
Abstract
Routine HIV surveillance cannot distinguish between recent and older infections: HIV-positive individuals reported soon or long after infection are both considered new diagnoses from a surveillance perspective, notwithstanding the time since infection. This lack of specificity makes it difficult to understand the jurisdiction-specific trends in HIV epidemiology needed for prevention planning. Previous efforts have been made to discern such timing of infection, but these methodologies are not easily applied in a public health setting. We wished to develop a simple protocol, using routinely collected information, to classify newly diagnosed infections as recent or older, and to enumerate and characterize recent versus older infections. Applying our methodology to a review of HIV cases reported between January 2011 and December 2014, we classified 62% of cases; one-third of these were recent infections. Although men who have sex with men (MSM) and persons from HIV-endemic countries (HEC) disproportionally accounted for new HIV diagnoses, the dynamics of HIV transmission within these groups differed dramatically: MSM accounted for the majority of recent infections, whereas persons from HEC accounted for the majority of older infections. Among older infections, one-quarter were previously unaware of their infection. Categorizing cases in this manner yielded greater, jurisdiction-specific understanding of HIV, and guides subpopulation-specific interventions.
Keywords
Introduction
HIV diagnoses are reportable to public health authorities across Canada. 1 However, because many people are not diagnosed with HIV in a timely fashion – due to, for example, poor access to, or inadequate assessments during, care – infections reported to public health are not always recently acquired.2,3 That is, public health surveillance in Canada captures new diagnoses irrespective of whether these cases are new infections or not. Because prompt diagnosis can correspond with improved patient outcomes and decreased onward HIV transmission,4,5 previous efforts have attempted to discern the proportion of persons who are diagnosed recently versus later after infection.6,7 Further benefits of knowing such information is that it helps frontline care providers and policy-makers know the extent to which persons living with HIV access established testing services, and thus provides suggestions about where and among whom HIV testing services should be targeted.
Many previous efforts to determine the proportion of people diagnosed recently after acquiring HIV, however, relied on specialized laboratory or research protocols, 6 or were limited to clinical settings. 7 These strategies are thus not practical for routine frontline practice or for broader understanding of HIV epidemiology. Consequently, using routinely collected public health data – rather than a specialized or additional data collection protocol – we sought to identify specific sub-groups of HIV cases who come to the attention of public health either early or later in infection. To undertake this analysis, we reviewed HIV surveillance data for a public health jurisdiction (Ottawa, Canada) with the following goals: (1) determine if HIV cases can be categorized into recent versus older infections based on routinely-collected information in the public health case management chart and (2) quantify and characterize cases reported soon after infection (‘recent’) versus later in infection (‘older’), and cases reported later in infection who were aware of being HIV-positive (‘older, aware’) versus those unaware (‘older, unaware’).
Methodology
Laboratory confirmation
In Ottawa, HIV testing occurs in the Ontario Public Health Laboratories, where samples are screened with a fourth generation chemiluminescent micro-particle immunoassay (CMIA) that can detect anti-HIV antibodies (IgM and IgG) and p24 antigens but cannot identify which component of the test is reactive.
8
This test, the ARCHITECT®, has a published sensitivity approaching 100% and specificity of 99.5% when used to screen venous blood samples from persons >12 weeks after HIV exposure.
8
Because the various markers of HIV seroconversion are staggered, however, the ARCHITECT® can likely detect 99.99% (99.995–99.973%) of new infections after 6 weeks.
9
This is because, on average, the HIV p24 antigen becomes detectable 7 days (range: 5–10) after HIV RNA, followed by IgM and IgG 3 days (range: 2–5) after the p24 (Figure 1). Then, over the next 6 days (range: 4–8), the p24 becomes negative, and the Western Blot is positive, negative, or indeterminate. Lastly, after 70 days (range: 40–122), the Western Blot is positive (with the p31 antigen negative).9,10
Biological responses and test detection during HIV infection.
Based on the foregoing, the algorithm for the ARCHITECT® dictates that a negative CMIA result is interpreted as ‘HIV antibody-Non-Reactive.’ 11 A positive or indeterminate CMIA result, in contrast, undergoes Western Blot analysis specific to HIV-1. 11 If the Western Blot is positive, the result is ‘Positive for HIV-1 Antibody.’ Samples with a negative or indeterminate Western Blot result are analyzed with the VIDAS HIV p24 II assay. 11 Positive samples from this assay are re-tested using the VIDAS HIV p24 II Confirmatory Assay. 11 Confirmed p24 positive samples are reported as ‘Evidence of HIV-1 Infection prior to Seroconversion.’ 11 If the CMIA result is positive, yet with negative or indeterminate Western Blot and/or p24 antigen results, the test is deemed ‘inconclusive,’ with a recommendation for re-testing four weeks later. 11
Reporting to Public Health
In Ontario, by law, laboratories and healthcare providers must report, to local public health departments, the detection of HIV antibody with confirmation, or detection of HIV nucleic acid or p24 antigen, in persons older than 18 months.12–14 Public health departments must, in turn, record reported cases of HIV using the Integrated Public Health Information System (iPHIS). 15 This database standardizes the information collected about persons diagnosed with HIV, and includes, among other items, basic demographic details, risk factors, previous negative HIV results, symptoms and AIDS defining illnesses, and reason for testing. 15
For this project, records for HIV-positive individuals reported to Ottawa Public Health (OPH) from 2011 through 2014 (n = 317) were extracted from iPHIS. OPH case management charts for these individuals were reviewed to confirm the data in iPHIS as well as to collect timing of symptoms and HIV exposures through a review of the public health and infectious disease notes. Using this information, we then categorized cases as ‘recent’ (infection most likely occurring within the year prior to report of the case to OPH), ‘older’ (infection most likely occurring more than a year prior to report of the case to OPH), or ‘unknown’ (timing of infection cannot be determined); and to sub-categorize ‘older’ cases as previously ‘aware’ (individuals who report being previously diagnosed with HIV) or ‘unaware’ of their infection (individuals who do not report being previously diagnosed with HIV). A one-year cut-off for recent infections was used for surveillance purposes only and is not based on the biological course of HIV; also, most screening guidelines recommend testing annually or more frequently if at higher risk.
Previous HIV testing, as reported by the individual was the primary consideration during categorization. Individuals with a negative laboratory test within the year prior to report or a reactive p24 upon report were categorized as having a ‘recent’ infection (Figure 2a), while those with a positive laboratory test more than one year previously were categorized as having an ‘older’ infection (Figure 2b). Individuals with neither of these laboratory results were categorized as ‘recent’ if they met two secondary criteria for recent infection or ‘older’ if they met one secondary criterion for older infection.
Criteria used to determine whether timing of infection relative to public health reporting is (a) recent (< 1 year), or (b) older (>1 year).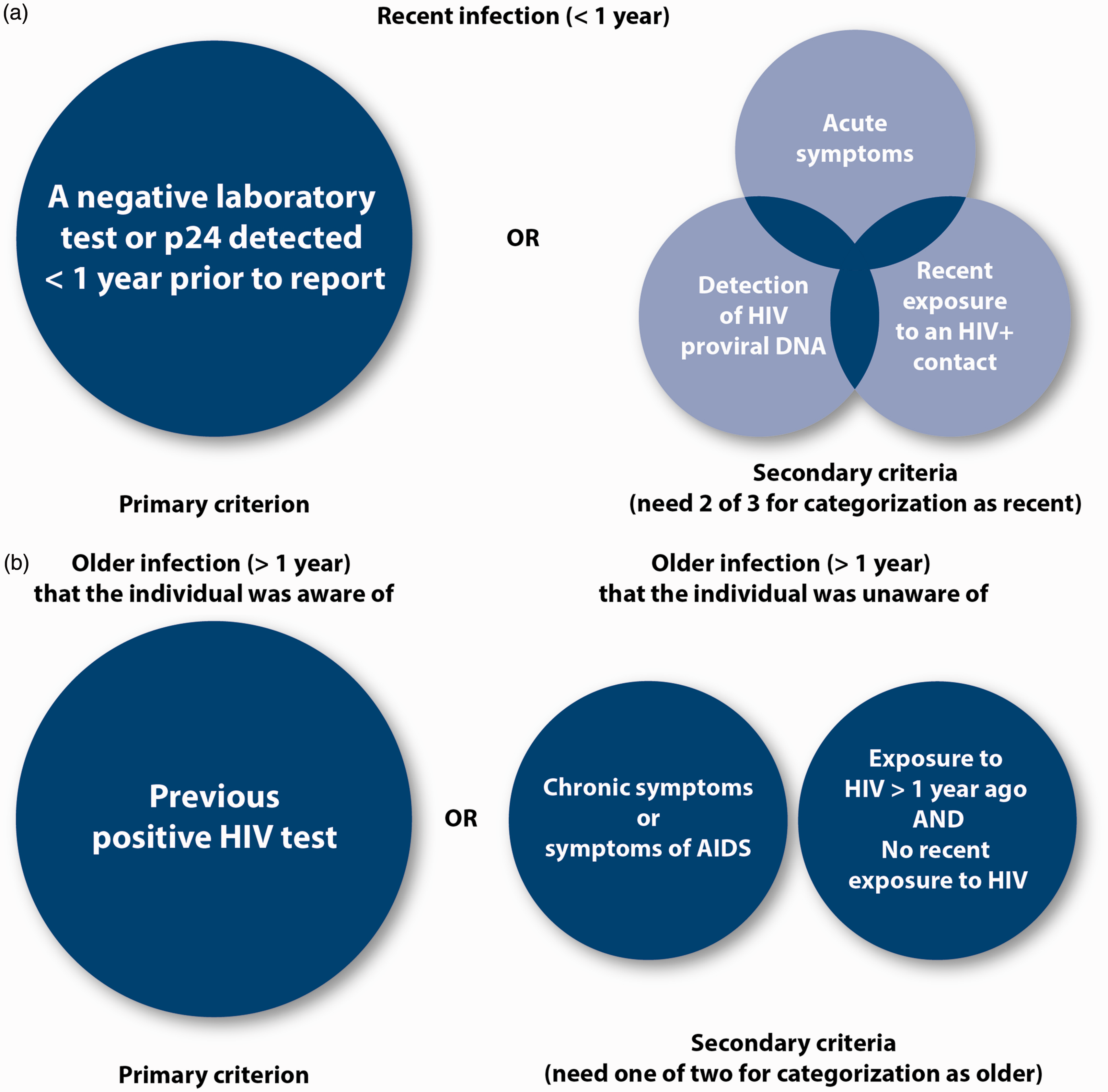
Secondary criteria for recent infection include recent contact that could transmit HIV with an HIV-positive person, symptoms consistent with an acute HIV infection, and detection of HIV proviral DNA. Symptoms considered suggestive of an acute HIV infection include, based on the reported overall frequency of occurrence, fever (75%); fatigue; (68%); myalgia (49%); rash (48%); headache (45%); pharyngitis (40%); cervical adenopathy (39%); arthralgia (30%); night sweats (28%); and diarrhea (27%). 16 The presence of acute symptoms alone within the one year prior to diagnosis was not sufficient to categorize a case as recent because these symptoms are non-specific. 17
Secondary criteria for older infection include exposure to HIV more than one year ago and no recent exposure to HIV, the presence of AIDS defining diseases, and symptoms of chronic HIV infections (i.e., oral hairy leukoplakia, unexplained fever, fatigue or lethargy, unexplained weight loss, chronic diarrhea, unexplained lymphadenopathy, cervical dysplasia, dyspnea and dry cough, loss of vision, recurrent or chronic candida (oral, vaginal), dysphagia, red/purple nodular or mucosal lesions, herpes zoster (especially if severe, multidermatomal or disseminated), unexplained anemia of chronic disease, increased frequency, or severity of mucocutaneous herpes simplex infection). 13 Older infections with a previous positive laboratory result were sub-categorized as ‘older, aware,’ and older infections without a previous positive laboratory result were categorized as ‘older, unaware.’ Individuals tested anonymously, as well as others without enough information to rule out recent or older infection, were categorized as having an infection of ‘unknown’ timing. Because CD4+ cell counts are not reported in the local jurisdiction, they could not be incorporated. Our categorization process thus differs from the Centers for Disease Control practice, 18 which relies on a combination of CD4+ cell count and the presence/absence of opportunistic infections.
The reason for HIV testing is determined from the healthcare provider’s perspective. ‘Routine screening’ as a reason for testing refers to testing carried out without clinical suspicion of HIV or for individuals who tested nominally in order to enter care (e.g. had previous anonymous testing or tested positive outside of Ontario). ‘Immigration screening’ as a reason for testing refers to testing carried out during an individual’s application to immigrate to Ottawa. ‘Symptoms’ was determined to be the reason for testing if the individual presented with HIV-compatible symptoms (early or late stage). ‘Contact tracing’ as a reason for testing refers to individuals tested as a result of contact tracing for a recently-diagnosed case of HIV.
The Ottawa Public Health Research Ethics Board (REB) judged this project not to need REB approval, as it uses routinely-collected public health surveillance data.
Analysis
The association between reporting early or later in infection and demographic factors, risk factors, and reason for testing was determined using Stata version 14.0. The Wilcoxon rank sum test was used to compare differences in age. All other factors were subjected to univariate Chi square analysis; subsequently, all significant demographic factors and risk factors, with the exception of factors with a correlation coefficient of ≤–0.65 or ≥0.65, were analyzed in a multivariable logistic regression model. Associations were considered significant at the α < 0.1 level.
Results
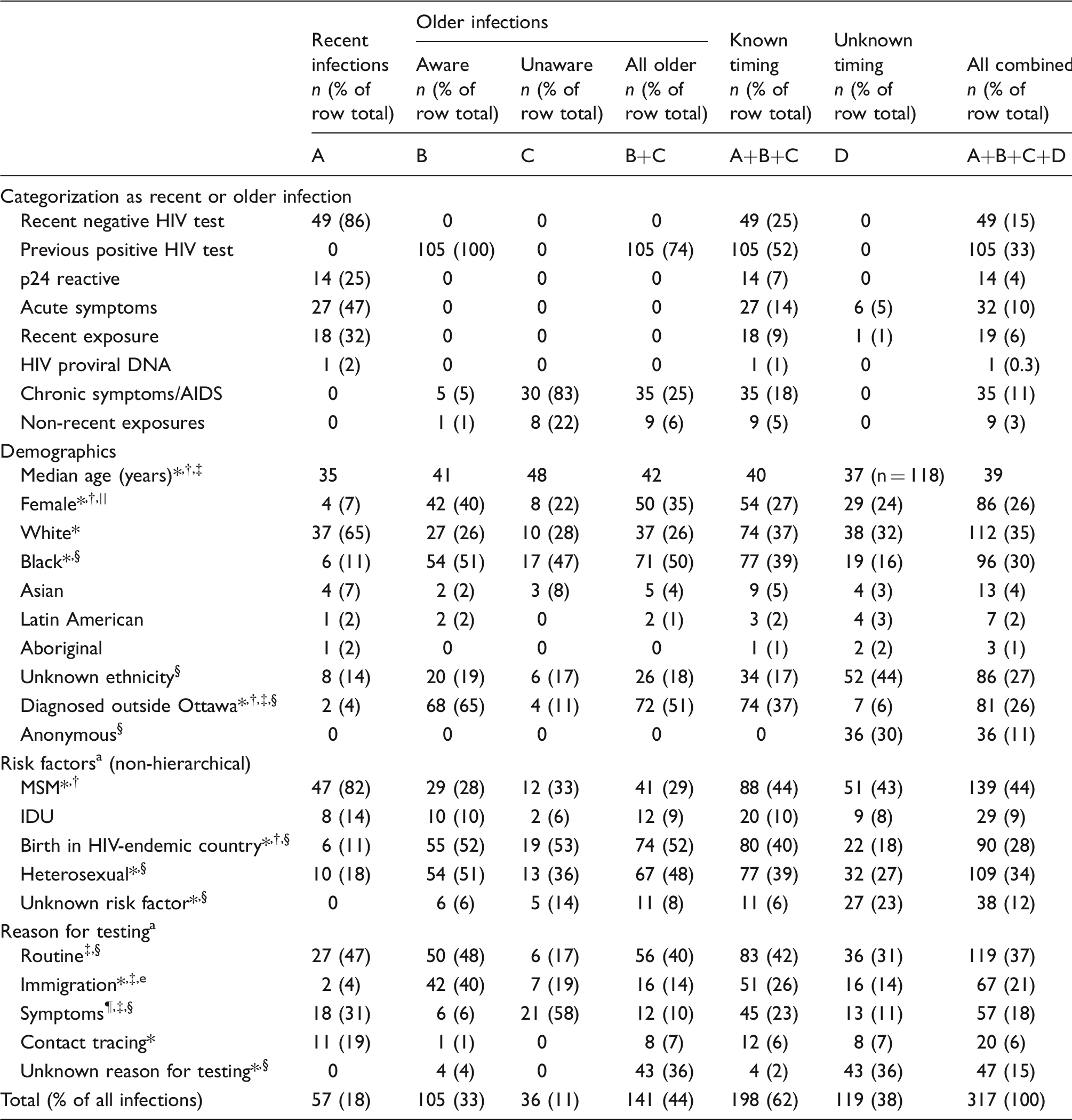
We were able to categorize 63% (n = 198/317) of HIV cases reported to Ottawa Public Health from January 2011 through December 2014 with respect to timing of infection relative to reporting (Table 1). Recent infections comprised 18% of cases, and older infections accounted for 44% of cases, including 11% of who were previously unaware of their infection.
Cases that could not be categorized as recent or older had insufficient information or information consistent with both a recent and an older infection (65%); were tested anonymously, thereby not allowing for the follow up necessary to collect information (30%); or were otherwise lost to follow up (5%).
Characteristics and comparison of recent and older HIV infections, Ottawa, 2011–2014.
MSM: men who have sex with men; IDU: persons who inject drugs.
Notes:
Column headings are as follows:
Recent infections (A): infections determined to have most likely occurred within the year prior to report of the case to public health.
Older, ‘Aware’ (B): infections determined to have most likely occurred more than a year prior to report of the case to public health in which the individual was previously aware of the infection.
Older, ‘Unaware’ (C): infections determined to have most likely occurred more than a year prior to report of the case to public health in which the individual was previously unaware of the infection.
Unknown Timing (D): infections for which timing of infection relative to report to public health cannot be determined.
*p < 0.05 in univariate analysis comparing recent and older infections.
p < 0.05 in multivariable analysis comparing recent and older infections.
p < 0.05 in univariate analysis comparing ‘older, aware’ and ‘older, unaware’ infections.
p < 0.05 in univariate analysis comparing infections with known timing and unknown timing.
p < 0.1 in univariate analysis comparing ‘older, aware’ and ‘older, unaware’ infections.
p < 0.1 in univariate analysis comparing recent and older infections.
Cases can have more than one risk factor or reason for testing.
Recent versus older infections
Cases diagnosed with recent infection significantly differed from cases diagnosed with older infection with respect to demographic factors (Table 1). In univariate analysis, individuals reported with recent infection were more likely than individuals reported with older infection to be younger (median, 35 years vs 42 years), male (93% vs 65%), White (65% vs 26%), and diagnosed while living in or immigrating to Ottawa (96% vs 49%). Individuals with recent infection were less likely to be Black (11% vs 50%) or born in an HIV-endemic country (11% vs 52%). Black ethnicity and heterosexual sex were each correlated with birth in an HIV-endemic country; thus, only one (birth in an HIV-endemic country) was used in the multivariable model.
Classification of recent and older HIV infections according to hierarchical a risk factor categories, Ottawa, 2011–2014.
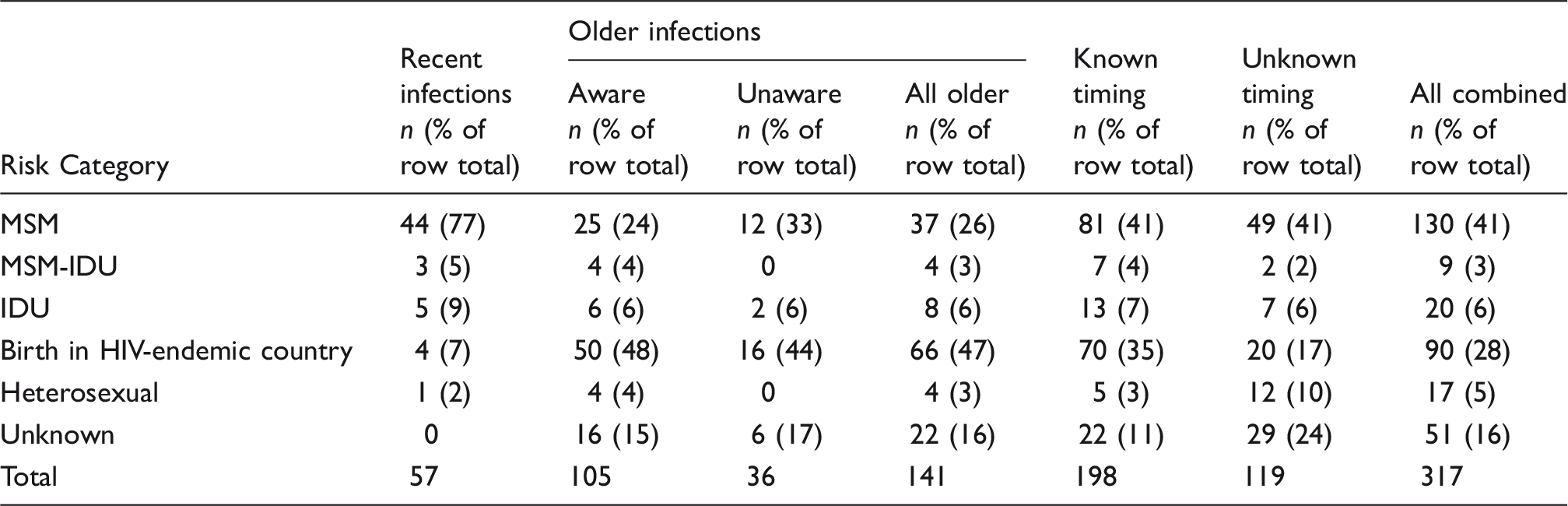
MSM: men who have sex with men; IDU: persons who inject drugs; MSM-IDU: men who have sex with men and inject drugs.
When more than one risk factor is reported for a case, the case was classified according to a mutually exclusive hierarchy which assigns the case to the exposure category which represents the most likely source of HIV infection, according to Remis and Liu J. 19
Cases diagnosed with recent infection significantly differed from cases diagnosed with older infection with respect to risk category. In univariate analyses, recent cases were more likely than cases diagnosed with older infection to be males reporting sex with males (MSM) (82% vs 29%), and were less likely to report sex with the opposite sex (18% vs 48%). In multivariable analysis, MSM were associated with recent infection; birth in an HIV-endemic county and diagnosis outside Ottawa were associated with older infection.
Lastly, reason for testing varied between cases diagnosed with recent infection and those diagnosed with older infection. Routine testing was the most common reason for testing in both groups (42%); however, among individuals with recent infection, contact tracing (19%) and symptoms (31%) were more represented as reasons for testing. Among individuals with older infection, immigration (14%) was more represented as a reason for testing.
Aware versus unaware older infections
There were significant differences between cases with older infection who were previously aware of their infection, compared with those who were unaware of their infection (Table 1). Individuals unaware of their older infection were more likely than individuals aware of their older infection to be older (median, 48 years vs 41 years) and male (78% vs 60%); otherwise, the distribution of risk factors between the two subgroups was similar. Immigration and routine screening were more represented as reasons for testing among individuals previously aware of an older infection (40% and 48% vs 19% and 17%), and symptoms was more represented as a reason for testing among individuals unaware of an older infection (58% vs 6%).
Men who have sex with men
Characteristics of sub-populations of HIV cases with respect to MSM status, origin, and sex, Ottawa, 2011 –2014.
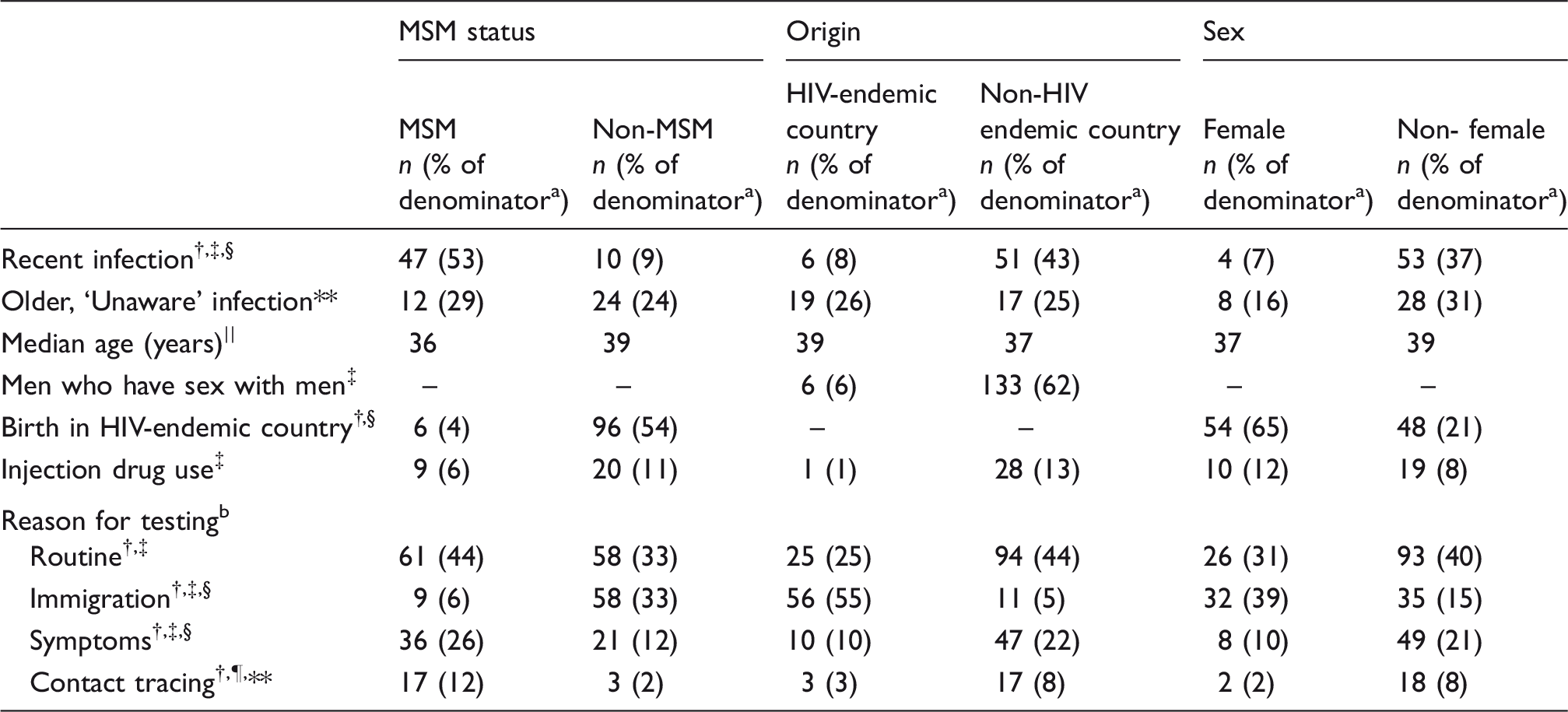
MSM: men who have sex with men; IDU: persons who inject drugs.
Denominators used to calculate percent: • Recent infection – cases with known timing of infection (total = 198; MSM = 88, non-MSM = 110; birth in HIV-endemic country = 80, birth not in HIV-endemic country = 118; female = 54, non-female = 144). • Older infection of which the person was previously unaware – all cases with older infection (n = 141; MSM = 41, non-MSM = 100; birth in HIV-endemic country = 74, birth not in HIV-endemic country = 67; female = 50, non-female = 91). • MSM, birth in HIV-endemic country, IDU, and reason for testing – all cases (n = 317; MSM = 139, non-MSM = 178; birth in HIV-endemic country = 102, birth not in HIV-endemic country = 215; female = 83, non-female = 234).
Cases can have more than one reason for testing.
p < 0.05 comparing MSM and non-MSM.
p < 0.05 comparing origin in an HIV-endemic country and origin in a non-HIV endemic country.
p < 0.05 comparing female and non-female.
p < 0.1 comparing MSM and non-MSM.
p < 0.1 comparing origin in an HIV-endemic country and origin in a non-HIV endemic country. **p < 0.1 comparing female and non-female.
Birth in a country endemic for HIV
Compared with cases not identified as born in an HIV-endemic country, cases born in an HIV-endemic country were more likely to be reported later in infection (92% vs 57%) (Table 3). Cases born in an HIV-endemic country did not differ significantly in age from the rest of cases, but were more likely to be tested as a result of immigration screening (55% vs 5%), and less likely as a result of routine screening (25% vs 44%) and symptoms (10% vs 22%). Among cases from an HIV-endemic country who were not diagnosed during immigration, no older infections and 25% of recent infections were among persons who use injection drugs (data not shown).
Females
Females were more likely than non-females to be diagnosed later in infection (93% vs 63%), and females with older infection were less likely than non-females to be unaware of their infection (16% vs 31%) (Table 3). Thirty-nine percent of female cases (vs 15% of non-females) were tested during immigration. Among females not diagnosed during immigration, 11% of older infections and 100% of recent infections were among persons who reported injection drug use (data not shown).
Discussion
In this paper, we present the outcomes of using information contained in iPHIS and local public health case management files to retrospectively categorize newly reported HIV diagnoses as ‘recent’ (infection likely occurred less than one year from case report to OPH), or as ‘older’ (infection likely occurred more than one year prior to such reporting). A review of cases diagnosed from January 2011 through December 2014 resulted in the categorization of 62% of such cases, with approximately 1 in 3 of the classified cases categorized as recent infections.
At least two limitations are worth noting. First, we were unable to categorize almost one-third of cases; those which we categorized may not be representative of all cases. Second, our findings do not represent disease incidence because differential or delayed access to testing, testing that is not reportable to public health, and re-testing after anonymous testing to access care can all cause HIV reporting rates to differ from incidence. Despite these limitations, this analysis raised a few noteworthy points.
First, overall, our results aligned with established trends in reported HIV diagnoses in Canada. 20 The sub-groups of MSM and persons born in an HIV-endemic country accounted for 41% and 28% of local HIV reported cases, respectively, compared to the national incidence estimates of 54% and 14%, respectively. 20 Our analysis thus confirmed that these two groups are key HIV priority populations both locally and nationally.
Second, categorization into recent and older infection helped us better understand the epidemiology of HIV in Ottawa. We now better understand that, among our groups most affected by HIV, MSM accounted for the majority of recent infections, whereas persons born in HIV-endemic countries accounted for the majority of older cases. More specifically, MSM accounted for 77% of recent cases (while, notably, MSM plus IDU accounted for 91% of recent cases), and persons born in HIV-endemic countries accounted for 47% of all older infections and 44% of older infections that people were unaware of. Additionally, we found that injection drug use was associated with recent infection among cases from HIV-endemic countries and among women (although these numbers were small).
Third, the finding of the predominance of MSM among recent cases suggests that HIV incidence and/or frequency of testing is higher in this group. Support for the former comes from studies that, when taken together, suggest that acute HIV infections in a population may propagate ongoing and elevated transmission rates within that population.21–24 (Specifically, this relates to high viral load during early HIV infection, which, in some studies, has corresponded with up to 20% of HIV contacts becoming HIV-positive after sexual contact with a person in this stage of HIV infection. 24 ) Support for the latter point, in contrast, comes from studies of MSM and of people from HIV-endemic countries, which found that relatively fewer HIV-positive MSM were unaware of their HIV status,20,25,26 thus suggesting that testing strategies, including a local gay men’s testing site, 27 and testing norms among gay men, may be leading to faster detection of HIV infections among MSM. We nevertheless question if local testing norms and practices would be sufficient to increase the proportion of recent cases from 54% nationally to 77% locally. Additional research is thus required to determine whether our finding represents a truly increased HIV incidence rate, or if it is an artifact of increased testing.
Lastly, the finding that a sizable fraction of individuals with older infection were previously unaware of their infection highlights the need for ongoing case-finding efforts. Indeed, it suggests that established testing initiatives, while enabling certain persons to become aware of their HIV infection recently after acquisition, do not work for all. While a large fraction of individuals from countries where HIV is endemic were previously unaware of an older infection, considerable fractions of men who have sex with men and persons who inject drugs were also previously unaware of their infection. Thus, the reach of current testing strategies needs to be extended across risk groups.
The findings from our methodology for characterizing HIV cases have policy and programmatic implications. Aligning with the UNAIDS strategy ‘know your epidemic,’ 28 with jurisdiction-specific information such as we presented herein, local HIV prevention workers can target specific subgroups in their regions based on their burden of infection. This would include, for example, enhanced case-finding and contact tracing for groups with evidence of a high proportion of recent infections (in Ottawa, MSM); increased access to testing for groups with a high proportion of older infections (in Ottawa, individuals from HIV-endemic countries and females); and specific outreach strategies to ensure diagnosis and subsequent access to care for other sub-populations in which infections occur (in Ottawa, IDU). With increased understanding of the nuances of local HIV epidemics, HIV prevention workers can tailor and target services to specific priority populations as fits the dynamics of the epidemic within their networks, and subsequently work toward decreasing the ongoing burden of this infection for all.
Footnotes
Acknowledgements
The authors acknowledge the support of Ottawa Public Health’s Healthy Sexuality and Risk Reduction Unit and the contributions of case manager Lauren Orser during data extraction. The authors also acknowledge the contributions of the OPH Epidemiology Unit and Hugues Sampasa while preparing the manuscript. Finally, the authors thank the Government of Ontario’s Ministry of Training and Innovation for a training award (POB).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by an Early Researcher Award from the Ontario Ministry of Research and Innovation (POB).