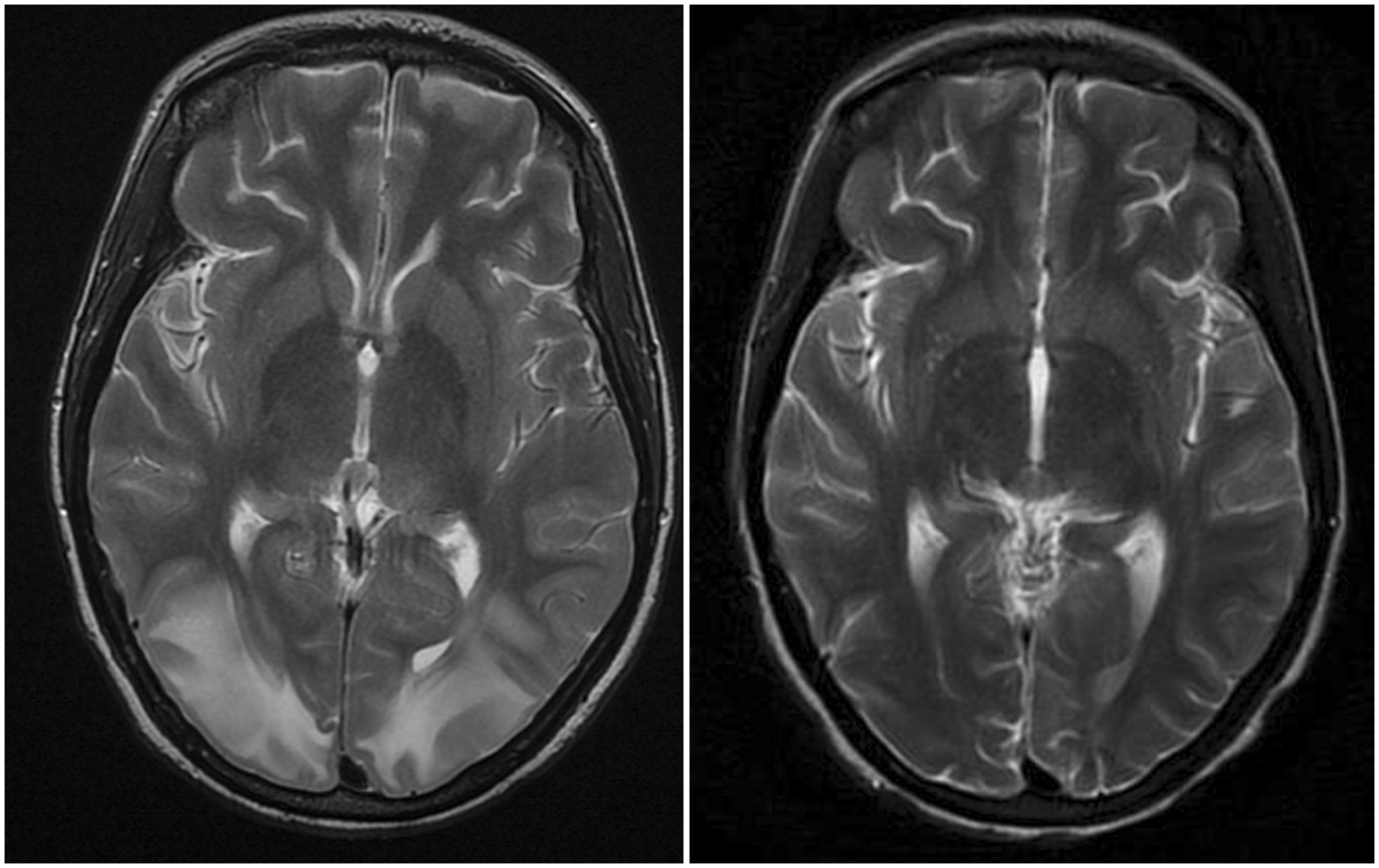
Corrected calcium was 2.56 g/ml after seven days of corticosteroids, which were stopped on day 50. Corrected calcium levels increased to 2.98 g/ml after steroid cessation and she became confused. She had a further single generalised seizure on day 61. Corticosteroids were restarted and tapered over four weeks with close monitoring of serum calcium. CT brain at the time of the second seizure episode showed bilateral parieto-occipital low density change consistent with PRES. An MRI of the brain scan two weeks later, when calcium was normal, showed resolution of the radiological features of PRES (see Figure 1).
Discussion
PRES is characterised by headache, confusion, seizures and visual loss. It is thought to occur due to vasogenic oedema due to disruption of the bloodflow to the blood-brain barrier leading to white-matter changes and has a number of aetiologies. 6 PRES is diagnosed on the basis of clinical as well as neuroradiological findings. In patients with PRES and normal blood pressure, including hypercalcaemia,1,9 the mechanism is thought to be cytotoxicity. Immune system (T-cell) activation leads to endothelial cell activation, resulting in vascular instability. This results in vasoconstriction and downstream hypoperfusion with subsequent blood-brain barrier dysfunction and vasogenic cerebral oedema. 6
Disseminated histoplasmosis rarely causes hypercalcaemia, 10 the cause of which is believed to be similar to other granulomatous diseases where hypercalcaemia is caused by an extrarenal overproduction of calcitriol. 7 Hypercalcaemia in these cases is treated with steroids. 8 This patient had a raised parathyroid hormone as a result of renal failure11,12; unfortunately, vitamin D levels were not performed. However, the rapid response of the calcium level to steroids on two occasions suggests the aetiology is unlikely to be primary hyperparathyroidism. 13 Subsequent calcium levels post-discharge have been normal.
Disseminated histoplasmosis is a rare diagnosis in HIV-infected individuals in Europe. Hypercalcaemia is a rare complication. PRES is a clinicoradiological diagnosis of a reversible cause of white matter change with multiple aetiologies.
In this patient, a single cause for the first episode of PRES is difficult to determine as the patient was hypertensive with hypercalcaemia and renal failure. However, at the time of the second seizure episode, the patient was normotensive with normal renal function making hypercalcaemia more likely.
The cause of PRES is often multifactorial. 6 Although uncommon in patients with HIV infection, it should be considered as a differential in immunosuppressed patients who develop neurological signs.
The patient remains well after one year of follow-up.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.