
Abstract
Men who have sex with men are disproportionately impacted by HIV and substance use is a key driver of HIV risk and transmission among this population. We conducted a cross-sectional survey of 3242 HIV-negative substance-using men who have sex with men aged 18 + in the San Francisco Bay Area from March 2009 to May 2012. Demographic characteristics and sexual risk and substance use behaviors in the last six months were collected using structured telephone questionnaires. We used multivariable logistic regression to identify independent demographic and behavioral predictors of recent HIV testing. In all, 65% reported having an HIV test in the last six months. In multivariable analysis, increasing age (aOR = 0.87, 95% CI = 0.84–0.90) and drinking alcohol (<1 drink/day: 0.65, 0.46–0.92; 2–3 drinks/day: 0.64, 0.45–0.91; 4 + drinks/day: 0.52, 0.35–0.78) were negatively associated with recent HIV testing. Having two or more condomless anal intercourse partners (2.17, 1.69–2.79) was positively associated with having a recent HIV test, whereas condomless anal intercourse with serodiscordant partners was not significantly associated with testing. Older men who have sex with men and those who drink alcohol may benefit from specific targeting in efforts to expand HIV testing. Inherently riskier discordant serostatus of partners is not as significant a motivator of HIV testing as condomless anal intercourse in general.
Introduction
More than one in eight of the 1.2 million people living with HIV are unaware of their HIV status and these individuals account for nearly a third of HIV transmissions in the United States (US).1,2 Men who have sex with men (MSM) are the demographic group most severely affected by the HIV epidemic, representing only 2% of the total US population, but accounting for 65% of the nearly 48,000 estimated HIV diagnoses in 2013.3,4 Moreover, new HIV diagnoses among MSM are increasing. 4
Frequent HIV testing and early HIV detection are the foundation of effective care and prevention efforts. 5 The Centers for Disease Control and Prevention (CDC) recommends that sexually active MSM get tested at least annually and the San Francisco Department of Public Health recommends testing at least once every six months.6,7 Recently, a large-scale randomized clinical trial concluded that early detection of HIV infection and initiation of antiretroviral therapy (ART) significantly reduces the risk of developing AIDS and other serious illnesses. 8 In addition, early HIV detection and virologic suppression through treatment with ART effectively reduces HIV transmission (i.e. treatment as prevention).9,10 Moreover, reductions in high-risk sexual behavior are seen in individuals after they become aware of their positive HIV status. 11 Despite the significant personal and community impacts of HIV testing and subsequent treatment of HIV-positive individuals, data from the 2011 US National HIV Behavioral Surveillance indicate that one-third of HIV-positive MSM are not aware of their infection and one-third of all MSM had not been tested in the last 12 months.12,13 Highlighting the significance of this issue, the latest update of the National HIV/AIDS Strategy for the United States includes widespread testing and linkage to continuous and comprehensive care for persons living with HIV as areas of critical focus for the next five years. 14
Prior research identified links between substance use and both sexual risk behaviors and HIV infection among MSM, making substance-using MSM a particularly vulnerable population.15–17 In addition to a heightened risk of HIV acquisition and transmission, substance use has also been adversely associated with other HIV-related outcomes among individuals infected with HIV, including lower CD4 T-cell count, viral suppression, and medication adherence.18–25 Although substance use has been identified as an important risk factor for multiple outcomes from acquisition to treatment of an HIV infection, little is known about the relationship between substance use and HIV testing behaviors. The use of amyl nitrate inhalants (i.e. poppers) has been linked to increased HIV testing among MSM in King County, Washington, but no studies have investigated the relationship between alcohol or other specific illicit substances and HIV testing behaviors.26,27 Moreover, no study has examined correlates of recent HIV testing among a population of substance-using MSM, who are at higher risk for infection. To address these gaps and inform efforts to expand HIV testing, we aim to identify the demographic, sexual risk behavior, and specific substance use correlates of reporting an HIV test in the last six months (as recommended by San Francisco's testing guidelines for MSM) among a large cross-sectional cohort of substance-using MSM in San Francisco. Specifically, we hope that our findings will help to identify distinct groups of substance-using MSM who may be under-tested and appropriate for targeted testing efforts.
Materials and methods
Study sample
We conducted a convenience-based cross-sectional survey of HIV-negative substance-using MSM aged 18 and older in the San Francisco Bay Area as part of the screening phase of a randomized clinical trial testing the efficacy of a behavioral HIV prevention intervention (Project ECHO). 28 Project ECHO was a randomized controlled trial assessing the efficacy of adapted personalized cognitive counseling for reducing sexual risk among episodic substance-using MSM. Survey participants were recruited through MSM-specific websites, print advertisements, and active outreach in MSM venues and events. All participants provided informed consent to participate in the survey and study procedures were approved by the Committee on Human Research, University of California, San Francisco (approval number: 10-03925).
Data collection
Trained staff administered structured telephone questionnaires consisting of 45 questions to MSM willing to be screened for Project ECHO. Telephone interviews lasted 10–15 minutes and occurred between March 2009 and May 2012. Demographic characteristics, sexual behaviors, substance use frequency, HIV testing history, and self-reported HIV serostatus of sexual partners from the past six months were collected.
Measures
HIV testing
The primary outcome was participant self-report of an HIV test within the six months prior to the telephone interview (i.e. meeting San Francisco's HIV testing guidelines). This was assessed in the questionnaire by asking whether or not participants had ever been tested for HIV and received the results and, if so, how long ago their most recent test occurred. Possible responses to this latter question were less than six months, six months to less than one year, one year to less than two years, two years to less than three years, three years to less than five years, five years to less than ten years, and ten years or more.
Demographic characteristics
Demographic characteristics assessed were age and race/ethnicity. Race and ethnicity were initially collected as two separate variables: primary race (i.e. Asian/Pacific-Islander, Black/African-American, Mixed, Native-American, white, or other) and ethnicity (i.e. Latino/Hispanic or non-Latino/Hispanic). Participants of any primary race who indicated being Latino/Hispanic were categorized as being Latino/Hispanic and non-Latino/Hispanic participants were categorized as white, black, Asian/Pacific-Islander, or mixed/other.
Sexual behaviors
Sexual behaviors assessed were any condomless anal intercourse (CAI) with male partners, number of CAI male partners (collected as zero, one, or two or more), any CAI with serodiscordant male partners (SDCAI, defined as any CAI with HIV-positive or unknown status partners, which is consistent with previous studies),16,17 number of SDCAI male partners (collected as zero, one, or two or more), and any vaginal sex with female partners. All sexual behaviors were assessed over the entire six-month period preceding the interview.
Substance use behaviors
Use of methamphetamine, cocaine/crack, and poppers were assessed by frequency of use in the last six months. Frequency of use of these substances was initially collected as never, less than once per month, once per month, two to three days per month, once per week, two to three days per week, four to six days per week, or every day. Consistent with previous studies,16,17 frequency of use was re-categorized as no use, episodic use (less than weekly), and weekly or more frequent use. Alcohol use was assessed in the last 30 days as no use, light use (one or fewer drinks per day), moderate use (two to three drinks per day), and heavy use (four or more drinks per day).
Statistical analysis
We assessed bivariate relationships between demographic characteristics, sexual behaviors, and substance use behaviors and self-report of a recent HIV test using Wilcoxon rank-sum and Chi square tests, as appropriate.
We used a multivariable logistic regression model to identify independent predictors of recent HIV testing. Variables that were significant in our bivariate analysis (p < 0.10) were included in our model. The model was fit with age (scaled to units of 5 years), race/ethnicity, number of CAI partners, number of SDCAI partners, frequency of use of meth, cocaine/crack, and poppers, and amount of alcohol use.
Results
Demographic and behavioral characteristics
Sample characteristics and bivariate analysis assessing differences between participants who reported an HIV test in prior six months and those who did not.
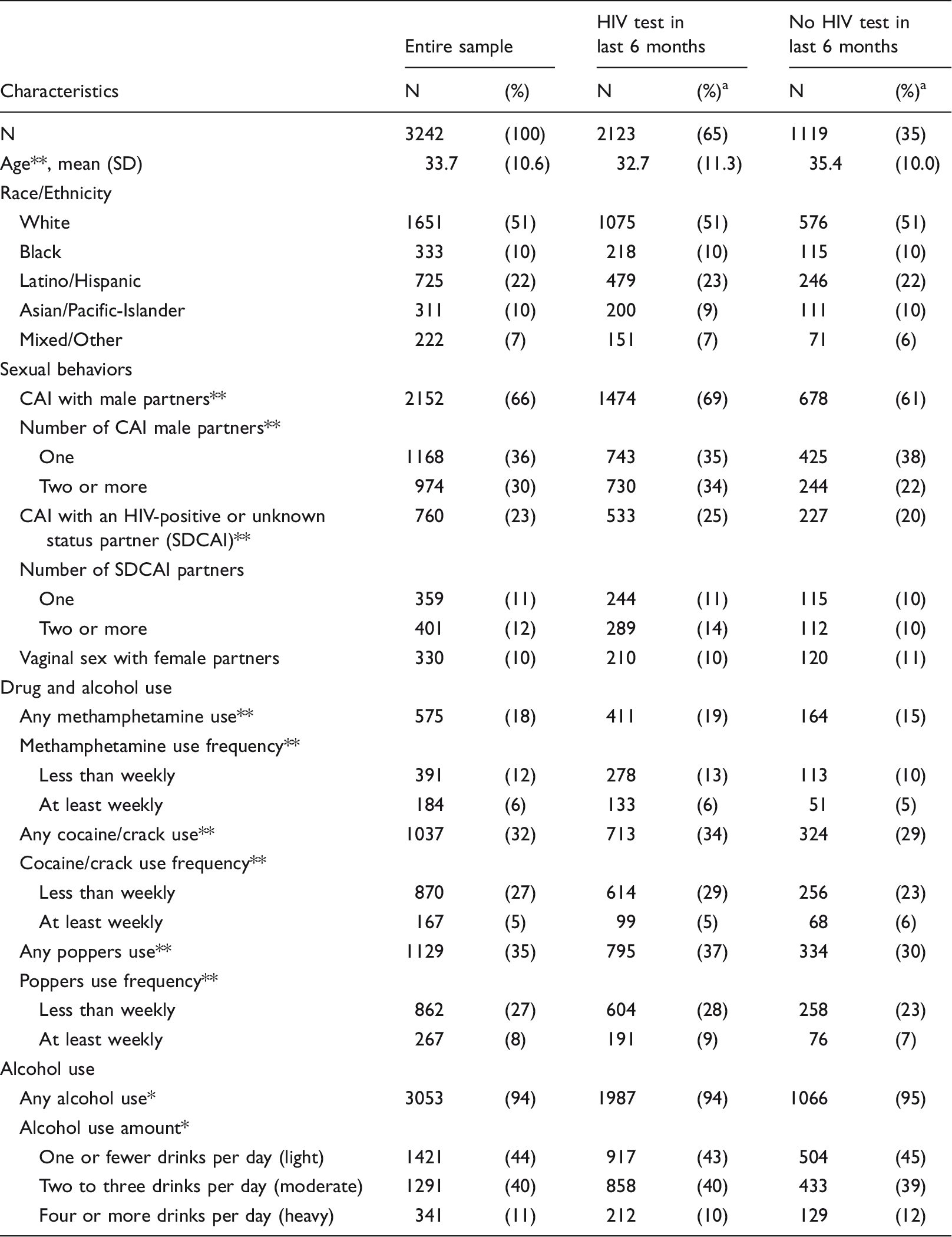
CAI: condomless anal intercourse; SDCAI: serodiscordant condomless anal intercourse.
p < 0.1
p < 0.05 from Wilcoxon rank-sum and Chi square tests.
Percentages of N represent the proportion of the entire sample, whereas all other percentages represent the proportion of those who either did or did not report an HIV test in the six months prior to being interviewed.
Nearly two-thirds (65%) reported having an HIV test in the prior six months. Sixty-six percent reported engaging in CAI, with 23% of all participants engaging in CAI with a serodiscordant partner; 18% used meth, 32% used cocaine or crack, 35% used poppers, and 94% drank alcohol.
Multivariable analysis
Multivariable logistic regression model assessing odds of reporting an HIV test in the last six months.
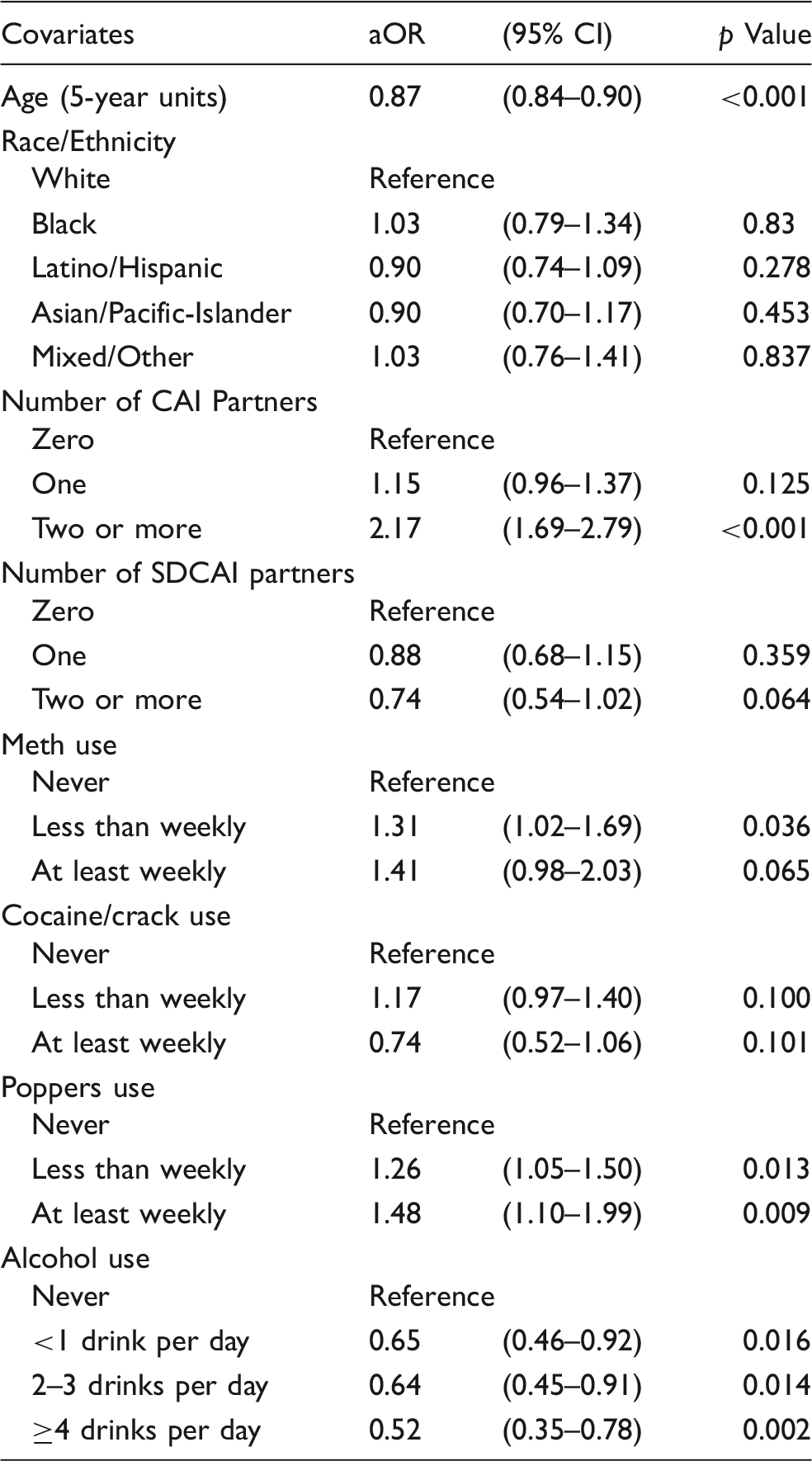
CAI: condomless anal intercourse; SDCAI: serodiscordant condomless anal intercourse.
Discussion
In this large cross-sectional study of substance-using MSM in San Francisco, we observed high rates of recent HIV testing and identified demographic and behavioral characteristics associated with reporting a recent HIV test. Specifically, MSM who had engaged in CAI, and those who used methamphetamine or poppers were more likely to have reported a recent HIV test, whereas older MSM and those who consumed alcohol were less likely. These findings have implications for targeted testing and outreach efforts, particularly as we intensify efforts to initiate early HIV treatment to improve HIV-related health outcomes and implement treatment as prevention strategies.
The proportion of participants reporting a recent HIV test was higher in our study (65% in the last six months; 85% in the last 12 months) than in the National HIV Behavioral Surveillance System (66% in the last 12 months), a national sample of MSM. 12 This is likely a reflection of the higher rates of HIV testing in San Francisco compared to the US overall, which may be the result of local guidelines that call for more frequent testing among MSM (i.e. at least every six months) than the national CDC guidelines (i.e. at least annually).
In multivariable analysis, increasing age was negatively associated with having been recently tested. These results are consistent with other studies that identified provider assumptions regarding sexual behavior and risk as well as lower perceived risk among older adults as key obstacles in linking this population to HIV testing. 29 Highlighting the urgency of this issue is the rising number of HIV diagnoses among older adults, which increased by 19% among adults aged 55 and older from 2010 to 2013. 4 A study of older adults in a large North American cohort found that adults aged 50 or older made up a significantly larger proportion of individuals presenting for HIV care in 2007 compared to 10 years prior and, compared to younger adults, had a lower median CD4 cell count when first presenting for HIV care and were significantly more likely to have had an AIDS-defining diagnosis at or within three months before their first presentation for care. 30 Older MSM may be affected by increasing HIV risk, greater likelihood of delayed presentation for care, and multiple barriers to HIV testing, which highlights them as a particularly vulnerable group to be targeted with expanded availability of HIV testing. Among older adults, having a recent doctor visit is associated with having a recent HIV test and encouragement from healthcare providers is a key facilitator of HIV testing, suggesting that healthcare professionals may play an important role in expanding coverage of HIV testing in this population.31,32
The positive findings related to CAI, number of CAI partners, and HIV testing are consistent with prior research; however, our exploration of both CAI and SDCAI suggest that CAI, regardless of partner serostatus, is a stronger correlate of HIV testing behavior relative to SDCAI. Study participants may recognize the limitations of sero-sorting (i.e. having CAI with individuals presumed to have the same serostatus) as an HIV prevention measure and instead seek testing based on their sexual activity overall. However, these links between CAI, serostatus of sexual partners, perceived risk, and HIV testing warrant further exploration that is beyond the scope of this analysis.
Use of methamphetamine and use of poppers were positively associated with having been recently tested for HIV, independent of sexual risk behavior. The link between use of poppers and HIV testing is consistent with prior research, but the pathway through which this association is manifested has not been thoroughly explored;26,27 to our knowledge, this is the first study to report an association between methamphetamine use and recent HIV testing. One plausible explanation for these associations is that engagement in high-risk sexual behaviors that have been linked with the use of these substances, such as participation in group sex events or sexual marathons (defined as prolonged sexual activity over hours or days), may motivate MSM to get tested for HIV with greater frequency.33,34 Alternatively, an extensive media campaign launched in 2008 and aimed to reduce methamphetamine use among MSM in California may have influenced testing behaviors in this population by highlighting links between methamphetamine use and HIV risk. 35 However, targeted research examining these linkages is necessary to fully elucidate the pathways by which they operate and identify any gaps in testing engagement among MSM who use methamphetamine or poppers.
We also found that MSM who consume any alcohol (light, moderate, or heavy use) are less likely to have had a recent HIV test, which is particularly notable given the high prevalence of alcohol use in both our sample and MSM in general. 36 Moreover, multiple studies identified heavy alcohol use and binge drinking as significant drivers of HIV seroconversion.37,38 Hence, MSM who drink heavily may be at increased risk for HIV infection and less likely to be aware of their HIV status as a result of less frequent testing. Our findings highlight the potential suitability of offering rapid testing in community-based settings that involve alcohol consumption. Indeed, several studies have shown the feasibility and cost-effectiveness of mobile testing efforts at bars, nightclubs, and community events that may involve alcohol, such as Gay Pride events.39–41 These strategies should be further explored in efforts to expand HIV testing among HIV-positive MSM who consume alcohol and may be both unaware of their infection and at heightened risk of transmission.
In addition to the potential expansion of HIV testing through healthcare settings for older MSM and community settings for those who consume alcohol, future studies should examine the acceptability of HIV home tests among these populations of MSM. 42 HIV home tests have been shown to be highly acceptable among MSM in general, but no studies have evaluated the uptake or acceptability of these tests among older MSM, those who consume alcohol, or any other MSM subgroup.43–46
More comprehensive HIV testing among MSM, particularly among the groups we have identified as being under-tested, may reduce HIV transmission by facilitating treatment as prevention strategies as well as by motivating safer sexual behaviors among HIV-positive individuals; however, it is important that expanded testing occur in conjunction with other effective prevention strategies that target HIV-negative individuals, including pre-exposure prophylaxis (PrEP), post-exposure prophylaxis (PEP), condoms, and behavioral interventions that aim to reduce sexual risk. 47
Our study has several limitations. First, our convenience sample may not be generalizable to all substance-using MSM. Second, the self-reported data in this study may be subject to recall or social desirability bias. Third, our cross-sectional measure of HIV testing only captures the date of each participant's most recent HIV test and does not necessarily correspond to frequency of testing. Fourth, because we leveraged limited phone screen data, we did not have access to other potential confounders associated with substance use, sexual risk, and HIV testing behaviors, such as education, income, or an inclination for sensation seeking or risk-taking behavior.36,48
This study identified multiple groups, older substance-using MSM and those who drink alcohol, who may benefit from specific targeting in efforts to expand HIV testing. We also added to prior evidence that MSM engaging in CAI and with more partners tend to get tested more frequently, but also found that inherently riskier discordant serostatus of partners is not as significant a motivator of HIV testing. Additionally, we highlighted the links between the use of both methamphetamine and poppers and HIV testing behaviors, emphasizing the need for further research to better understand these mechanisms and inform HIV testing outreach strategies targeting substance-using MSM. These findings are of particular importance given the essential role of earlier detection of HIV infection in both effective individual care and population prevention efforts.
Footnotes
Acknowledgements
The authors acknowledge John Farley, Alic Shook, Reggie Gage, and the study field recruitment team for their invaluable contributions during data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Centers for Disease Control and Prevention under cooperative agreement UR6PS000684 to Public Health Foundation Enterprises, City of Industry, CA.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention or the San Francisco Department of Public Health.