
Abstract
Trichomoniasis caused by the protozoan parasite Trichomonas vaginalis (TV) is one of the most commonly occurring sexually transmitted infections of non-viral origin. This study examines the prevalence of TV infection amongst consenting symptomatic women attending three of the largest sexual health clinics in Scotland, United Kingdom. In addition, an evaluation of three testing methods to identify TV from vaginal fluid was performed involving the commercial Hologic APTIMA TV transcription-mediated amplification assay, a real-time PCR assay and microscopy. A total of 398 patients consented to participation and all were tested by the three methods. The prevalence of TV was 2.8% (n = 11), with both molecular assays correctly detecting an additional two cases of TV compared to microscopy. The prevalence of three other sexually transmitted pathogens, namely Chlamydia trachomatis, Neisseria gonorrhoeae and herpes simplex virus were 7.3% (n = 31), 0.3% (n = 1) and 1.5% (n = 6), respectively. The majority of TV cases (78%; n = 8) occurred in women greater than 29 years of age compared to most Chlamydia trachomatis cases, who were aged 30 or less (97%; n = 30).
Introduction
Trichomonas vaginalis (TV), a motile protozoan parasite and causative agent of trichomoniasis, is the most prevalent, non-viral, sexually transmitted infection (STI) with an estimated 248 million new cases each year worldwide (WHO). 1
Signs and symptoms of trichomoniasis include vaginal discharge which may have a foul odour, urethritis and cervical bleeding, although an estimated 25% of patients diagnosed within sexual health clinics may be asymptomatic. 2 In addition, TV has been associated with complications in pregnancy and the transmission of HIV. It may also predispose infected women to pelvic inflammatory disease, and may be associated with cervical cancer and post-hysterectomy infection. 3
Given the non-specific clinical signs and symptoms of TV infection combined with the high rate of asymptomatic cases and the potentially serious sequelae, it is essential to have sensitive and specific diagnostic methods to enable better patient management and to prevent spread of infection, leading to a greater understanding of this under-diagnosed condition.
Recent British Association for Sexual Health and HIV (BASHH) guidelines recommend selective testing for TV in female patients presenting with, or identified on examination as having vaginal discharge, vulvitis, and/or vaginitis. Testing of men is recommended for contacts of known TV cases, and should also be considered in those with persistent urethritis. 4 In Scotland, wet mount microscopy (+/− culture) is the main method used routinely to identify TV, yet both techniques have lower sensitivity. Microscopy is considered highly specific however, though its sensitivity can be variable, ranging from 30% to 60% depending on the comparator method employed and the expertise of the microscopist.5,6 Extended periods of culture are required to ensure optimal sensitivity, leading to delays in the reporting of results. In addition, prompt processing of samples is required to prevent pathogen degradation.
Molecular assays, both in-house and commercial, have led to improved TV diagnostic sensitivity.7–11 Such assays do not rely on the specimen being viable and permit testing out-with local clinics whilst requiring minimal laboratory manipulation and data interpretation.
In this study, the prevalence and detection of TV infection in female patients attending three large sexual health clinics in Scotland were investigated using three methods: the FDA-approved Hologic transcription-mediated amplification TV APTIMA assay (TVA), an in-house real-time PCR assay and microscopy.
Methods
Study design and procedures
Ethical approval was sought (REC reference 13/WS/0205) to include female participants aged over 16 presenting with a complaint of vaginal discharge attending either the Chalmers Sexual Health Centre, Edinburgh, the Sandyford Central Sexual Health Centre, Glasgow or the Sexual and Reproductive Health Clinic, Ninewells Hospital, Dundee. In addition to the routine swab taken for microbiological testing, two additional swabs were collected: one for the commercial APTIMA TV (ATV) molecular assay and the other for an in-house real-time PCR assay. Molecular testing was performed by the Scottish Parasite Diagnostic and Reference Laboratory (SPDRL), Glasgow. For the in-house assay, DNA was extracted using the QIAamp DNA kit (Qiagen Ltd) and subjected to amplification using primers and probes as described previously on the LightCycler® 480 System (Roche Diagnostics Ltd, UK). 9
Due to the lack of sensitivity using conventional microscopy, the study definition of true positivity was based on comparison with the other tests and assigned when two of the three investigated methods were positive.
Results
Comparison of microscopy, ATV and Q-PCR assay detection of Trichomonas vaginalis (TV).
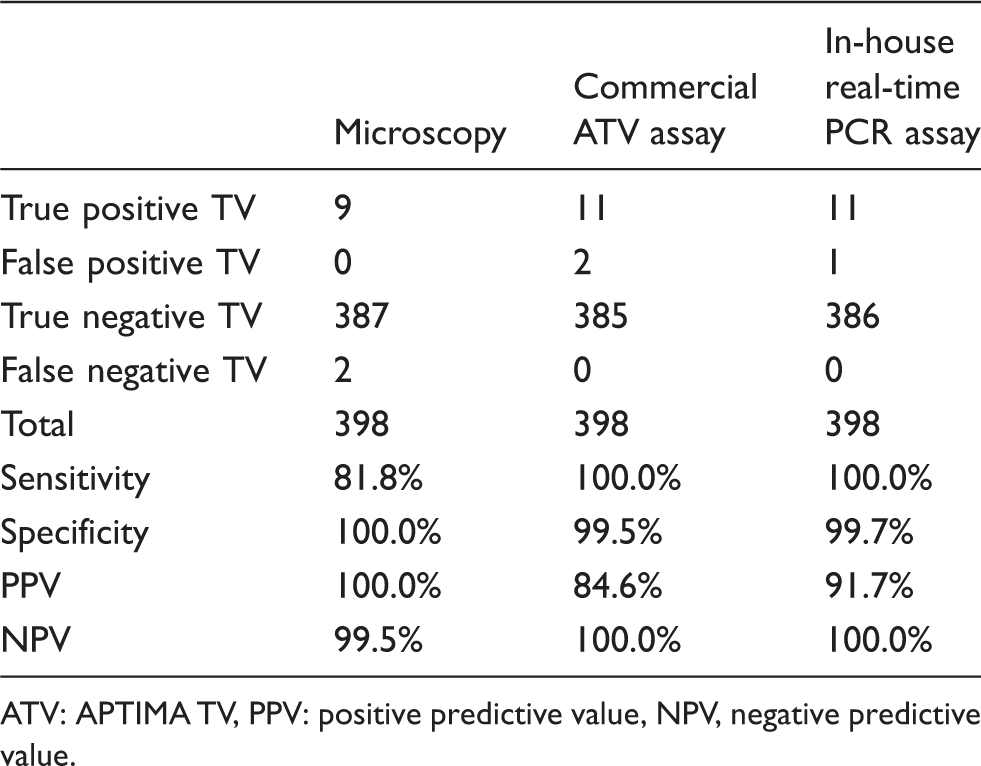
ATV: APTIMA TV, PPV: positive predictive value, NPV, negative predictive value.
Screening results for other pathogens were available for 395 patients where the prevalences of Neisseria gonorrhoeae (NG), Chlamydia trachomatis (CT) and herpes simplex virus (HSV) were 0.3% (n = 1), 7.3% (n = 31) and 1.5% (n = 6), respectively.
Of those screened for TV, co-infections were noted in two patients; one had both TV and HSV whilst another patient was infected with TV and CT. In one patient where TV was absent, both NG and CT were detected. No other STIs were noted in the study group. Bacterial vaginosis and vaginal candidiasis were documented in 3.8% (n = 15) and 2.8% (n = 11) of patients, respectively, none of which were concurrent with TV infection. The comparative prevalence data for TV, CT and NG, characterised according to age, are outlined in Figure 1.
Comparative data for Trichomonas vaginalis (TV), Chlamydia trachomatis (CT) and Neisseria gonorrhoeae (NG).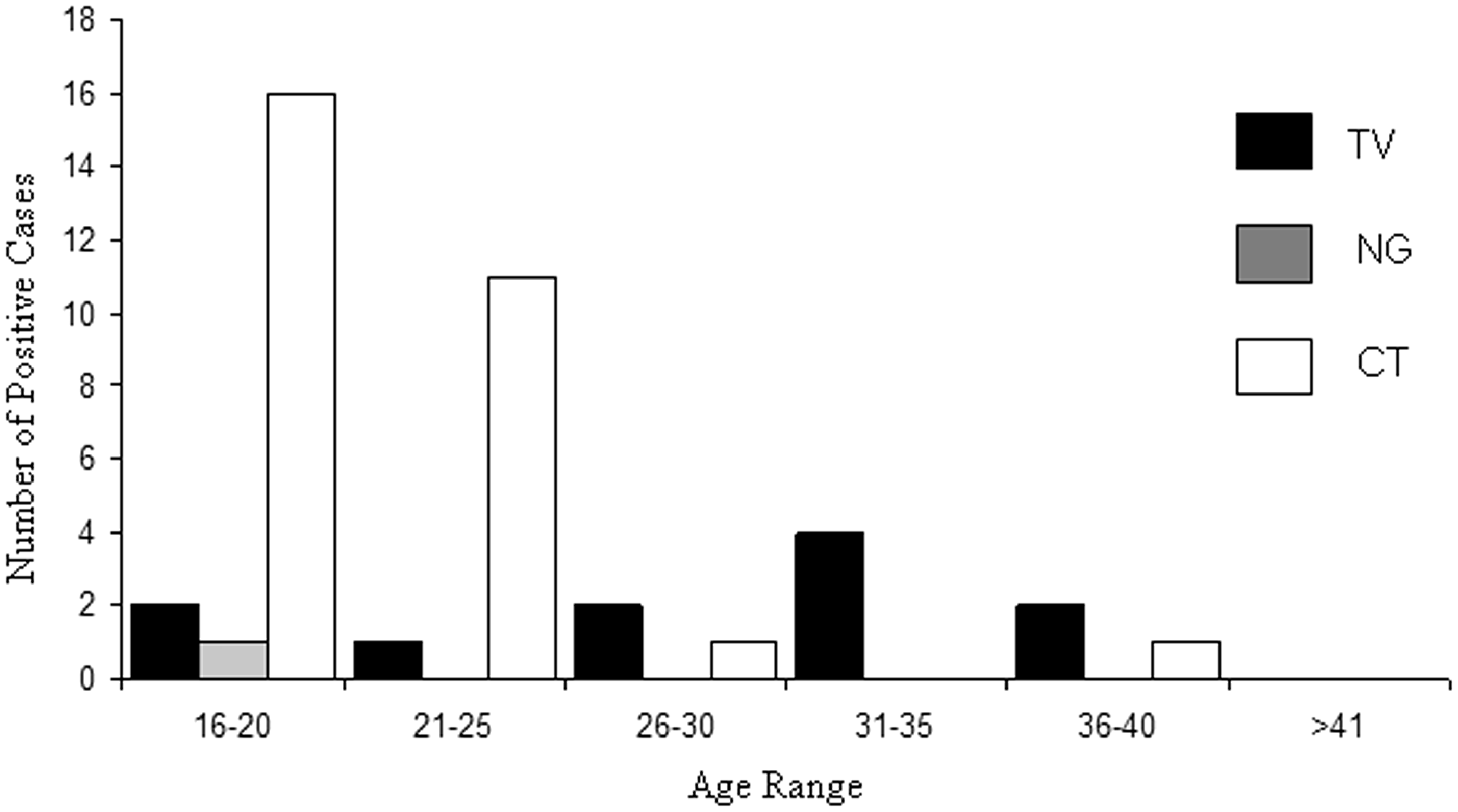
Although the most common age group to be tested for TV was within the 21–25 age range (137 / 398; 34%) (Figure 2), of the 11 cases of TV confirmed by more than one method 73% (n = 8) were seen in patients aged over 29 (Figure 1).
Age distribution of symptomatic women tested for Trichomonas vaginalis (TV).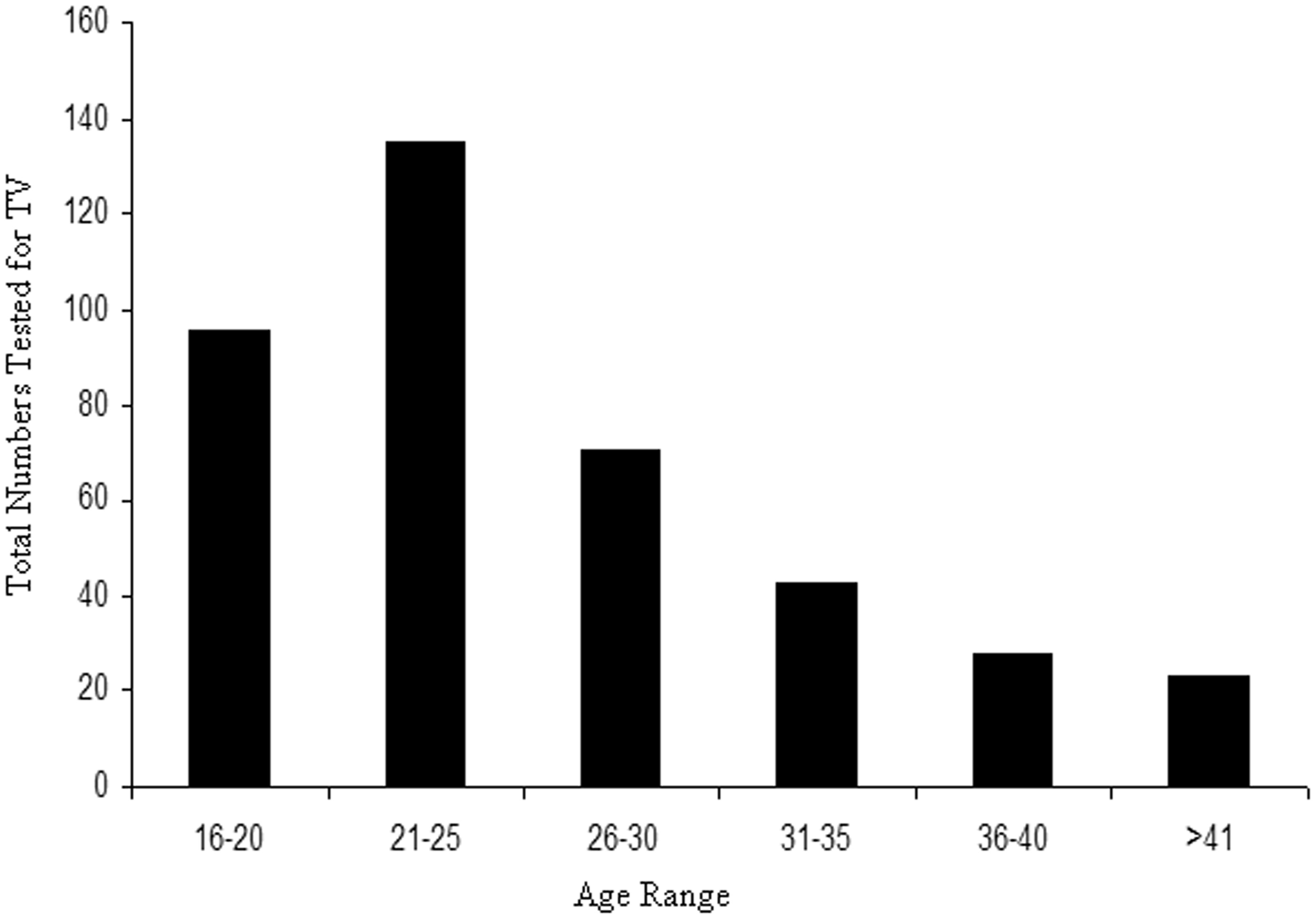
In contrast, 97% (n = 30) of CT cases were diagnosed in those aged 30 or less (Figure 1). The sole patient diagnosed with NG infection was aged 18.
Ethnicity data were available for 375 patients. Three hundred and fifty-five patients were of white ethnicity (British, Scottish, Irish or other), six were of mixed race, eight were of Asian ethnicity and six identified as being of African ethnicity. Ten cases of confirmed TV infection were identified from patients of white ethnicity, with one further case being found in a patient of Asian ethnicity. Of the 31 cases of CT, the majority (n = 30) were identified in patients of white ethnicity. The remaining CT-positive patient was of undocumented race, and the single case of CT and NG co-infection was detected in a patient of white ethnicity.
Discussion
This is the first multi-centre study in Scotland to provide an estimate of the prevalence of TV and compare it with that of other sexually transmitted pathogens. In addition, the study provides evidence to assist with developing future testing algorithms for the most cost-effective, sensitive and rapid method for diagnosing TV within the clinic setting. The prevalence of TV was nine-fold higher than the prevalence of NG, yet almost three-fold lower than that of CT. Comparing data with the rest of the UK, there is variation in the prevalence of TV where, in England, a range of positivity rates have been described (0–10%).12,13 A number of factors may account for such variations, including the patient selection criteria and also patient demographics such as age and ethnicity. In our study, TV prevalence was highest in women aged between 30 and 64 years of age. Conversely, CT infection rates were highest in patients less than 30 years of age. This distribution of TV is supportive of data described by Huppert et al., where almost half of their TV-positive patient were aged 30 or over. 14 The observation that TV prevalence may be higher in those outside the expected age range for STI screening provides evidence for a targeted approach for TV testing.
UK data have highlighted non-White ethnicity and increasing age as being associated with TV infection. 12 In our population, 10 of the 11 positive TV cases were found in Caucasian patients, with the remaining one positive case being identified in a patient of Asian origin. Multivariate analysis of the data presented in this study (data not shown) did not highlight statistically significant risk factors associated with TV infection. The study limitations included the low sample size, the small number of positive TV cases and the lack of non-Caucasians being tested (only 5% of the total) which are likely to impact on the lack of risk factors associated with TV.
We provide supporting evidence that both the commercial and the in-house molecular assays exhibited increased sensitivity when compared to microscopy. Even though microscopy was performed within each clinic by expert microscopists thus ensuring optimal assay sensitivity, it was found to be less sensitive. This sensitivity described for microscopy in this report was higher than many other groups, when compared to a singular molecular test; however, not all previous studies have included a comparator molecular test for result verification. Both molecular tests correctly identified all microscopy-positive samples; in addition to two further true TV-positive cases.
In addition to the two molecular assays described in this report, other strategies for TV testing include the use of multiplex molecular assays which include in-house and commercial assays such as the Roche Aurora FLOW and the BD MAX™ System (BD diagnostics), which detect CT, TV and NG in a single sample.15,16 Rapid and commercial point of care tests such as the OSOM Trichomonas Rapid Test (Genzyme Diagnostics, USA) are being employed as alternatives to molecular testing. These tests have been reported to have high sensitivity and specificity, comparable with that of molecular assays and much better than microscopy.17,18 They may be useful, particularly in settings where specialised molecular equipment is not available.
The implementation of molecular techniques may aid patient management and improve our understanding of the epidemiology of TV disease by capturing accurate data. However, an important factor to consider is the cost implication of introducing such techniques which are considerably more expensive than conventional methodologies. Therefore, it is likely that a tailored approach being more cost-effective in high risk groups would be preferable. In the USA and the UK, testing is recommended for all symptomatic women presenting with vaginal discharge.19,20 In the USA, TV screening is currently recommended annually for all HIV-infected women, and screening also considered for asymptomatic women at ‘high risk’. In a study of 6335 patients, Muzny et al. state that molecular testing detects over 30% more infections than microscopy alone and suggests that screening of TV should be performed routinely particularly in people over aged 40. 21 However, in the UK there are no current recommendations for TV screening. Our study provides Scottish-wide data on the prevalence of TV in symptomatic women to support the development of an evidence-based algorithm for the most suitable testing method for a rapid diagnosis of this pathogen. By considering the options for implementing an accurate diagnosis of TV, this will allow prompt treatment of affected individuals and will initiate partner notification, thus minimising the spread of infection of this under-diagnosed pathogen.
Footnotes
Acknowledgements
We would like to thank Hologic UK for providing the equipment and reagents for the ATV assay and to staff within the sexual health centres for assisting with the consent / sampling procedures.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.