
Abstract
In the UK, despite its low sensitivity, wet mount microscopy is often the only method of detecting Trichomonas vaginalis infection. A study was conducted in symptomatic women to compare the performance of five methods for detecting T. vaginalis: an in-house polymerase chain reaction (PCR); Aptima T. vaginalis kit; OSOM ®Trichomonas Rapid Test; culture and microscopy. Symptomatic women underwent routine testing; microscopy and further swabs were taken for molecular testing, OSOM and culture. A true positive was defined as a sample that was positive for T. vaginalis by two or more different methods. Two hundred and forty-six women were recruited: 24 patients were positive for T. vaginalis by two or more different methods. Of these 24 patients, 21 patients were detected by real-time PCR (sensitivity 88%); 22 patients were detected by the Aptima T. vaginalis kit (sensitivity 92%); 22 patients were detected by OSOM (sensitivity 92%); nine were detected by wet mount microscopy (sensitivity 38%); and 21 were detected by culture (sensitivity 88%). Two patients were positive by just one method and were not considered true positives. All the other detection methods had a sensitivity to detect T. vaginalis that was significantly greater than wet mount microscopy, highlighting the number of cases that are routinely missed even in symptomatic women if microscopy is the only diagnostic method available.
Keywords
Introduction
Trichomonas vaginalis (TV) is the most common non-viral sexually transmitted infection (STI) in the world 1 but relatively uncommon in the UK. TV infection in UK Genitourinary clinics is mainly (and often exclusively) diagnosed by wet mount microscopy 2 alone. Microscopy is known to have a low and variable sensitivity and therefore greatly underestimates the true prevalence of TV infection. Culture of TV is still regarded as the gold standard diagnostic method but it is not routinely performed in clinics mainly due to time, cost and requirement for an incubator. Nucleic Acid Amplification tests (NAATs) for detecting TV infection have been shown to be highly sensitive and specific in studies. 3 However, the lack of a commercially available test until recently has meant that using this approach has not been possible for many laboratories. 4 Several Point-of-Care Tests (POCT) for TV are also now widely available but have not been well utilised in UK clinics despite higher rates of sensitivity than wet mount microscopy being reported. 5 The OSOM Trichomonas Rapid Test is a POCT for professional use (Sekisui Diagnostics Lexington, MA, USA) and is able to provide results in 10 min. This is therefore a very feasible test to perform in a clinic setting, providing immediate results for the patient and expediting the care pathway.
Symptomatic TV infection in women can cause vulval irritation, dysuria and a malodorous discharge. It has been long associated with complications in women and pregnancy complications. 6 There is now an increasing amount of evidence showing an epidemiological and biological relationship between TV and human immunodeficiency virus (HIV) infection. Data from cohort studies have shown the presence of TV infection to increase the risk of HIV acquisition.7,8 This information is particularly relevant to the local area where the rates of HIV in the community are the highest in the UK: locally 12.2 per 1000 15–59 year olds are known to be HIV positive. 9
TV is known to be more prevalent in Black African and Caribbean populations.10,11 The clinic is based in a multi-ethnic area of London; in 2012, 50% of the patients who were seen self-reported as Black background – of which 19% were Black African, 16% were Black Caribbean and 10% Black British. In 2012, the clinic reported 200 cases of TV where 6638 cases were reported to Public Health England in the same time period. 12 Local data have shown higher rates of TV compared to the rest of the UK with higher prevalence detected on transcription-mediated amplification (TMA) testing compared to microscopy. 13 However, very few studies have evaluated molecular methods and POCT together and compared them to culture and microscopy. The aim of this study was to evaluate a real-time in-house PCR targeting a TV-specific repeat,14,15 the Aptima TV molecular test, OSOM Trichomonas Rapid Test and culture to diagnose TV infection in symptomatic women and compare this to the current main method of diagnosis: wet mount microscopy.
Method
A prospective study was conducted to evaluate five different tests to diagnose TV infection in women attending a Sexual Reproductive Health Clinic in London. This is a walk-in, fully integrated sexual health service providing STI diagnosis, management and contraceptive care. A power calculation was conducted which assumed the sensitivity of 70% for microscopy and sensitivity of 90% for POCT. This showed that to achieve a power of 75% (with the level of significance of 0.05%), the study required 50 observations.
Sample collection
All symptomatic women aged over 18 years who presented to the clinic on Monday and Tuesday from September 2011 to January 2012 were invited to enrol. Recruitment was limited to these days as the cultures were read at 72 h and staff capacity was not available to read the cultures at the weekend. Women who would normally have undergone a full pelvic examination based on their presentation were invited to participate in the study. This included all but was not limited to those patients with symptoms of pelvic pain, dysuria, vaginal discharge and vulval itch. All women regardless of symptoms, who presented to the clinic during the recruitment period, were provided with an information sheet about the study. After the initial clinical consultation, if the clinician decided that they met the inclusion criteria they were invited to participate in the study.
Women with a recently diagnosed TV infection (six weeks), those who had recent metronidazole (two weeks), those under the age of 18 years and women who were unable to give consent due to lack of mental capacity or language reasons were excluded from the study. All doctors and nurses working in the clinic were involved in recruitment and sample collection. All health care providers were trained on how to take the study swabs, label and process samples in order to maintain consistency throughout the study. The order of the extra swabs was randomised but each swab was taken from the same part of the vaginal wall. However, since the viable organism load required for the molecular tests is much less than that required for culture and microscopy, the authors were aware that the latter two tests may underperform as a result. Study posters with flow charts and photos detailing sample collection were displayed in clinical areas for clinicians to refer to.
Written and verbal consent was obtained from all women who entered into the study, who then underwent routine clinical evaluation including wet mount microscopy.
Laboratory testing
A further three extra vaginal swabs were taken for study purposes.
A dry swab was taken from the lateral vaginal wall, placed into an Aptima transport container and sent to the Sexually Transmitted Bacteria Reference Unit (STBRU). Upon receipt, the buffer was then split into two aliquots. A DNA extraction was (Nucleic acid isolation kit, Version 10; Roche Diagnostics Ltd, Germany) performed on the first aliquot, followed by a TV-specific real-time PCR (targeting the DNA repeat region).3,15 In the event that the specimen was positive, the result was confirmed using a second real-time PCR targeting the β-tubulin gene. 15
The second aliquot of transport buffer and swab was then stored at −20°C until the end of the study when it was tested using the Aptima TV kit on the Panther robot according to manufacturer’s instructions (Gen-Probe Inc., San Diego, CA, USA).
A further dry swab was taken for the OSOM Trichomonas Rapid Test from the vaginal wall. This was performed on a daily basis by a trained technician in a separate clinical area to the main laboratory in line with the manufacturers’ guidelines.
A swab for culture was taken from the vaginal wall for 30 s and then immediately inoculated into the culture pouch of the TV Inpouch Culture System (Biomed, Diagnostics, Santa Clara, California, USA). This system allows direct inoculation and visualisation of the culture medium. The individual culture pouches were incubated at 37°C and then read at 72 h for the presence of motile trichomonads using microscopy.
The wet film sample was taken as per usual clinic protocol. Staff reading the slides would vary due to the large nature of the clinic. All staff performing microscopy undergo competency-based training and assessment in concordance with local guidelines.
All testing were performed by trained personnel who were blinded to the results of the other testing methods.
Follow-up
All the results from the study were collated on a weekly basis and women were contacted for treatment in the cases where the wet mount microscopy was negative and either one or more of the tests from the study were found to be positive. Women who were treated with metronidazole for bacterial vaginosis on the day and were later found to have TV infection were still contacted and counselled and offered contact tracing.
Planned analysis
Demographic data were extracted from the local database and entered into STATA (Stata Corp.) using the CSI command to calculate proportional differences. Sensitivity, specificity, negative predictive value (NPV) and positive predictive value (PPV) were calculated. Confidence intervals (95%) were calculated for the individual test modalities using a positive result by two different tests as the reference standard.
Ethical approval for the study was obtained from Dulwich Research and Ethics Committee London (reference 11/LO/1058).
Results
Test performance and TV prevalence
The concordance between five different methods used for detecting Trichomonas infection in symptomatic women.
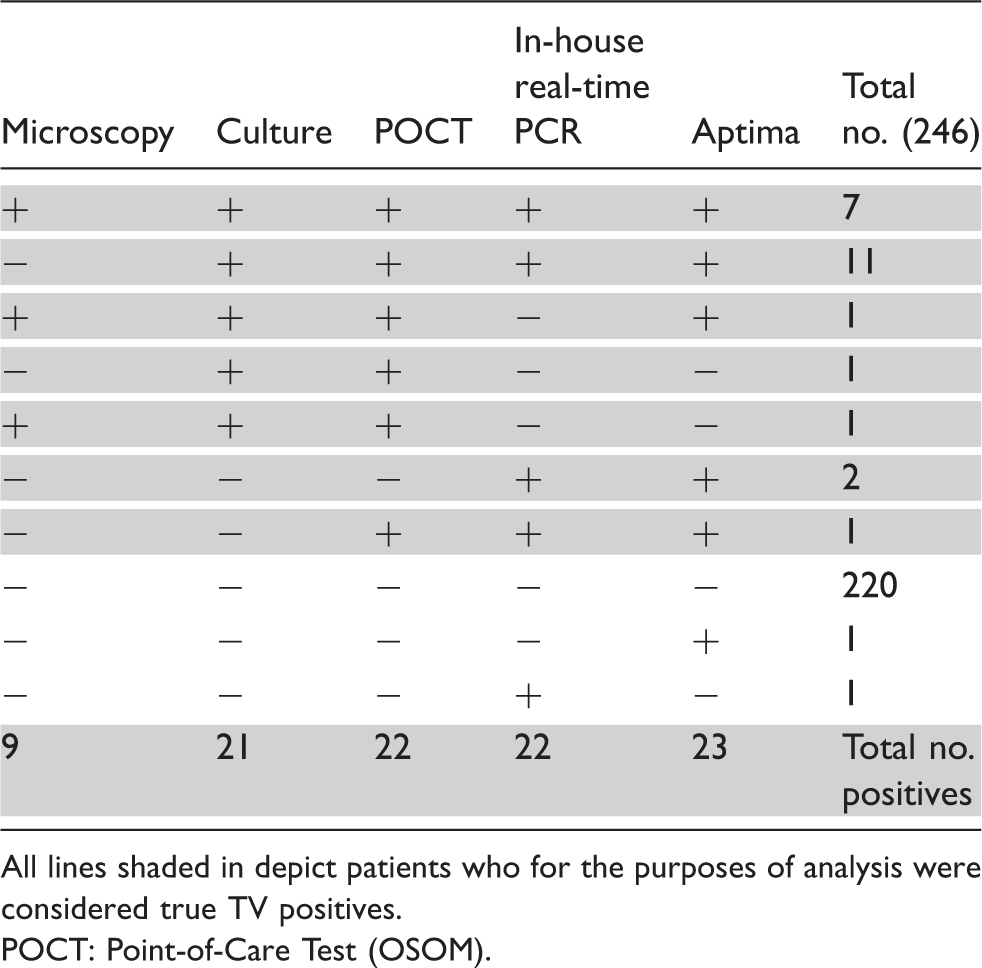
All lines shaded in depict patients who for the purposes of analysis were considered true TV positives.
POCT: Point-of-Care Test (OSOM).
Sensitivity, specificity, NPV and PPV (using two positive tests as reference standard).
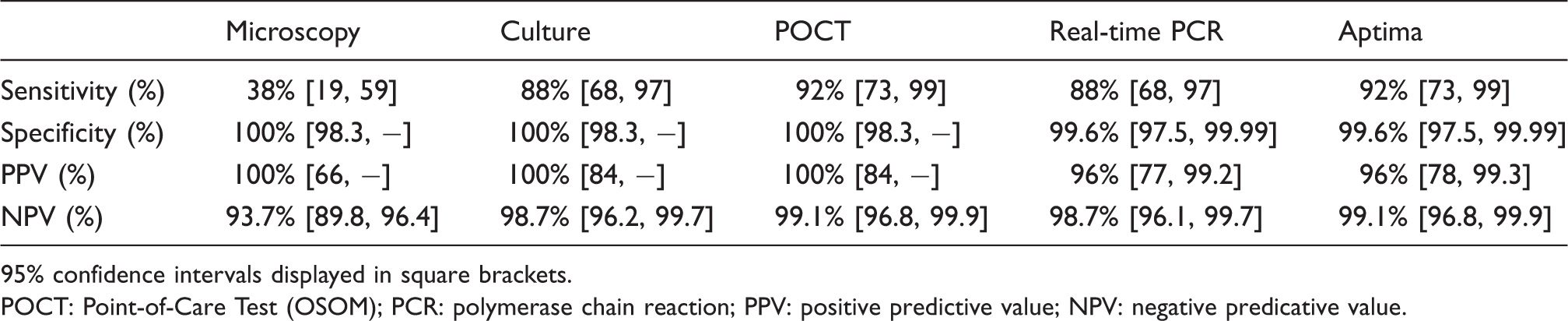
95% confidence intervals displayed in square brackets.
POCT: Point-of-Care Test (OSOM); PCR: polymerase chain reaction; PPV: positive predictive value; NPV: negative predicative value.
The prevalence of TV infection in symptomatic women diagnosed with microscopy alone in the clinic was 3.66%. The prevalence of TV using two positive results as a reference standard was 9.75%.
Demographics
Demographic characteristics of women testing positive and negative for TV with details of ethnicity and concurrent STI at that visit.
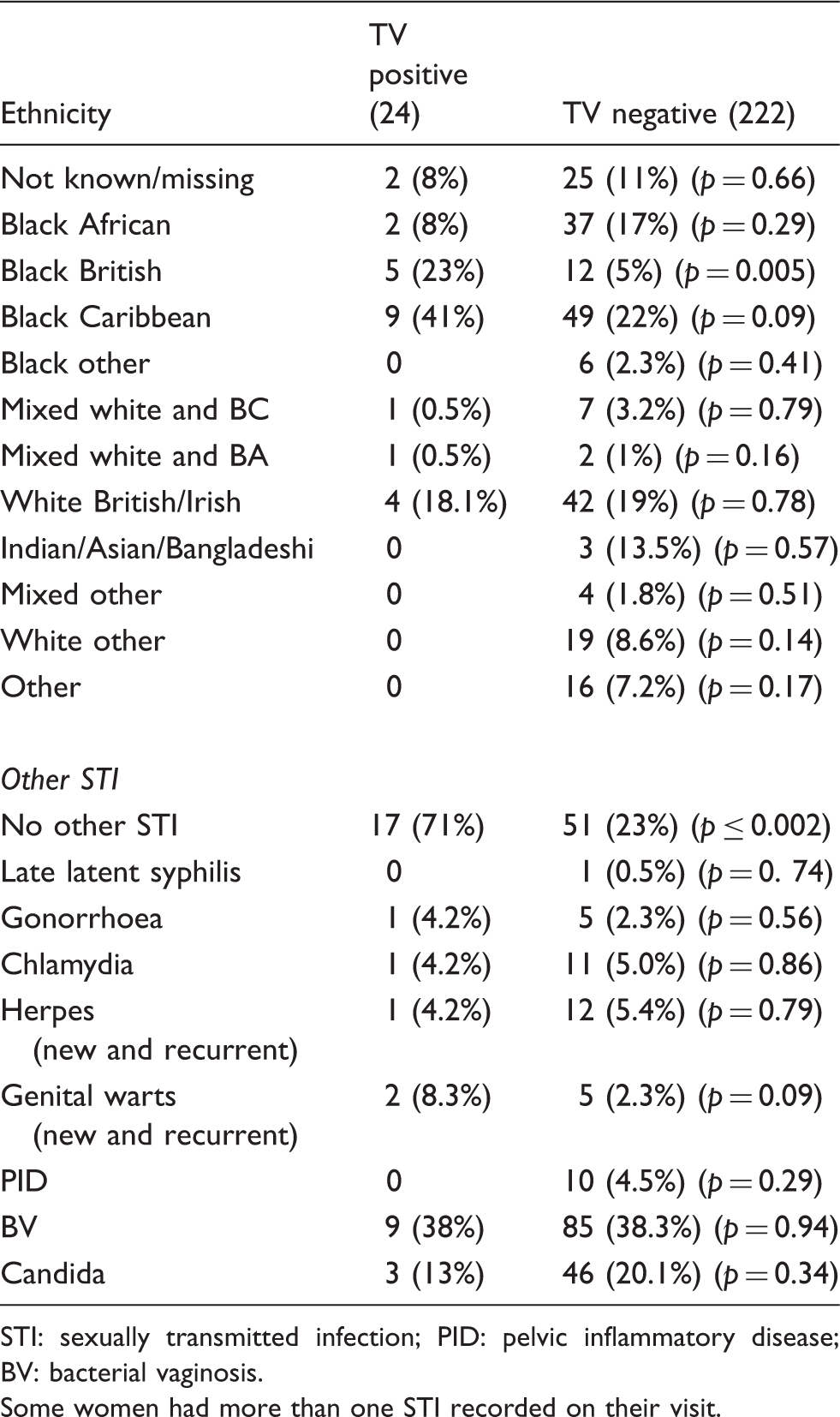
STI: sexually transmitted infection; PID: pelvic inflammatory disease; BV: bacterial vaginosis.
Some women had more than one STI recorded on their visit.
Discussion
This study has shown that in-house real-time PCR, the Aptima TV kit and the OSOM Trichomonas Rapid Test have a higher sensitivity compared to wet mount microscopy to detect TV infection in symptomatic women. These results also suggest that the OSOM Trichomonas Rapid Test had equivalent sensitivity and specificity to in-house real-time PCR and the Aptima TV.
In this study, wet mount microscopy was found to perform very poorly. Due to the busy nature of the clinic, there were different operators evaluating the slides and this may have contributed to the lower sensitivity of this technique. This study was also limited by a small and select group of women with a high prevalence of TV and selection bias may have affected recruitment into the study. There were no data collected on those who declined to participate in the study. Although anecdotally, we are aware that women preferred to avoid extra time in the clinic and were concerned about further invasive tests. This study does not include asymptomatic women but there are data supporting the use of PCR in this group and for self-screening. 16 The OSOM has been evaluated in self-testing 17 but is not yet licensed in asymptomatics.
For purposes of the study, the OSOM was only tested in batches; however, the major benefit of the OSOM is rapid results which negates the need to return for results and treatment, which has been shown to be cost effective. 5 Following the study findings, costing data were used to project implementation in the clinic and this was shown to be significantly cost effective. 18 The OSOM was also easy to set up and unlike microscopy requires minimal training to operate.
The prevalence of TV infection in symptomatic women using two positive test results as the gold standard was found to be 9.75%, greater than double the diagnoses made by wet mount microscopy alone (3.7%). The UK British Association for Sexual Health and HIV (BASHH) Guidelines 19 have recently been updated and refer to the use of molecular tests. In the light of our study findings where wet mount microscopy was shown to have poor sensitivity even in symptomatic women, we would recommend the use of either PCR/Aptima or OSOM over microscopy in high-risk patients.
Clinicians such as general practitioners and community clinics without access to microscopy or laboratory services should consider OSOM to diagnose TV infection. In view of the relationship between HIV and TV infection, women with HIV should be referred for annual routine screening with either PCR/Aptima or OSOM in line with the CDC guidelines. 20 Molecular testing for TV should be routinely considered in symptomatic women who have had negative microscopy, especially in a high prevalence area.
Footnotes
Acknowledgements
The authors would like to acknowledge the staff of The Sexually Transmitted Bacteria Reference Unit at Public Health England and Camberwell Sexual Reproductive Clinic.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was undertaken as a BASHH/PHE Fellowship.