
Abstract
Summary
Due to the shared risk factors for viral transmission, coinfection of human immunodeficiency virus (HIV) and hepatitis C virus (HCV) is common. This study examined the seroprevalence of HCV among HIV–infected patients in inpatient and outpatient settings. A retrospective chart review of 256 HIV–infected patients was conducted in Prince George's Hospital Center (inpatients from 1 September 2011 to 1 March 2012) and Glenridge Medical Center (outpatients from 1 January 2011 to 31 December 2012). The mean age of the population was 46 ± 12 and 44 ± 11 for inpatients and outpatients, respectively. HIV–infected men comprised 61.9% inpatients and 64.8% outpatients. The overall prevalence of HCV infection in HIV/AIDS patients was 12.5% (32/256), with a higher prevalence in the inpatient group than that in the outpatient group (24.6% vs 11.2%, p < 0.01). The percentages of drug abuse (43.8% vs 16.5%, p < 0.01) and alcoholism (25.0% and 14.3%, p < 0.05) in HCV/HIV–coinfected patients were higher than those in HIV–monoinfected patients. In addition, only 64.9% of HIV–infected and 50.0% of HCV/HIV–coinfected inpatients were followed up with outside care after discharge. To our knowledge, this study, for the first time, revealed that HCV/HIV coinfection was significantly higher in inpatients compared to outpatients. Considering the high prevalence and comorbidities associated with HCV/HIV coinfection, it is recommended that evaluation of hepatic damage, especially fibrosis, should be initiated during hospitalization as well as outpatient care.
Keywords
Introduction
Both human immunodeficiency virus (HIV) and hepatitis C virus (HCV) can cause chronic infections. Due to the shared risk factors for viral transmission (including injection drug use, sexual transmission, blood transfusion, occupational exposures, etc), coinfection of HIV and HCV is common. The prevalence of HCV infection is approximately 1.3% in the United States population, 1 however, among HIV-infected patients, HCV prevalence is much higher and varies by risk factors between 10.2 and 80.8%. 2 It is estimated that approximately 1.2 million HIV-infected patients in the United States are coinfected with HCV. 3 Currently, liver disease is one of the leading causes of hospitalization and death in HIV-positive individuals, and co-infection with the HCV is a major contributor to this trend. According to the latest D:A:D survey, 4 liver disease represents 9% of deaths in HIV-positive patients. It is well known that HIV infection has deleterious effects on the natural course of HCV infection, which results in a higher rate of HCV progression to fibrosis and hepatocellular carcinoma due to the presence of immunosuppression associated with HIV infection. HCV may also contribute to increased morbidity and mortality in coinfected individuals through chronic immune activation and HCV-associated proinflammatory pathways, 5 which ultimately lead to an increased risk of cardiovascular event, kidney disease, mental illness and cancer in this population. 6
Current guidelines recommend that all HIV-infected patients receive HCV screening and more recently, the US CDC recommended all ‘baby boomers’ (born during 1945 through 1965) should be screened for HCV infection.7,8 Considering the different comorbidities and critical medical conditions between inpatient and outpatient HIV/AIDS patients, the prevalence of HCV infection may be different. In the current study, we retrospectively reviewed 256 HIV-infected patients' charts at Prince George's Hospital Center in Maryland and compared the prevalence of HCV/HIV coinfection based on the type of care (inpatient vs outpatient).
Materials and methods
Study design
This cross-sectional study was conducted at Prince George's Hospital Center, an inner city hospital serving Maryland/DC great metro area, and Glenridge Medical Center, an ambulatory care/outpatient centre affiliated with Prince George's Hospital Center. This study examined retrospective electronic medical records (EMR) of 97 inpatients and 159 outpatients who were infected with HIV.
Data collection and analysis
We extracted demographic information and clinical information including inpatient (Prince George's Hospital Center) and outpatient (Glenridge Medical Center) ICD-9 diagnosis codes. The data collection for this study was approved by the Institutional Review Board of Prince George's Hospital Center. Descriptive statistics were computed to describe the demographic and clinical variables. Fisher's exact test was performed to analyze categorical variables. p < 0.05 was considered statistically significant. PRISM 5.0 software was used to analyze the data (GraphPad Software, Inc.).
Results
Demographics
Demographics of HIV-infected patients.
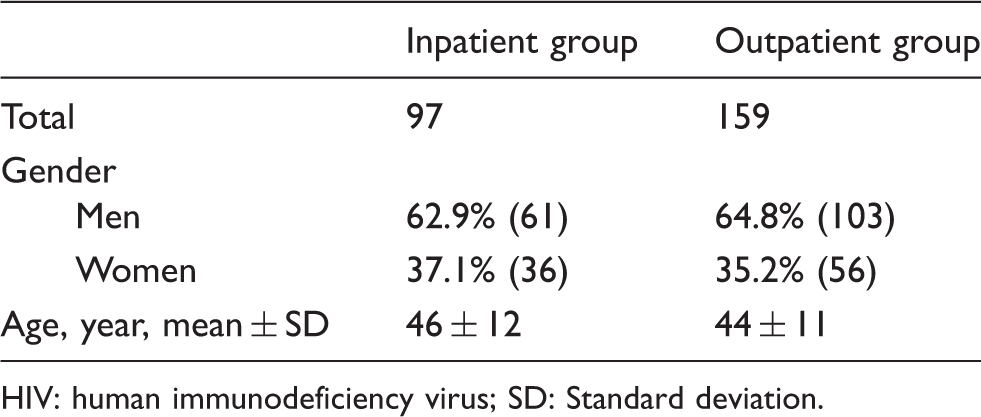
HIV: human immunodeficiency virus; SD: Standard deviation.
Clinical characteristics of HIV-infected inpatients and outpatients
Clinical characteristics of HIV-infected inpatients and outpatients.
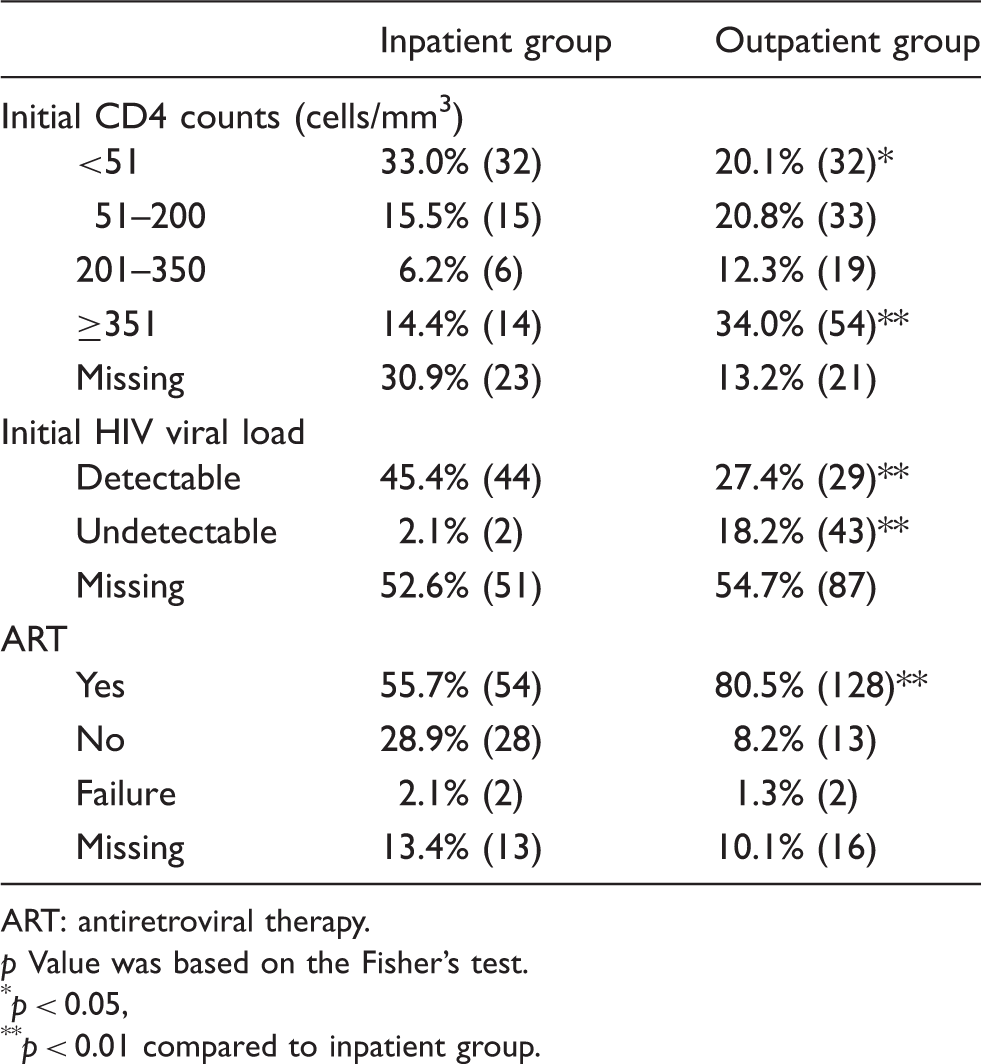
ART: antiretroviral therapy.
p Value was based on the Fisher's test.
p < 0.05,
p < 0.01 compared to inpatient group.
HCV infection in HIV/AIDS patients
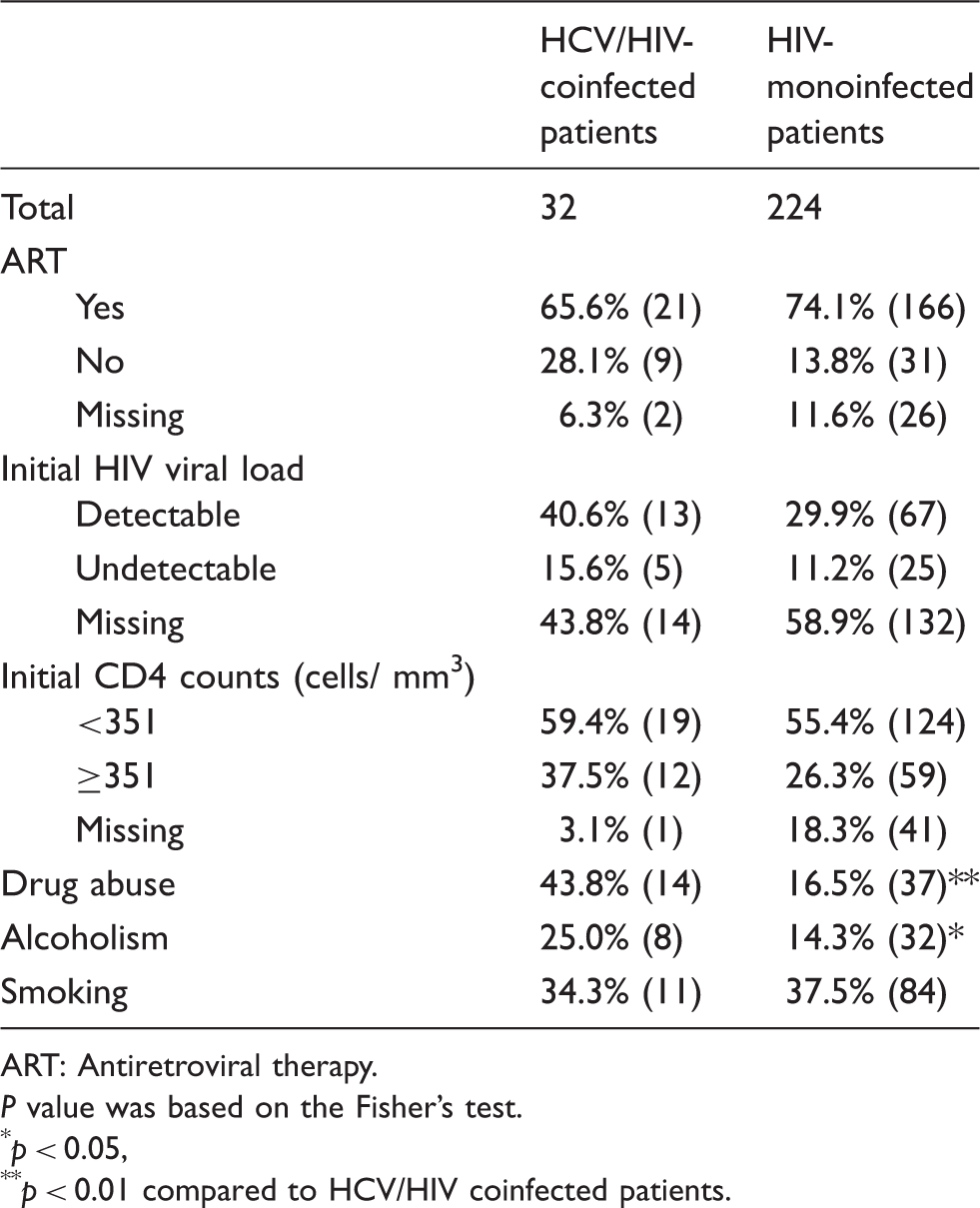
The overall prevalence of HCV infection in HIV/AIDS patients was 12.5% (32/256), with a higher prevalence in the inpatient group than that in the outpatient group (24.6% vs 11.2%, p < 0.01) (Figure 1). As shown in Table 3, a similar percentage of patients were on ART between HCV/HIV coinfected and HIV monoinfected inpatients (65.6% and 74.1%). Patients with detectable initial HIV viral load and initial CD4 counts <351 cells/mm3 in HCV/HIV coinfected patients and HIV monoinfected patients was 40.6% vs 29.9% and 59.4% vs 55.4%, respectively. The percentage of drug abuse (43.8% vs 16.5%, p < 0.01) and alcoholism (25.0% vs 14.3%, p < 0.05) was higher in HCV/HIV coinfected patients compared to HIV-monoinfected patients. No significant difference was found in smoking between the two groups.
The prevalence of HCV coinfection in HIV-infected inpatients and outpatients. Fisher's test was performed. *p < 0.01. Comparison of HIV-related variables and risk factors among HCV/HIV-coinfected and HIV-monoinfected patients. ART: Antiretroviral therapy. P value was based on the Fisher's test. p < 0.05, p < 0.01 compared to HCV/HIV coinfected patients.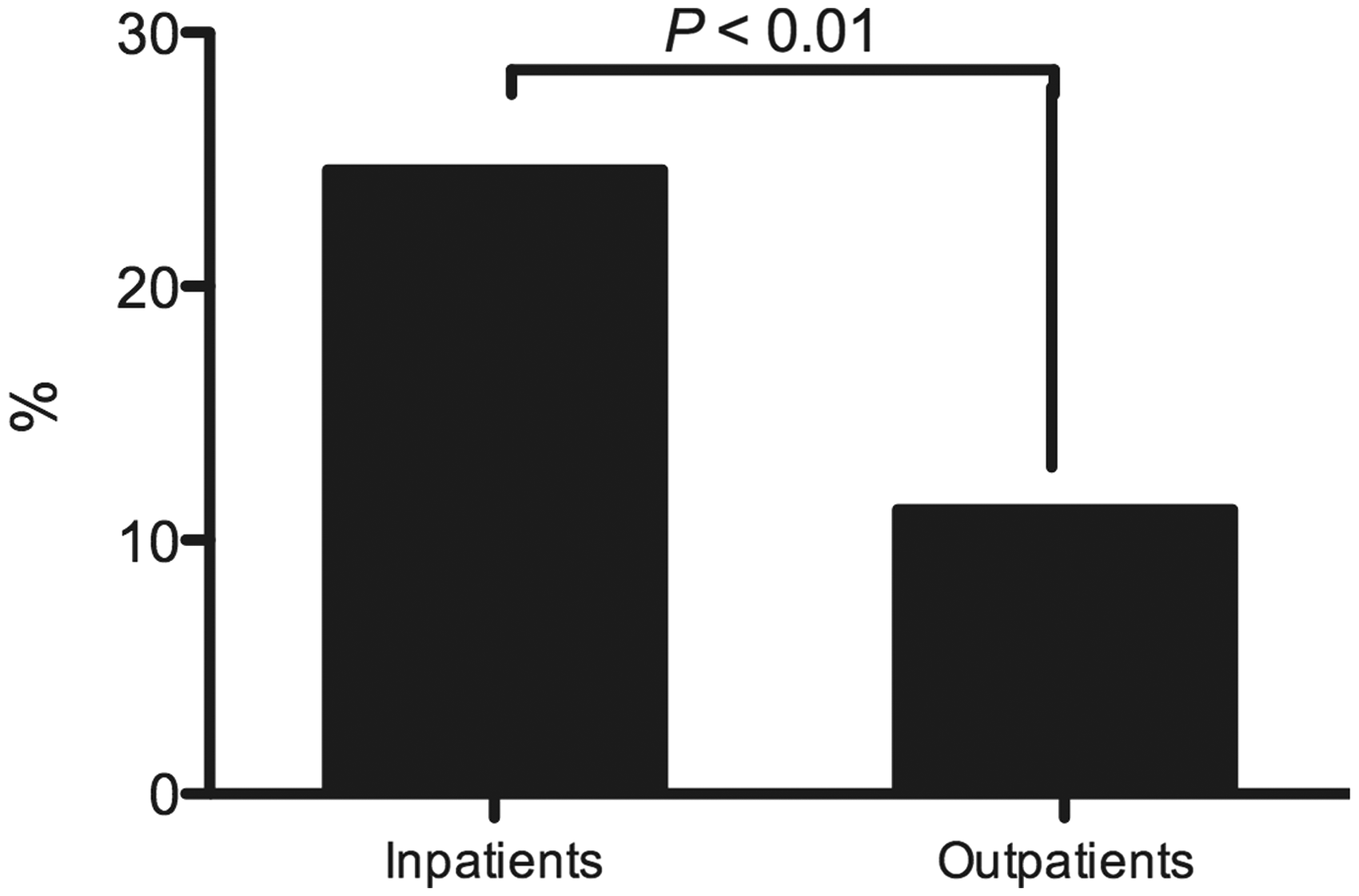
The comorbidities of HIV-infected inpatients
Among the 97 HIV-infected inpatients, the average number of admissions was two and mean length of stay was 7.2 days. The comorbidities between HIV-monoinfected and HCV/HIV-coinfected patients included: altered mental status (17.5% vs 37.5%), mental illness including major depression and suicidal ideation (14.4% vs 31.3%) and proteinuria (33.0% vs 43.8%). Furthermore, only 64.9% of HIV-monoinfected inpatients and 50.0% of HCV/HIV-coinfected inpatients were followed up with outside care (Figure 2).
Comorbidities and follow-up in HIV-monoinfected and HCV/HIV-coinfected inpatients. AMS: altered mental status. Mental illness includes major depression and suicidal ideation.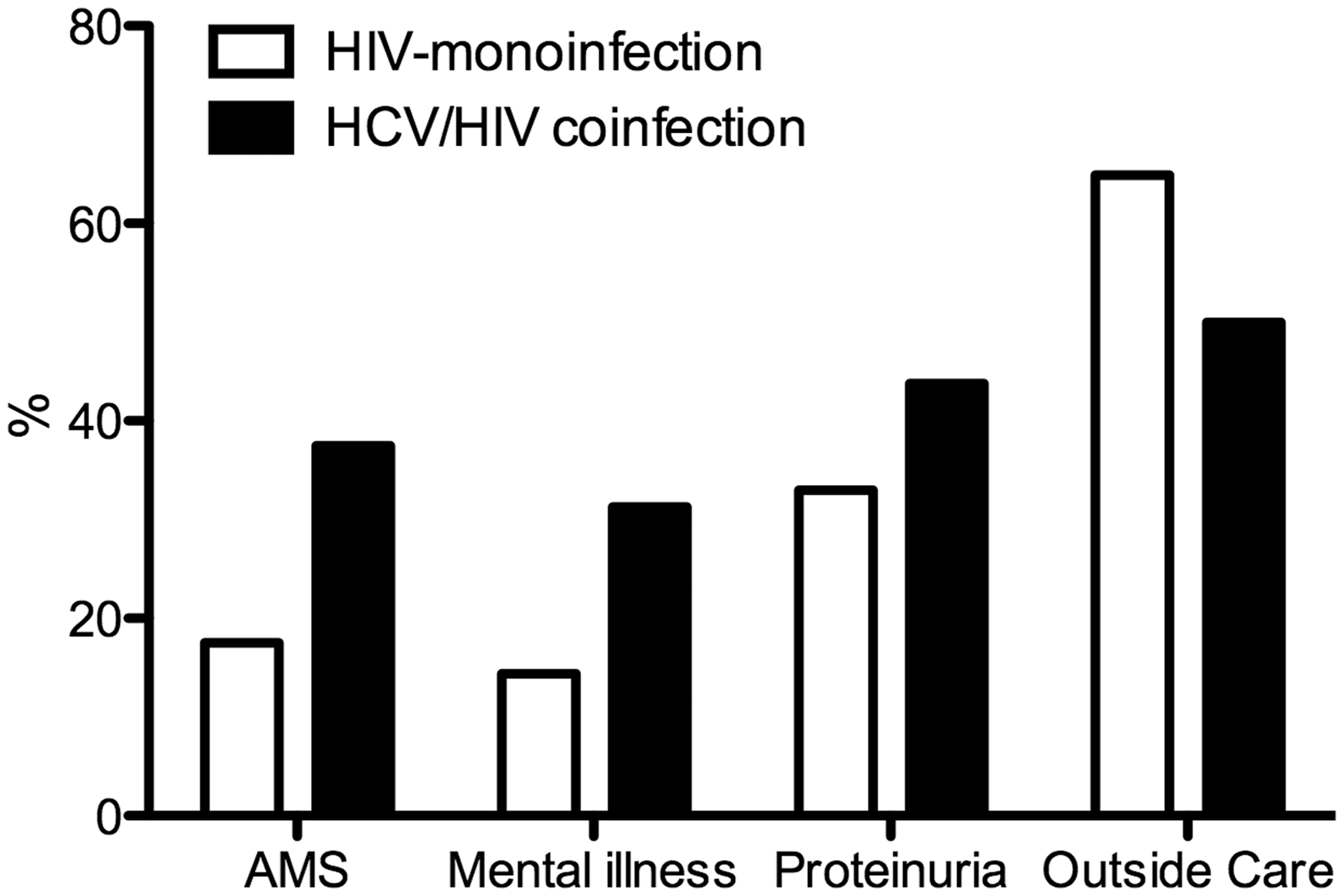
Discussion
HCV-related liver disease is an important contributor to morbidity and mortality in the HIV-infected population. In the current study, the prevalence of HCV infection was 12.5% in HIV/AIDS patients (24.6% for inpatients and 11.2% for outpatients, respectively), which is lower than 33.0% described by Staples et al. 9 in the Atlanta VA Cohort Study (HAVACS). Despite the diverse patients' socio-economic and demographic statuses, the difference was most likely due to the different routes of viral transmission among risk groups. The prevalence of HCV/HIV coinfection varies markedly among risk groups. Our study reported that 43.8% of HCV/HIV-coinfected patients and 16.5% HIV-monoinfected patients were drug users. Sherman et al. 10 reported that HCV seroprevalence in HIV-infected patients ranged from 4% in low-risk patients population to 73% in the high-risk population, especially intravenous drug users (IVDU). Rosen et al. 11 reported 65% seroprevalence of HCV infection in HIV-positive prisoners. In other countries such as Ukraine and Russia where IVDU is the main route of HIV transmission, Soriano et al. 12 reported that coinfection rate is as high as 70%. Our study, consistent with other reports, showed HCV prevalence among HIV-infected patients is significantly higher than the 1.3% of general prevalence of HCV infection in the United States population, which is mainly due to shared modes of transmission of the two viruses. Our data about initial CD4 counts and HIV viral load indicate that inpatients' immune systems are weaker than that of outpatients. In addition, a significantly lower percentage of inpatients underwent ART and had more comorbidities, which may explain our finding about high HCV/HIV-coinfection prevalence in inpatients compared to outpatients.
Despite the controversy regarding whether HCV infection does or does not have a deleterious effect on the course of HIV infection, 13 current guidelines recommend that ART should be considered for HCV/HIV-coinfected patients regardless of CD4 counts. Our study reported a similar percentage of patients receiving ART between HCV/HIV-coinfected and HIV-monoinfected inpatients, i.e. 65.6% vs 74.1%. No significant difference was detected between the two groups for their initial detectable HIV viral load and initial CD4 counts, which was consistent with the report by Rockstroh et al. 14 that HCV serostatus did not affect virologic and immunologic responses. On the other hand, there is well-established evidence for faster liver disease progression in HCV/HIV-coinfected patients compared to HCV monoinfection. 15 From a meta-analysis, 16 individuals with HCV/HIV coinfection had increased risk of progression to liver fibrosis and decompensated liver disease as well as extrahepatic manifestations and morbidities such as kidney disease, cardiovascular event and cancer. All of these support the need for treating hepatitis C as early as possible in this patient population. However, due to poor efficacy of the standard treatment peginterferon/ribavirin (Peg IFN/RBV), the reality is that a majority of HCV/HIV-coinfected individuals may not be evaluated for or receive therapy at all. In our patient population, less than 5% of HCV/HIV-coinfected patients received anti-HCV treatment. Fortunately, recently published clinical trials with new proteinase inhibitors (PIs) telaprevir or boceprevir have yielded substantial advances in the field. 17 However, due to the complexity of treatment for both HIV and HCV, current guidelines recommend to prefer initiating ART and delaying HCV therapy in patients with low CD4 counts (<200 cells/ mm3), and deferring ART until completion of HCV therapy in ART-naïve patients with CD4 counts >500 cells/mm3. The challenges during the management including potential drug–drug interactions, overlapping toxicities and large pill burden still exist, and thus it is wise to manage under the close supervision of a multidisciplinary team.
Since no vaccine against either of these viruses is yet available, emphasizing the importance of surveillance strategies is critical. The current study further showed that only 64.9% HIV-infected and 50.0% of HCV/HIV-coinfected inpatients are followed up with outside care. Multiple factors, including non-compliance of this patient population may contribute to loss of follow up in the current study; on the other hand, a portion of the patients are followed up by their primary care physicians and thus not included in our statistics. Currently, serum alpha-fetoprotein (AFP) is the most widely used biomarker for hepatocellular carcinoma (HCC) surveillance. However, due to the low sensitivity, liver ultrasonography (US) is commonly used in addition to AFP to help detect small hepatic tumours <3 cm. In patients with chronic HCV infection who developed cirrhosis, US combined with AFP measurement every 6 months is the standard method of HCC surveillance. In the past, HCV patients were largely managed by hepatologists because HCV mainly presented with end-stage liver disease, such as ascites, encephalopathy and bleeding varices. Now, as HCV screening has become routine and HCV is a common diagnosis among asymptomatic individuals, infectious disease specialists should take over the management of these patients. On the other hand, given the fact that ART for HIV must be life-long, treatment and follow-up of HCV in HIV-infected patients most likely will be with HIV care providers. In addition, the lessons and experience from HIV care should be very helpful because of the similarity between the two viruses infection including managing the genotype, viral load, drug resistance and combination therapy.
Lifestyle habits such as alcohol abuse 18 and smoking 19 are associated with adverse effects on both HIV and HCV progression. Interventions regarding lifestyle habits should be implemented during the management of HCV/HIV coinfection. It has been reported that, heavy alcohol use has a synergistic effect on HCV-related liver injury in HCV/HIV coinfection, with a higher likelihood of persistent infection, lower sustained response to HCV antiviral therapy and more rapid progression of liver fibrosis and end-stage liver disease.20,21 Our results showed higher percentage of alcoholism in HCV/HIV coinfected patients than in HIV-monoinfected patients. Some reports 19 suggested the synergistic effects between smoking and HCV infection on the risk of HCC. Our data did not show any difference on smoking between HCV/HIV coinfected and HIV-monoinfected patients. However, it is still critical for this patient population to quit smoking to decrease the risk of cardiovascular disease and cancer associated with HCV infection.
This study has several limitations. First, the patient populations in the current study are likely to belong to the lower end of the socio-economic spectrum and, therefore, may not be representative of the general population. Second, though HIV testing is routine, HCV screening test is also recommended by guidelines for HIV-infected patients. Not all of the patients in our study were screened for HCV, which reduced the reliability of comparison. Third, the time of HIV infection is unknown, which may reduce the validity in comparing the synergistic effects of HIV/HCV coinfection to HIV monoinfection on virologic and immunologic responses. As a result, such findings should be incorporated into future prospective cohort studies. Despite the shortcomings described above, the current study highlights a number of new and important findings. To our knowledge, this is the first report comparing HCV/HIV coinfection between outpatients and inpatients. We showed a high seroprevalence of HCV infection in HIV/AIDS inpatients than outpatients. Furthermore, we showed that only half of HCV/HIV-coinfected inpatients were followed up after hospital discharge. Considering the high prevalence and comorbidities of HCV/HIV coinfection, it is highly recommended that evaluation of hepatic damage, especially fibrosis, should be carefully initiated during hospitalization or outpatient care. And also efforts aimed at following up this population cannot be overemphasized. Furthermore, longitudinal study comparing HCV/HIV co-infection among in- vs out-patients about HIV and HCV viral replication, hepatotoxicity and response to treatment over time is desirable in the future.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.