
Abstract
CD4 + lymphocyte counts are routinely ordered during the early phases of antiretroviral therapy and for prophylaxis of opportunistic infections in HIV-positive patients. Flow cytometry is the standard methodology for CD4 counts in Brazilian reference laboratories. However, these laboratories are located in large cities, frequently distant from patients, thus limiting patient access and delaying results. We compared a point-of-care test with flow cytometry determination of CD4+ T lymphocyte counts in HIV patients. We analysed 107 consecutive samples by both methods. Overall, the point-of-care test performed well, with excellent agreement between it and the standard method. Test results were concordant for patients with CD4+ T lymphocyte values above and below 200 cells/mm 3. The performance characteristics obtained were sensitivity 94% (95% CI 89.5–98.5%), specificity 93% (95% CI 88.2–97.8%), positive predictive value 86% (95% CI 79.4–92.6%), and negative predictive value 97% (95% CI 94–100%). The high sensitivity and specificity of the point-of-care test methodology suggest its utility as an alternative method for rapid measurement of CD4+ T lymphocytes in patients with limited access to reference laboratories, enabling prompt therapeutic intervention for patients at risk of progression to AIDS.
Introduction
The CD4+ T lymphocyte (TL) count is the most significant parameter in evaluations of immune function in HIV-positive patients. It guides the start of antiretroviral therapy, dictates the need for prophylaxis against opportunistic infections, and monitors treatment response.1–3 It is crucial to identify patients who are significantly immunocompromised, but in resource-limited settings this detection can be delayed because of limited access to laboratory tests and medical care. 4 Upon diagnosis of HIV infection, it may be several months before a patient is scheduled for their first appointment with a doctor-time that cannot be wasted for severely immunosuppressed individuals. When there are acute symptoms, prompt evaluation of the patient's CD4+ count is necessary to determine the appropriate clinical approach.3,5,6 The Brazilian Public Health System offers laboratory monitoring of CD4+ T cells and viral load to all HIV patients. However, while the blood samples are taken upon diagnosis, results reporting and therapy initiation are delayed because service demand is overwhelmingly high, and the public health laboratories are usually located far from their patients. 7
The Alere Pima™ offers point-of-care testing (POCT) of CD4+ lymphocyte count, providing a possible solution to bridge the gap between the laboratory and the doctor's office.2,8 It is portable and battery-charged, and is thus ideal for areas in Brazil with limited resources. We tested the efficacy of the Pima™ in comparison to a standard CD4+ count by flow cytometry (FACSCalibur, Becton & Dickinson Biosciences, San Jose, CA, USA). With a better understanding of the equipment's qualities and limitations, we aimed to identify settings in which the POCT CD4+ count would be most valuable in Brazil.
Material and methods
This was a prospective study using venous blood samples from HIV patients at specialised ambulatory facilities in an academic tertiary care hospital in Curitiba, Southern Brazil. The study was conducted from November 2012 to May 2013. All participants were adults, and the results were not available to the health staff, which only had access to laboratory-based flow cytometry for the standard CD4+ count. The Institutional Review Board of the Hospital de Clínicas, Universidade Federal do Paraná (HC-UFPR) approved the study (Approval number 02239612.4.0000.0096).
The samples were stored for no more than 2 days in EDTA tubes, and CD4+ lymphocyte count was performed by flow cytometry and the Alere Pima™ POCT simultaneously. The FACSCalibur™ (BD Biosciences) is a multiparametric immunostaining instrument that measures cell size (FSC) and cell complexity (SSC). Flow cytometry of peripheral blood lymphocytes was performed using conventional stain-and-lyse sample preparation techniques. This technique uses BD Trucount™ tubes for absolute counting of leukocytes, using magnetic beads coupled to CD3 (FITC), CD8 (PE), CD45 (PERCP), and CD4 (APC) monoclonal antibodies. After obtaining flow cytometry results, the samples were processed and analysed by Alere Pima™ within 3 hours. Each sample was loaded in a Pima™ Cartridge and immediately placed in the Pima™ Analyzer; after 20 minutes, the results were printed and noted for statistical analyses.
Statistical analysis
Data were compiled using JMP Software Version 5.2.1 and analysed in GraphPad Prism Version 5.03. The Mann-Whitney test was used to assess differences between groups; continuous data are expressed as median ± interquartile range. Results were compared using the Wilcoxon matched-pairs test, and Spearman's rank correlation coefficient was calculated for continuous factors. All p values are two-tailed, and a value of < 0.05 was considered significant.
Operational characteristics and 95% CIs of the Pima™ tests were calculated considering the CD4 + count (FACSCalibur™) cut-off of 350 cells/mm 3. To assess the degree of concordance between tests, Cohen's kappa coefficient was used, for which the results were divided into two groups of < 200 and ≥ 200 cells/mm 3.
Results
CD4+ lymphocyte counts were analysed simultaneously by Pima™ and flow cytometry in 107 consecutive samples. Median values of CD4+ T cells were 468 cells/mm 3 (IQR, 294–656) and 493 cells/mm 3 (IQR, 280–688), respectively. The majority of these patients were on combination antiretroviral therapy (cART), which explains the high median values of CD4 + cells observed. Overall, the Pima™ POC test performed well, with excellent agreement between it and the standard method (kappa = 0.9; IC 95%: 0.773–1.012).
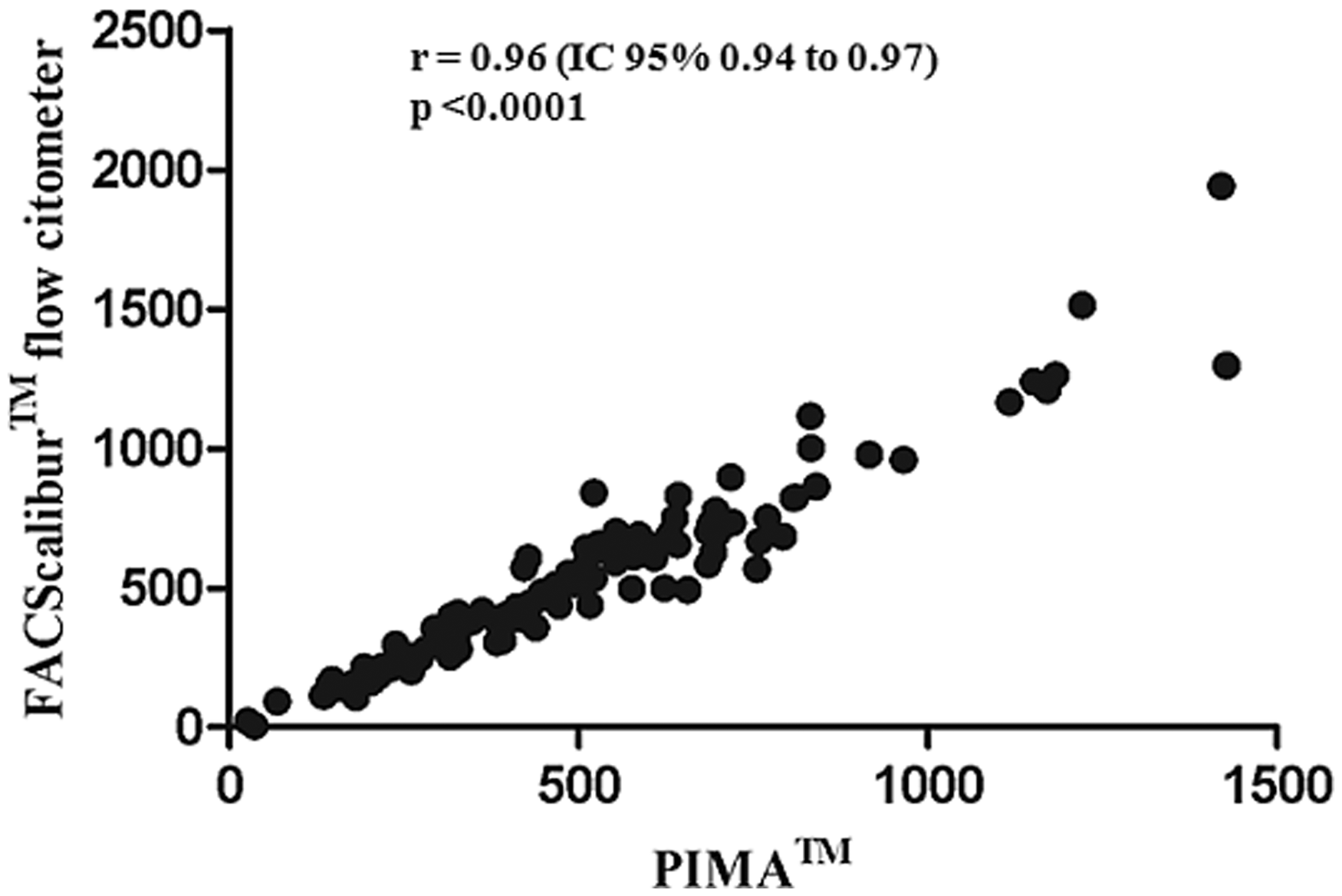
A comparison of absolute CD4+ count values demonstrated a significant difference between the quantities obtained for values below 200 cells/mm 3 or above 500 cells/mm 3. Test results did not differ for values between 200 and 500 cells/mm 3 (Figure 1). The flow cytometry and POCT CD4 values were strongly correlated, with a correlation coefficient value of r = 0.96 (IC 95% 0.94 to 0.97), p < 0.0001 (Figure 2).
CD4+ T lymphocyte counts obtained by PIMA™ and flow cytometry (FACSCalibur). (a) All studied samples. (b) Samples with CD4+ ≥ 200 and ≤ 500 cells/mm 3. Correlation of PIMA™ and FACSCalibur CD4+ T lymphocyte counts.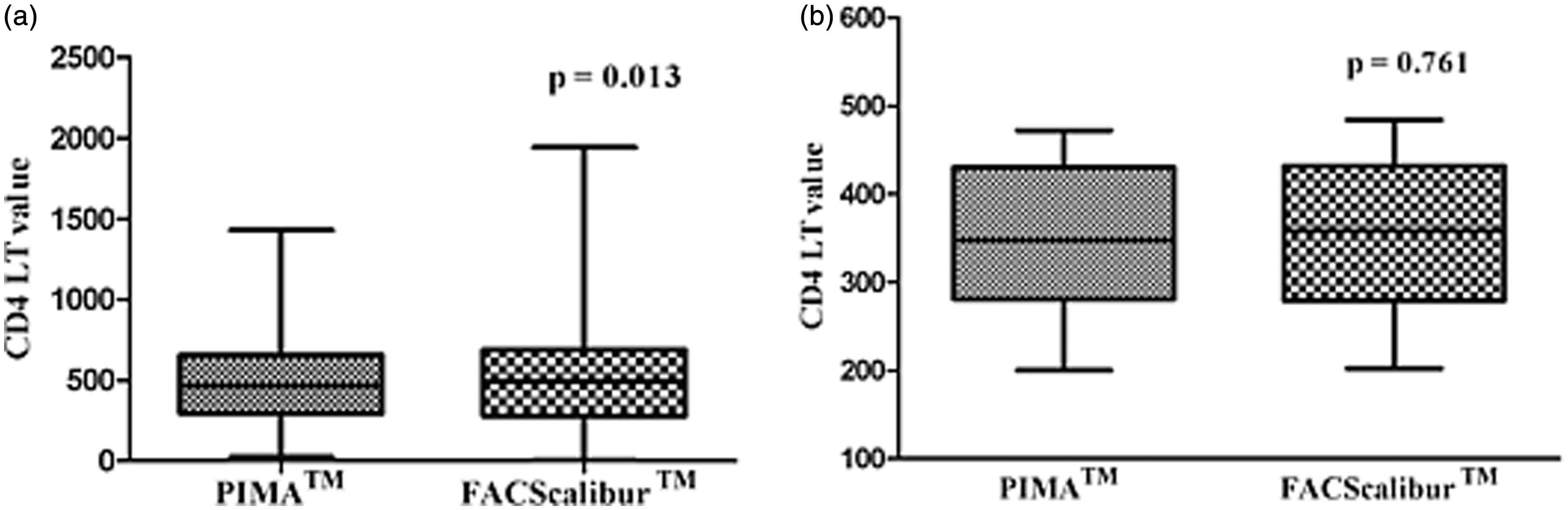
The following performance characteristics were obtained: sensitivity 94% (95% CI 89.5–98.5%), specificity 93% (95% CI 88.2–97.8%), positive predictive value 86% (95% CI 79.4–92.6%), and negative predictive value 97% (95% CI 94–100%).
Discussion
The Pima™ POCT is an efficient method for CD4+ count determination and is appropriate for use at sites with limited resources and access to laboratory services, with the benefits of portability and ease of implementation. While there was a significant difference in absolute lymphocyte values reported by each method, the Pima™ POCT had reliable results for identifying immunocompromised patients when compared to the gold standard laboratory flow cytometer.
Precise monitoring of absolute lymphocyte counts is essential for effective HIV patient management, and the identification of low CD4+ counts is crucial for identifying patients in need of immediate treatment and care. This can be particularly important in newly diagnosed patients, who might otherwise be forced to wait months for their first medical appointment. Unlike the FACScalibur flow cytometer, the PIMA POCT is a cytometer that does the counting of all cells that were simultaneously placed in the cartridge. With this, an overlay of cells could not be eventually counted. Therefore, high counts of lymphocytes in the flow cytometer may be underestimated by the rapid test. Previous studies have shown that the Pima™ analyzer is more accurate at low CD4+ count values and is efficient for classifying patients with lymphocyte values below 200 cells/mm3.9,10
Brazil is deeply socio-economically diverse; some areas have extremely restricted diagnostic laboratories, where samples from HIV patients are collected and sent for analysis at distant reference centres. In 2011, 38,776 patients were diagnosed with HIV in Brazil; 11 a sizable portion of these patients must wait several months before their first post-diagnosis clinical appointment. While these faults need to be addressed properly with various improvements on the Public Health System, such changes require a long and active process. Implementation of the Alere Pima™ within public facilities in resource-limited regions and urban diagnostic centres could quickly help resolve this issue by pinpointing those who need immediate, preferential care. This could incur additional costs, but prioritising care for significantly immunocompromised individuals could prevent subsequent treatments for opportunistic infections and complications.
The POCT for CD4+ T cells would be a great addition to public facilities, but due to its limitations should not be used as the sole test for cell counts. It does not provide an absolute T lymphocyte count as precise as the gold standard flow cytometer. Also, while the cartridges are designed for use with capillary blood samples, venous blood samples have shown to be more accurate and should be chosen when possible.3,4 The focus for implementation of the Alere Pima™ should be on early detection of immunocompromised patients, improving the management of the overwhelming number of HIV cases in Brazil and other developing countries.
Footnotes
Conflict of interest
The equipment to perform the point-of-care CD4+ T lymphocyte counts were provided by the company Alere™. The funders had no role in study design, data collection and analysis, decision, or preparation of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.