
Abstract
The association between bacterial vaginosis (BV) and incident sexually transmitted infections (STIs) in a cohort of high-risk women from Durban, South Africa was investigated in this study. We undertook a secondary analysis of the Methods for Improving Reproductive Health in Africa trial that assessed effectiveness of the latex diaphragm and lubricant gel on HIV prevention among women. During study visits, urine specimens were collected for testing for Neisseria gonorrhoeae, Chlamydia trachomatis and Trichomonas vaginalis. The presence of BV was based on vaginal pH and wet mount test assessments. The association between BV and the risk for incident STIs was determined using the Cox proportional hazards model. Prevalence of BV was 31% in a cohort of 435 women tested at baseline. Among these women, BV was significantly associated with incident Trichomonas vaginalis (14.6 per 100 PY, p = 0.03) and Chlamydia trachomatis infections (15.8 per 100 PY, p = 0.04). BV remained a significant predictor for Trichomonas vaginalis infections even after adjusting for potential confounders such as age and marital status (HR: 1.60, 95% CI: 1.00, 2.57, p = 0.04). Our study showed an association between baseline BV infections and incident Trichomonas vaginalis and Chlamydia trachomatis infections. Women with BV infections should be counselled on the use of condoms and the risk of new STIs.
Introduction
The presence of Lactobacillus species in the vagina has been shown to maintain a healthy vaginal environment through the production of organic acids such as lactic acid, hydrogen peroxide or lactocins. 1 Bacterial vaginosis (BV), which is associated with an overabundance of anaerobic and facultative bacteria (Gardnerella vaginalis, Bacteroides sp., Mobiluncus sp. and genital mycoplasmas), results in an elevated vaginal pH2,3 and an increase in malodorous vaginal discharge. 3
BV represents the main cause of abnormal vaginal discharge in women of reproductive age, 4 and has been linked to considerable gynaecologic and obstetric morbidity such as preterm delivery, pelvic inflammatory disease (PID) and upper genital tract infections. 5 A systematic review and meta-analysis which investigated the association between sexual risk factors and BV have suggested that BV may be sexually transmitted since many studies have shown that BV-positive individuals have been associated with having a high number of lifetime or recent sexual partners, having an early age of sexual debut and lack of condom use during sex acts. 6
Several studies have reported a strong association between BV and sexually transmitted infections (STIs) such as Neisseria gonorrhoeae, Chlamydia trachomatis and Trichomonas vaginalis.7–9 Alterations in the microbiological environment of the vagina such as those that occur in BV are considered risk factors for the acquisition of STIs. 10
In this study, we investigated the factors associated with baseline BV infections and the association between BV and the acquisition of N. gonorrhoeae, C. trachomatis and T. vaginalis infections in a cohort of high-risk, human immunodeficiency virus (HIV)-negative, non-pregnant women from Durban, South Africa.
Methods
Study sites
This is a secondary analysis of the Methods for Improving Reproductive Health in Africa (MIRA) study. MIRA was a phase III trial that assessed the effectiveness of the latex diaphragm with a lubricant gel in preventing heterosexual acquisition of HIV among women in southern Africa. However, the provision of diaphragms and lubricant gels in addition to male condoms provided no beneficial effect. 11 The trial was conducted between 2003 and 2005 in South Africa and Zimbabwe. This analysis is based only on participants recruited and enrolled at the Durban sites. In Durban, the study was conducted at two trial sites, rural Umkomaas (a peri-urban region located 60 km south of Durban) and Bothas Hill (a rural area located 40 km west of Durban).
Study participants
Women were recruited from family planning, well-baby and general health clinics for participation in this study. The main eligibility criteria for the study included: women aged 18 to 49 years old, sexually active (coital frequency at least four times per month on average), HIV-negative based on testing within 14 days prior to enrollment, C. trachomatis- and N. gonorrhoeae-negative based on testing within 30 days prior to enrollment or, if positive, completed treatment before enrollment, have a healthy cervix as assessed by naked-eye speculum exam at enrollment, planning to live in the study area for the duration of the study, and willing and able to give informed consent. Participants provided written informed consent prior to study procedures being conducted. Participants were followed quarterly with a mean follow-up of 18 woman-months per participant. Participants had completed physical examinations at all study visits to identify any abnormalities of the cervix and to detect any cervicovaginal infections. Testing for HIV and STIs were also done at all study visits. BV was assessed at enrollment and when clinically indicated. Our rationale for using baseline BV data was to primarily assess the association between prevalent BV infections and the risk for incident STIs.
The study protocol and informed consents were approved by the Biomedical Research Ethics Committee at the University of KwaZulu-Natal as well as the study-specific Institutional Review Boards. This study was registered with ClinicalTrials.gov, number NCT00121459.
Clinical data collection
At screening (baseline visit), verbal consent to assess initial eligibility, followed by written informed consent for all study procedures was obtained. Data on demographics, sexual behavior and clinical history were obtained. Clinical history included data on treatment of STIs or reproductive tract infections (RTIs). STIs and RTIs were treated according to the United States Centres for Disease Control and Prevention guidelines. 12
Laboratory procedures
Urine specimens were collected for polymerase chain reaction (PCR) testing for N. gonorrhoeae, C. trachomatis and T. vaginalis (Roche Pharmaceuticals, USA). The presence of BV was assessed by Amsel’s criteria (i.e. the presence of three or more of the following: vaginal pH > 4.5, clue cells on microscopy, positive whiff test, abnormal homogenous vaginal discharge). 13
Data analysis
Factors associated with baseline BV infections.
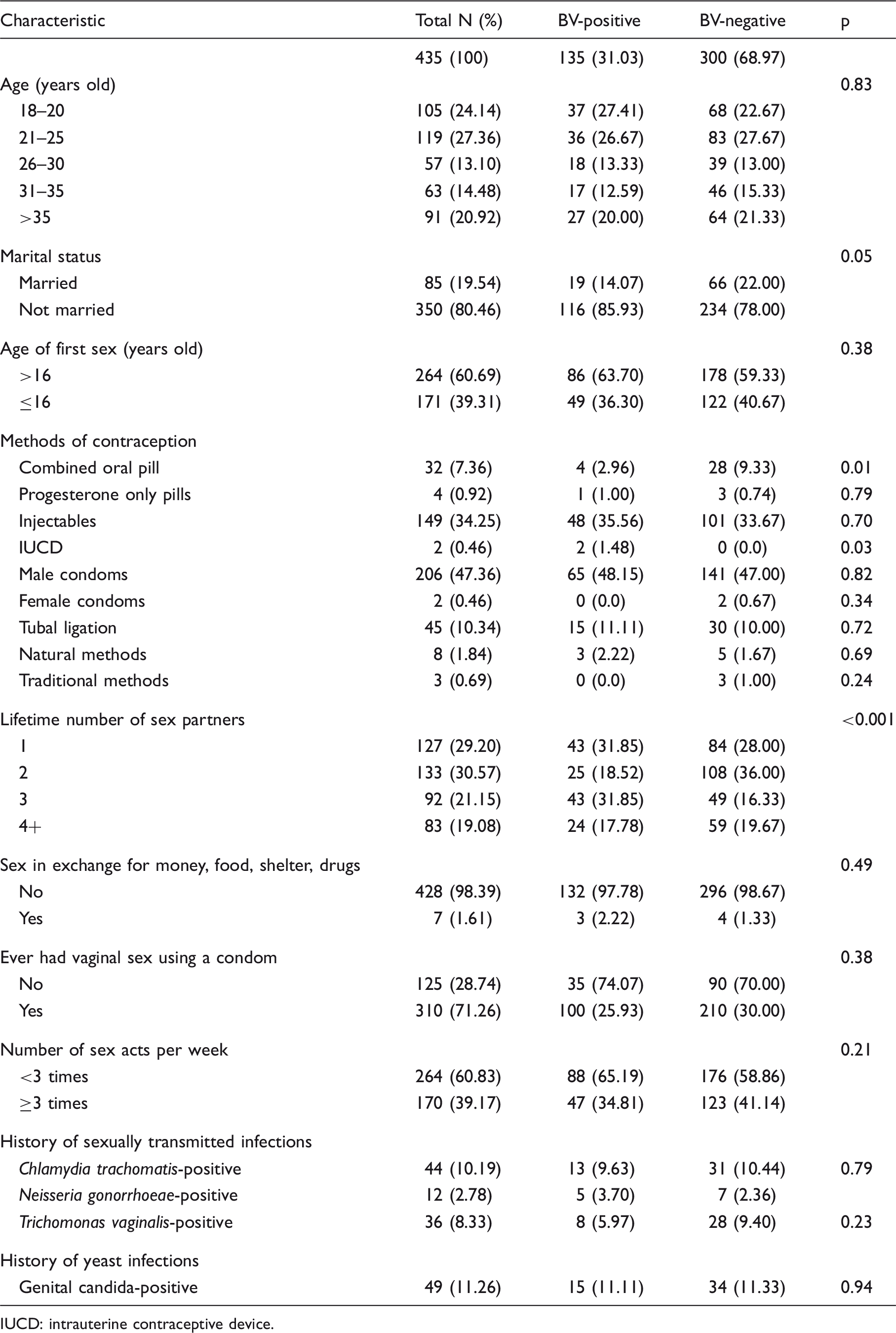
IUCD: intrauterine contraceptive device.
Results
Characteristics of the study population
Of the 1485 women enrolled in this study, 435 women who had an abnormal physical examination (abnormal vaginal epithelium, abnormal vaginal discharge, abnormal perineum/perianal area, abnormal cervical mucus, abnormal cervical epithelium) were included in this analysis. The median age of the women was 25 years (inter quartile range: 21–35). Most women were unmarried (80.46%) and had experienced first sex at >16 years of age (60.69%). Male condoms were the main contraceptive method for 47.36% of the women and 34.25% of the women used injectable hormonal contraceptives. A history of genital candida (11%), C. trachomatis (10.19%) and T. vaginalis infections (8.33%) was common whereas N. gonorrhoeae infections were rare (2.78%). A larger proportion of women reported having had sex <3 times in the past week (60.83%), and most women reported having two or more lifetime sex partners (70.8%).
Characteristics of the study population associated with BV status
The baseline characteristics of the women according to BV status are described in Table 1. At baseline, 300 (68.97%) women had tested negative for BV, whereas 135 (31.03%) were diagnosed as positive. The prevalence of BV was higher in unmarried women (85.93% vs. 14.07%, p = 0.05). Use of combined oral contraceptive pills was shown to have a significant protective effect against infection (p = 0.01), whereas a contrary effect was observed in women who had an intrauterine contraceptive device (IUCD) (p = 0.03). Having three lifetime sex partners was also significantly associated with baseline BV infections (p < 0.001).
Baseline BV in association with incident of STIs
The association between BV and acquisition of sexually transmitted infections.
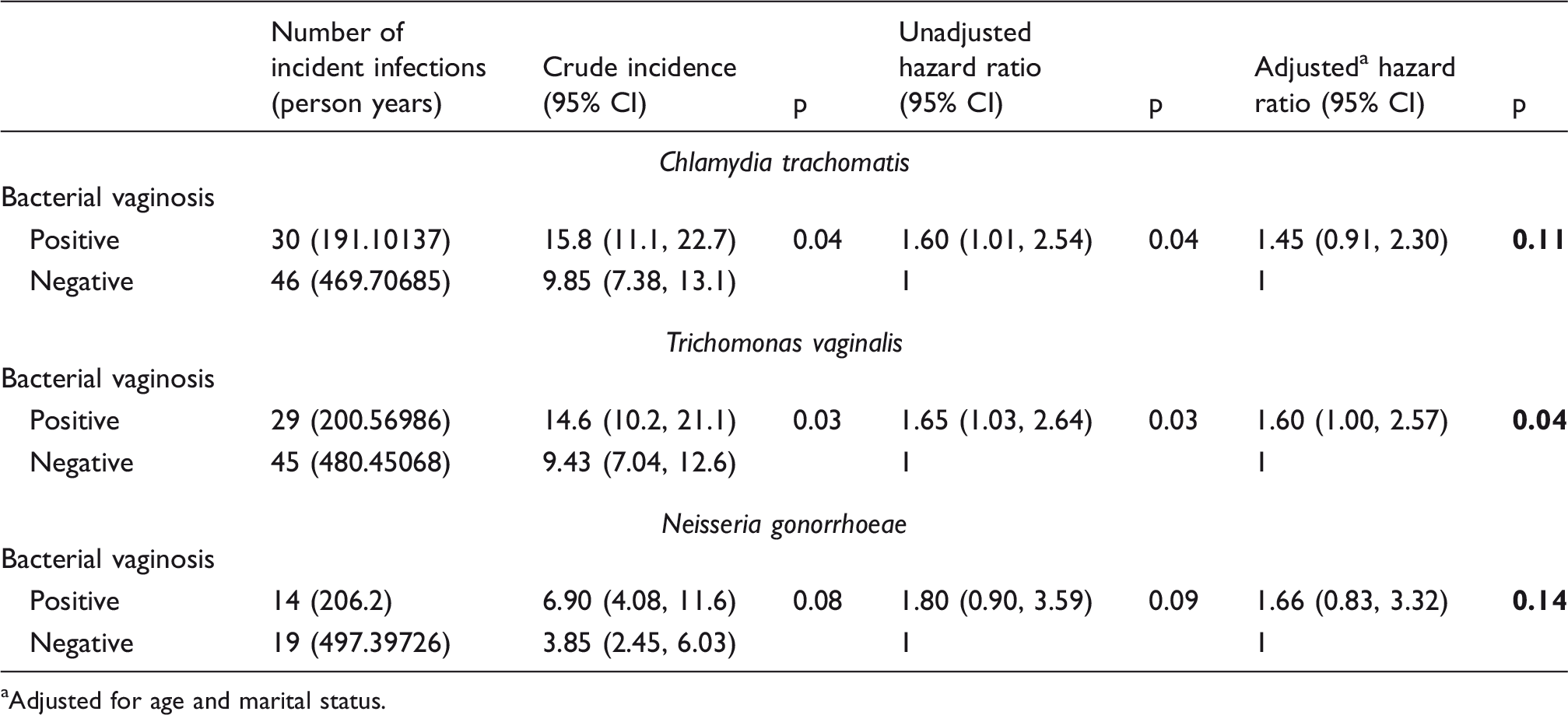
Adjusted for age and marital status.
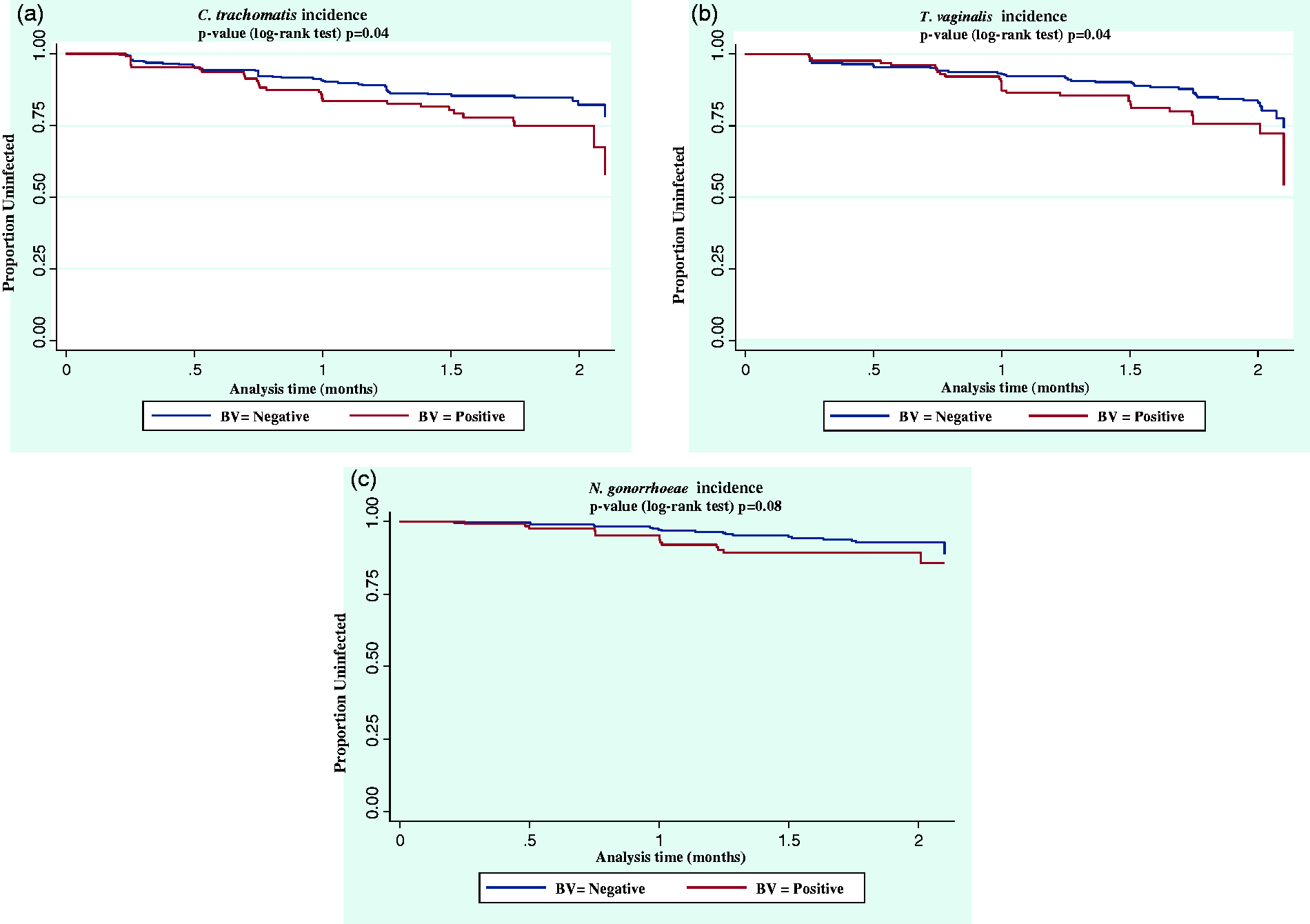
Kaplan–Meier plots showing the survival rates for the individual sexually transmitted infections according to baseline BV status with the crude STI incidence rates calculated for each variable with the respective p-values. (a) C. trachomatis incidence; (b) T. vaginalis incidence and (c) N. gonorrhoeae incidence.
There were 74 incident T. vaginalis infections in total, and 29 infections were detected in the group of women diagnosed with BV (200.6 PY). Similarly, a higher T. vaginalis incidence rate (14.6 per 100 PY) was reported for women with baseline BV when compared to women who tested BV negative (14.6 per 100 PY vs. 9.43 per 100 PY), (p = 0.03), respectively. The Kaplan–Meier curves, stratified by BV status at baseline, are presented in Figure 1(b).
Overall, there were 33 incident N. gonorrhoeae infections of which 14 infections were shown to be present in the group of women diagnosed with BV (206.2 PY). Although the number of incident N. gonorrhoeae infections was higher in women with BV infection when compared to women who were BV negative (6.9 per 100 PY vs. 3.85 per 100 PY), this result was not statistically significant (p = 0.08). There was no significant difference between BV status and future N. gonorrhoeae infections (Figure 1(c)).
In the univariate analysis, BV was shown to be significantly associated with incident T. vaginalis infections (Hazard ratio [HR]: 1.65, 95% Confidence Interval [CI]: 1.03, 2.64, p = 0.03) and C. trachomatis infections (HR 1.60, 95% CI: 1.01, 2.54, p = 0.04). In the multivariate analysis BV remained a significant predictor for T. vaginalis infections even after adjusting for potential confounders such as age and marital status (HR: 1.60, 95% CI: 1.00, 2.57, p = 0.04).
Discussion
Our study identified an association between baseline BV infections and the acquisition of T. vaginalis infections. Similar findings were reported in previous published studies.9,14,15 In a study conducted by Balkus et al., 9 BV was shown to significantly increase the likelihood of T. vaginalis infections by more than two-fold. Similarly, Gatski et al. 14 showed that abnormal vaginal flora was also associated with an increased risk of acquiring T. vaginalis, suggesting that BV may increase a woman’s susceptibility to T. vaginalis infection. The clinical association between BV and T. vaginalis infections has been described by Brotman. 15 According to Brotman, 15 in vitro data have revealed that Trichomonas grows better at elevated pH, such as that which occurs in a clinically defined BV state.
In our study, we did not find an association between BV and incident C. trachomatis infections. The findings of our study are confirmed by a recently conducted study by Masese et al. 16 In our study, all women who showed signs of BV were treated with metronidazole. It has been shown that BV-positive women who are treated with metronidazole have significantly fewer cases of incident C. trachomatis infections compared with women that are untreated. 15
Although previous studies have found that women who were diagnosed with baseline BV were associated with an increased risk for incident N. gonorrhoeae infections,7,15 the findings of our study did not confirm this. To the best of our knowledge, there were no other published studies that showed similar findings to our study, thereby limiting our basis for comparisons. To this end, we suggest that the inability to detect statistically significant effects could be attributed to the relatively small number of women who tested positive for N. gonorrhoeae, i.e. 33 infections in total of which 14 infections were detected in the BV-positive group, resulting in reduced power.
We acknowledge the following limitation: the data presented in this study are limited to the population of women in which the research was conducted and may not be representative of women in the general population. In addition, for this analysis, we focused primarily on the assessment of BV conducted at baseline, and this may not be representative of the vaginal environment around the time of infection which remains unknown. Due to baseline BV testing only being performed on symptomatic patients, we also acknowledge that the prevalence of BV at baseline presented may be overestimated in our analysis. Despite these limitations, this study emphasises the role of BV as a risk factor for STIs in women in the communities that we work with. Our findings therefore advocate the need for strengthening STI prevention efforts among women in high burden STI settings. Additionally, our efforts also need to be directed towards investigating newer treatment options for BV which produces high cure rates since BV is a highly recurrent infection and predisposing factor for future STIs.
Footnotes
Acknowledgements
We gratefully acknowledge the contribution of the women who participated in this study. We thank the MIRA team at the University of California (San Francisco), Ibis Reproductive Health and members of the HIV Prevention Research Unit (MRC South Africa).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the financial support of the Bill and Melinda Gates Foundation (Grant number 21082).